
Comparison of SARS-CoV-2 Detection by Rapid Antigen and by Three Commercial RT-qPCR Tests: A Study from Martin University Hospital in Slovakia

 , , , , , , , , and
, , , , , , , , and
Abstract
:1. Introduction
2. Results
2.1. SARS-CoV-2 Antigen Detection
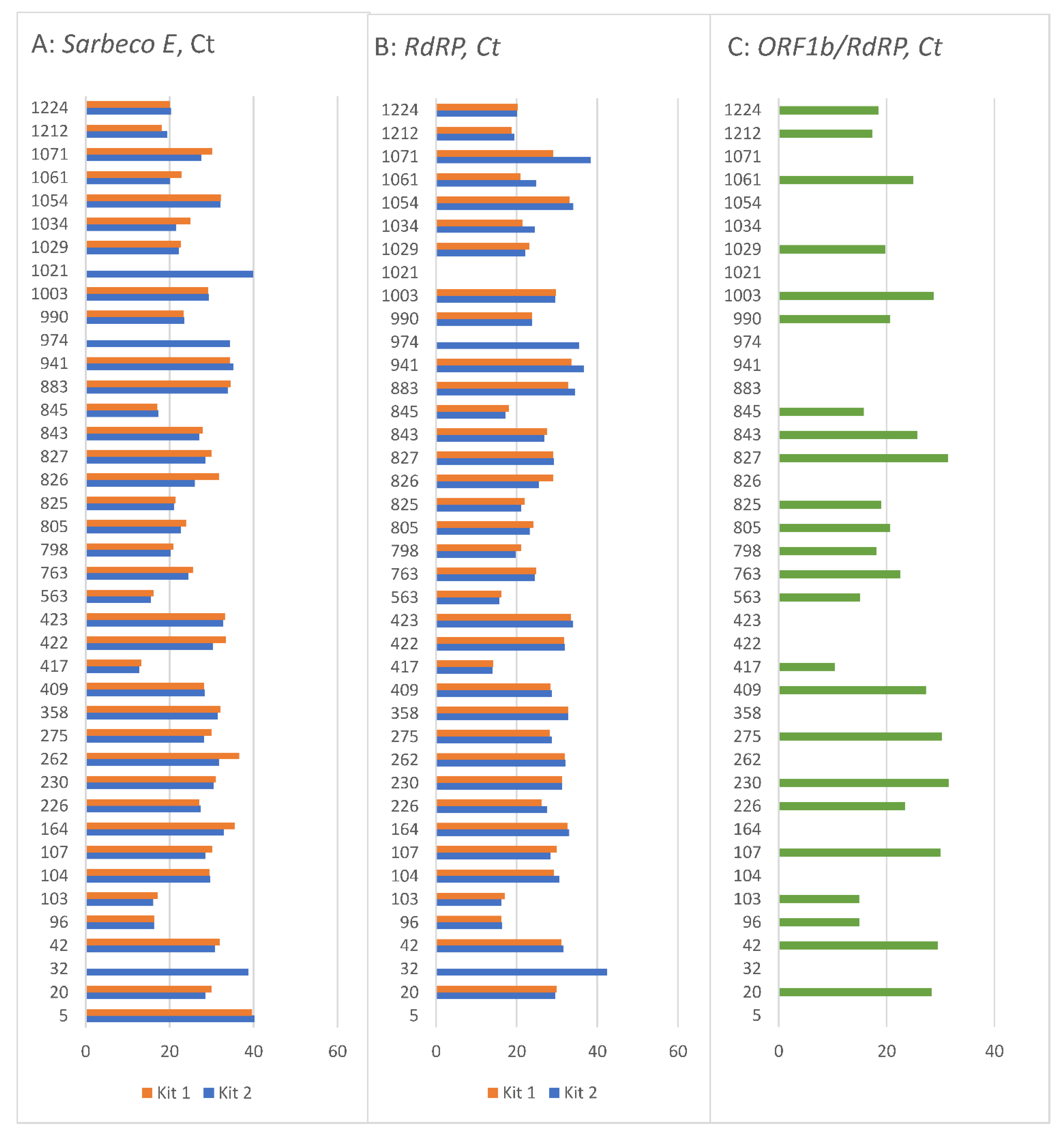
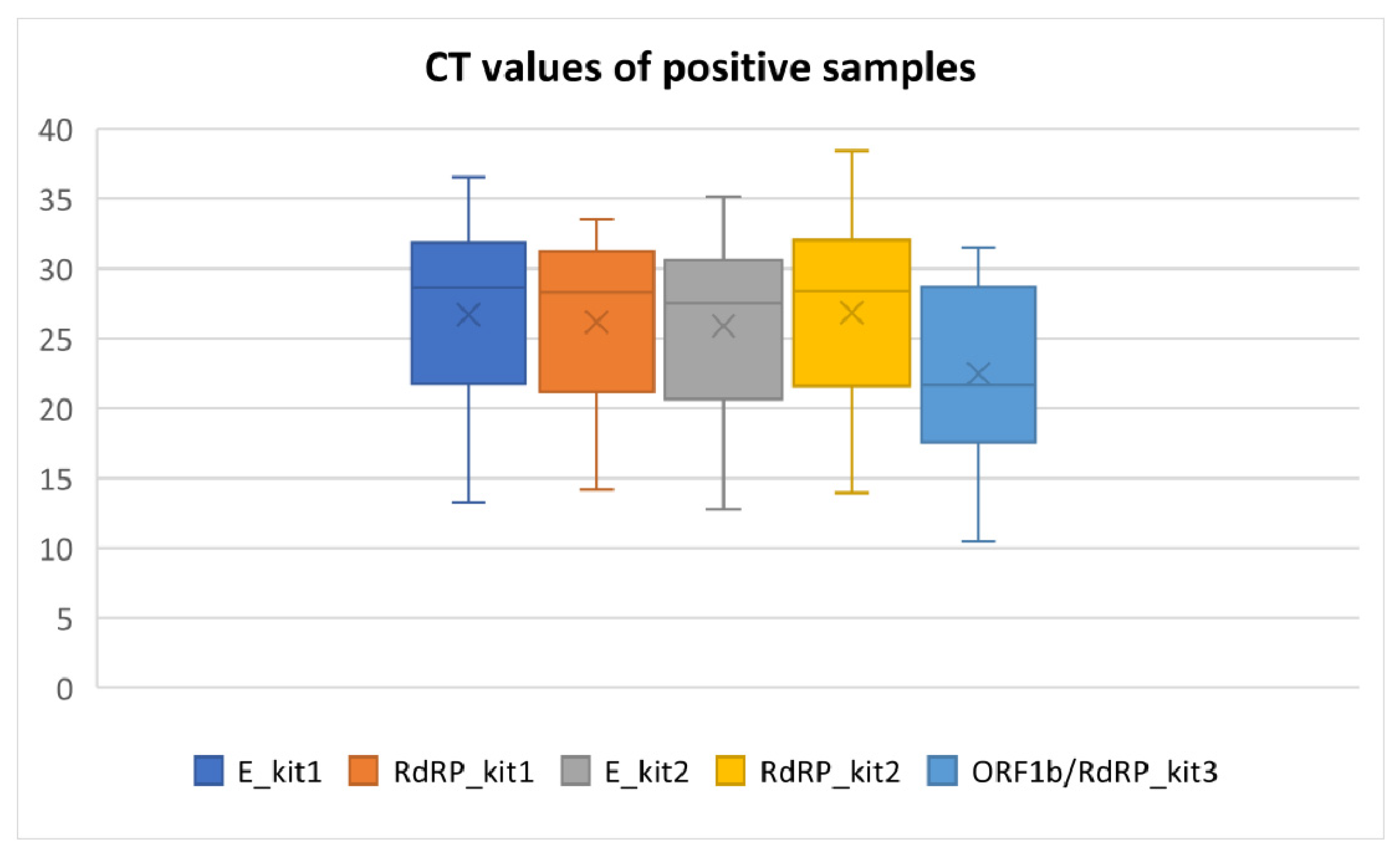
2.2. SARS-CoV-2 RT-qPCR Testing
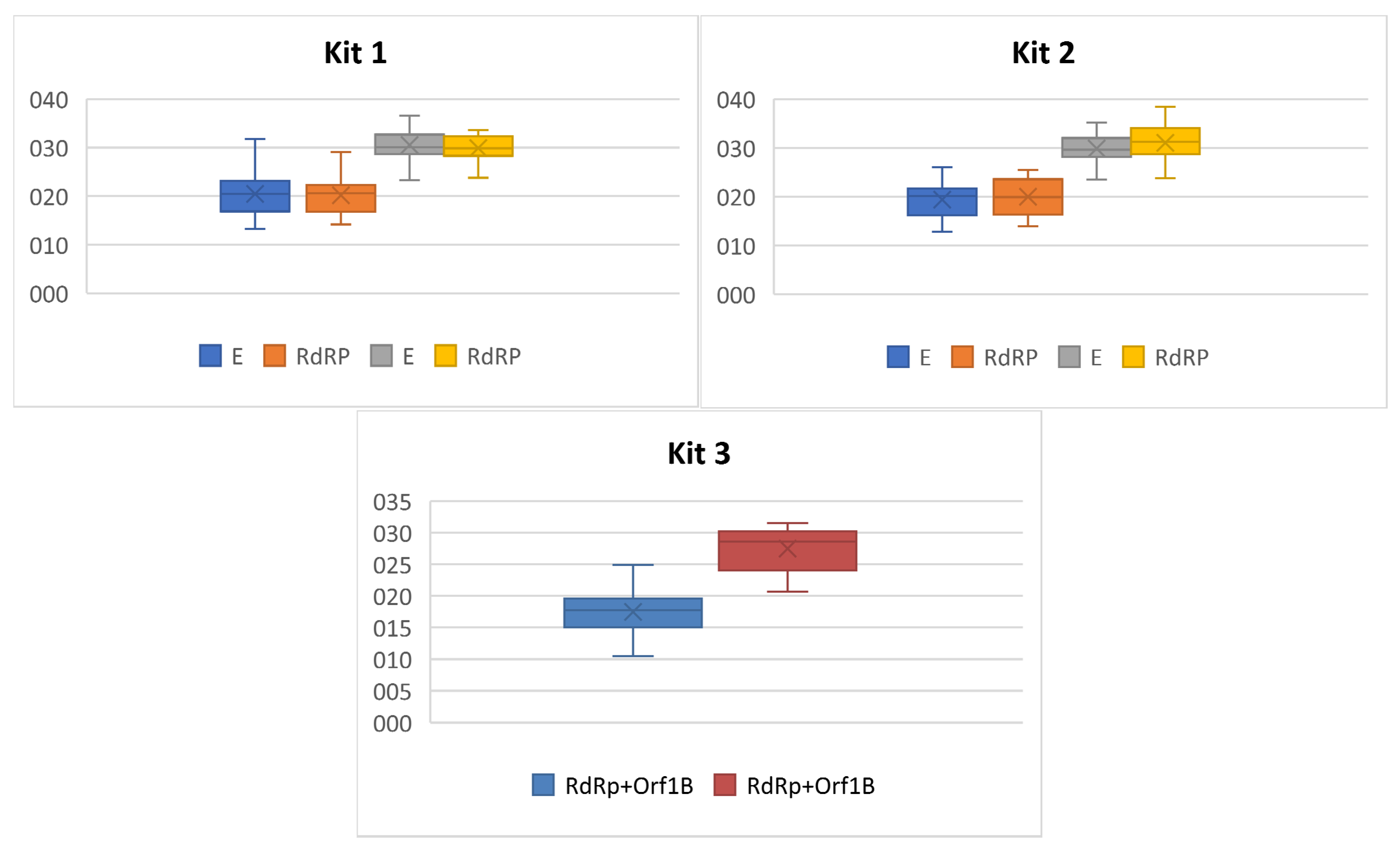
2.3. Antigen and RT-qPCR Testing
3. Discussion
3.1. Antigen Testing
3.2. RT-qPCR and Ct Values
4. Materials and Methods
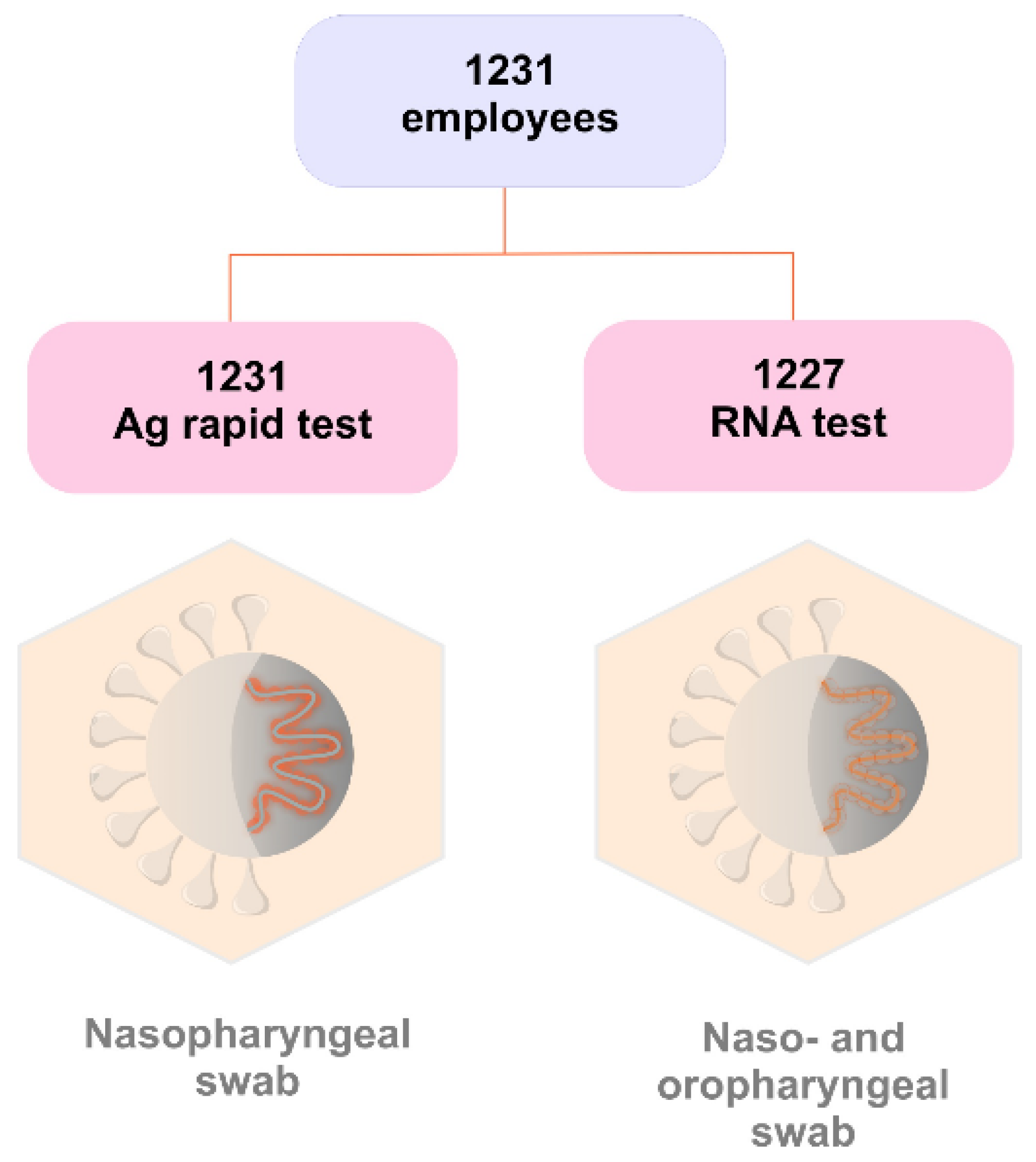
4.1. Subjects and Sampling
4.2. Antigen Testing
4.3. RNA Isolation
4.4. RT-qPCR Testing by Three Different CE IVD Kits
4.5. Statistical Analyses
5. Conclusions
- The results confirmed that the Standard Q COVID-19 Ag test (SD Biosensor) has an advantage in its ability to detect people with lower Ct values, who can be assumed to have higher viral load and thus pose the highest risk of virus transmission.
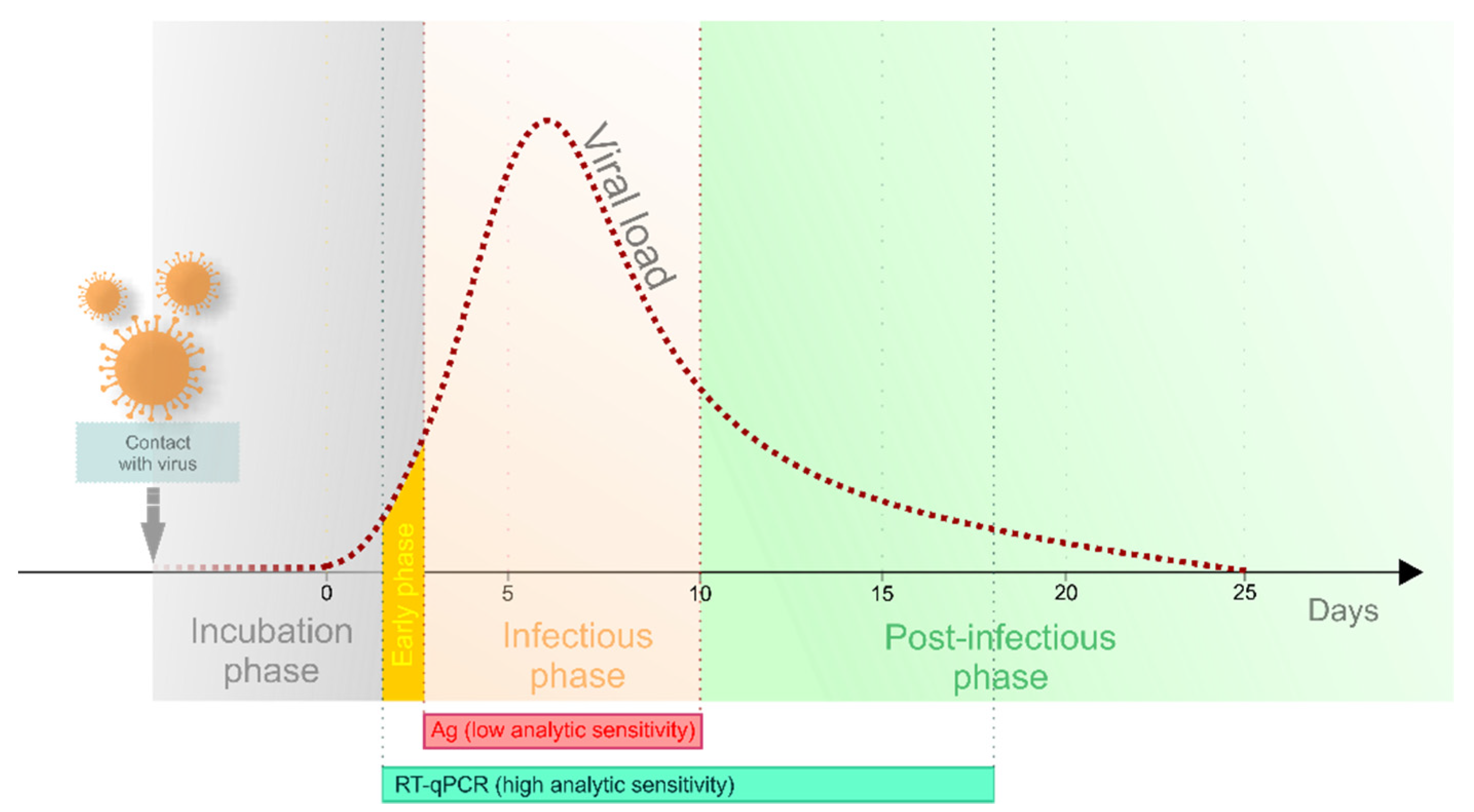
- The relatively high number of false-negative results from the antigen test increases the risk of silent virus shedding in the population. If used in mass testing, thousands of individuals could receive incorrect results and proceed to spread the virus, especially if tested at an early phase of viral infection.
- The antigen test is therefore time-limited, and its utilisation in blanket population screening should be re-considered given that the benefit vs. risk ratio is questionable.
- The sensitivity and specificity of an antigen test compared to the gold standard RT-qPCR testing is not accurate unless RT-qPCR sensitivity limits are included in the algorithm.
- Providing row Ct values is not sufficient. We proved that one sample can have variable Ct values if different assays are used. Moreover, the same Ct value of kits with different sensitivity represent a discrepant amount of virus copies (even in the thousands). Additionally, identical Ct detected by one kit can have different infectivity aspects depending on the disease phase.
- The algorithm for RT-PCR testing should also calculate actual health status, and if an early phase is suspected, retesting should be considered in the cases when Ct was detected above the threshold resulting in a negative result.
- Clear guidelines for pre-analytical, analytical and post-analytical steps, including chemistry quality, are needed to uniform the testing.
- Normalisation of Ct values by standard dilution curve, counting virus copies could allow inter-kit comparison between laboratories and epidemiological monitoring.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| B2M | the gene encoding human beta-2-microglobulin |
| COVID-19 | coronavirus disease 2019, the official name for the disease caused by the virus |
| Ct | cycle threshold |
| E gene | the gene encoding the small membrane envelope protein of the SARS-CoV-2 virus |
| LOD | limit of detection |
| NPV | negative predictive value |
| ORF1B | gene encoding open-reading frame 1b of the SARS-CoV-2 virus |
| PPV | positive predictive value |
| RdRP gene | the gene encoding the RNA-dependent RNA polymerase of the SARS-CoV-2 virus |
| RNase P | the gene encoding human nuclear ribonuclease P |
| RT-qPCR | quantitative reverse transcription PCR |
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus 2, the official name for the virus causing the disease |
References
- Coronaviridae Study Group of the International Committee on Taxonomy of Viruses. The species Severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020, 5, 536–544. [Google Scholar] [CrossRef] [Green Version]
- Payne, S. Family Coronaviridae. Viruses 2017, 149–158. [Google Scholar] [CrossRef]
- Araf, Y.; Faruqui, N.A.; Anwar, S.; Hosen, M.J. SARS-CoV-2: A New Dimension to Our Understanding of Coronaviruses. Int. Microbiol. 2020, 24, 19–24. [Google Scholar] [CrossRef]
- Ur Rehman, M.F.; Fariha, C.; Anwar, A.; Shahzad, N.; Ahmad, M.; Mukhtar, S.; Farhan Ul Haque, M. Novel Coronavirus Disease (COVID-19) Pandemic: A Recent Mini Review. Comput. Struct. Biotechnol. J. 2021, 19, 612–623. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Hu, G.; Wang, Y.; Zhao, X.; Ji, F.; Ren, W.; Gong, M.; Ju, X.; Li, C.; Hong, J.; et al. Functional and Genetic Analysis of Viral Receptor Ace2 Orthologs Reveals a Broad Potential Host Range of Sars-Cov-2. Proc. Natl. Acad. Sci. USA 2020, 118, e2025373118. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Liu, Q.; Guo, D. Emerging Coronaviruses: Genome Structure, Replication, and Pathogenesis. J. Med Virol. 2020, 92, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Kumar, D.; Batra, L.; Malik, M.T. Insights of Novel Coronavirus(Sars-Cov-2) Disease Outbreak, Management and Treatment. AIMS Microbiol. 2020, 6, 183–203. [Google Scholar] [CrossRef]
- MacLean, O.A.; Lytras, S.; Weaver, S.; Singer, J.B.; Boni, M.F.; Lemey, P.; Kosakovsky Pond, S.L.; Robertson, D.L. Natural Selection in the Evolution of SARS-CoV-2 in of SARS-CoV-2 in Bats Created a Generalist Virus and Highly Capable Human Pathogen. PLoS Biol. 2021, 19, e3001115. [Google Scholar] [CrossRef] [PubMed]
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 1 April 2021).
- WHO Coronavirus (COVID-19) Dashboard_Global_Slovakia. Available online: https://covid19.who.int/region/euro/country/sk (accessed on 1 April 2021).
- Jeong, E.; Hagose, M.; Jung, H.; Ki, M.; Flahault, A. Understanding South Korea’s Response to the COVID-19 Outbreak: A Real-Time Analysis. Int. J. Environ. Res. Public Health 2020, 17, 9571. [Google Scholar] [CrossRef] [PubMed]
- Pavelka, M.; Van-Zandvoort, K.; Abbott, S.; Sherratt, K.; Majdan, M.; Jarčuška, P.; Krajčí, M.; Flasche, S.; Funk, S. The Effectiveness of Population-Wide, Rapid Antigen Test Based Screening in Reducing SARS-CoV-2 Infection Prevalence in Slovakia. Science 2021, 372, 635–641. [Google Scholar] [CrossRef]
- Frnda, J.; Durica, M. On Pilot Massive COVID-19 Testing by Antigen Tests in Europe. Case Study: Slovakia. Infect. Dis. Rep. 2021, 13, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus Update (Live): Cases and Deaths from COVID-19 Virus Pandemic. Available online: https://www.worldometers.info/coronavirus/country/slovakia/#graph-cases-daily (accessed on 1 April 2021).
- Davies, N.G.; Abbott, S.; Barnard, R.C.; Jarvis, C.I.; Kucharski, A.J.; Munday, J.D.; Pearson, C.A.B.; Russell, T.W.; Tully, D.C.; Washburne, A.D.; et al. Estimated Transmissibility and Impact of SARS-CoV-2 Lineage B.1.1.7 in England. Science 2021, 372, eabg3055. [Google Scholar] [CrossRef] [PubMed]
- Challen, R.; Brooks-Pollock, E.; Read, J.M.; Dyson, L.; Tsaneva-Atanasova, K.; Danon, L. Risk of Mortality in Patients Infected with SARS-CoV-2 Variant of Concern 202012/1: Matched Cohort Study. BMJ 2021, 372, n579. [Google Scholar] [CrossRef] [PubMed]
- Thommes, L.; Burkert, F.R.; Öttl, K.-W.; Goldin, D.; Loacker, L.; Lanser, L.; Griesmacher, A.; Theurl, I.; Weiss, G.; Bellmann-Weiler, R. Comparative Evaluation of Four SARS-CoV-2 Antigen Tests in Hospitalized Patients. Int. J. Infect. Dis. 2021, 105, 144–146. [Google Scholar] [CrossRef]
- Saeed, U.; Uppal, S.R.; Piracha, Z.Z.; Rasheed, A.; Aftab, Z.; Zaheer, H.; Uppal, R. Evaluation of SARS-CoV-2 Antigen-Based Rapid Diagnostic Kits in Pakistan: Formulation of COVID-19 National Testing Strategy. Virol. J. 2021, 18, 34. [Google Scholar] [CrossRef]
- Mak, G.C.; Lau, S.S.; Wong, K.K.; Chow, N.L.; Lau, C.S.; Lam, E.T.; Chan, R.C.; Tsang, D.N. Analytical Sensitivity and Clinical Sensitivity of the Three Rapid Antigen Detection Kits for Detection of SARS-CoV-2 Virus. J. Clin. Virol. 2020, 133, 104684. [Google Scholar] [CrossRef] [PubMed]
- Eftekhari, A.; Alipour, M.; Chodari, L.; Dizaj, S.M.; Ardalan, M.R.; Samiei, M.; Sharifi, S.; Vahed, S.Z.; Huseynova, I.; Khalilov, R.; et al. A Comprehensive Review of Detection Methods for SARS-CoV-2. Microorganisms 2021, 9, 232. [Google Scholar] [CrossRef]
- Alpdagtas, S.; Ilhan, E.; Uysal, E.; Sengor, M.; Ustundag, C.B.; Gunduz, O. Evaluation of Current Diagnostic Methods for COVID-19. APL Bioeng. 2020, 4, 041506. [Google Scholar] [CrossRef]
- Carter, L.J.; Garner, L.V.; Smoot, J.W.; Li, Y.; Zhou, Q.; Saveson, C.J.; Sasso, J.M.; Gregg, A.C.; Soares, D.J.; Beskid, T.R.; et al. Assay Techniques and Test Development for COVID-19 Diagnosis. ACS Cent. Sci. 2020, 6, 591–605. [Google Scholar] [CrossRef]
- Antigen Detection in the Diagnosis of SARS-CoV-2 Infection Using Rapid Immunoassays. Interim Guidance. Available online: https://www.who.int/publications/i/item/antigen-detection-in-the-diagnosis-of-sars-cov-2infection-using-rapid-immunoassays (accessed on 27 March 2021).
- Benzigar, M.R.; Bhattacharjee, R.; Baharfar, M.; Liu, G. Current Methods for Diagnosis of Human Coronaviruses: Pros and Cons. Anal. Bioanal. Chem. 2020, 413, 2311–2330. [Google Scholar] [CrossRef]
- La Marca, A.; Capuzzo, M.; Paglia, T.; Roli, L.; Trenti, T.; Nelson, S.M. Testing for SARS-CoV-2 (COVID-19): A Systematic Review and Clinical Guide to Molecular and Serological in-Vitro Diagnostic Assays. Reprod. Biomed. Online 2020, 41, 483–499. [Google Scholar] [CrossRef] [PubMed]
- West, R.; Kobokovich, A.; Connell, N.; Gronvall, G.K. COVID-19 Antibody Tests: A Valuable Public Health Tool with Limited Relevance to Individuals. Trends Microbiol. 2021, 29, 214–223. [Google Scholar] [CrossRef] [PubMed]
- Cevik, M.; Kuppalli, K.; Kindrachuk, J.; Peiris, M. Virology, Transmission, and Pathogenesis of SARS-CoV-2. BMJ 2020, 371, m3862. [Google Scholar] [CrossRef] [PubMed]
- Falzone, L.; Musso, N.; Gattuso, G.; Bongiorno, D.; Palermo, C.I.; Scalia, G.; Libra, M.; Stefani, S. Sensitivity Assessment of Droplet Digital PCR for SARS-CoV-2 Detection. Int. J. Mol. Med. 2020, 46, 957–964. [Google Scholar] [CrossRef] [PubMed]
- Crozier, A.; Rajan, S.; Buchan, I.; McKee, M. Put to the Test: Use of Rapid Testing Technologies for Covid-19. BMJ 2021, 372, n208. [Google Scholar] [CrossRef]
- COVID AUTOMAT.Systém Pre Monitorovanie Vývoja Epidémie A Prijímanie Protiepidemických Opatrenia V Závislosti Od Intenzity Šírenia SARS-CoV-2 (COVID-19). Available online: https://www.minv.sk/?tlacove-spravy&sprava=covid-automat-pravidla-a-vynimky-zo-zakazu-vychadzania-ucinne-od-25-marca (accessed on 27 March 2021).
- Národné Centrum Zdravotníckych Informácií. Available online: https://covid-19.nczisk.sk/sk (accessed on 13 May 2021).
- Guglielmi, G. Rapid Coronavirus Tests: A Guide for the Perplexed. Nature 2021, 590, 202–205. [Google Scholar] [CrossRef]
- Trunfio, M.; Venuti, F.; Alladio, F.; Longo, B.M.; Burdino, E.; Cerutti, F.; Ghisetti, V.; Bertucci, R.; Picco, C.; Bonora, S.; et al. Diagnostic SARS-CoV-2 Cycle Threshold Value Predicts Disease Severity, Survival, and Six-Month Sequelae in COVID-19 Symptomatic Patients. Viruses 2021, 13, 281. [Google Scholar] [CrossRef]
- Rao, S.N.; Manissero, D.; Steele, V.R.; Pareja, J. A Narrative Systematic Review of the Clinical Utility of Cycle Threshold Values in the Context of COVID-19. Infect. Dis. Ther. 2020, 9, 573–586. [Google Scholar] [CrossRef]
- Choudhuri, J.; Carter, J.; Nelson, R.; Skalina, K.; Osterbur-Badhey, M.; Johnston, A.; Goldstein, D.; Paroder, M.; Szymanski, J. SARS-CoV-2 PCR Cycle Threshold at Hospital Admission Associated with Patient Mortality. PLoS ONE 2020, 15, e0244777. [Google Scholar] [CrossRef]
- Bryan, A.; Fink, S.L.; Gattuso, M.A.; Pepper, G.; Chaudhary, A.; Wener, M.H.; Morishima, C.; Jerome, K.R.; Mathias, P.C.; Greninger, A.L. SARS-CoV-2 Viral Load on Admission Is Associated with 30-Day Mortality. Open Forum Infect. Dis. 2020, 7, ofaa535. [Google Scholar] [CrossRef] [PubMed]
- Yu, F.; Yan, L.; Wang, N.; Yang, S.; Wang, L.; Tang, Y.; Gao, G.; Wang, S.; Ma, C.; Xie, R.; et al. Quantitative Detection and Viral Load Analysis of SARS-CoV-2 in Infected Patients. Clin. Infect. Dis. 2020, 71, 793–798. [Google Scholar] [CrossRef] [Green Version]
- Watson, J.; Whiting, P.F.; Brush, J.E. Interpreting a Covid-19 Test Result. BMJ 2020, 369, m1808. [Google Scholar] [CrossRef]
- Binnicker, M.J. Challenges and Controversies to Testing for COVID-19. J. Clin. Microbiol. 2020, 58, e01695-20. [Google Scholar] [CrossRef]
- Dahdouh, E.; Lázaro-Perona, F.; Romero-Gómez, M.P.; Mingorance, J.; García-Rodriguez, J. Ct Values from SARS-CoV-2 Diagnostic PCR Assays Should Not Be Used as Direct Estimates of Viral Load. J. Infect. 2020, 82, 414–451. [Google Scholar] [CrossRef]
- Gaston, D.C.; Malinis, M.; Osborn, R.; Peaper, D.R.; Landry, M.; Juthani-Mehta, M.; Azar, M.M. Clinical Implications of SARS-CoV-2 Cycle Threshold Values in Solid Organ Transplant Recipients. Am. J. Transplant. 2020, 21, 1304–1311. [Google Scholar] [CrossRef]
- Zhang, Z.; Bi, Q.; Fang, S.; Wei, L.; Wang, X.; He, J.; Wu, Y.; Liu, X.; Gao, W.; Zhang, R.; et al. Insight into the Practical Performance of RT-PCR Testing for SARS-CoV-2 Using Serological Data: A Cohort Study. Lancet Microbe. 2021, 2, e79–e87. [Google Scholar] [CrossRef]
- Payne, D.; Newton, D.; Evans, P.; Osman, H.; Baretto, R. Preanalytical issues affecting the diagnosis of COVID-19. J. Clin. pathol. 2021, 74, 207–208. [Google Scholar] [CrossRef] [PubMed]
- Engelmann, I.; Alidjinou, E.K.; Ogiez, J.; Pagneux, Q.; Miloudi, S.; Benhalima, I.; Ouafi, M.; Sane, F.; Hober, D.; Rousswel, A.; et al. Preanalytical Issues and Cycle Threshold Values in SARS-CoV-2 Real-Time RT-PCR Testing: Should Test Results Include These? ACS Omega 2021, 6, 6528–6536. [Google Scholar] [CrossRef]
- Shah, S.; Singhal, T.; Davar, N.; Thakkar, P. No Correlation between Ct Values and Severity of Disease or Mortality in Patients with COVID 19 Disease. Indian J. Med. Microbiol. 2020, 39, 116. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Hu, M.; Ren, Y.; Xu, X.; Wang, Z.; Lyu, X.; Wu, W.; Li, Z.; Gong, X.; Xiang, Z.; et al. Evaluation of Seven Commercial SARS-CoV-2 RNA Detection Kits Based on Real-Time Polymerase Chain Reaction(PCR) in China. Clin. Chem. Lab. Med. 2020, 58, e149–e153. [Google Scholar] [CrossRef]
- Reijns, M.A.M.; Thompson, L.; Acosta, J.C.; Black, H.A.; Sanchez-Luque, F.J.; Diamond, A.; Parry, D.A.; Daniels, A.; O’Shea, M.; Uggenti, C.; et al. A Sensitive and Affordable Multiplex RT-QPCR Assay for SARS-CoV-2 Detection. PLoS Biol. 2020, 18, e3001030. [Google Scholar] [CrossRef]
- Marinowic, D.R.; Zanirati, G.; Rodrigues, F.V.F.; Grahl, M.V.C.; Alcará, A.M.; Machado, D.C.; Da Costa, J.C. A New SYBR Green Real-Time PCR to Detect SARS-CoV-2. Sci. Rep. 2021, 11, 2224. [Google Scholar] [CrossRef] [PubMed]
- Kudo, E.; Israelow, B.; Vogels, C.B.F.; Lu, P.; Wyllie, A.L.; Tokuyama, M.; Venkataraman, A.; Brackney, D.E.; Ott, I.M.; Petrone, M.E.; et al. Detection of SARS-CoV-2 RNA by Multiplex RTqPCR. PLoS Biol. 2020, 18, e3000867. [Google Scholar] [CrossRef] [PubMed]
- Barreto, H.G.; de Pádua Milagres, F.A.; de Araújo, G.C.; Daúde, M.M.; Benedito, V.A. Diagnosing the Novel SARS-CoV-2 by Quantitative RT-PCR: Variations and Opportunities. J. Mol. Med. 2020, 98, 1727–1736. [Google Scholar] [CrossRef]
- Jang, W.S.; Lim, D.H.; Yoon, J.; Kim, A.; Lim, M.; Nam, J.; Yanagihara, R.; Ryu, S.-W.; Jung, B.K.; Ryoo, N.-H.; et al. Development of a Multiplex Loop-Mediated Isothermal Amplification(LAMP) Assay for on-Site Diagnosis of SARS CoV-2. PLoS ONE 2021, 16, e0248042. [Google Scholar] [CrossRef]
- Han, M.S.; Byun, J.H.; Cho, Y.; Rim, J.H. RT-PCR for SARS-CoV-2: Quantitative versus qualitative. Lancet Infect. Dis. 2021, 21, 165. [Google Scholar] [CrossRef]
- Schnuriger, A.; Perrier, M.; Marinho, V.; Michel, Y.; Saloum, K.; Boukli, N.; Lambert-Niclot, S.; Amiel, C.; Fofana, D.B.; Gozlan, J.; et al. Caution in interpretation of SARS-CoV-2 quantification based on RT-PCR cycle threshold value. Diagn. Microbiol. Infect. Dis. 2021, 100, 115366. [Google Scholar] [CrossRef] [PubMed]
- Tom, M.R.; Mina, M.J. To interpret the SARS-CoV-2 test, consider the cycle threshold value. Clin. Infect. Dis. 2020, 71, 2252–2254. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Targeted Genes | |||||
|---|---|---|---|---|---|
| Kit 1 | Kit 2 | Kit 3 | |||
| E | RdRP | E | RdRP | ORF1b/RdRP | |
| n | 36 | 36 | 37 | 37 | 24 |
| Median | 28.64 | 28.28 | 27.51 | 28.36 | 21.65 |
| Mean | 26.70 | 26.17 | 25.89 | 26.84 | 22.47 |
| SD | 6.30 | 5.81 | 6.03 | 6.53 | 6.21 |
| Min | 13.24 | 14.16 | 12.80 | 13.96 | 10.45 |
| Max | 36.55 | 33.54 | 35.12 | 38.42 | 31.50 |
| Kit 1 | Kit 2 | Kit 3 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Ag + | Ag − | Ag + | Ag − | Ag + | Ag − | |||||
| E | RdRP | E | RdRP | E | RdRP | E | RdRP | ORF1b/RdRP | ORF1b/RdRP | |
| n | 14 | 14 | 22 | 22 | 14 | 14 | 23 | 23 | 12 | 12 |
| median | 20.48 | 20.61 | 30.14 | 29.92 | 20.10 | 19.90 | 29.62 | 31.20 | 17.77 | 28.59 |
| mean | 20.47 | 20.16 | 30.67 | 30.00 | 19.37 | 19.99 | 29.86 | 31.01 | 17.47 | 27.47 |
| SD | 4.71 | 3.86 | 3.19 | 2.77 | 3.46 | 3.73 | 2.97 | 3.68 | 3.64 | 3.59 |
| min | 13.24 | 14.16 | 23.31 | 23.76 | 12.80 | 13.96 | 23.52 | 23.74 | 10.45 | 20.70 |
| max | 31.80 | 29.03 | 36.55 | 33.54 | 26.00 | 25.45 | 35.12 | 38.42 | 24.92 | 31.50 |
| Kit 1 | Kit 2 | Kit 3 | |
|---|---|---|---|
| Kit Name | vDetect COVID-19 RT-qPCR Diagnostic Kit | gb SARS-CoV-2 Multiplex | Genvinset COVID-19 [E] kit |
| Company | MultiplexDX, Slovak republic | GENERI BIOTECH s.r.o., Czech republic | BDR Diagnostics, Spain |
| Targeted genes | E, RdRP | E, RdRP | ORF1b + RdRP |
| Control gene | RNase P | B2M | RNase P |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dankova, Z.; Novakova, E.; Skerenova, M.; Holubekova, V.; Lucansky, V.; Dvorska, D.; Brany, D.; Kolkova, Z.; Strnadel, J.; Mersakova, S.; et al. Comparison of SARS-CoV-2 Detection by Rapid Antigen and by Three Commercial RT-qPCR Tests: A Study from Martin University Hospital in Slovakia. Int. J. Environ. Res. Public Health 2021, 18, 7037. https://doi.org/10.3390/ijerph18137037
Dankova Z, Novakova E, Skerenova M, Holubekova V, Lucansky V, Dvorska D, Brany D, Kolkova Z, Strnadel J, Mersakova S, et al. Comparison of SARS-CoV-2 Detection by Rapid Antigen and by Three Commercial RT-qPCR Tests: A Study from Martin University Hospital in Slovakia. International Journal of Environmental Research and Public Health. 2021; 18(13):7037. https://doi.org/10.3390/ijerph18137037
Chicago/Turabian StyleDankova, Zuzana, Elena Novakova, Maria Skerenova, Veronika Holubekova, Vincent Lucansky, Dana Dvorska, Dusan Brany, Zuzana Kolkova, Jan Strnadel, Sandra Mersakova, and et al. 2021. "Comparison of SARS-CoV-2 Detection by Rapid Antigen and by Three Commercial RT-qPCR Tests: A Study from Martin University Hospital in Slovakia" International Journal of Environmental Research and Public Health 18, no. 13: 7037. https://doi.org/10.3390/ijerph18137037
APA StyleDankova, Z., Novakova, E., Skerenova, M., Holubekova, V., Lucansky, V., Dvorska, D., Brany, D., Kolkova, Z., Strnadel, J., Mersakova, S., Janikova, K., Samec, M., Pokusa, M., Petras, M., Sarlinova, M., Kasubova, I., Loderer, D., Sadlonova, V., Kompanikova, J., ... Halasova, E. (2021). Comparison of SARS-CoV-2 Detection by Rapid Antigen and by Three Commercial RT-qPCR Tests: A Study from Martin University Hospital in Slovakia. International Journal of Environmental Research and Public Health, 18(13), 7037. https://doi.org/10.3390/ijerph18137037