Zumba®, Fat Mass and Maximum Oxygen Consumption: A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection and Eligibility Criteria
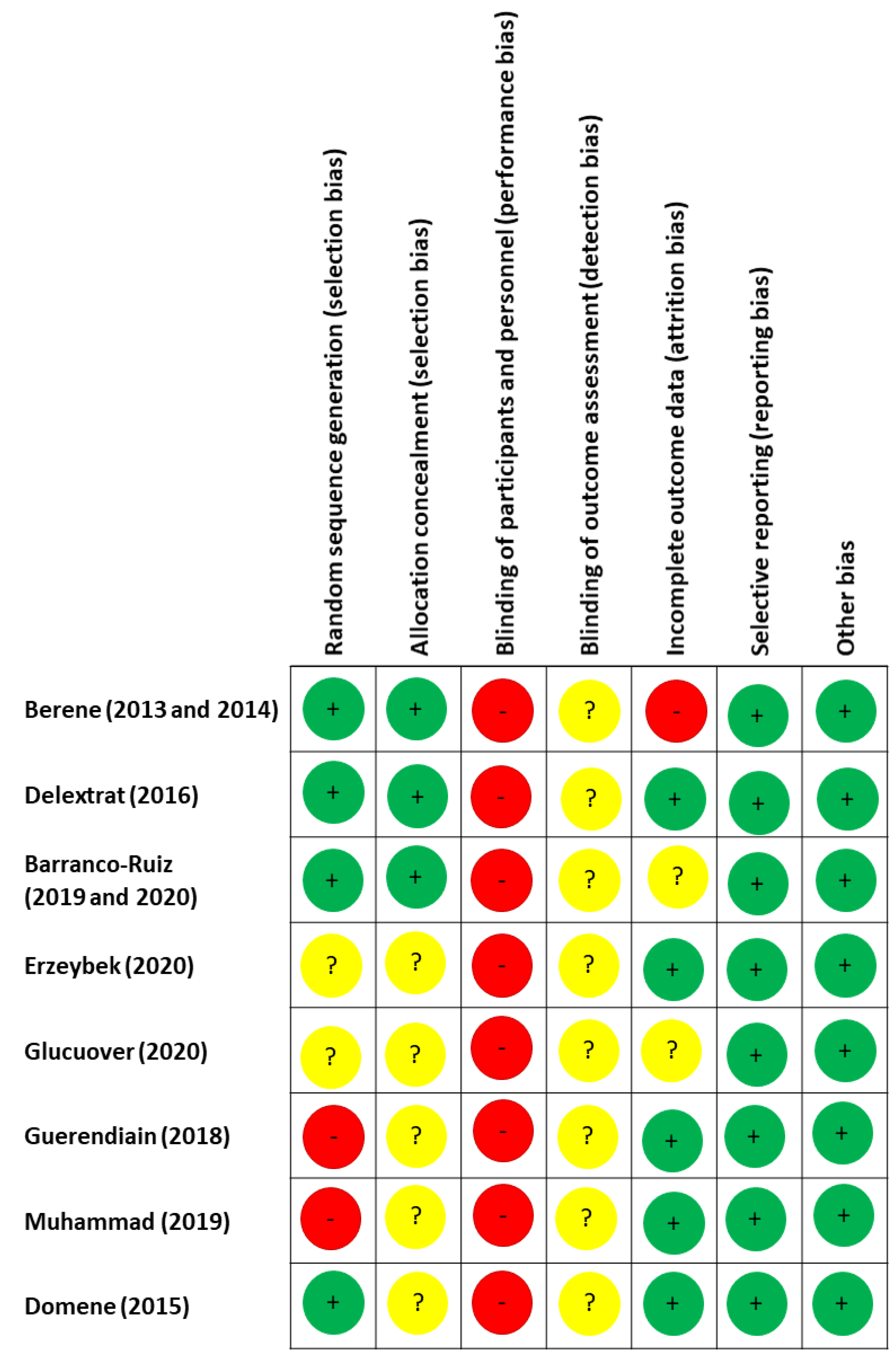
2.3. Quality of Evidence and Risk of Bias
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Quality of Evidence and Risk of Bias
3.3. Study Characteristics
3.4. Interventions
3.5. Outcome Measures
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Deurenberg, P.; Yap, M.; van Staveren, W.A. Body mass index and percent body fat: A meta analysis among different ethnic groups. Int. J. Obes. Relat. Metab. Disord. J. Int. Assoc. Study Obes. 1998, 22, 1164–1171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Physical Status: The Use and Interpretation of Anthropometry; Report of a WHO Expert Committee, Technical Report Series No. 854; WHO: Geneva, Switzerland, 1995. [Google Scholar]
- De Lorenzo, A.; Deurenberg, P.; Pietrantuono, M.; Di Daniele, N.; Cervelli, V.; Andreoli, A. How fat is obese? Acta Diabetol. 2003, 40 (Suppl. S1), S254–S257. [Google Scholar] [CrossRef]
- Jakicic, J.M.; Rogers, R.J.; Davis, K.K.; Collins, K.A. Role of Physical Activity and Exercise in Treating Patients with Overweight and Obesity. Clin. Chem. 2018, 64, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Koh, I.-S.; Minn, Y.-K.; Suk, S.-H. Body Fat Mass and Risk of Cerebrovascular Lesions: The PRESENT (Prevention of Stroke and Dementia) Project. Int. J. Environ. Res. Public Health 2019, 16, 2840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauer, U.E.; Briss, P.A.; Goodman, R.A.; Bowman, B.A. Prevention of chronic disease in the 21st century: Elimination of the leading preventable causes of premature death and disability in the USA. Lancet 2014, 384, 45–52. [Google Scholar] [CrossRef]
- Srikanthan, P.; Horwich, T.B.; Tseng, C.H. Relation of Muscle Mass and Fat Mass to Cardiovascular Disease Mortality. Am. J.Cardiol. 2016, 117, 1355–1360. [Google Scholar] [CrossRef]
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. Circulation 2014, 129, S102–S138. [Google Scholar] [CrossRef] [Green Version]
- Lee, W.S. Body fatness charts based on BMI and waist circumference. Obesity 2016, 24, 245–249. [Google Scholar] [CrossRef]
- Calling, S.; Hedblad, B.O.; Engström, G.; Berglund, G.; Janzon, L. Effects of body fatness and physical activity on cardiovascular risk: Risk prediction using the bioelectrical impedance method. Scand. J. Public Health 2006, 34, 568–575. [Google Scholar] [CrossRef]
- Padwal, R.; Majumdar, S.R.; Leslie, W.D. Relationship among body fat percentage, body mass index, and all-cause mortality. Ann. Intern. Med. 2016, 165, 604. [Google Scholar] [CrossRef]
- Gómez-Ambrosi, J.; Silva, C.; Galofré, J.C.; Escalada, J.; Santos, S.; Millán, D.; Vila, N.; Ibañez, P.; Gil, M.J.; Valentí, V. Body mass index classification misses subjects with increased cardiometabolic risk factors related to elevated adiposity. Int. J. Obes. 2012, 36, 286–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ochner, C.N.; Barrios, D.M.; Lee, C.D.; Pi-Sunyer, F.X. Biological mechanisms that promote weight regain following weight loss in obese humans. Physiol. Behav. 2013, 120, 106–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bacon, A.P.; Carter, R.E.; Ogle, E.A.; Joyner, M.J. VO2max trainability and high intensity interval training in humans: A meta-analysis. PLoS ONE 2013, 8, e73182. [Google Scholar] [CrossRef] [PubMed]
- Wilson, M.G.; Ellison, G.M.; Cable, N.T. Basic science behind the cardiovascular benefits of exercise. Br. J. Sports Med. 2016, 50, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.; Chen, W.; Wang, R.; Qi, Q.; Li, K.; Zhang, W.; Wang, H. Association of apolipoprotein E polymorphism with maximal oxygen uptake after exercise training: A study of Chinese young adult. Lipids Health Dis. 2014, 13, 40. [Google Scholar] [CrossRef] [Green Version]
- Dale, L.P.; LeBlanc, A.G.; Orr, K.; Berry, T.; Deshpande, S.; Latimer-Cheung, A.E.; O’Reilly, N.; Rhodes, R.E.; Tremblay, M.S.; Faulkner, G. Canadian physical activity guidelines for adults: Are Canadians aware? Appl. Physiol. Nutr. Metab. 2016, 41, 1008–1011. [Google Scholar] [CrossRef] [Green Version]
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K. American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med. Sci. Sports Exerc. 2009, 41, 459–471. [Google Scholar] [CrossRef]
- Riebe, D.; Blissmer, B.; Greene, G.; Caldwell, M.; Ruggiero, L.; Stillwell, K.M.; Nigg, C.R. Long-term maintenance of exercise and healthy eating behaviors in overweight adults. Prev. Med. 2005, 40, 769–778. [Google Scholar] [CrossRef]
- Chavarrias, M.; Carlos-Vivas, J.; Pérez-Gómez, J. Health benefits of Zumba: A systematic review. J. Sport Health Res. 2018, 10, 327–338. [Google Scholar]
- Domene, P.A.; Moir, H.J.; Pummell, E.; Knox, A.; Easton, C. The health-enhancing efficacy of Zumba® fitness: An 8-week randomised controlled study. J. Sports Sci. 2016, 34, 1396–1404. [Google Scholar] [CrossRef] [Green Version]
- Hemmingsson, E.; Page, A.; Fox, K.; Rössner, S. Influencing adherence to physical activity behaviour change in obese adults. Näringsforskning 2001, 45, 114–119. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PloS Med. 2009, 6, e1000097. [Google Scholar]
- GRADE Working Group. Grading quality of evidence and strength of recommendations. BMJ 2004, 328, 1490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. Cochrane bias methods group; cochrane statistical methods group. Cochrane Collab. Tool Assess. Risk Bias Randomised Trials. BMJ 2011, 343, d5928. [Google Scholar]
- Delextrat, A.A.; Warner, S.; Graham, S.; Neupert, E. An 8-Week Exercise Intervention Based on Zumba Improves Aerobic Fitness and Psychological Well-Being in Healthy Women. J. Phys. Act. Health 2016, 13, 131–139. [Google Scholar] [CrossRef]
- Barene, S.; Krustrup, P.; Jackman, S.R.; Brekke, O.L.; Holtermann, A. Do soccer and Zumba exercise improve fitness and indicators of health among female hospital employees? A 12-week RCT. Scand. J. Med. Sci. Sports 2014, 24, 990–999. [Google Scholar] [CrossRef] [PubMed]
- Barene, S.; Krustrup, P.; Brekke, O.L.; Holtermann, A. Soccer and Zumba as health-promoting activities among female hospital employees: A 40-weeks cluster randomised intervention study. J. Sports Sci. 2014, 32, 1539–1549. [Google Scholar] [CrossRef]
- Guerendiain, M.; Villa-González, E.; Barranco-Ruiz, Y. Body composition and dairy intake in sedentary employees who participated in a healthy program based on nutrition education and Zumba. Clin. Nutr. 2019, 38, 2277–2286. [Google Scholar] [CrossRef]
- Gucluover, A. The effect of 8-week Zumba® fitness on body composition of turkish womens. Prog. Nutr. 2020, 22, 316–322. [Google Scholar]
- Erzeybek, M.S. Investigation of the Effect of Oscillation (Swing) and Zumba Training on Body Fat Percentage Values in Women. Int. J. Appl. Exerc. Physiol. 2020, 9, 92–100. [Google Scholar]
- Muhammad, H.F.L.; Safika, E.L.; Wahyuni, F.C.; Ermamilia, A.; Huriyati, E. The Effect of Zumba Training on Body Composition, Dietary Intake, Sleep Quality, and Duration in Adult Sedentary Women With Overweight. Top. Clin. Nutr. 2019, 34, 277–286. [Google Scholar] [CrossRef]
- Barranco-Ruiz, Y.; Ramírez-Vélez, R.; Martínez-Amat, A.; Villa-González, E. Effect of Two Choreographed Fitness Group-Workouts on the Body Composition, Cardiovascular and Metabolic Health of Sedentary Female Workers. Int. J. Environ. Res. Public Health 2019, 16, 4986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barranco-Ruiz, Y.; Villa-González, E. Health-Related Physical Fitness Benefits in Sedentary Women Employees after an Exercise Intervention with Zumba Fitness®. Int. J. Environ. Res. Public Health 2020, 17, 2632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acsm. ACSM’s Guidelines for Exercise Testing and Prescription; Wolters Kluwer: Philadelphia, PA, USA, 2017. [Google Scholar]
- Fritzen, A.M.; Thøgersen, F.B.; Thybo, K.; Vissing, C.R.; Krag, T.O.; Ruiz-Ruiz, C.; Risom, L.; Wibrand, F.; Høeg, L.D.; Kiens, B.; et al. Adaptations in Mitochondrial Enzymatic Activity Occurs Independent of Genomic Dosage in Response to Aerobic Exercise Training and Deconditioning in Human Skeletal Muscle. Cells 2019, 8, 237. [Google Scholar] [CrossRef] [Green Version]
- Purdom, T.; Kravitz, L.; Dokladny, K.; Mermier, C. Understanding the factors that effect maximal fat oxidation. J. Int. Soc. Sports Nutr. 2018, 15, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Achten, J.; Jeukendrup, A.E. Optimizing fat oxidation through exercise and diet. Nutrition 2004, 20, 716–727. [Google Scholar] [CrossRef]
- Mika, A.; Macaluso, F.; Barone, R.; Di Felice, V.; Sledzinski, T. Effect of exercise on fatty acid metabolism and adipokine secretion in adipose tissue. Front. Physiol. 2019, 10, 26. [Google Scholar] [CrossRef] [Green Version]
- Johnstone, A.M.; Murison, S.D.; Duncan, J.S.; Rance, K.A.; Speakman, J.R. Factors influencing variation in basal metabolic rate include fat-free mass, fat mass, age, and circulating thyroxine but not sex, circulating leptin, or triiodothyronine. Am. J. Clin. Nutr. 2005, 82, 941–948. [Google Scholar] [CrossRef] [Green Version]
- Piers, L.S.; Soares, M.J.; McCormack, L.M.; O’Dea, K. Is there evidence for an age-related reduction in metabolic rate? J. Appl. Physiol. 1998, 85, 2196–2204. [Google Scholar] [CrossRef]
- Luettgen, M.; Foster, C.; Doberstein, S.; Mikat, R.; Porcari, J. Zumba®: Is the “fitness-party” a good workout? J. Sports Sci. Med. 2012, 11, 357–358. [Google Scholar]
- Demers, M.; Thomas, A.; Wittich, W.; McKinley, P. Implementing a novel dance intervention in rehabilitation: Perceived barriers and facilitators. Disabil. Rehabil. 2015, 37, 1066–1072. [Google Scholar] [CrossRef] [PubMed]
- Plotnikoff, R.C.; Taylor, L.M.; Wilson, P.M.; Courneya, K.S.; Sigal, R.J.; Birkett, N.; Raine, K.; Svenson, L.W. Factors associated with physical activity in Canadian adults with diabetes. Med. Sci. Sports Exerc. 2006, 38, 1526–1534. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, R.E.; Fiala, B.; Conner, M. A review and meta-analysis of affective judgments and physical activity in adult populations. Ann. Behav. Med. A Publ. Soc. Behav. Med. 2009, 38, 180–204. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.M.; Williams, G.C.; Patrick, H.; Deci, E.L. Self-determination theory and physical activity: The dynamics of motivation in development and wellness. Hell. J. Psychol. 2009, 6, 107–124. [Google Scholar]
- Rossmeissl, A.; Lenk, S.; Hanssen, H.; Donath, L.; Schmidt-Trucksäss, A.; Schäfer, J. ZumBeat: Evaluation of a Zumba Dance Intervention in Postmenopausal Overweight Women. Sports 2016, 4, 5. [Google Scholar] [CrossRef] [Green Version]
- Araneta, M.R.; Tanori, D. Benefits of Zumba Fitness® among sedentary adults with components of the metabolic syndrome: A pilot study. J. Sports Med. Phys. Fit. 2015, 55, 1227–1233. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| RCT | Weeks | Sample Size of Groups and Sex | Age |
|---|---|---|---|
| Delextrat, Warner, Graham, and Neupert (2016) | 8 | ZU: 22 (females) CG: 22 (females) | 26.6 (5.4) 27.9 (6.0) |
| Barene, Krustrup, Brekke, and Holtermann (2014) | 40 | ZU: 25 (0 males, 25 females) CG: 25 (2 males, 23 females) | 45.9 (9.6) 47.4 (9.5) |
| Barene, Krustrup, Jackman, Brekke, and Holtermann (2013) | 12 | ZU: 35 (0 males, 30 females) CG: 35 (3 males, 31 females) | 45.9 (9.6) 47.4 (9.5) |
| Barranco-Ruiz (2019) | 16 | ZU: 39 (females) CG: 31 (females) | 39.87 (7) 38.19 (5.6) |
| Erzeybek (2020) | 8 | ZU: 9 (females) CG: 9 (females) | 26.5 (1.8) 28.3 (3.2) |
| Gucluover (2020) | 8 | ZU: 14 (females) CG: 14 (females) | 18–35 |
| Guerendiain (2018) | 16 | ZU: 38 (86.84% females) CG: 28 (71.43% females) | 38.24 (8.09 39.32 (6.40) |
| Muhammad (2019) | 6 | ZU: 29 (females) CG: 28 (females) | 21.1 (0.4) 21.4 (0.4) |
| Barranco-Ruiz, and Villa-González (2020) | 16 | ZU: 33 (females) CG: 33 (females) | 38.06 (7.11) 38.06 (7.11) |
| Domene, Moir, Pummell, Knox, and Easton (2016) | 8 | ZU: 10 (females) CG: 10 (females) | 33 (11) 35 (13) |
| RCT | Exercise Group | Control Group | Duration | Days Per | Training |
|---|---|---|---|---|---|
| Type of Exercise | Type of Exercise | Week | Sessions | ||
| Delextrat, Warner, Graham, and Neupert (2016) [26] | Zumba® workouts (1-h length each one) | Carried on normal daily activities | 8 weeks | 3 | 24 |
| Classes performed at home following a DVD | |||||
| Barene, Krustrup, Brekke, and Holtermann (2014) [28] | Zumba® workouts (1-h length) | No intervention | 40 weeks | 2–3 | NR |
| Certified instructor | |||||
| Barene, Krustrup, Jackman, Brekke, and Holtermann (2013) [27] | Zumba® workouts (1-h length) | No intervention | 12 weeks | 2–3 | NR |
| Certified instructor | |||||
| Barranco-Ruiz (2019) [33] | Zumba® workouts (1-h length) Certified instructor | No intervention | 16 weeks | 3 | NR |
| Erzeybek (2020) [31] | Zumba® workouts (45-min length) | Oscillation training | 8 weeks | 3 | NR |
| Gucluover (2020) [30] | Zumba® workouts (1-h length) | Carried on normal daily activities | 8 weeks | 3 | NR |
| Guerendiain (2018) [29] | Zumba® workouts (1-h length) | Zumba® workouts plus body weight | 16 weeks | 3 | NR |
| Muhammad (2019) [32] | Zumba® workouts (1-h length) | Educational program | 6 weeks | 2 | NR |
| Barranco-Ruiz, and Villa-González (2020) [34] | Zumba® workouts (1-h length) Certified instructor | No intervention | 16 weeks | 3 | NR |
| Domene, Moir, Pummell, Knox, and Easton (2016) [21] | Zumba® workouts (1-h length each one) classes were taught by certified instructor | Carried on normal daily activities | 8 weeks | 1–2 | 12 |
| Authors | Weeks | Groups | Pre-Test | Post-Test | Change (Δ) | P-Values | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Intragroup | Between Groups | ||||||||||
| Delextrat, Warner, Graham, and Neupert (2016) [26] | 8 | ZU | 26.7 | ± | 5.7 | 26.4 | ± | 5.1 | −0.3 | NS | 0.908 |
| CG | 23.5 | ± | 5.7 | 23.6 | ± | 3.5 | 0.1 | NS | |||
| Barene, Krustrup, Brekke, and Holtermann (2013) [27] | 12 | ZU | 35.9 | ± | 5.8 | 34.9 | ± | 5.7 | −1 | - | 0.07 |
| CG | 36.3 | ± | 6.4 | 35.9 | ± | 6.4 | −0.4 | - | |||
| Barene, Krustrup, Jackman, Brekke, and Holtermann (2014) [28] | 40 | ZU | 35.9 | ± | 5.8 | 35.2 | ± | 5.8 | −0.7 | - | 0.003 |
| CG | 36.3 | ± | 6.4 | 36.9 | ± | 6.6 | 0.6 | - | |||
| Barranco-Ruiz (2019) [33] | 16 | ZU | 22.74 | ± | 4.31 | 19.75 | ± | 4.22 | −2.99 | S | <0.001 |
| CG | 19.95 | ± | 1.88 | 20.31 | ± | 3.54 | −0.36 | NS | |||
| Erzeybek et al. (2020) [31] | 8 | ZU | 22.74 | ± | 2.17 | 21.84 | ± | 7.42 | −0.9 | NS | 0.157 |
| CG | 29.09 | ± | 5.51 | 27.03 | ± | 5.73 | −2.06 | S | |||
| Gucluover (2020) [30] | 8 | ZU | 31.66 | ± | 7.34 | 30.22 | ± | 7.16 | −1.44 | S | NR |
| CG | 30.78 | ± | 8.38 | 31.40 | ± | 8.41 | 0.62 | NS | |||
| Guerendiain (2018) [29] | 6 | ZU | 22.13 | ± | 4.48 | 18.80 | ± | 3.40 | −3.33 | S | NS |
| CG | 21.36 | ± | 3.08 | 17.99 | ± | 2.91 | −3.37 | S | |||
| Muhammad (2019) [32] | 6 | ZU | 33.4 | ± | 0.5 | 33 | ± | 0.5 | −0.4 | NS | 0.023 |
| CG | 33.3 | ± | 0.4 | 33.6 | ± | 0.5 | 0.3 | S | |||
| Domene et al. (2016) [21] | 8 | ZU | 30.9 | ± | 5.5 | - | - | −1.2 | S | <0.05 | |
| CG | 31.7 | ± | 5.8 | - | - | 0 | NS | ||||
| Authors | Weeks | Groups | Pre-Test | Post-Test | Change (Δ) | P-Values | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Intragroup | Between Groups | ||||||||||
| Domene, Moir, Pummell, Knox, and Easton (2016) [21] | 8 | ZU | 29.4 | ± | 5.9 | NR | ± | NR | 3.1 | S | <0.05 |
| CG | 28.0 | ± | 6.7 | NR | ± | NR | −0.7 | NS | |||
| Delextrat, Warner, Graham, and Neupert (2016) [26] | 8 | ZU | 38.1 | ± | 4.6 | 39.3 | ± | 4.0 | 1.2 | S | |
| CG | 38.3 | ± | 5.3 | 37.3 | ± | 5.4 | −1.0 | NS | 0.01 | ||
| Barene, Krustrup, Brekke, and Holtermann (2014) [28] | 40 | ZU | 31.8 | ± | 6.7 | 32.4 | ± | 5.8 | 0.6 | NR | 0.001 |
| CG | 33.1 | ± | 6.7 | 33.4 | ± | 6.9 | 0.3 | NR | |||
| Barene, Krustrup, Jackman, Brekke, and Holtermann (2013) [27] | 12 | ZU | 31.8 | ± | 6.7 | 32.8 | ± | 6.3 | 1 | NR | <0.05 |
| CG | 33.1 | ± | 6.7 | 32.6 | ± | 6.8 | −0.5 | NR | |||
| Barranco-Ruiz, and Villa-González (2020) [34] | 16 | ZU | 34.67 | ± | 3.94 | 36.00 | ± | 3.84 | 1.33 | S | 0.030 |
| CG | 32.63 | ± | 5.87 | 32.49 | ± | 6.27 | −0.14 | NS | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chavarrias, M.; Villafaina, S.; Lavín-Pérez, A.M.; Carlos-Vivas, J.; Merellano-Navarro, E.; Pérez-Gómez, J. Zumba®, Fat Mass and Maximum Oxygen Consumption: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 105. https://doi.org/10.3390/ijerph18010105
Chavarrias M, Villafaina S, Lavín-Pérez AM, Carlos-Vivas J, Merellano-Navarro E, Pérez-Gómez J. Zumba®, Fat Mass and Maximum Oxygen Consumption: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(1):105. https://doi.org/10.3390/ijerph18010105
Chicago/Turabian StyleChavarrias, Manuel, Santos Villafaina, Ana Myriam Lavín-Pérez, Jorge Carlos-Vivas, Eugenio Merellano-Navarro, and Jorge Pérez-Gómez. 2021. "Zumba®, Fat Mass and Maximum Oxygen Consumption: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 1: 105. https://doi.org/10.3390/ijerph18010105