Experiences of Homeless Families in Parenthood: A Systematic Review and Synthesis of Qualitative Evidence

 , , ,
, , ,  and
and
Abstract
1. Introduction
2. Methods
2.1. Inclusion Criteria
2.2. Exclusion Criteria
2.3. Search Strategy
2.4. Evaluation of the Methodological Quality
2.5. Data Extraction
2.6. Data Synthesis
3. Results
3.1. Methodological Quality
3.2. Results of the Extracted Data
3.3. Synthesis of the Qualitative Research’s Results
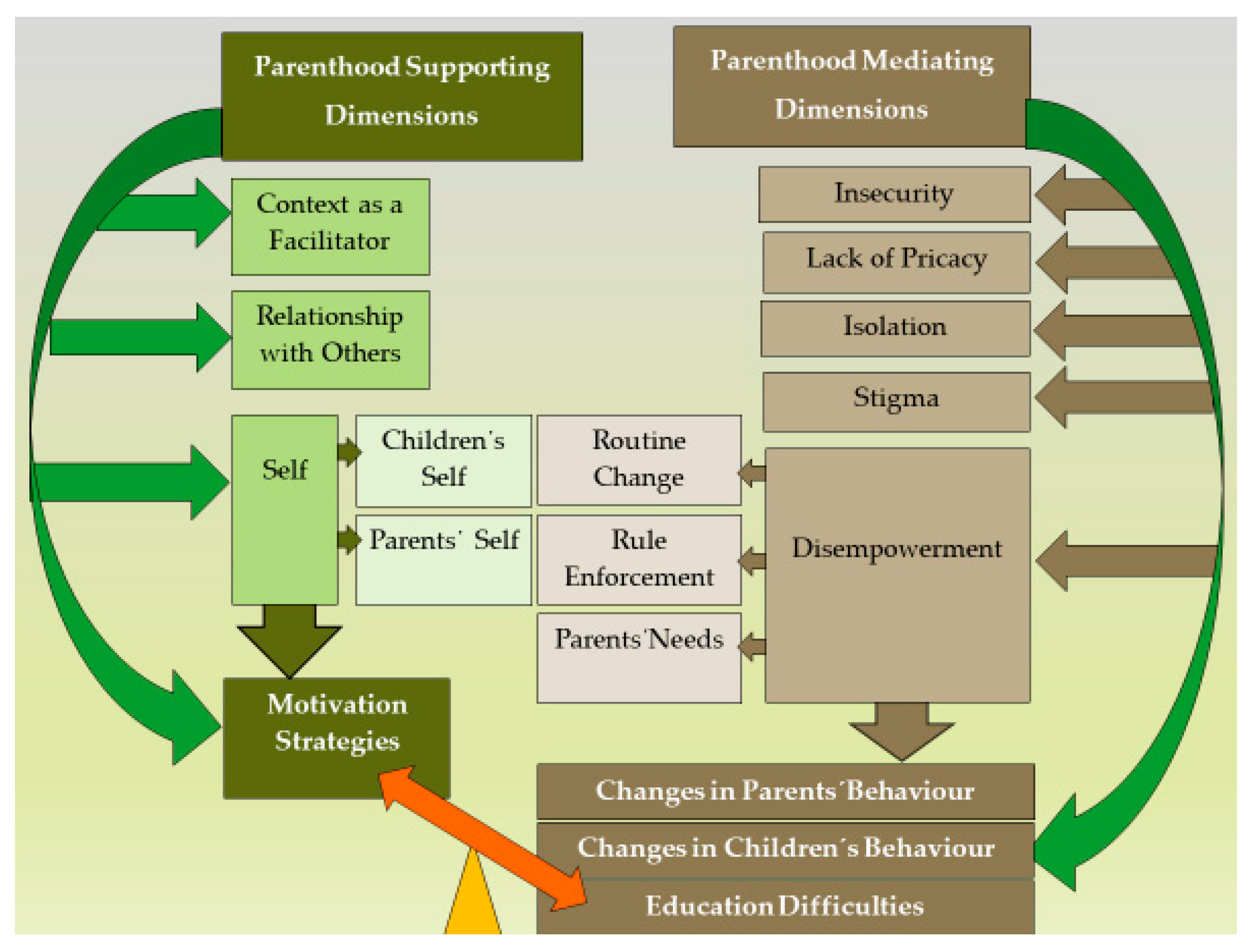
3.4. Synthesis of the Findings
3.4.1. Parenthood Mediating Dimensions
3.4.2. Parenthood Supporting Dimensions
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ordem dos Enfermeiros. CIPE® Versão2—Classificação Internacional Para a Prática de Enfermagem; Ordem Dos Enfermeiros: Lisboa, Portugal, 2011. [Google Scholar]
- Meleis, A.I.; Sawyer, L.M.; Im, E.O.; Messias, D.K.H.; Schumacher, K. Experiencing transitions: An emerging middle-range theory. Adv. Nurs. Sci. 2000, 23, 2–28. [Google Scholar] [CrossRef] [PubMed]
- Meleis, A.I. Transitions Theory: Middle Range and Situation Specific Theories in Nursing Research and Practice; Springer Publishing Company: New York, NY, USA, 2010. [Google Scholar]
- Meleis, A.I. Theoretical Nursing: Development and Progress, 5th ed.; Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012. [Google Scholar]
- Meleis, A.I. Theoretical Nursing: Development and Progress, 4th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2007. [Google Scholar]
- Barroso, R.G.; Machado, C. Definições, dimensões e determinantes da parentalidade. Psychologica 2010, 52, 211–229. [Google Scholar] [CrossRef]
- Hoghughi, M. Parenting: An introduction. In Handbook of Parenting: Theory and Research for Practice; Hoghughi, M., Long, N., Eds.; SAGE Publications Ltd.: London, UK, 2004. [Google Scholar]
- Ordem dos Enfermeiros. Guia Orientador de Boa Prática: Adaptação à Parentalidade Durante a Hospitalização; Ordem dos Enfermeiros: Lisboa, Portugal, 2015. [Google Scholar]
- Cruz, O. Parentalidade; LivPsic: Porto, Portugal, 2005. [Google Scholar]
- Figueiredo, M.H. Modelo Dinâmico de Avaliação e Intervenção Familiar: Uma Abordagem Colaborativa em Enfermagem de Família, 1st ed.; Lusociência—Edições Técnicas e Científicas, Lda: Loures, Portugal, 2012. [Google Scholar]
- Macana, E.C.; Comim, F. O papel das práticas e estilos parentais no desenvolvimento da primeira infância. In Fundamentos da Família Como Promotora do Desenvolvimento Infantil: Parentalidade em Foco; Pluciennik, G.A., Lazzari, M.C., Chicaro, M.F., Eds.; Fundação Maria Cecilia Souto Vidigal: São Paulo, Brasil, 2015. [Google Scholar]
- Nichiata, L.Y.I.; Bertolozzi, M.R.; Takahashi, R.F.; Fracolli, L.A. The use of the “Vulnerability” concept in the nursing area. Rev Latino Am. Enferm. 2008, 16, 923–928. [Google Scholar] [CrossRef] [PubMed]
- Meleis, A.I. Theoretical Nursing: Development and Progress, 6th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2018. [Google Scholar]
- Ministério do Trabalho, Solidariedade e Segurança Social. Estratégia Nacional para a Integração das Pessoas em Situação de Sem-Abrigo (ENIPSSA) 2017-2023. In Presidência do Conselho de Ministros, Resolução do Conselho de Ministros n.º 107/2017, Diário da República n.º 142/2017—Série, I. Available online: https://data.dre.pt/eli/resolconsmin/107/2017/07/25/p/dre/pt/html (accessed on 5 January 2019).
- Anderson, L.; Stuttaford, M.; Vostanis, P. A family support service for homeless children and parents: User and staff perspectives. Child Fam. Soc. Work 2006, 11, 119–127. [Google Scholar] [CrossRef]
- Vostanis, P. Mental health of homeless children and their families. Adv. Psychiatr. Treat 2002, 8, 463–469. [Google Scholar] [CrossRef]
- Kim, K.; Garcia, I. Why Do Homeless Families Exit and Return the Homeless Shelter? Factors Affecting the Risk of Family Homelessness in Salt Lake County (Utah, USA) As a Case Study. Int. J. Environ. Res. Public Health 2019, 16, 4328. [Google Scholar] [CrossRef]
- Simões Figueiredo, A.; Seabra, P.; Sarreira-Santos, A.; Vollrath, A.; Medeiros Garcia, L.; Vidal, T.; Neves Amado, J. Nursing consultation in a public bathhouse: A community resource for the vulnerable population in a European capital. Issues Ment. Health Nurs. 2019, 40, 28–32. [Google Scholar] [CrossRef]
- Gultekin, L.; Brush, B.L. In their own words: Exploring family pathways to housing instability. J. Fam. Nurs. 2017, 23, 90–115. [Google Scholar] [CrossRef]
- Simões Figueiredo, A.; Vidal, T.; Sarreira-Santos, A.; Medeiros-Garcia, L.; García-Padilla, F.; Seabra, P. Nursing consultation in public showers: What lies beyond the results? Issues Ment. Health Nurs. 2019, 40, 535–536. [Google Scholar] [CrossRef]
- Grant, R.; Gracy, D.; Goldsmith, G. Twenty-five years of child and family homelessness: Where are we now? Am. J. Public Health 2013, 103, e1–e10. [Google Scholar] [CrossRef]
- Pleace, N. Family Homelessness in Europe. In Homeless in Europe. Family Homelessness in Europe; Feantsa: Brussels, Belgium, 2019; Available online: https://www.feantsa.org/public/user/Resources/magazine/2019/Autumn/Homeless_in_Europe_Magazine_Autumn2019_final.pdf (accessed on 18 November 2019).
- Baptista, I.; Marlier, E. Fighting Homelessnes Sand Housing Exclusion in Europe: A Study of National Policies; European Commission: Brussels, Belgium, 2019. [Google Scholar]
- Martin-Fernandez, J.; Lioret, S.; Vuillermoz, C.; Chauvin, P.; Vandentorren, S. Food Insecurity in Homeless Families in the Paris Region (France): Results from the ENFAMS Survey. Int. J. Environ. Res. Public Health 2018, 15, 420. [Google Scholar] [CrossRef]
- Sylvestre, J.; Kerman, N.; Polillo, A.; Lee, C.M.; Aubry, T.; Czechowski, K. A qualitative study of the pathways into and impacts of family homelessness. J. Fam. Issues 2018, 39, 2265–2285. [Google Scholar] [CrossRef]
- Bassuk, E.L.; Richard, M.K.; Tsertsvadze, A. The prevalence of mental illness in homeless children: A systematic review and meta-analysis. J. Am. Acad. Child Adoles. Psychiatr. 2015, 54, 86–96. [Google Scholar] [CrossRef] [PubMed]
- Haskett, M.E.; Armstrong, J.M.; Tisdale, J. Developmental status and social-emotional functioning of young children experiencing homelessness. Early Child. Educ. J. 2015, 44, 19–125. [Google Scholar] [CrossRef]
- Mzwandile, A.; Mabhala, M.A.; Yohannes, A. Being at the Bottom Rung of the Ladder in an Unequal Society: A Qualitative Analysis of Stories of People without a Home. Int. J. Environ. Res. Public Health 2019, 16, 4620. [Google Scholar] [CrossRef]
- Gaetz, S.; O’grady, B.; Kidd, S.; Schwan, K. Without a Home: The National Youth Homelessness Survey. Available online: https://homelesshub.ca/sites/default/files/WithoutAHome-final.pdf (accessed on 21 January 2019).
- Perlman, S.; Sheller, S.; Hudson, K.M.; Wilson, C.L. Parenting in the face of homelessness. In Supporting Families Experiencing Homelessness. Current Practices and Future Directions; Haskett, M., Perlman, S., Cowan, B.A., Eds.; Springer: New York, NY, USA, 2014. [Google Scholar]
- Baptista, I. Women and homelessness. In Homelessness Research in Europe: Festschrift for Bill Edgar and Joe Doherty; O’Sullivan, E., Busch-Geertsema, V., Quilgars, D., Pleace, N., Eds.; Feantsa: Brussels, Belgium, 2010. [Google Scholar]
- Lockwood, C.; Porrit, K.; Munn, Z.; Rittenmeyer, L.; Salmond, S.; Bjerrum, M.; Loveday, H.; Carrier, J.; Stannard, D. Chapter 2: Systematic reviews of qualitative evidence. In Joanna Briggs Institute Reviewer’s Manual; Aromataris, E., Munn, Z., Eds.; The Joanna Briggs Institute: Adelaide, Australia, 2017; Available online: https://reviewersmanual.joannabriggs.org/ (accessed on 30 January 2019).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Anthony, E.R.; Vincent, A.; Shin, Y. Parenting and child experiences in shelter: A qualitative study exploring the effect of homelessness on the parent-child relationship. Child. Fam. Soc. Work 2017, 23, 8–15. [Google Scholar] [CrossRef]
- Cosgrove, L.; Flynn, C. Marginalized mothers: Parenting without a home. Anal. Soc. Issues Public Policy 2005, 5, 127–143. [Google Scholar] [CrossRef]
- Haskett, M.E.; Armstrong, J.; Neal, S.C.; Aldianto, K. Perceptions of triple P-positive parenting program seminars among parents experiencing homelessness. J. Child Fam. Stud. 2018, 27, 1957–1967. [Google Scholar] [CrossRef]
- Holtrop, K.; McNeil, S.; McWey, L.M. It’s a struggle but I can do it. I’m doing it for me and my kids: The psychosocial characteristics and life experiences of at-risk homeless parents in transitional housing. J. Marital Fam. Ther. 2015, 41, 177–191. [Google Scholar] [CrossRef]
- Lindsey, E.W. The process of restabilization for mother-headed homeless families: How social workers can help. J. Fam. Soc. Work 1997, 2, 49–72. [Google Scholar] [CrossRef]
- Morris, R.I.; Butt, R.A. Parents’ perspectives on homelessness and its effects on the educational development of their children. J. Sch. Nurs. 2003, 19, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Roche, S.; Barker, J.; McArthur, M. ‘Performing’ fathering while homeless: Utilising a critical social work perspective. Br. J. Soc. Work 2018, 48, 283–301. [Google Scholar] [CrossRef]
- Tischler, V.; Karim, K.; Rustall, S.; Gregory, P.; Vostanis, P. A family support service for homeless children and parents: Users’ perspectives and characteristics. Health Soc. Care Community 2004, 12, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Vanleit, B.; Starrett, R.; Crowe, T.K. Occupational concerns of women who are homeless and have children: An occupational justice critique. Occup. Ther. Heal. Care 2006, 20, 47–62. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Database | Search Strategy |
|---|---|
| PubMed | (((((((((((((((((parenting) OR parenting styles) OR parenting practices) OR parent education) OR childrearing) OR family practice) OR parenting education) OR parenting education) OR parental behaviour) OR parent* behaviour) OR parent* education) OR parent* attitudes) OR altered parenting) OR parent* roll) OR parenthood)) AND ((((homeless persons) OR homeless people) OR homelessness) OR vulnerable populations)) AND (((((((((((((parent* OR biological parents) OR child of impaired parents) OR marriage) OR spouses) OR mothers) OR fathers) OR parents) OR only child) OR nuclear family) OR single parent) OR single parent family) OR family) |
| CINAHL | (parent* OR biological parents OR child of impaired parents OR marriage OR spouses OR mothers OR fathers OR parents OR only child OR nuclear family OR single parent OR single parent family OR family) AND (homeless persons OR homeless people OR homelessness OR vulnerable populations) AND ((MH “Parenting”) OR “parenting” OR (MH “Altered Parenting (NANDA)”) OR (MH “Parenting (Iowa NOC)”) OR (MH “Parenting Alteration (Saba CCC)”) OR (MH “Parenting Education”) OR (MH “Risk for Altered Parenting (NANDA)” OR parenting styles OR parenting practices OR child-rearing OR family practice OR parental behaviour OR parent* behaviour OR parent* education OR parent* attitudes OR parent* role OR parenthood) |
| Quote | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 |
|---|---|---|---|---|---|---|---|---|---|---|
| Anderson et al. 2006 [15] | Y | Y | Y | Y | Y | N | Y | Y | N | Y |
| Anthony et al., 2017 [34] | Y | Y | Y | Y | Y | N | Y | Y | Y | Y |
| Cosgrove and Flynn, 2005 [35] | N | Y | Y | NC | Y | N | Y | Y | N | NC |
| Haskett et al., 2018 [36] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Holtrop et al., 2015 [37] | Y | Y | Y | Y | Y | N | Y | Y | Y | NC |
| Lindsey, 1997 [38] | Y | Y | Y | Y | Y | N | N | Y | N | NC |
| Morris and Butt, 2003 [39] | N | Y | Y | Y | Y | N | Y | Y | Y | Y |
| Roche et al., 2018 [40] | Y | Y | Y | Y | Y | N | Y | Y | Y | Y |
| Sylvestre et al., 2018 [25] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Tischler et al., 2004 [41] | Y | Y | Y | NC | Y | N | Y | NC | Y | N |
| Vanleit et al., 2006 [42] | Y | Y | Y | Y | Y | N | Y | Y | Y | N |
| % Yes | 81.82 | 100 | 100 | 81.82 | 100 | 18.18 | 90.91 | 90.91 | 72.73 | 54.55 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andrade, F.M.R.; Simões Figueiredo, A.; Capelas, M.L.; Charepe, Z.; Deodato, S. Experiences of Homeless Families in Parenthood: A Systematic Review and Synthesis of Qualitative Evidence. Int. J. Environ. Res. Public Health 2020, 17, 2712. https://doi.org/10.3390/ijerph17082712
Andrade FMR, Simões Figueiredo A, Capelas ML, Charepe Z, Deodato S. Experiences of Homeless Families in Parenthood: A Systematic Review and Synthesis of Qualitative Evidence. International Journal of Environmental Research and Public Health. 2020; 17(8):2712. https://doi.org/10.3390/ijerph17082712
Chicago/Turabian StyleAndrade, Filipa Maria Reinhardt, Amélia Simões Figueiredo, Manuel Luís Capelas, Zaida Charepe, and Sérgio Deodato. 2020. "Experiences of Homeless Families in Parenthood: A Systematic Review and Synthesis of Qualitative Evidence" International Journal of Environmental Research and Public Health 17, no. 8: 2712. https://doi.org/10.3390/ijerph17082712
APA StyleAndrade, F. M. R., Simões Figueiredo, A., Capelas, M. L., Charepe, Z., & Deodato, S. (2020). Experiences of Homeless Families in Parenthood: A Systematic Review and Synthesis of Qualitative Evidence. International Journal of Environmental Research and Public Health, 17(8), 2712. https://doi.org/10.3390/ijerph17082712