1. Introduction
Animal Assisted Interventions (AAIs) comprise a broad array of planned activities that involve animals for the purpose of improving human health and wellness. AAIs involve activities with teams of humans and animals with the aim of achieving therapeutic (Animal Assisted Therapy; AAT) or educational (Animal Assisted Education; AAE) goals. The AAIs also include Animal-Assisted Activities (AAA), such as informal interactions/visitations conducted on a volunteer basis by those teams for motivational, educational, or recreational purposes [
1]. AATs provide well-being, promote the health of the patients [
2], and assist in cognitive, emotional–affective, social, and linguistic rehabilitation [
3,
4,
5,
6].
In particular, results of several studies mainly involving dogs indicate significant benefits of AAT in people with psychophysical and mental health disorders, such as adults with Autism Spectrum Disorder [
7], as well as Alzheimer disease and other dementias [
6,
8,
9], and also during psychotherapy for adolescents [
10]. As reported by Serpell and colleagues [
11], various animal species are used in AAIs, but the dog is the most widely used species, especially in the AAT and in the AAA [
3,
12,
13]. In AAT and AAA, patients interact with dogs by inter-specific relationship activities involving as petting, physical contact, brushing, playing, and strolling with the dog. Shen et al. [
12] demonstrated that bodily contact may contribute significantly to AAT effectiveness. On the other hand, during these activities, the patients (often very young or old, or immunocompromised) may have physical contact with the dog’s mucosae and fur, and can be exposed to the bacteria, fungi, and parasites sub-clinically carried by the dog [
14,
15,
16]. Therefore, a conflict exists between the need to preserve bodily contact during AAT and AAA, while reducing the risk of transmission of zoonotic agents.
As reported in scientific literature, different bacterial species can be carried by the dog and transmitted to humans [
17,
18,
19,
20,
21,
22].
ESKAPE bacteria (i.e.,
Enterococcus faecium,
Staphylococcus aureus,
Klebsiella pneumoniae,
Acinetobacter baumannii,
Pseudomonas aeruginosa, and
Enterobacter species) are a group of common opportunistic pathogens associated mainly with nosocomial infections [
23]. The acronym ESKAPE was used for the first time in 2008 by Rice [
23] and was coined to reflect these microorganism’s ability to escape killing by antibiotics by developing antimicrobial resistance, and challenge eradication by conventional therapies. The ESKAPE group of bacteria cause significant morbidity and mortality and increased resource utilization in healthcare facilities [
24,
25]. Moreover, World Health Organization (WHO) has recently listed most ESKAPE bacteria in the list of 12 microorganism against which new antibiotics are urgently needed [
26].
Enterococcus faecium is commensal microorganism of the normal gastrointestinal flora in humans and animals.
E. faecium can be transmitted to humans via direct contact with livestock as well as companion animals [
27]. Recently, the results of some studies highlighted the potential for zoonotic transmission of ampicillin- and vancomycin-resistant
E. faecium from the dog [
27,
28,
29,
30].
Staphylococcus aureus is part of the cutaneous microbiome of animals and humans and is one of the leading causes of fatal nosocomial infection in humans [
31]. It can cause a range of infections, such as mild-to severe skin and soft tissue infections, endocarditis, osteomyelitis, and fatal pneumonia [
32]. According to the sensitivity to antibiotic drugs,
S. aureus can be divided into methicillin-sensitive
Staphylococcus aureus (MSSA) and methicillin-resistant
Staphylococcus aureus (MRSA). MRSA is one of the most significant bacteria causing both hospital and community-acquired infections in humans [
17].
K. pneumoniae is Gram-negative member of the Enterobacteriaceae, considered one of the common opportunistic agents causing respiratory and urinary tract infections in humans and dogs [
33,
34,
35,
36,
37].
K. pneumoniae strains have a significant ability to acquire resistance to antibiotics, and as such, it is of a public health concern. [
38]. Marques and colleagues [
35] reported the fecal colonization and sharing of
K. pneumoniae clonal lineages between healthy humans and dogs living in close contact, suggesting the role of dogs as reservoirs of this bacterium.
A. baumannii is the most clinically significant pathogen implicated in human nosocomial infections [
39]. In humans,
A. baumannii infections involve mainly the respiratory tract, but meningitis and urinary tract infections may also occur [
40,
41,
42]. Animals represent a potential reservoir of
A. baumannii, and the risk of transmission could increase in companion animals which are in direct contact or closer vicinity to humans [
43].
P. aeruginosa is increasingly recognized as an opportunistic pathogen causing chronic and recurrent infections in both humans and animals [
44]. In humans, it causes nosocomial and healthcare-associated infections in immunocompromised patients [
45,
46]. Fernandes and colleagues [
47] demonstrated a zoo-anthroponotic transmission (human–to-dog) of VIM-2–producing
P. aeruginosa in the household following a person’s hospital discharge.
Enterobacter spp., particularly
E. aerogenes and
E. cloacae, have been associated with nosocomial foci and are considered opportunistic pathogens [
48].
Enterobacter spp. can cause numerous types of infections, including brain abscess, pneumonia, meningitis, septicemia, urinary tract (especially catheter-related) infections, and intestinal infections [
49]. Transmission occurs through direct or indirect contact of the mucosal surfaces with the host organism [
50].
There are few reports concerning the risks related to infections with ESKAPE bacteria in the contexts of AAIs, particularly in the AAT, and in the AAA in healthcare facilities. Therefore, the present review and meta-analysis aims at analyzing the published data on the presence of ESKAPE bacteria in the dog, in order to assess the risk of zoonotic transmission in these contexts. By our study, we intend to make an indirect assessment of the zoonotic risk deriving from contact with the dog, assuming its role as a healthy and/or asymptomatic carrier of ESKAPE bacteria in AAIs, but in particular in AAT context and in the AAA in healthcare facilities.
4. Discussion
Our work aimed to systematically review data on the presence of pathogens bacteria ESKAPE in dogs, within the period of 2000 to 2019, focusing on the presence, percentage estimates, type of samples such as swabs and biological samples (i.e., feces, urines), dog category, and geographic distribution of the study (country and continent). The choice of the factors mentioned above and reported in the respective tables is related to the possibility of zoonotic transmission of the bacteria of the ESKAPE group from the dog to the human during AAT and AAA in health context. In particular, considering the great recent attention to these bacteria causing of nosocomial death by their characteristics of antibiotic resistance [
110], the articles indexed and published in the last twenty years have been considered; the type of sample performed from the dog was highlighted to assess not only the variety of tropism of these bacteria but also to make a prediction of the body regions (of the dog) at risk of contamination and with which the patients/users involved make contact directly or indirectly; in our opinion, it was also noteworthy to consider the category of belonging of the dog (owned and non-owned) since the dogs that are involved in the AAIs, and in particular in the AAT, are owned dogs [
5,
6,
111,
112]. Finally, we also considered it appropriate to consider the geographical distribution of the studies obtained in order to have an overview of the interest of researchers in this topic and considering that AAIs are now widespread all over the world, especially in industrialized countries [
113,
114,
115].
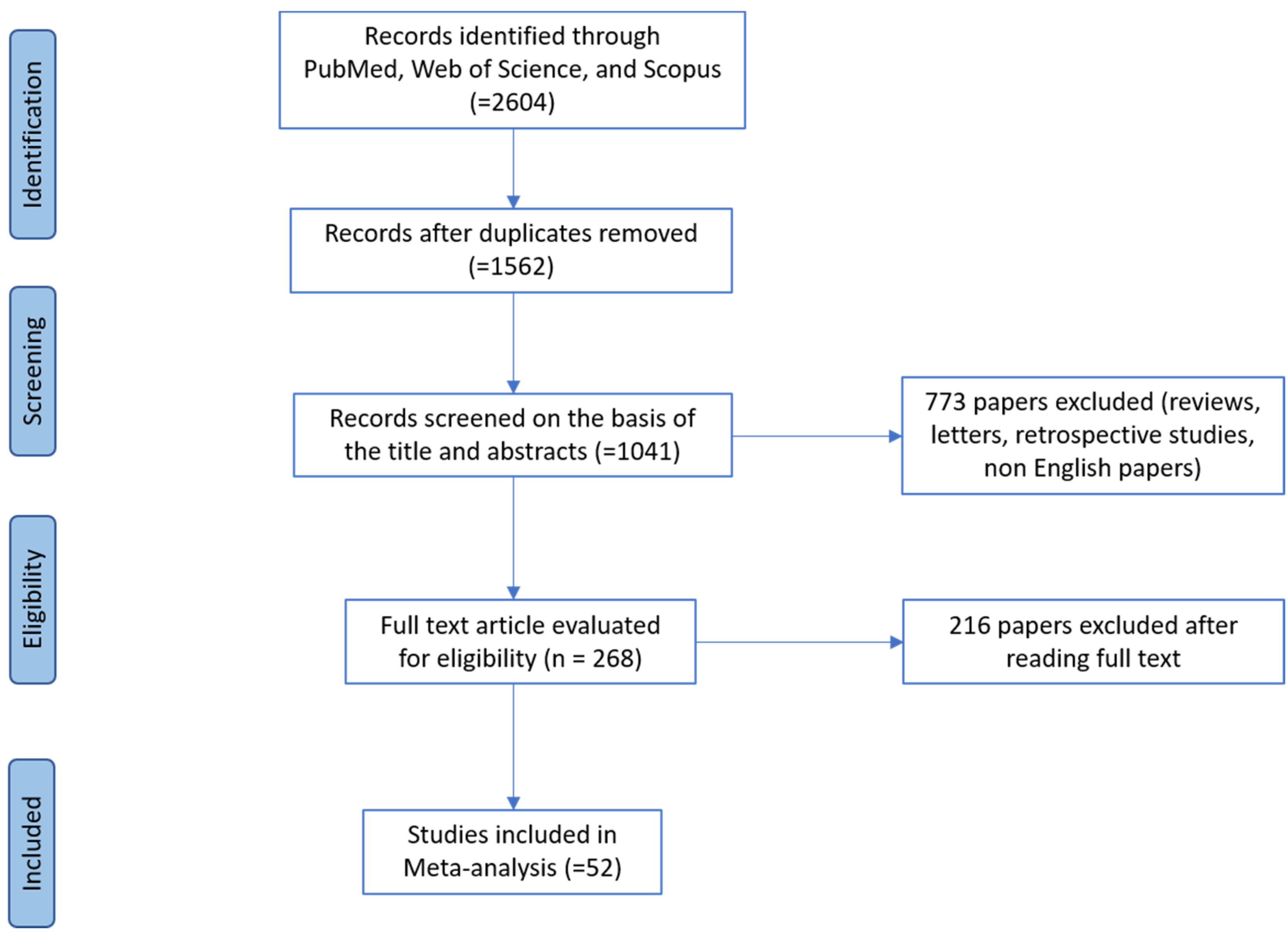
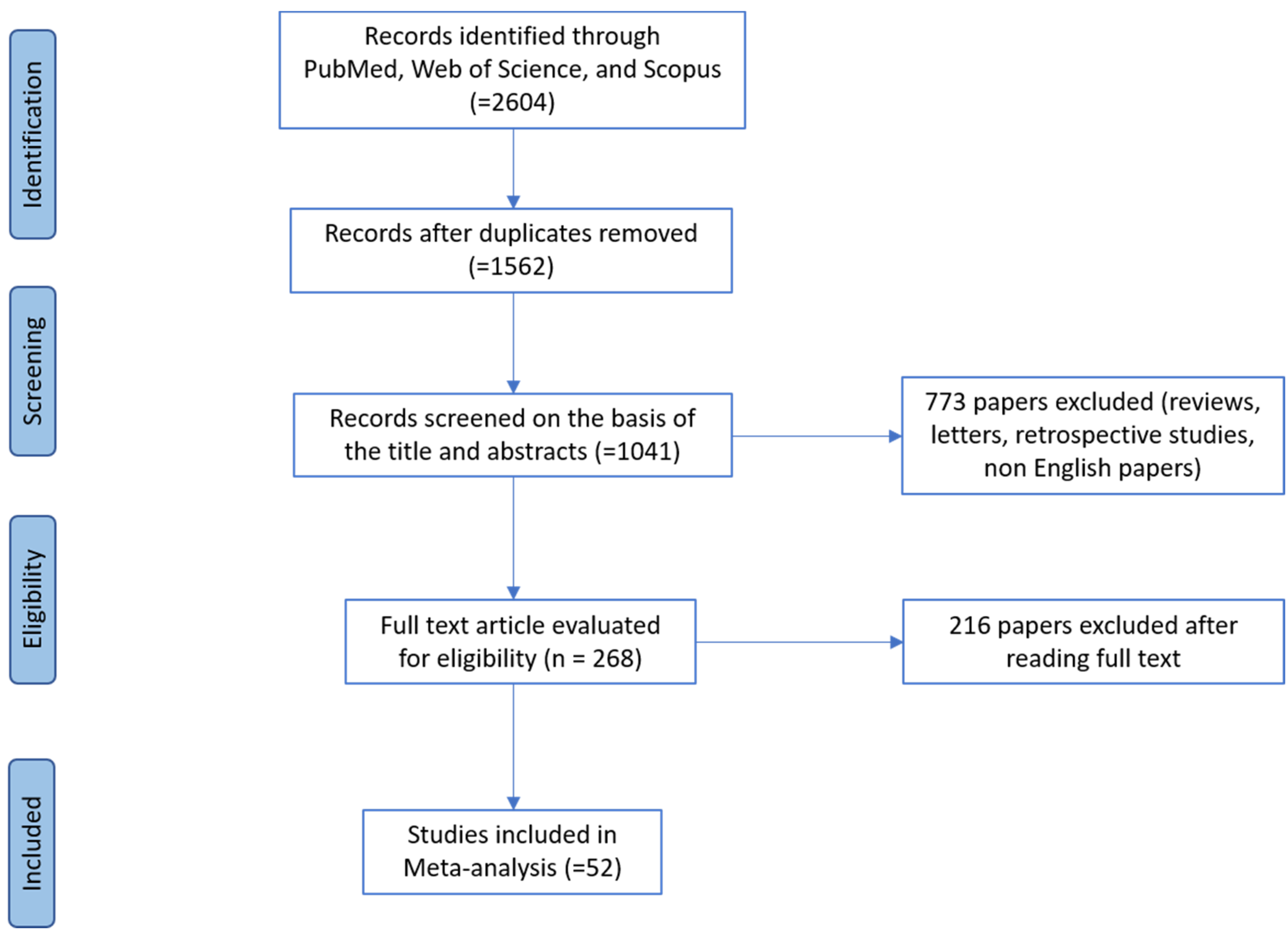
Our online search returned 52 papers published in different countries of the five Continents considered later of appropriate quality to provide useful data to evaluate the presence of these bacteria in the dogs. The geographical distribution of studies regarding ESKAPE bacteria group in the dog, in the present study is shown in the respective table to each bacterium.
As previously reported, we have considered the papers related to the presence of these bacteria in dogs since there is a large correlated lack in the control of dogs involved in AAT. In fact, this type of non-pharmacological therapy is carried out in settings such as hospitals or healthcare facilities and is often aimed at patients belonging to risk categories (e.g., dialysis patients, hospitalized patients, and immunosuppressed or immunocompromised patients) [
5,
116].
Despite the proven risk of these nosocomial opportunistic bacteria and the numerous investigations carried out both in the medical and veterinary fields, the studies concerning the dog involved in AAT and AAA in health context are very small. Particularly, the bacteria belonging to the MRSA group, together with
E. faecium, represent the most studied bacteria of the ESKAPE group in the dog and mentioned in the
Guidelines of the American Journal of Infection Control defined by Lefebvre and colleagues in 2008 [
19], as well as in other scientific contributions published in international and national journals [
117,
118,
119,
120]. The lack of standardized control programs of ESKAPE in the dogs involved in AAT at the international level and in worldwide introduces a knowledge gap and makes it difficult to estimate related risk level for humans and thoroughly investigate transmission potential dynamics of these pathogens.
4.1. Enterococcus faecium
As reported by Bang and colleagues [
27] Enterococci can be transmitted to humans via direct contact with animals. Moreover, as reported by Cinquepalmi and colleagues [
70], the contact between pets and their owners is closer than in the past, therefore, contamination of urban roads with dog feces containing multidrug-resistant microorganisms is also a problem for public and environmental health. In our study, a total of 16 studies have been returned on the
E. faecium presence in dogs but none have been carried out regarding the dogs involved in the AAIs or particularly in AAT and AAA in health context. Furthermore, as reported by Lefebvre and colleagues [
19], dogs involved in AAIs should undergo health checks for resistant
E. faecium as they can play a role in the spread of this nosocomial pathogen. The first report regarding the presence of
E. faecium vancomycin resistant in dogs was made in 2002 by Simjee and colleagues [
75] and the studies of other researchers have resumed with greater intensity since 2014. Recently, some studies were performed to highlight the transmission of
E. faecium ampicillin- and vancomycin-resistant from the dog to humans [
27,
28,
29,
30,
73]. Differently, Rodrigues and colleagues [
74] as well as Kataoka and colleagues [
68] showed that the strains of
E. faecium isolated in their studies were resistant to many antibiotics but not to vancomycin, indicating that the risk of transmission of these strains to humans or the transfer of their resistance genes to others is limited bacteria belonging to the endogenous flora of the human. Almost all the studies included in this Review-Metanalysis isolated bacteria from feces [
27,
28,
29,
30] or rectal [
65,
66], oral [
67], and different swabs were performed in remaining studies [
69,
72]. Interestingly, more recent studies have reconfirmed the dog’s status as a carrier of
E. faecium but have also demonstrated its horizontal transfer to humans through contact and licking. Healthy livestock and pets can harbor enterococcal pathogens that can be transferred through the food chain, as well as through close associations such as embracing and licking humans [
66]. Previously, the study by Jackson and colleagues [
72] performed rectal and skin swabs, signaling the presence of
E. faecium not only in the former but also in the neighboring regions of the abdomen and rear train. Furthermore, dogs (and cats) can act as reserves of antimicrobial resistance genes that can be transferred from pets to people [
72]. Multi-drug resistant
E. faecium has been isolated and identified from dogs with urinary tract infections supporting the hypothesis that enterococci are a true uropathogen and not just an opportunistic organism [
64]. Finally, dogs are frequent carriers of CC17-related lineages and can play a role in the spread of this nosocomial pathogen [
71].
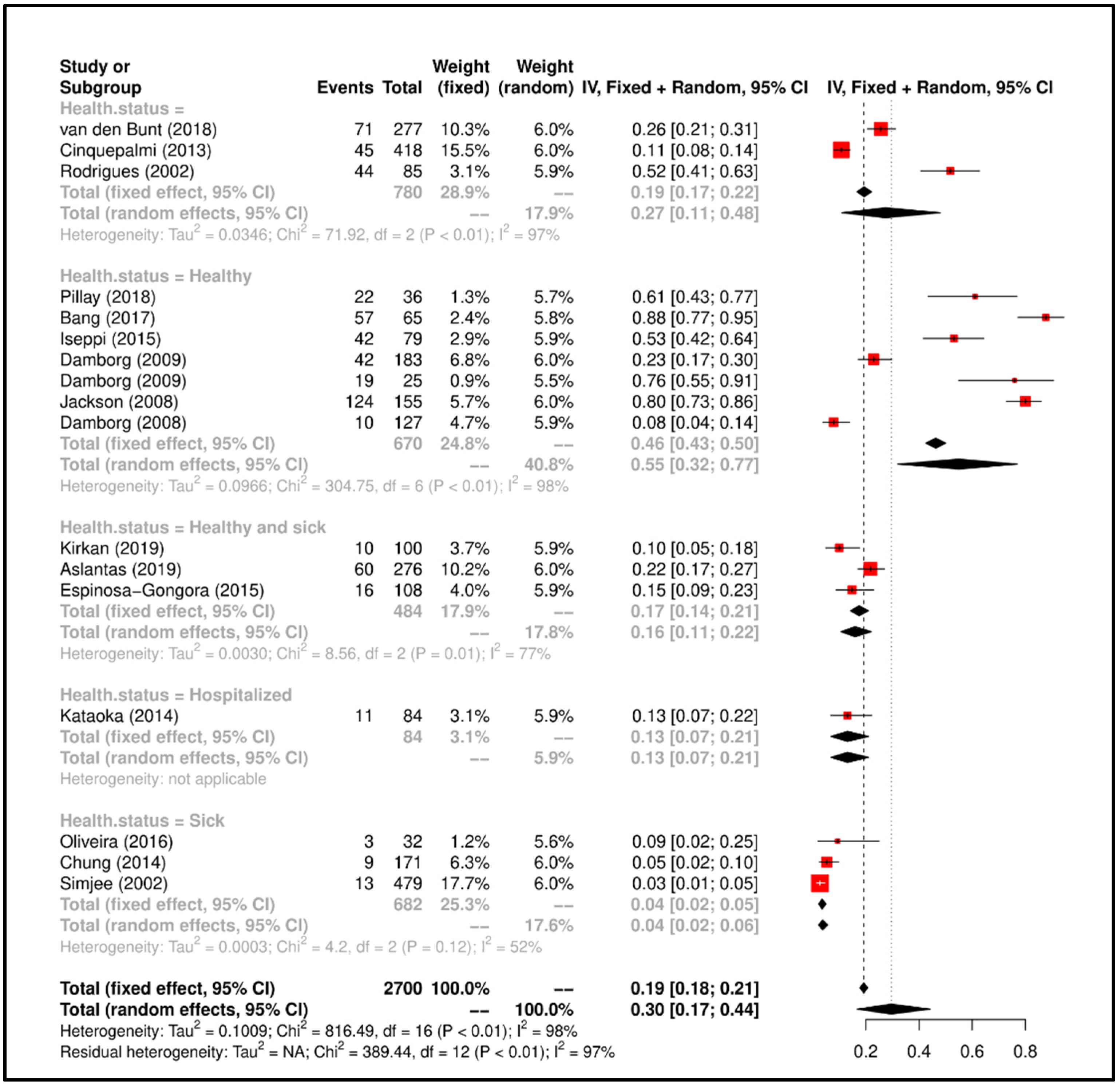
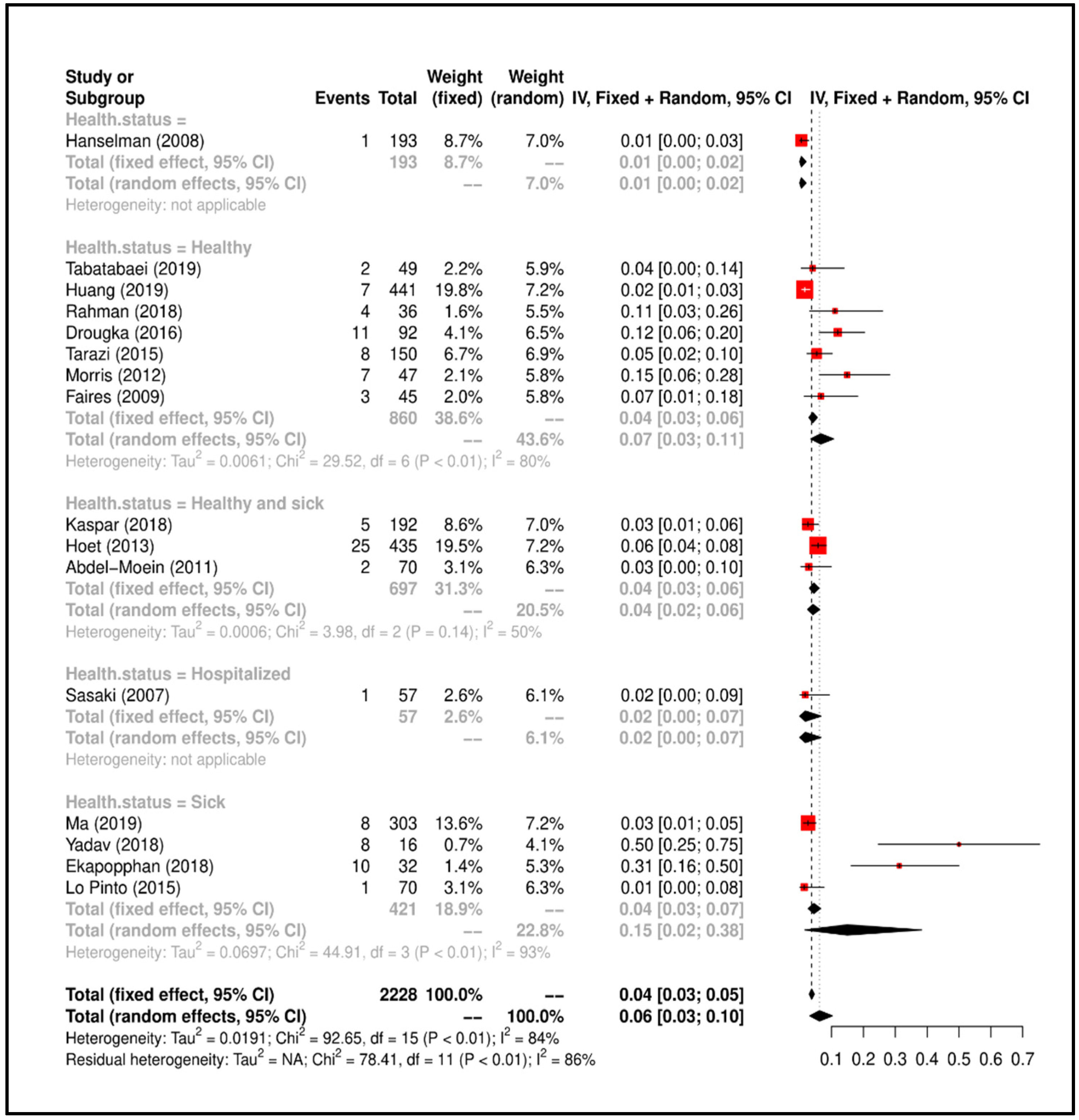
Finally, based on the different clinical conditions of the dogs sampled in the papers included in this paper, also from the results of the Metanalysis it emerges that there is a greater prevalence of studies involving healthy [
27,
30,
66,
71,
72,
73] and “healthy and sick” dogs [
29,
64,
65]. Therefore, in line with what reported by the American Guidelines [
19], it should be mandatory to perform the microbiological control of the dog in the AAT and in the AAA in health context, avoiding the possible risk of transmission of
E. faecium.
4.2. Staphylococcus aureus
Animal-to-human MRSA infection appears to be more evident in immunocompromised patients [
17]. The bacteria belonging to the MRSA group, together with
E. faecium, represent the bacteria of the ESKAPE group most studied in the dog and mentioned in the already mentioned Guidelines of the
American Journal of Infection Control defined by Lefebvre and colleagues [
19], but also in other scientific contributions published in international and national journals. While very few papers emphasize the need to monitor the presence of this bacterium in dogs involved in AAIs [
117,
118,
119,
120]. In line with the elective tropism of the staphylococci for the mucous membranes of the upper respiratory tract and for the skin, six studies were conducted on nasal swabs, six on nasal and perineal swabs, two on eye lesions, skin and pyogenic lesions, and one on ear swabs. It is interesting to note that inter-species transmission has been evaluated in all included studies not only from dog to human but also between the dog, farm animals and humans. In this regard, it is very interesting to underline the study by Lo Pinto and colleagues [
84], in which the authors highlight the zoonotic risk for dogs of having a four times higher probability of contracting staphylococcal keratitis if belonging to people employed in veterinary work. Moreover, Hoet and colleagues [
86] suggest that the owner’s profession was significantly associated, and the dogs owned by veterinarian students had a 20.5-fold probability (95% CI 4.5−93.6;
p-value = 0.01) more likely to be MRSA positive compared to dogs owned by customers with different professions. The 2018 studies of Yadav and colleagues [
79], Rahman and colleagues [
80], and Kaspar and colleagues [
81] highlighted the potential risk of transmission of MRSA strains from farm animals to dogs, highlighting how, again, the latter act as healthy and asymptomatic carriers of MRSA strains. In addition, the studies by Morris and colleagues [
87] and Faires and colleagues [
89] in which the possibility of colonization of dogs when sharing the domestic space with people or other animals with MRSA infection is evaluated.
Tabatabaei and colleagues [
76] showed that pets and veterinarians could be potential sources of multidrug-resistant methicillin
S. aureus (and multidrug-resistant methicillin
S. pseudintermedius) in Iran. Ma and colleagues [
77] carried out an epidemiological survey on dogs (and cats) showing a prevalence of MRSA equal to 2.6%. Dogs had a statistically more significant probability of carrying positive coagulase staphylococci than cats (
p < 0.001). This study highlights important differences in the diversity and transport patterns of commensal staphylococci between dogs and cats in Australia. Huang and colleagues [
78] carried out a study on the prevalence and characteristics of MRSA isolated from animals in shelter in Taiwan. The MRSA strains isolated in this study were like those already isolated from the human population in the past, indicating potential public health risks. Yadav and colleagues [
79] carried out their study in India, evaluating the presence of MRSA in different animal species (cattle, buffalo, and dogs). In their article, eight strains of MRSA that exhibited methicillin resistance and possessed the
mecA gene were isolated from dogs. It is interesting to note that the study by Kaspar and colleagues [
81] highlighted the presence in the dog of the MRSA lineages typically described for cattle, underlining the impact of the spread of multi-drug resistant microorganisms. Drougka and colleagues [
83], through the comparison between genetic markers, have shown that identical or very similar strains of MRSA spread between animals and veterinary staff. Pets harbor Panton-Valentine leukocidin (PVL) positive clones which are a possible source for transmission to humans. Tarazi and colleagues [
85] found a strong association between the isolated strains of MRSA from dogs and those of humans that are in close contact with them (breeding centers and associated staff).
Pets can host pandemic strains of MRSA while residing in a family with an infected person. However, the source of MRSA for the animal cannot always be attributed to the human patient [
87]. The presence of MRSA in apparently healthy and/or sick dogs makes it an emerging veterinary pathogen that could be considered a public health burden if widespread in our community outside hospitals [
88]. Faires and colleagues [
89] underlined the high prevalence of concomitant colonization of MRSA, and the identification of indistinguishable strains in humans and dogs (and cats) of the same family, suggesting the possible inter-species transmission of MRSA. Although the prevalence of colonization of these methicillin-resistant strains (
S. pseudintermedius,
S. aureus and
S. schleiferi subsp.
coagulans) was low, the combined prevalence of 3.1% can be a source of concern for both animal health and the public one [
90].
At last, based on the health status of the dogs sampled in the papers included in our work and also from the results of the Metanalysis, it emerges that there is a greater prevalence of studies involving healthy [
76,
78,
80,
83,
85,
87,
89] and “healthy and sick” dogs [
81,
86,
88]. Therefore, consistently with what reported by the
American Guidelines [
19] and by the scientific contribution of other Authors [
15,
17,
20], it should be mandatory to perform the microbiological control of the dog involved in the AAT and in the AAA in health context, to avoid the possible risk of transmission of these bacteria.
4.3. Klebsiella pneumoniae
Recently, the World Health Organization (WHO) published a global priority list of antibiotic-resistant bacteria and
K. pneumoniae have been included in the “Priority 1: Critical” group (third-generation cephalosporin (3GC)-and/ or carbapenem-resistant Enterobacteriaceae) [
26]. Marques and colleagues [
36] reported the fecal colonization and sharing of
K. pneumoniae clonal lineages between healthy humans and dogs living in close contact, suggesting the role of dogs as reservoirs of this bacterium, even though those strains were neither multidrug resistant nor hypervirulent.
The analyzed studies are uniformly distributed with regards to the sampling between rectal swabs, urinary and fecal samples, in line with the known enteric and urinary K. pneumoniae tropism, particularly in dogs.
The results of the study by Hong and colleagues [
92] indicate the transmission and direct spread of extended-spectrum cephalosporin (ESC)-resistant Enterobacteriaceae, such as
K. pneumoniae, between humans and pets. Zhang and colleagues [
93] support the hypothesis of transfer of resistant bacteria between man and dog, since CTX-M-1 has been frequently found in fecal dog Enterobacteriaceae, while it is still rare in human Enterobacteriaceae in Canada, therefore suggesting the transfer of bacteria resistant to dogs from farm animals or other sources. Chanchaithong and colleagues [
94] showed the high percentage of drug resistance among
K. pneumoniae isolates, underlining that in the clinical practice of small animals’ routine detection of Extended-Spectrum Beta-Lactamase (ESBL)-producing bacteria is necessary, using reliable laboratory methods. The data shown by Liu and colleagues [
34] highlight the alarming resistance to beta-lactamase in
Klebsiella (and
Enterobacter) species of canine origin in India, emphasizing them as indicators of antimicrobial resistance. Sharif and colleagues [
95] emphasize the need for active surveillance studies on pets that live very close to humans, since inter-species transmission can occur within the same family. Gonzales-Torralba and colleagues [
96] reported the first report concerning the isolation of bacteria that produce OXA-48 from pets. In particular, the clonal nature of
K. pneumoniae would suggest nosocomial diffusion rather than repeated introduction by individual patients into the clinic. Abdel-Moein and colleagues [
97] highlight the risk of transmission of
K. pneumoniae infections, via the oro-fecal route, which could occur after handling infected pets or using contaminated objects within families.
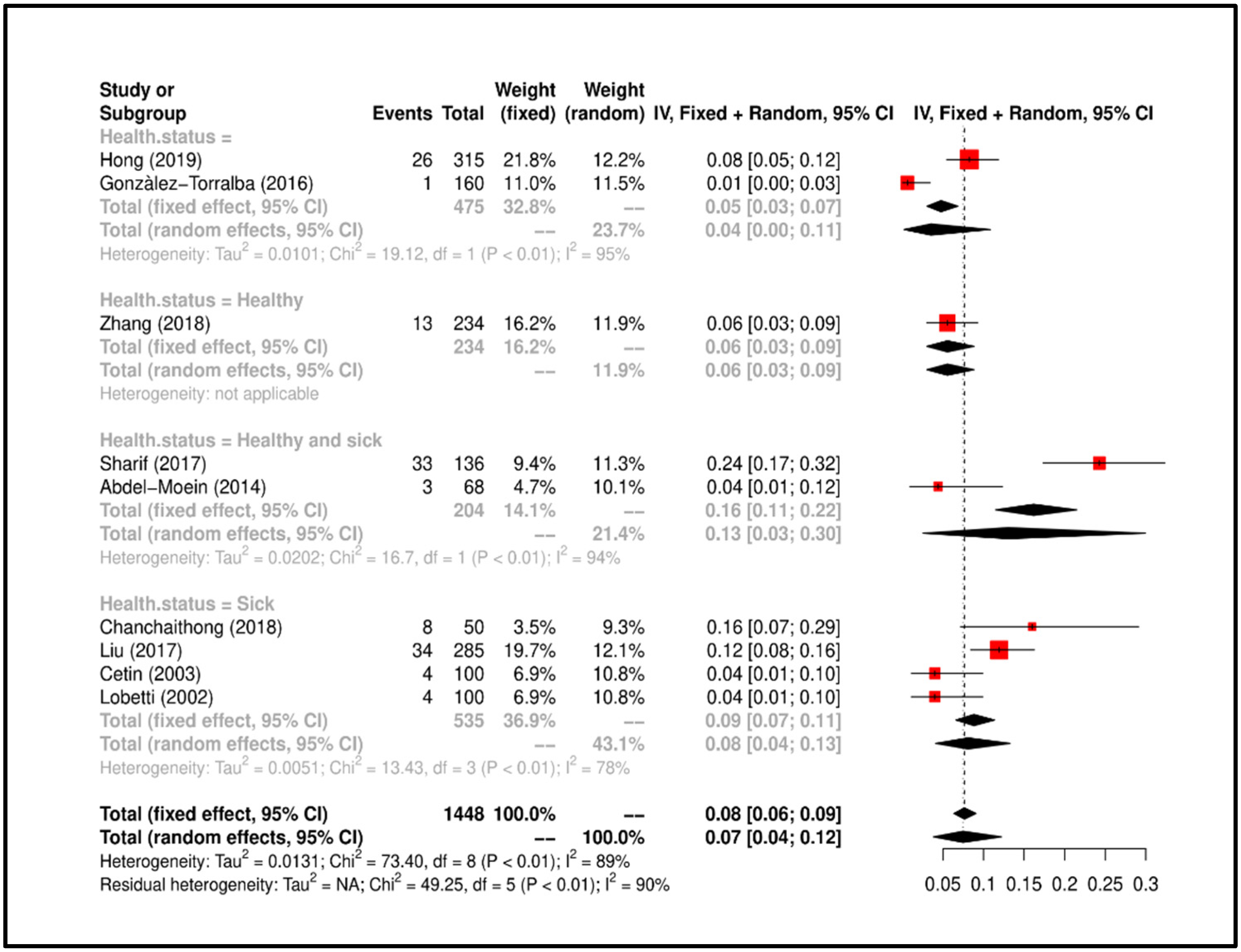
From the data of the papers included in this work and from the results of the Meta-analysis, if on the one hand it emerged that the sampled dogs were mainly sick subjects [
34,
94,
98,
99]; on the other hand in two studies [
95,
97], both “healthy and sick” dogs were sampled. Instead, Zhang and colleagues [
93] showed the presence of
K. pneumoniae in healthy dogs. These findings additionally elucidate the need to perform the microbiological control of the dogs involved in the AAT and in the AAA in health context, avoiding the possible risk of transmission of this bacterium and contamination even in the home context.
4.4. Acinetobacter baumannii
Animals represent a potential reservoir of
A. baumannii and can contribute to the dissemination of new emerging carbapenemases. The risk of transmission could increase in companion animals which are in more direct contact and closer vicinity with humans and are more prone to transfer or acquire
A. baumannii [
43]. In addition,
A. baumanni has also been identified on the skin and in feces of healthy dogs [
100,
101]. The studies concerning the presence of
A. baumannii denote the fairly recent attention towards this species/bacterial group (from 2014 to 2018) and despite the elective tropism of
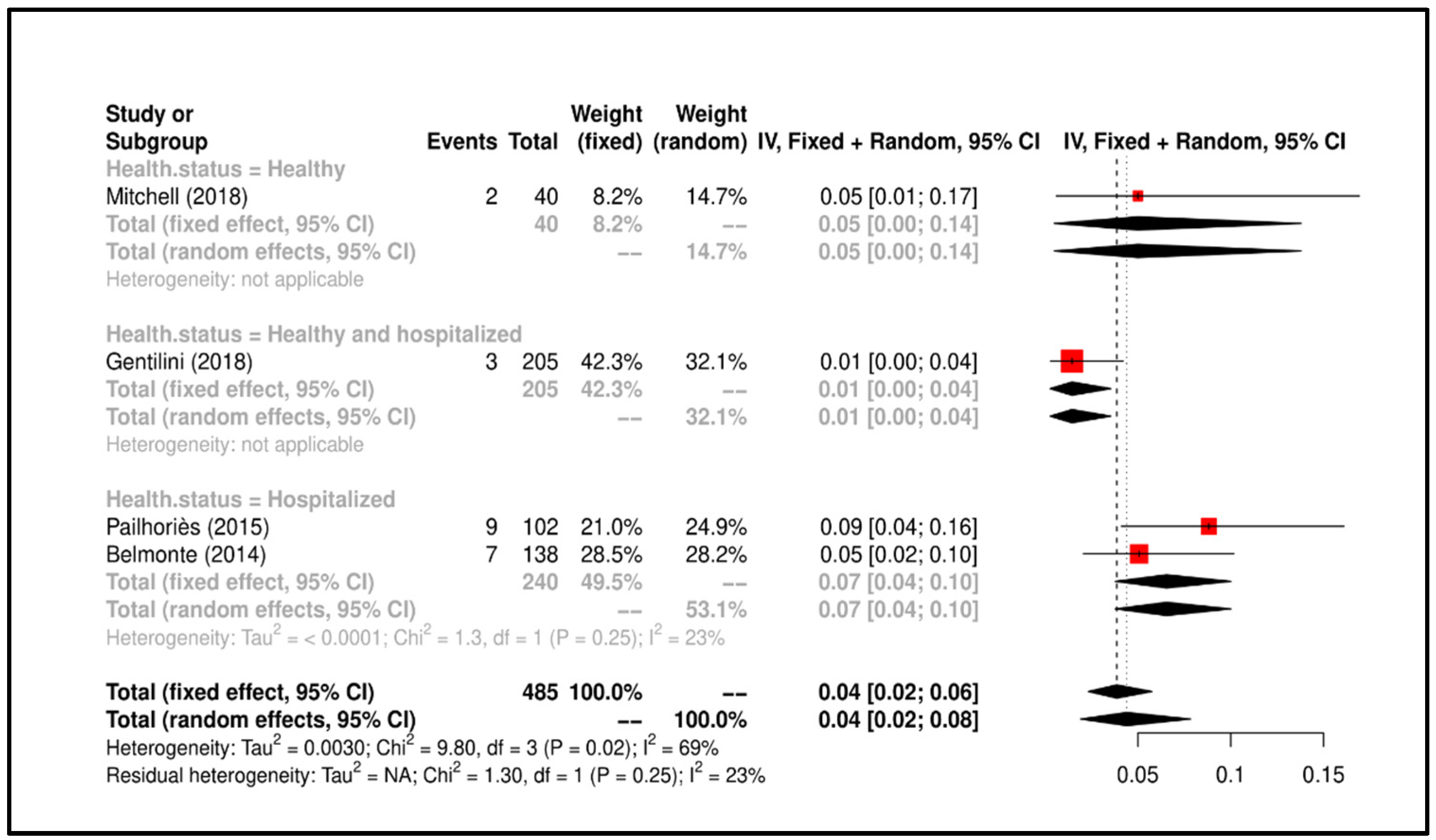
A. baumanni for the digestive system, heterogeneity of the samples taken (feces, rectal, oral, and skin swabs) was reported. Particularly, to be noted as all the studies indicated above were carried out in the context of veterinary hospitals or veterinary clinics. More specifically, Gentilini and colleagues [
100] estimated the risk of colonization by Gram-negative, non-fermenting carbapenem-resistant bacteria in pets admitted to veterinary tertiary care centers, highlighting their potential role in the diffusion of resistance genes between animals and humans. The study reported by Mitchell and colleagues [
100] showed that
Acinetobacter spp. they can survive on the skin of dogs, which can become potential reservoirs of infection. Pailhoriès and coll. [
102] have shown that
A. baumannii strains are present in non-hospital settings on Reunion Island but Previously, Belmonte and colleagues [
103] had assessed already the presence of
A. baumannii in pets (dogs and cats) hospitalized in nine veterinary clinics on Reunion Island.
There are very few articles found in the literature and included in our work, therefore it is not scientifically correct to make conclusive statements on the risk of the transmission of
A. baumannii from dog to man. Considering this, we can only emphasize that the dogs sampled in the study of Mitchell et at. [
101] were healthy and that skin swabs had been performed, emphasizing the need to carefully monitor the dogs involved in AAT and AAA in the health context, considering the frequent contact that occurs in the respective settings.
4.5. Pseudomonas aeruginosa
In animals, particularly in dogs and cats,
P. aeruginosa causes otitis external/media, corneal ulcers, urinary tract infection, and pyoderma [
82,
98,
104]. However, only a few studies have highlighted the potential risk from contact with dogs infected with
P. aeruginosa. In this regard, only Lefebvre and colleagues [
20] have evaluated the presence of this bacterium in dogs visiting hospitalized people, while very few other studies have considered human–dog–environment transmission in the veterinary facilities, such as hospital and clinics [
46,
47,
82].
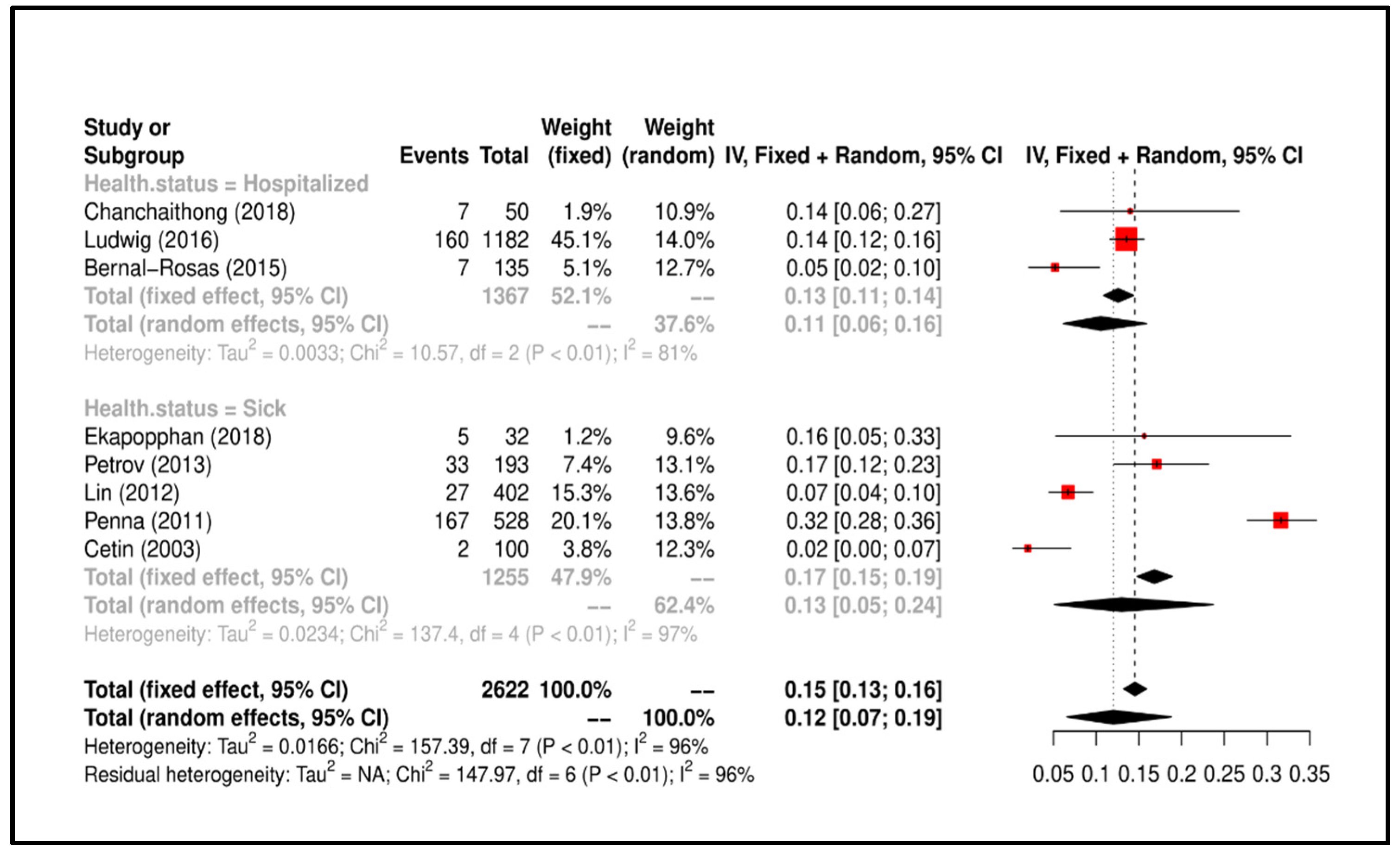
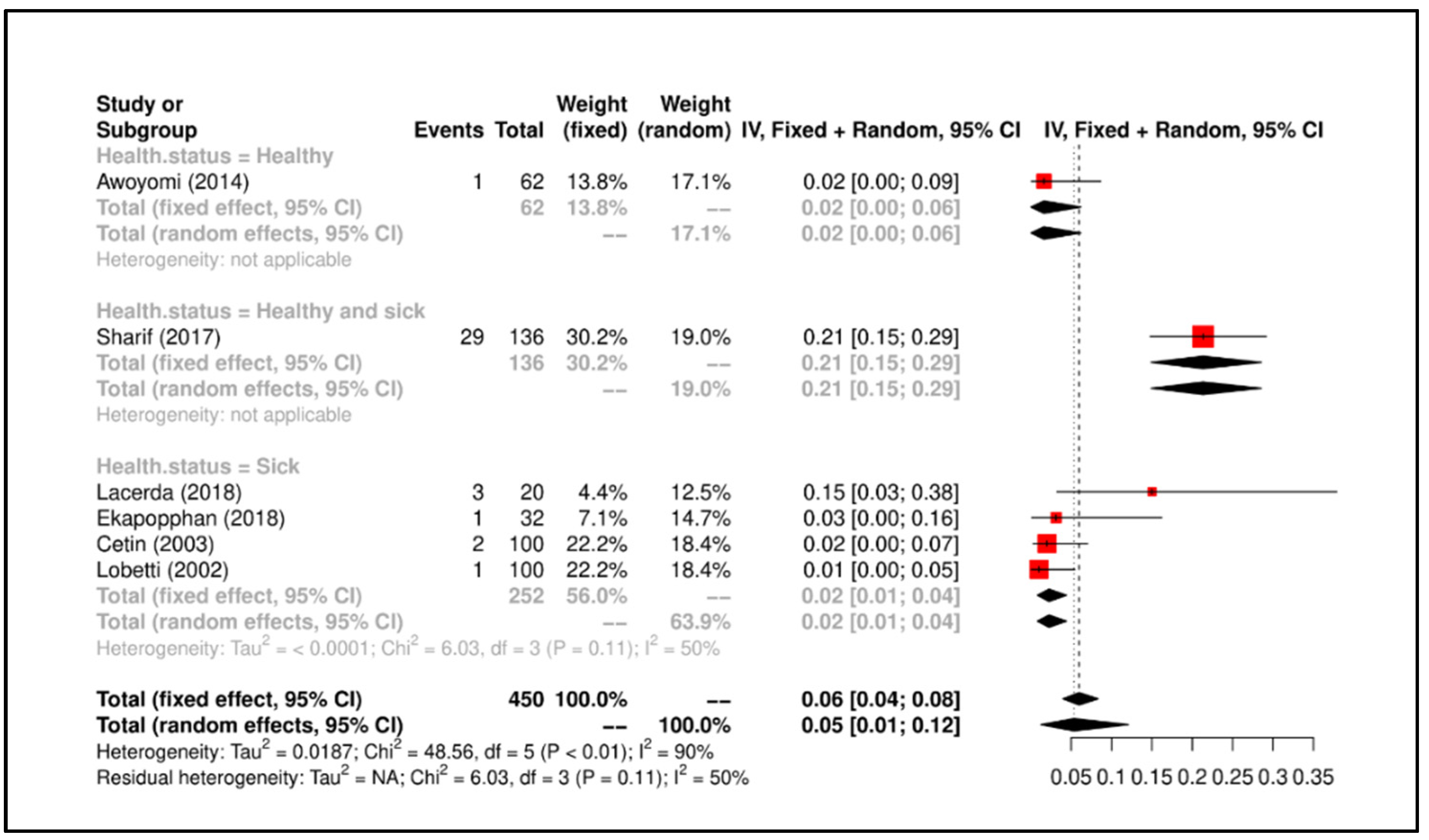
The studies included in this Review-Metanalysis start from 2003 by Cetin and colleagues [
98] (these authors conducted a multi-bacterial study also assessing the presence of
K. pneumoniae and
Enterobacter spp.) to arrive at 2018 with the paper by Ekapopphan and colleagues [
82], (these authors also conducted a multi-bacterial study also evaluating the presence of MRSA and
Enterobacter spp.). None of the studies included evaluated the presence of resistant
P. aeruginosa in dogs involved in AAI. For the purposes of our investigation, highlighting the risk resulting from contact with certain body regions, the data reported by Penna and colleagues [
107], which indicates the presence of
P. aeruginosa in cases of canine external otitis and the data reported by Ludwig and colleagues [
104] which indicates the presence of the bacterium in soft tissues, skin, and superficial wounds. As observed in human hospitals,
P. aeruginosa acts as one of the multi-resistant microorganisms of veterinary clinical relevance [
105]. Note the study by Lin and colleagues [
46] on the antimicrobial resistance profiles of
P. aeruginosa strains of canine origin in China, as it represents the first report of the oxacillin
bla-OXA-31 resistance gene of this bacterium in a canine isolate.
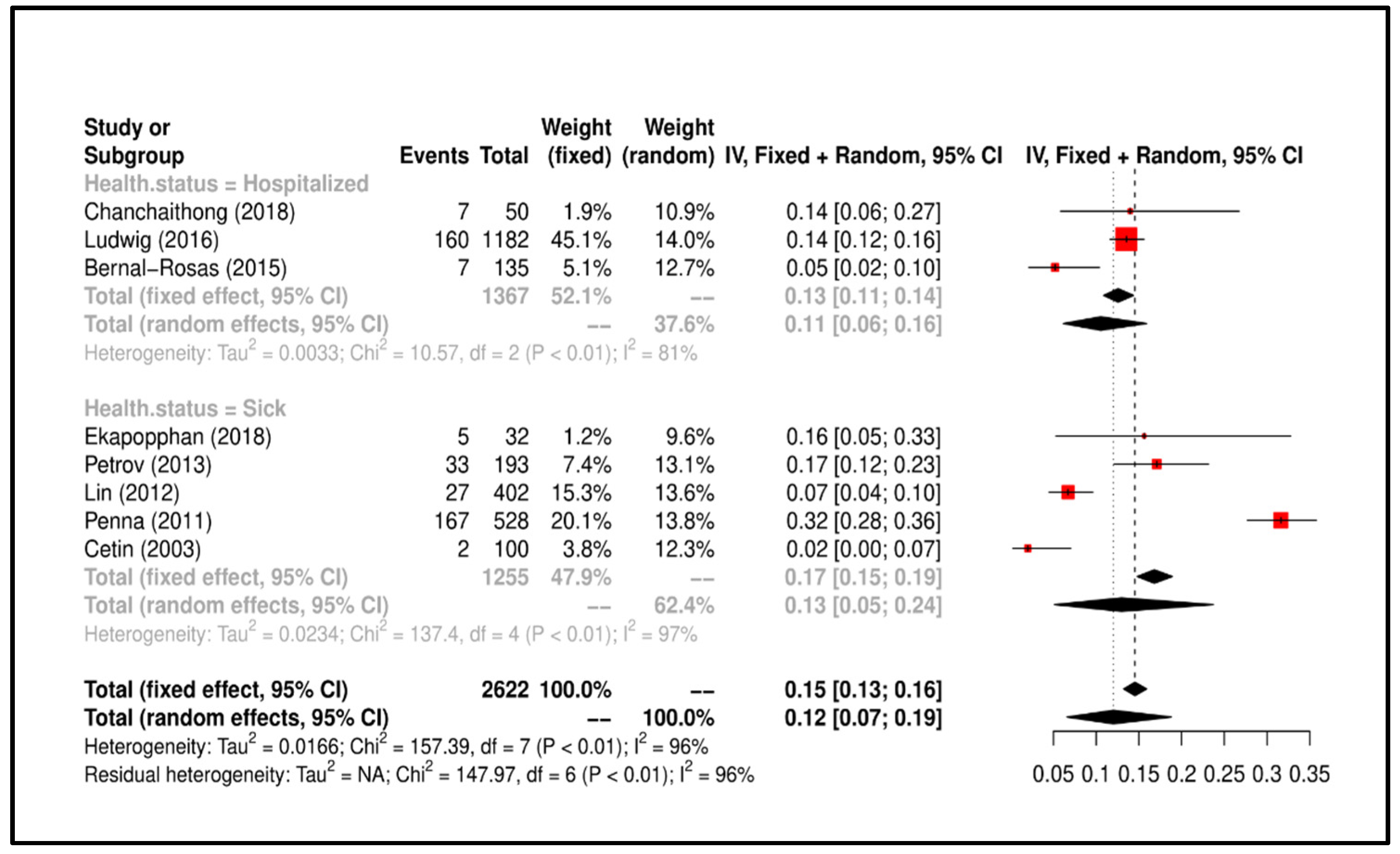
From the data that emerged in our study, it appears clearly that P. aeruginosa causes urinary and auricular symptoms and infects soft tissues. In fact, all the included studies sampled sick or hospitalized dogs. Therefore, the risk of transmission to humans is mainly due to contact with symptomatic dogs but this does not exclude that there may be asymptomatic or reservoir dogs of this bacterium as a commensal of the urinary tract or ear.
4.6. Enterobacter spp.
Enterobacter spp. have been observed in device-related intravascular infections and surgical site infections (mainly postoperative or related to devices such as biliary stents). Transmission occurs through direct or indirect contact of the mucosal surfaces with the infectious agent (e.g., transfer from contaminated hands to contaminated neonatal units or urinals) or, in the case of endogenous flora, through transfer to adjacent body sites sensitive and sterile [
48,
49,
50].
Few papers are present in the literature reporting epidemiological investigation data on the presence of
Enterobacter spp. in dogs, and they considered its presence mainly in urine samples [
94], intravenous catheters [
99], ocular [
82,
108], oral [
109], and rectal [
95] swabs.
In 2003, Cetin and colleagues [
98] were the first to report the presence of
Enterobacter spp., in association with other bacterial species, in dogs with urinary problems. These authors conducted a multi-bacterial study evaluating the presence of
K. pneumoniae and
P. aeruginosa. The attention, after about 10 years of silence, was then directed to other body regions such as the oral cavity [
109], the rectum [
95], to get to the most recent studies of Ekapopphan and colleagues [
82] and Lacerda and colleagues [
108], which reported the presence of
Enterobacter spp. in ocular swabs (cornea and conjunctiva). The alarming incidence of beta-lactamase resistance found in this study by Sharif and colleagues [
95], could probably be the result of the indiscriminate use of antibiotics in veterinary practice, which reflects the possible risk of therapeutic failures that can occur in the treatment of infections caused by
Enterobacter spp. Awoyomi and colleagues [
109] highlighted that the oral cavities of hunting dogs can carry multi-resistant bacteria, of significant importance for public health since they could be transferred to humans through contaminated hunting tools and bite wounds.
The few studies included in this Review-Metanalysis underline the need not to underestimate the potential transmission risk of bacteria belonging to the Enterobacter genus, since based on the antibiotic-resistance data that emerged and the genetic analyzes carried out, these bacteria can be transferred through the bite wounds and more generally through contact with the dog’s external mucous membranes.
Finally, from the results of the Metanalysis, the sampled dogs were mostly sick subjects [
82,
98,
99,
108] but Sharif et al. [
95] and Awoyomi et al. [
109] showed positivity results in “healthy and sick” dogs and in healthy dogs, respectively. It is interesting to note that all the subjects sampled in the six studies concerning
Enterobacter spp. included in this Review and Meta-analysis were dogs owned. Our results, also in this case, require reflection on the need to subject the dogs involved in the AAT and in the AAA in health context.
4.7. Potential Limitations of the Data
The notable lack of papers on the presence of ESKAPE bacteria in the dog involved in AAT at the international levels, as well as individual surveys poor representative, might have affected the true estimates of these zoonoses in individual countries, in the continents and across the world. This study did not utilized data from abstracts, posters, and conference proceedings but only full paper publications. Furthermore, the included studies showed a great heterogeneity regarding the number of dogs sampled and the respective percentages of positivity, as well as the samples taken; the isolation and identification methods of the individual bacteria were not considered; except for Staphylococcus aureus methicillin resistant, the inclusion of papers was made considering the resistance to antibiotics and not to specific antibiotic categories (ampicillin-, vancomycin-, β-lactam resistant).
5. Conclusions
Currently, there is moderate attention by researchers to the role of the dog as a vector of the bacteria of the ESKAPE group, the international scientific literature is still not very sensitive and is scarcely aimed at assessing the risk related to the presence of these bacteria in the dogs involved in the AAT and AAA in the health context. From the literature included in this work it emerges that the risk of dog–human zoonotic transmission (and vice versa) concerns all bacteria of the ESKAPE group, therefore the level of surveillance must include mandatory microbiological controls and strong rules of hygienic and behavioral management of the animal. In this regard, the continuous and constant health control of the animals involved in the AAIs, with particular reference to the dog, should be a priority. In fact, the close contact between human and pets determines the risk of zoonosis and creates opportunities for interspecies transmission of resistant bacteria [
121].
In this aim, in our opinion, it is more and more necessary to a One Health approach, which involves the collaboration between veterinarians, physicians, public health operators, and epidemiologists, in order to prevent the transmission of such bacteria and to attain optimal health for humans, animals, and the environment. The AAIs, particularly the AAT, and the AAA in the health context, represent a concrete example of One Health approach and require necessarily an inter-disciplinary approach as they involve different health professionals. These operators, each according to their skills, work in team for people’s health, for the control and protection also of the health and welfare of the animal involved, for the prevention and control of zoonotic diseases.
Furthermore, we hope to be able to encourage a discussion with international experts regarding the need to draw up standardized hygiene-health-behavioral monitoring protocols, aimed at producing health and behavioral certifications valid for all dogs that perform AAT and AAA in the health context.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}