
The Health Status Transition and Medical Expenditure Evaluation of Elderly Population in China


 and
and 
Abstract
:1. Introduction
2. Data and Measures
2.1. Data
2.1.1. Data Source
2.1.2. Ethical Statement
2.1.3. Concept Definition
2.2. Improved Traditional Markov Model
2.3. TMP Model and Theoretical Framework
3. Results
3.1. Analysis of the Elderly Health Status Transition and Medical Expenditure
3.1.1. Measurement of the Health Transition Rate of the Elderly Based on the Markov Model
3.1.2. Analysis of the Relationship between Health Status and Medical Expenses
3.2. Prediction of Health Status Transition and Medical Expenditure of the Elderly
3.2.1. Prediction of the Population Size of Different Elderly Health Statuses
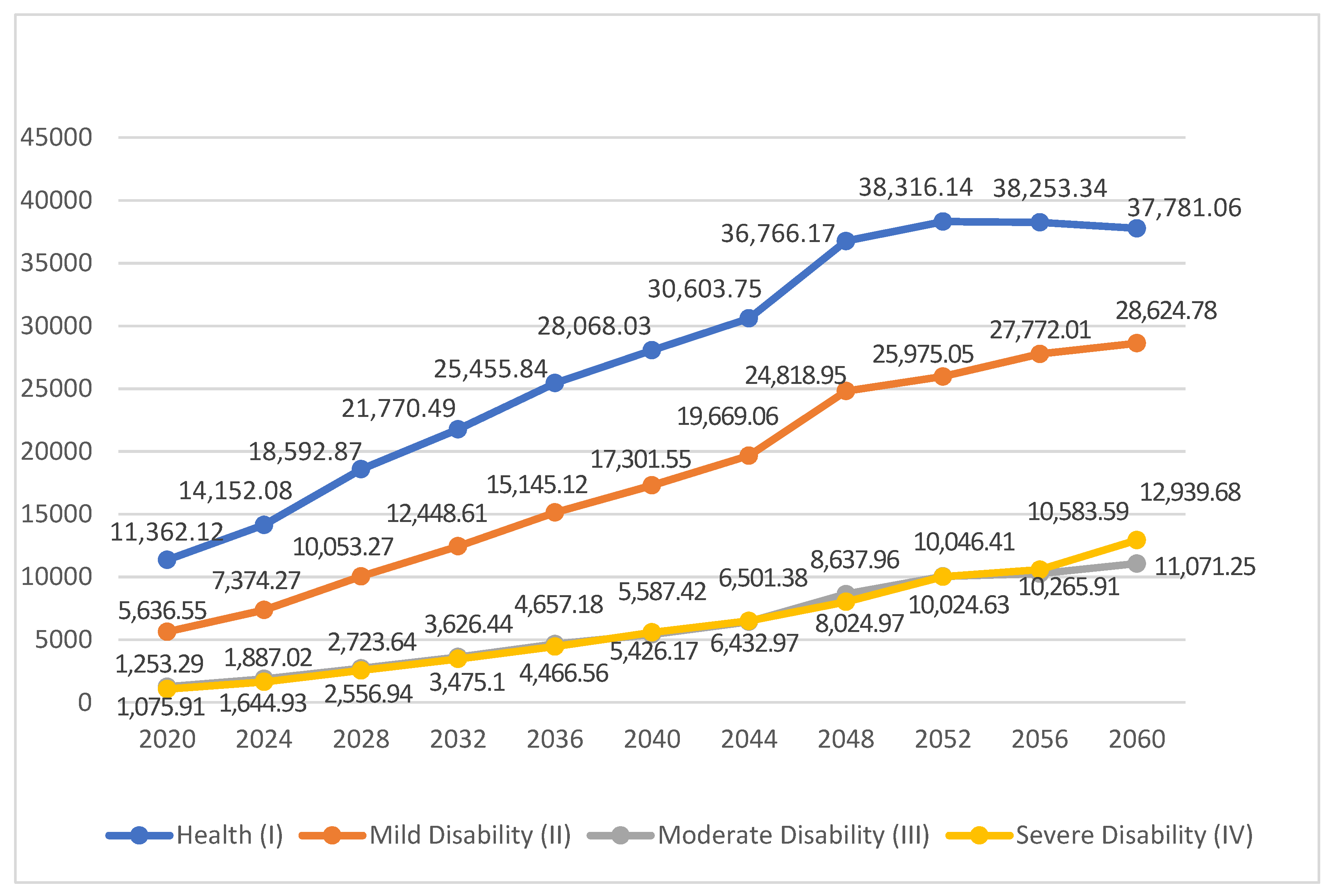
3.2.2. Prediction of Medical Expenditure for the Elderly in Different Health Conditions
4. Conclusions and Policy Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Ethical Statement
Conflicts of Interest
References
- Lu, J.; Liu, Q. Four decades of studies on population aging in China. China Popul. Dev. Stud. 2019, 3, 24–36. [Google Scholar] [CrossRef] [Green Version]
- National Bureau of Statistics. Age Composition and Dependency Ratio of Population. Available online: http://www.stats.gov.cn/tjsj/ndsj/2019/indexeh.htm (accessed on 3 April 2021).
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of illness in the aged: The index of ADL: A standardized measure of biological and psychosocial function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Yi, Z.; Vaupel, J.W.; Zhenyu, X.; Chunyuan, Z.; Yuzhi, L. Sociodemographic and health profiles of the oldest old in China. Popul. Dev. Rev. 2002, 28, 251–273. [Google Scholar] [CrossRef]
- Keyes, K.M.; Utz, R.L.; Robinson, W.; Li, G. What is a cohort effect? Comparison of three statistical methods for modeling cohort effects in obesity prevalence in the United States, 1971–2006. Soc. Sci. Med. 2010, 70, 1100–1108. [Google Scholar] [CrossRef] [Green Version]
- Reither, E.N.; Hauser, R.M.; Yang, Y. Do birth cohorts matter? Age-period-cohort analyses of the obesity epidemic in the United States. Soc. Sci. Med. 2009, 69, 1439–1448. [Google Scholar] [CrossRef] [Green Version]
- Bleakley, H. Health, human capital, and development. Annu. Rev. Econ. 2010, 2, 283–310. [Google Scholar] [CrossRef] [Green Version]
- Gallant, M.P.; Dorn, G.P. Gender and race differences in the predictors of daily health practices among older adults. Health Educ. Res. 2001, 16, 21–31. [Google Scholar] [CrossRef] [Green Version]
- Molarius, A.; Janson, S. Self-rated health, chronic diseases, and symptoms among middle-aged and elderly men and women. J. Clin. Epidemiol. 2002, 55, 364–370. [Google Scholar] [CrossRef]
- Zhang, Y.; Xiong, Y.; Yu, Q.; Shen, S.; Chen, L.; Lei, X. The activity of daily living (ADL) subgroups and health impairment among Chinese elderly: A latent profile analysis. BMC Geriatr. 2021, 21, 13–22. [Google Scholar]
- Spiers, N.; Jagger, C.; Clarke, M.; Arthur, A. Are gender differences in the relationship between self-rated health and mortality enduring? Results from three birth cohorts in Melton Mowbray, United Kingdom. Gerontologist 2003, 43, 406–411. [Google Scholar] [CrossRef] [Green Version]
- Weeks, W.B.; Kazis, L.E.; Shen, Y.; Cong, Z.; Ren, X.S.; Miller, D.; Lee, A.; Perlin, J.B. Differences in health-related quality of life in rural and urban veterans. Am. J. Public Health 2004, 94, 1762–1767. [Google Scholar] [CrossRef]
- Fogelholm, M.; Valve, R.; Absetz, P.; Heinonen, H.; Uutela, A.; Patja, K.; Karisto, A.; Konttinen, R.; Mäkelä, T.; Nissinen, A. Rural—Urban differences in health and health behaviour: A baseline description of a community health-promotion programme for the elderly. Scand. J. Public Health 2006, 34, 632–640. [Google Scholar] [CrossRef]
- Zimmer, Z.; Kwong, J. Socioeconomic Status and Health among Older Adults in Rural and Urban China. J. Aging Health 2004, 16, 44–70. [Google Scholar] [CrossRef] [PubMed]
- Akbari, H.; Taghizadeh-Hesary, F.; Heike, Y.; Bahadori, M. Cell Energy: A New Hypothesis in Decoding Cancer Evolution. Arch. Iran. Med. 2019, 22, 733–735. [Google Scholar]
- Nathanson, C.A. Illness and the feminine role: A theoretical review. Soc. Sci. Med. (1967) 1975, 9, 57–62. [Google Scholar] [CrossRef]
- Goldman, N. Marriage selection and mortality patterns: Inferences and fallacies. Demography 1993, 30, 189–208. [Google Scholar] [CrossRef]
- Lowry, D.; Xie, Y. Socioeconomic Status and Health Differentials in China: Convergence or Divergence at Older Ages? 2009. Available online: https://scholar.princeton.edu/sites/default/files/yuxie/files/lowry-xie2009.pdf (accessed on 23 June 2021).
- Lu, S.B.; Xiao, J.; Guo, B.M. Analysis of standard accounting method of economic compensation for ecological pollution in watershed. Sci. Total Environ. 2020, 737, 138157. [Google Scholar] [CrossRef] [PubMed]
- Galenkamp, H.; Deeg, D.J.; Huisman, M.; Hervonen, A.; Braam, A.W.; Jylhä, M. Is self-rated health still sensitive for changes in disease and functioning among nonagenarians? J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2013, 68, 848–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Comas-Herrera, A.; Wittenberg, R.; Pickard, L.; Knapp, M. Cognitive impairment in older people: Future demand for long-term care services and the associated costs. Int. J. Geriatr. Psychiatry A J. Psychiatry Late Life All. Sci. 2007, 22, 1037–1045. [Google Scholar] [CrossRef] [Green Version]
- Costa-Font, J.; Wittenberg, R.; Patxot, C.; Comas-Herrera, A.; Gori, C.; Di Maio, A.; Pickard, L.; Pozzi, A.; Rothgang, H. Projecting long-term care expenditure in four European Union member states: The influence of demographic scenarios. Soc. Ind. Res. 2008, 86, 303–321. [Google Scholar] [CrossRef] [Green Version]
- Lu, S.B.; Zhang, X.L.; Wang, J.H.; Pei, L. Impacts of different media on constructed wetlands for rural household sewage treatment. J. Clean. Prod. 2016, 127, 325–330. [Google Scholar] [CrossRef]
- Lu, S.; Bai, X.; Li, W.; Wang, N. Impacts of climate change on water resources and grain production. Technol. Forecast. Soc. Chang. 2019, 143, 76–84. [Google Scholar] [CrossRef]
- Chahed, S.; Demir, E.; Chaussalet, T.J.; Millard, P.H.; Toffa, S. Measuring and modelling occupancy time in NHS continuing healthcare. BMC Health Serv. Res. 2011, 11, 155. [Google Scholar] [CrossRef] [Green Version]
- Hu, H.; Li, Y.; Zhang, L. Estimation and Prediction of Demand of Chinese Elederly Long-term Care Services. Chin. J. Popul. Sci. 2015, 13, 79–89. [Google Scholar]
- Gagniuc, P.A. Markov Chains: From Theory to Implementation and Experimentation; John Wiley & Sons: Hoboken, NJ, USA, 2017; pp. 1–8. [Google Scholar]


{kind=link}
| Health Status | Description |
|---|---|
| Healthy (I) | Need no help in instrumental activities or daily living activities |
| Mild disability (II) | Need help in 1 or more instrumental activities, need no help in daily living activities |
| Moderate disability (III) | Need help in 1–3 daily living activities |
| Severe disability (IV) | Need help in 4 or more daily living activities |
| 2011 | 2013 | 2015 | |
|---|---|---|---|
| Healthy (I) | 75.05% | 72.31% | 70.22% |
| Mild disability (II) | 20.52% | 21.73% | 23.06% |
| Moderate disability (III) | 3.17% | 3.99% | 4.23% |
| Severe disability (IV) | 1.26% | 1.97% | 2.49% |
| Health Condition | Healthy (I) | Mild Disability (II) | Moderate Disability (III) | Severe Disability (IV) |
|---|---|---|---|---|
| Healthy (I) | 0.8215 | 0.1487 | 0.0264 | 0.0034 |
| Mild disability (II) | 0.2711 | 0.7045 | 0.0197 | 0.0047 |
| Moderate disability (III) | 0.0991 | 0.1214 | 0.5936 | 0.1859 |
| Severe disability (IV) | 0.0131 | 0.1599 | 0.3057 | 0.5213 |
| Independent Variable | Average Annual Medical Expenses for Families | Average Annual Medical Expenses for the Elderly | ||
|---|---|---|---|---|
| Participation Model (1) | Expenditure Model (2) | Participation Model (3) | Expenditure Model (4) | |
| Health Status | ||||
| Status I–IV | 0.318 *** (0.041) | 2792.1 *** (207.8) | 0.341 *** (0.027) | 4291.5 *** (151.6) |
| Demographic variables | ||||
| Age 60 years old and above | −0.038 *** (0.017) | −183.2 * (146.8) | −0.035 *** (0.012) | −131.4 (146.5) |
| Gender 1 = Male; 0 = Female | 0.057 (0.039) | −193.4 (155.6) | −0.061 * (0.028) | −255.3 (40.9) |
| Households Urban = 1; Rural = 0 | −0.257 *** (0.053) | 1135.0 *** (371.4) | 0.132 *** (0.039) | 2358.7 *** (90.4) |
| Socioeconomic status variables. | ||||
| Level of education 1 = Junior High School and above; 0 = other | 0.021 (0.064) | 218.7 (581.9) | 0.052 * (0.037) | 341.8 * (92.7) |
| Annual family income | 0.057 *** (0.017) | 2061.0 *** (143.5) | 0.038 *** (0.013) | 568.5 ** (37.2) |
| pension 1 = Yes; 0 = None | 0.306 *** (0.068) | −2018.5 ** (611.7) | 0.047 (0.045) | −2205.7 ** (105.6) |
| Health insurance 1 = Yes; 0 = None | 0.475 *** (0.084) | 994.9 (807.7) | 0.232 * (0.078) | 1385.5 * (257.4) |
| Health behavior variables. | ||||
| Physical exercise 1 = Yes; 0 = None | 0.219 (0.114) | 21.7 (24.4) | 0.067 *** (0.048) | 140.0 (80.3) |
| Social Activities 1 = Yes; 0 = None | 0.072 (0.094) | −606.8 * (141.6) | 0.261 *** (0.039) | −1219.5 * (71.2) |
| Smoking habits 1 = Yes; 0 = None | 0.104 ** (0.087) | −226.3 (103.4) | 0.072 * (0.049) | 1291.3 (107.7) |
| Constant | −0.452 *** (0.305) | −7042.1 *** (1488.9) | −0.079 *** (0.262) | −7534.9 (430.5) |
| Sample value | 1204 | 5608 | 1627 | 5185 |
| Year | Healthy (I) | Mild Disability (II) | Moderate Disability (III) | Severe Disability (IV) | Total |
|---|---|---|---|---|---|
| 2020 | 17,958.58 | 6253.92 | 1115.10 | 665.42 | 25,993.03 |
| 2024 | 19,053.55 | 6969.50 | 1430.15 | 866.59 | 28,319.79 |
| 2028 | 22,468.21 | 8528.18 | 1852.77 | 1209.07 | 34,058.22 |
| 2032 | 23,613.29 | 9478.42 | 2214.21 | 1474.91 | 36,780.83 |
| 2036 | 24,782.33 | 10,350.91 | 2552.28 | 1701.52 | 39,387.04 |
| 2040 | 24,964.58 | 10,802.49 | 2716.79 | 1944.61 | 40,428.47 |
| 2044 | 24,868.22 | 11,219.67 | 2942.60 | 2067.21 | 41,097.71 |
| 2048 | 25,486.19 | 12,077.20 | 3370.68 | 2446.67 | 43,380.73 |
| 2052 | 24,800.88 | 12,065.87 | 3487.22 | 2539.28 | 42,893.26 |
| 2056 | 23,586.41 | 12,020.60 | 3563.20 | 2553.49 | 41,723.71 |
| 2060 | 22,190.84 | 11,802.34 | 3660.55 | 2973.94 | 40,627.69 |
| Healthy (I) | Mild Disability (II) | Moderate Disability (III) | Severe Disability (IV) | |
|---|---|---|---|---|
| Average annual family health expenditure | 3754.79 | 4521.03 | 5699.14 | 7290.27 |
| Annual individual medical expenditure | 2572.06 | 4491.79 | 5540.11 | 8878.55 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, L.; Tang, Y.; Roshanmehr, F.; Bai, X.; Taghizadeh-Hesary, F.; Taghizadeh-Hesary, F. The Health Status Transition and Medical Expenditure Evaluation of Elderly Population in China. Int. J. Environ. Res. Public Health 2021, 18, 6907. https://doi.org/10.3390/ijerph18136907
Wang L, Tang Y, Roshanmehr F, Bai X, Taghizadeh-Hesary F, Taghizadeh-Hesary F. The Health Status Transition and Medical Expenditure Evaluation of Elderly Population in China. International Journal of Environmental Research and Public Health. 2021; 18(13):6907. https://doi.org/10.3390/ijerph18136907
Chicago/Turabian StyleWang, Lianjie, Yao Tang, Farnaz Roshanmehr, Xiao Bai, Farzad Taghizadeh-Hesary, and Farhad Taghizadeh-Hesary. 2021. "The Health Status Transition and Medical Expenditure Evaluation of Elderly Population in China" International Journal of Environmental Research and Public Health 18, no. 13: 6907. https://doi.org/10.3390/ijerph18136907
APA StyleWang, L., Tang, Y., Roshanmehr, F., Bai, X., Taghizadeh-Hesary, F., & Taghizadeh-Hesary, F. (2021). The Health Status Transition and Medical Expenditure Evaluation of Elderly Population in China. International Journal of Environmental Research and Public Health, 18(13), 6907. https://doi.org/10.3390/ijerph18136907