
Improvement in the Cognitive Aspects of Cultural Competence after Short-Term Overseas Study Programs


Abstract
:1. Introduction
1.1. Effects of Overseas Study Experiences on Cultural Competence
1.2. Essential Factors Affecting Cultural Competence
1.3. The Present Study
2. Materials and Methods
2.1. Participants
2.2. Overseas Study Programs
2.3. Measure Instrument
2.4. Research Procedure: Ethical Approval and Participants’ Recruitment
2.5. Statistical Analysis
3. Results
3.1. Demographic Data
3.2. Data of Cultural Competence
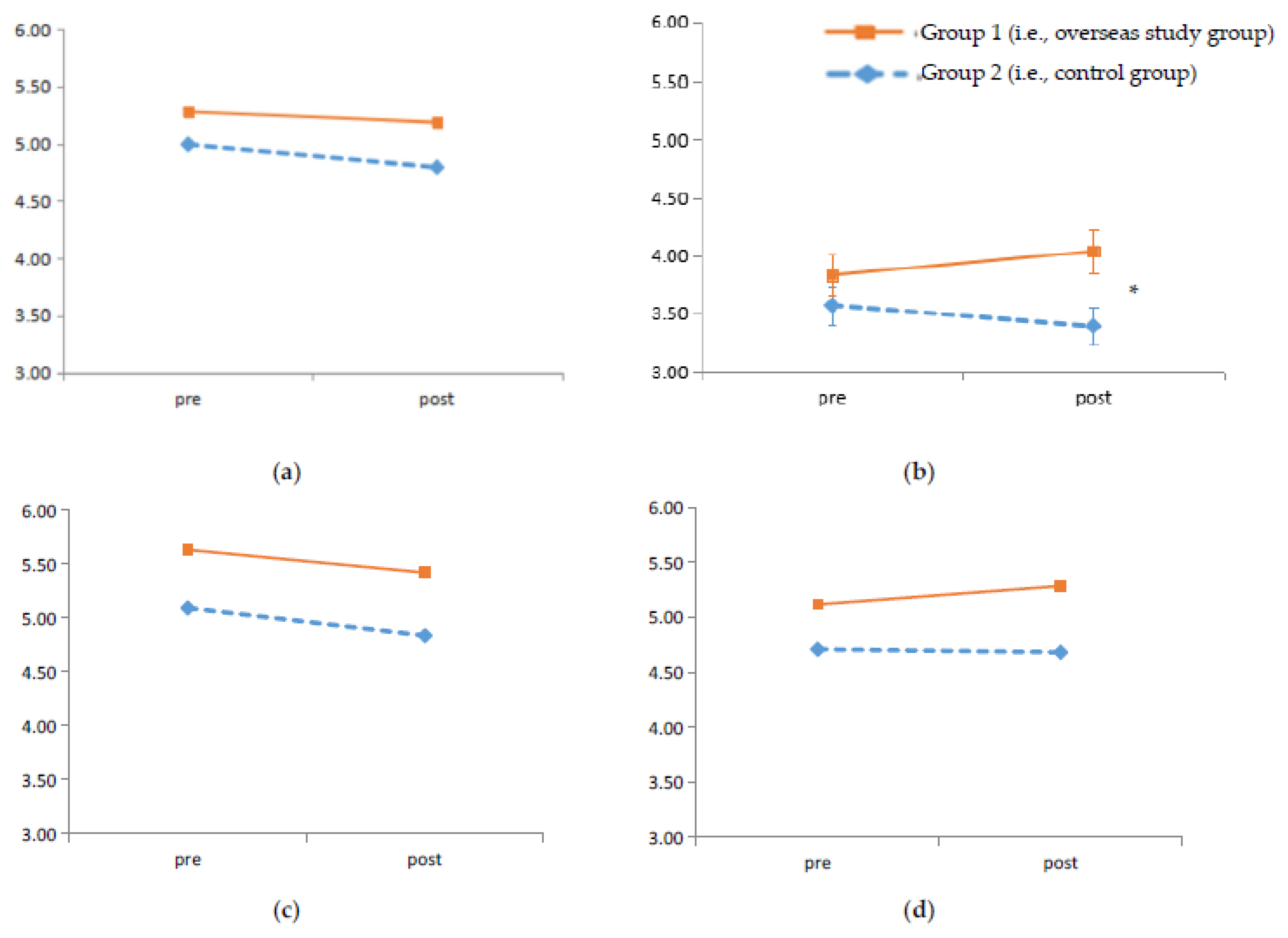
3.3. ANCOVA Analysis
4. Discussion
4.1. Effect of Short-Term Overseas Study Programs on Cultural Competence
4.2. Decreased Scores of Cultural Competence
4.3. Theoretical and Practical Implications
4.4. Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Health and Medical Research Council. Cultural Competency in Health: A Guide for Policy, Partnerships and Participation; National Health and Medical Research Council: Canberra, Australia, 2006; p. 7.
- Earley, P.C.; Ang, S. Cultural Intelligence: Individual Interactions across Cultures; Stanford University Press: Palo Alto, CA, USA, 2003. [Google Scholar]
- Fantini, A.; Tirmizi, A. Exploring and Assessing Intercultural Competence; World Learning Publications: Brattleboro, VT, USA, 2006; Volume 1. [Google Scholar]
- Flynn, P.M.; Betancourt, H.; Emerson, N.D.; Nunez, E.I.; Nance, C.M. Health professional cultural competence reduces the psychological and behavioral impact of negative healthcare encounters. Cul. Divers. Ethn. Min. 2019, 26, 1–9. [Google Scholar] [CrossRef]
- Campinha-Bacote, J. The Process of Cultural Competence in the Delivery of Healthcare Services: The Journey Continues; Transcultural CARE Associates: Blue Ash, OH, USA, 2007. [Google Scholar]
- Betancourt, J.R.; Green, A.R.; Carrillo, J.E.; Ananeh-Firempong, O. Defining cultural competence: A practical framework for addressing racial/ethnic disparities in health and health care. Public Health Rep. 2003, 118, 293–302. [Google Scholar] [CrossRef]
- Williams, D.R.; Mohammed, S.A. Discrimination and racial disparities in health: Evidence and needed research. J. Behav. Med. 2009, 32, 20–47. [Google Scholar] [CrossRef] [Green Version]
- Caffrey, R.A.; Neander, W.; Markle, D.; Stewart, B. Improving the cultural competence of nursing students: Results of integrating cultural content in the curriculum and an international immersion experience. J. Nurs. Educ. 2005, 44, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Australian Government|Department of Education, Skills and Employment. Australian Students Studying Overseas 2018 Survey Data Tables. Available online: https://internationaleducation.gov.au/research/australianstudentsoverseas/pages/australians-students-overseas.aspx (accessed on 18 June 2021).
- Chae, D.; Kim, J.; Kim, S.; Lee, J.; Park, S. Effectiveness of cultural competence educational interventions on health professionals and patient outcomes: A systematic review. Jpn. J. Nurs. Sci. 2020, 17, e12326. [Google Scholar] [CrossRef]
- Beach, M.C.; Price, E.G.; Gary, T.L.; Robinson, K.A.; Gozu, A.; Palacio, A.; Smarth, C.; Jenckes, M.W.; Feuerstein, C.; Bass, E.B.; et al. Cultural competence—A systematic review of health care provider educational interventions. Med. Care. 2005, 43, 356–373. [Google Scholar] [CrossRef]
- Institute of International Education. Detailed Duration of U.S. Study Abroad, 2005/06–2018/19. Open Doors Report on International Educational Exchange. Available online: https://opendoorsdata.org/data/us-study-abroad/duration-of-study-abroad/ (accessed on 18 June 2021).
- Baker, D.K.; Aǧar, E. International Summer Engineering Program on fuel cells for undergraduate engineering students. Int. J. Hydrogen Energy 2011, 36, 3712–3725. [Google Scholar] [CrossRef]
- Tarrant, M.; Lyons, K. The effect of short-term educational travel programs on environmental citizenship. Environ. Educ. Res. 2012, 18, 403–416. [Google Scholar] [CrossRef]
- Holmes, D.; Zayas, L.E.; Koyfman, A. Student objectives and learning experiences in a global health elective. J. Commun. Health 2012, 37, 927–934. [Google Scholar] [CrossRef]
- Long, T. Influence of international service-learning on nursing student self-efficacy toward cultural competence. J. Nurs. Educ. 2014, 53, 474–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amerson, R. The impact of service-learning on cultural competence. Nurs. Educ. Pers. 2010, 31, 18–22. [Google Scholar]
- Werremeyer, A.B.; Skoy, E.T. A Medical Mission to Guatemala as an Advanced Pharmacy Practice Experience. Am. J. Pharm. Educ. 2012, 76, 156. [Google Scholar] [CrossRef]
- Gower, S.; Duggan, R.; Dantas, J.; Boldy, D. One Year On: Cultural Competence of Australian Nursing Students Following International Service-Learning. J. Nurs. Educ. 2019, 58, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, F.; Stegmann, K.; Siebeck, M. Promoting medical competencies through international exchange programs: Benefits on communication and effective doctor-patient relationships. BMC Med. Educ. 2014, 14, 43. [Google Scholar] [CrossRef] [Green Version]
- Australian Government|Department of Foreign Affairs and Trade. About New Colombo Plan; 2021. Available online: https://www.dfat.gov.au/people-to-people/new-colombo-plan/about (accessed on 18 June 2021).
- Earnest, D.R.; Rosenbusch, K.; Wallace-Williams, D.; Keim, A.C. Study abroad in psychology: Increasing cultural competencies through experiential learning. Teach. Psychol. 2016, 43, 75–79. [Google Scholar] [CrossRef]
- Keane, E.; Provident, I. Combining online education with international service learning to increase cultural competence. Int. J. Allied Health Sci. Pract. 2017, 15, 7. [Google Scholar]
- Larson, K.L.; Ott, M.; Miles, J.M. International cultural immersion: En Vivo reflections in cultural competence. J. Cult. Divers. 2010, 17, 44–50. [Google Scholar]
- Charles, L.; Maltby, H.; Abrams, S.; Shea, J.; Brand, G.; Nicol, P. Expanding worldview: Australian nursing students’ experience of cultural immersion in India. Contemp. Nurs. 2014, 48, 67–75. [Google Scholar] [CrossRef]
- Coatsworth, K.; Hurley, J.; Miller-Rosser, K. A phenomenological study of student nurses volunteering in Nepal: Have their experiences altered their understanding of nursing? Collegian 2017, 24, 339–344. [Google Scholar] [CrossRef] [Green Version]
- Reid-Searl, K.; Dwyer, T.; Moxham, L.; Happell, B.; Sander, T. Rediscovering the essence of nursing: Exploring the impact of in clinical experience in Thailand for undergraduate nursing students from Australia. Nurs. Educ. Today 2011, 31, 892–897. [Google Scholar] [CrossRef]
- Burger, J.M. Personality; Wadsworth Cengage Learning: Belmont, Australia, 2011; Volume 8. [Google Scholar]
- Chamorro-Premuzic, T. Personality and Individual Differences; Wiley: Chichester, UK; Hoboken, NJ, USA, 2011; Volume 2. [Google Scholar]
- Van der Zee, K.I.; van Oudenhoven, J.P. The Multicultural Personality Questionnaire: A multidimensional instrument of multicultural effectiveness. Eur. J. Personal. 2000, 14, 291–309. [Google Scholar] [CrossRef]
- Caligiuri, P.; Tarique, I. Dynamic cross-cultural competencies and global leadership effectiveness. J. World Bus. 2012, 47, 612–622. [Google Scholar] [CrossRef]
- Wang, C.; Shakespear-Finch, J.; Dunne, M.P.; Hou, X.-Y.; Khawaja, N.G. How much can our universities do in the development of cultural intelligence? A cross-sectional study on health care students. Nurs. Educ. Today 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Dandy, J.; Pe-Pua, R. Attitudes to multiculturalism, immigration and cultural diversity: Comparison of dominant and non-dominant groups in three Australian states. Int. J. Intercult. Rel. 2010, 34, 34–46. [Google Scholar] [CrossRef]
- Cruz, J.P.; Estacio, J.C.; Bagtang, C.E.; Colet, P.C. Predictors of cultural competence among nursing students in the Philippines: A cross-sectional study. Nurs. Educ. Today 2016, 46, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Sherrill, W.W.; Mayo, R.M.; Truong, K.D.; Pribonic, A.P.; Schalkoff, C.A. Assessing medical student cultural competence: What really matters. Int. J. Med. Educ. 2016, 7, 248–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, J.S.; Kim, J.S. Effects of cultural education and cultural experiences on the cultural competence among undergraduate nursing students. Nurs. Educ. Pract. 2018, 29, 159–162. [Google Scholar] [CrossRef]
- Varela, O.E. Learning outcomes of study-abroad programs: A meta-analysis. Acad. Manag. Learn. Educ. 2017, 16, 531–561. [Google Scholar] [CrossRef]
- Kokko, R. Future nurses’ cultural competencies: What are their learning experiences during exchange and studies abroad? A systematic literature review. J. Nurs. Manag. 2011, 19, 673–682. [Google Scholar]
- Moon, T. Emotional intelligence correlates of the four-factor model of cultural intelligence. J. Manag. Psychol. 2010, 25, 876–898. [Google Scholar] [CrossRef]
- Ang, S.; van Dyne, L.; Koh, C.; Ng, K.Y.; Templer, K.J.; Tay, C.; Chandrasekar, N.A. Cultural intelligence: Its measurement and effects on cultural judgment and decision making, cultural adaptation and task performance. Manag. Organ. Rev. 2007, 3, 335–371. [Google Scholar] [CrossRef]
- Van der Zee, K.I.; van Oudenhoven, J.P. The Multicultural Personality Questionnaire: Reliability and validity of self-and other ratings of multicultural effectiveness. J. Res. Pers. 2001, 35, 278–288. [Google Scholar] [CrossRef]
- Van der Zee, K.I.; van Oudenhoven, J.P.; Ponterotto, J.; Fietzer, A. Multicultural Personality Questionnaire: Development of a short form. J. Person. Assess. 2013, 95, 118–124. [Google Scholar] [CrossRef]
- IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0; IBM Corp: Armonk, NY, USA, 2013. [Google Scholar]
- Godkin, M.A.; Savageau, J.A. The effect of a Global Multiculturalism Track on cultural competence of preclinical medical students. Fam. Med. 2001, 33, 178–186. [Google Scholar] [PubMed]
- Godkin, M.A.; Savageau, J.A. The effect of medical students’ international experiences on attitudes toward serving underserved multicultural populations. Fam. Med. 2003, 35, 273–278. [Google Scholar] [PubMed]
- Green, S.S.; Comer, L.; Elliott, L.; Neubrander, J. Exploring the value of an international service-learning experience in Honduras. Nurs. Educ. Pers. 2011, 32, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Wood, E.D.; St Peters, H.Y. Short-term cross-cultural study tours: Impact on cultural intelligence. Int. J. Hum. Resour. Man. 2014, 25, 558–570. [Google Scholar] [CrossRef]
- Kohlbry, P.W. The impact of international service-learning on nursing students’ cultural competency. J. Nurs. Scholarsh. 2016, 48, 303–311. [Google Scholar] [CrossRef]
- Jones, B.T.; Power, A.; Gray, T.; Downey, G.; Hall, T.; Son, T. If you build it, they may not come: Why Australian university students do not take part in outbound mobility experiences. J. Uni. Teach. Learn. Pract. 2016, 13, 1–15. [Google Scholar]
- Pasam, T.; Pasam, C.; Dake, R.; Soren, D.K. Incidence of depression, anxiety and sleep disorders in healthcare personal after the onset of Covid 19 pandemic—A survey based study. Crit. Care Innov. 2021, 4, 1–10. [Google Scholar]
- Thom, D.H.; Tirado, M.D.; Woon, T.L.; Mcbride, M.R. Development and evaluation of a cultural competency training curriculum. BMC Med. Educ. 2006, 6, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beagan, B.L. Teaching social and cultural awareness to medical students. Acad. Med. 2003, 78, 605–614. [Google Scholar] [CrossRef] [PubMed]
- Wros, P.; Archer, S. Comparing learning outcomes of international and local community partnerships for undergraduate nursing students. J. Commun. Health Nurs. 2010, 27, 216–225. [Google Scholar] [CrossRef] [PubMed]
- Levine, M. Transforming experiences: Nursing education and international immersion programs. J. Prof. Nurs. 2009, 25, 156–169. [Google Scholar] [CrossRef]
- Evanson, T.A.; Zust, B.L. “Bittersweet knowledge”: The long-term effects of an international experience. J. Nurs. Educ. 2006, 45, 412–419. [Google Scholar] [CrossRef]

{kind=link}
| Variable | Group 1 1 | Group 2 2 | ||
|---|---|---|---|---|
| n | (%) | n | (%) | |
| Age | ||||
| M ± SD | 23.81 ± 1.04 | 21.87 ± 0.75 | ||
| Gender | ||||
| Male | 4 | (12.5) | 4 | (8.7) |
| Female | 28 | (87.5) | 42 | (91.3) |
| University year level | ||||
| 1st | 0 | (0.0) | 3 | (6.5) |
| 2nd | 20 | (62.5) | 21 | (45.7) |
| 3rd | 9 | (28.1) | 19 | (41.3) |
| 4th | 3 | (9.4) | 3 | (7.5) |
| Religion | ||||
| None | 18 | (56.3) | 27 | (58.7) |
| Yes | 13 | (40.6) | 18 | (39.1) |
| Ethnicity | ||||
| Ethnic minority | 13 | (40.6) | 14 | (30.4) |
| Ethnic majority (Caucasian) | 19 | (59.4) | 32 | (69.6) |
| Speak another language except for English | ||||
| No | 20 | (62.5) | 33 | (71.7) |
| Yes | 12 | (37.5) | 13 | (28.3) |
| Language spoken in family | ||||
| English | 25 | (78.1) | 37 | (80.4) |
| Others | 7 | (21.9) | 9 | (19.6) |
| Income sufficiency | ||||
| M ± SD | 3.63 ± 0.18 | 3.89 ± 0.10 | ||
| Pre-Test | Post-Test | |||
|---|---|---|---|---|
| Group 1 1 (n = 32) | Group 2 2 (n = 46) | Group 1 (n = 32) | Group 2 (n = 46) | |
| Metacognitive-Cultural awareness | 5.28 ± 0.72 | 4.99 ± 0.90 | 5.19 ± 1.14 | 4.79 ± 0.87 |
| Cognitive-Cultural knowledge | 3.83 ± 0.97 | 3.57 ± 1.09 | 4.04 ± 1.05 | 3.39 ± 1.12 |
| Motivational-Cultural attitude | 5.63 ± 0.66 | 5.09 ± 0.97 | 5.42 ± 1.10 | 4.83 ± 1.00 |
| Behavioural-Cultural skills | 5.12 ± 1.02 | 4.71 ± 1.09 | 5.29 ± 1.20 | 4.68 ± 0.90 |
| Total cultural competence | 4.97 ± 0.64 | 4.59 ± 0.77 | 4.98 ± 1.04 | 4.43 ± 0.77 |
| Time | Group | Time × Group | Personality | Prior Overseas Study | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| F | p | F | p | F | p | F | p | F | p | |
| Metacognitive-Cultural awareness | 0.15 | 0.691 | 1.13 | 0.290 | 0.32 | 0.572 | 30.15 | <0.001 | 1.73 | 0.192 |
| Cognitive-Cultural knowledge | 0.002 | 0.961 | 1.94 | 0.168 | 4.54 | 0.037 | 16.51 | <0.001 | 0.42 | 0.521 |
| Motivational-Cultural attitude | 0.14 | 0.705 | 4.71 | 0.033 | 0.07 | 0.799 | 51.24 | <0.001 | 1.03 | 0.314 |
| Behavioural-Cultural skills | 0.54 | 0.464 | 4.54 | 0.036 | 0.27 | 0.604 | 3.22 | 0.077 | 0.13 | 0.715 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.; Hou, X.-Y.; Khawaja, N.G.; Dunne, M.P.; Shakespeare-Finch, J. Improvement in the Cognitive Aspects of Cultural Competence after Short-Term Overseas Study Programs. Int. J. Environ. Res. Public Health 2021, 18, 7102. https://doi.org/10.3390/ijerph18137102
Wang C, Hou X-Y, Khawaja NG, Dunne MP, Shakespeare-Finch J. Improvement in the Cognitive Aspects of Cultural Competence after Short-Term Overseas Study Programs. International Journal of Environmental Research and Public Health. 2021; 18(13):7102. https://doi.org/10.3390/ijerph18137102
Chicago/Turabian StyleWang, Chen, Xiang-Yu Hou, Nigar G. Khawaja, Michael P. Dunne, and Jane Shakespeare-Finch. 2021. "Improvement in the Cognitive Aspects of Cultural Competence after Short-Term Overseas Study Programs" International Journal of Environmental Research and Public Health 18, no. 13: 7102. https://doi.org/10.3390/ijerph18137102
APA StyleWang, C., Hou, X.-Y., Khawaja, N. G., Dunne, M. P., & Shakespeare-Finch, J. (2021). Improvement in the Cognitive Aspects of Cultural Competence after Short-Term Overseas Study Programs. International Journal of Environmental Research and Public Health, 18(13), 7102. https://doi.org/10.3390/ijerph18137102