
Automatic COVID-19 Detection Using Exemplar Hybrid Deep Features with X-ray Images


 ,
,  ,
,  , ,
, ,  ,
,  and
and 
Abstract
:1. Introduction
1.1. Motivation and Our Method
- choosing the most informative features automatically and
- denoting the effectiveness of this model using a conventional classifier. Bayesian optimisation is used to tune parameters of SVM classifier.
1.2. Literature Review
1.3. Contributions
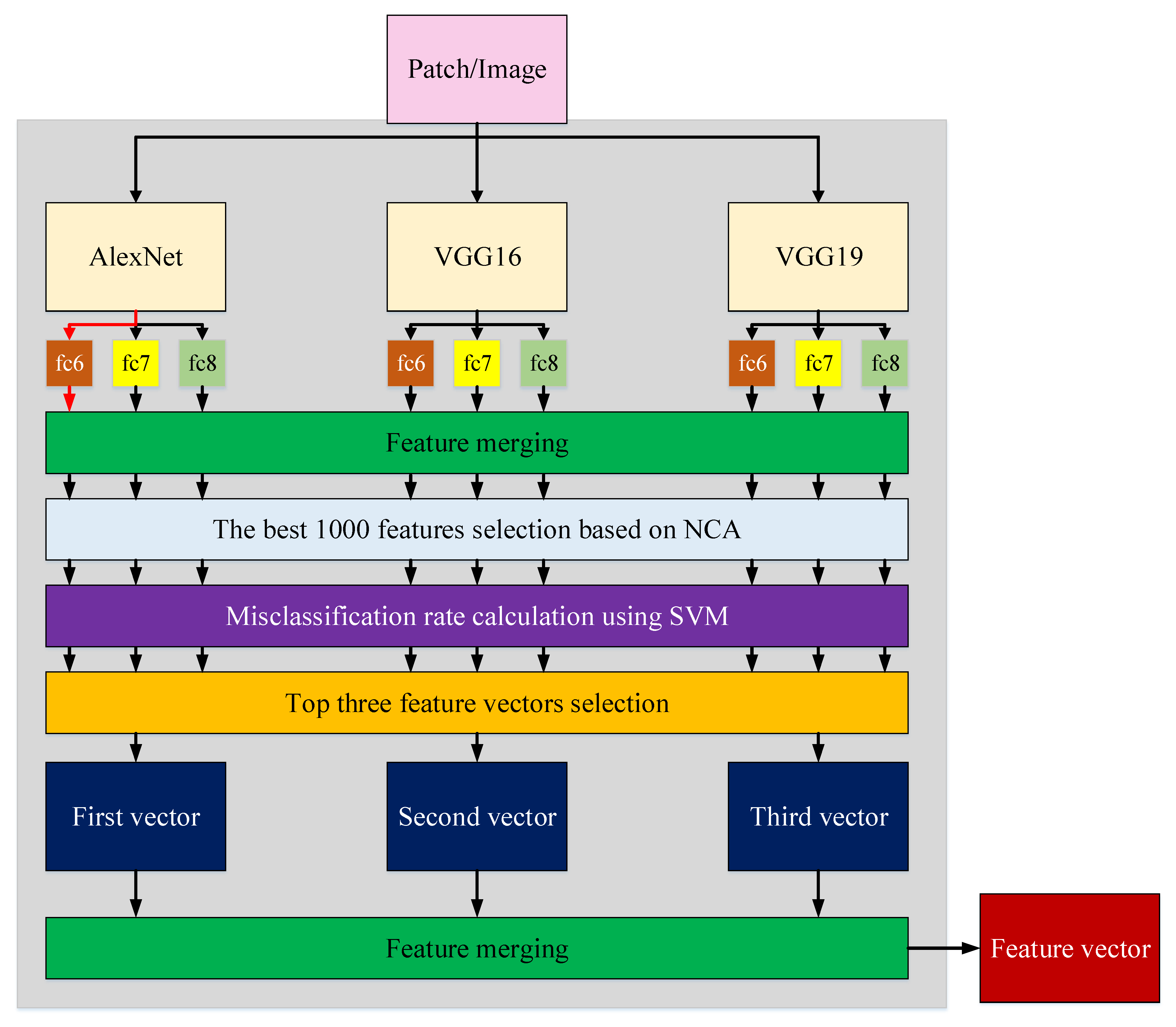
- This work presents a new X-ray image classification model using deep exemplar features. This model uses three cognitive phases, as described in Section 1.1. The proposed model is inspired by a Vision Transformer (ViT) [44]. In addition, this work presents a lightweight and highly accurate model using three pre-trained CNNs [30]. The proposed Exemplar COVID-19FclNet9 uses cognitive feature extraction, iterative feature selection and parameters to tune the SVM classifier to achieve high classification performance.
- Many machine learning models have been presented to classify COVID-19 [7,26,45]. The proposed Exemplar COVID-19FclNet9 model has been tested using four X-ray image databases. The universal high classification ability of the Exemplar COVID-19FclNet9 is used to justify the robustness of the developed model.
2. Materials and Methods
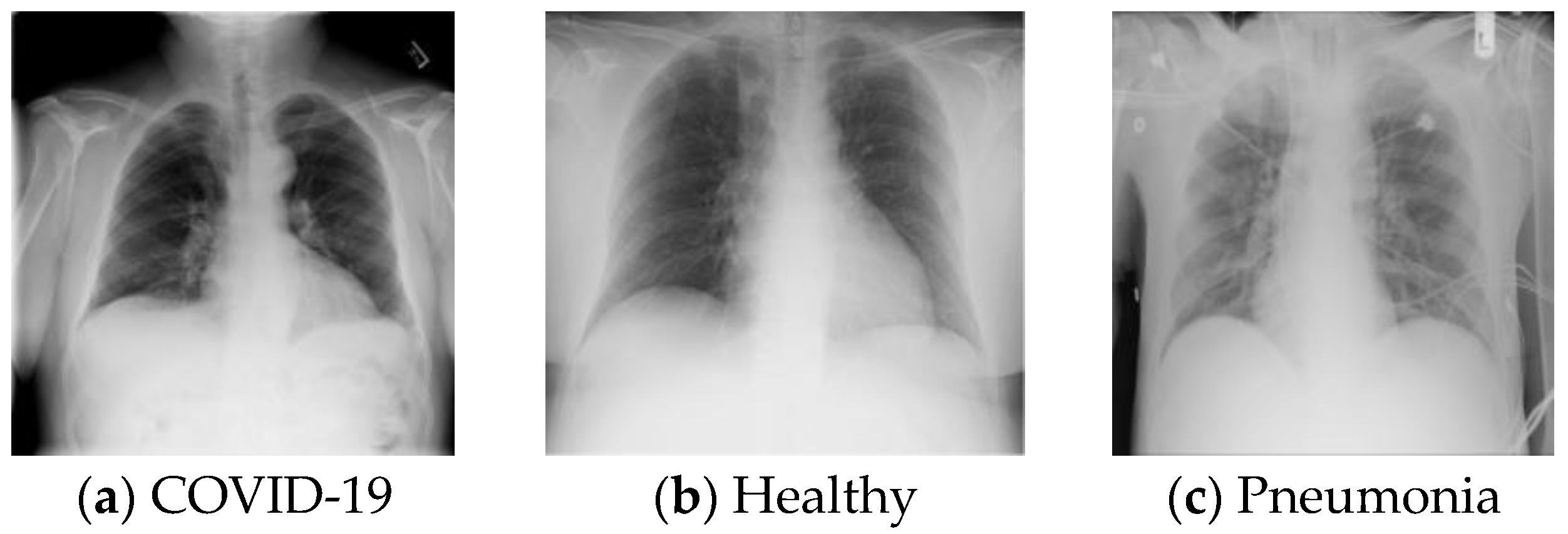
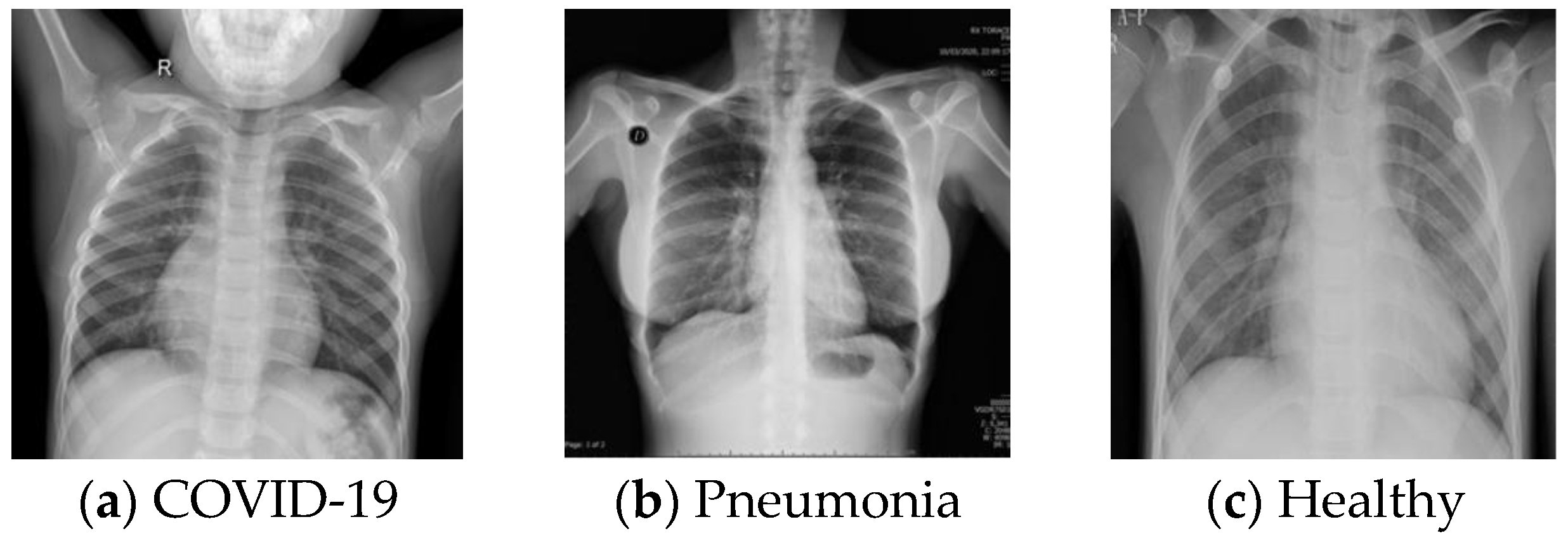
2.1. Materials
2.1.1. The First Database (DB1)
2.1.2. The Second Database (DB2)
2.1.3. The Third Database (DB3)
2.1.4. The Fourth Database (DB4)
2.2. Methods
| Algorithm 1 The algorithm used to implement proposed Exemplar COVID-19FclNet9 model |
| Input: X-ray image database |
| Output: Results |
| 00: Load X-ray image database. |
| 01: for k = 1 to dim do // Herein, dim is number of images. |
| 02: Read each image |
| 03: Divide X-ray image into exemplars/patches |
| 04: for j = 1 to 9 do |
| 05: Generate deep features from X-ray images and patches using fully connected layers. |
| 06: Merge generated features. |
| 07: Create jth feature () vector of the kth. |
| 08: end for j |
| 09: end for k |
| 10: for j = 1 to 9 do |
| 11: Apply NCA to and calculate indexes (). |
| 12: Select top 1000 features using . |
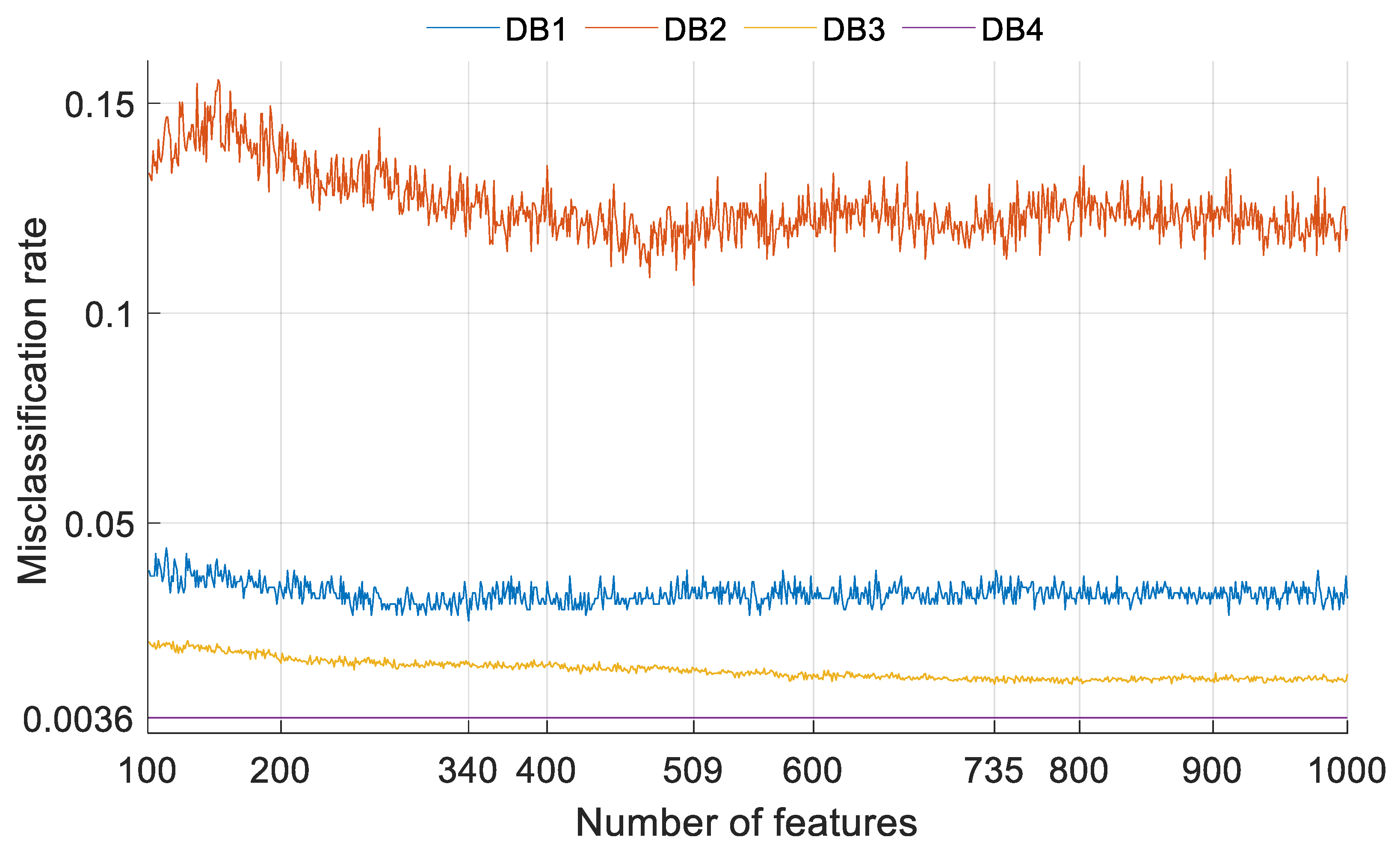
| 13: Calculate misclassification rates of the chosen 1000 features. |
| 14: end for j |
| 15: Select the best three chosen feature vectors. |
| 16: Merge the best three vectors. |
| 17: Employ iterative NCA to the merged features. |
| 18: Fed the chosen final feature vector to SVM classifier. |
| 19: Tune the parameters of the SVM classifier. |
| 20: Obtain results using the tuned SVM with 10-fold cross-validation. |
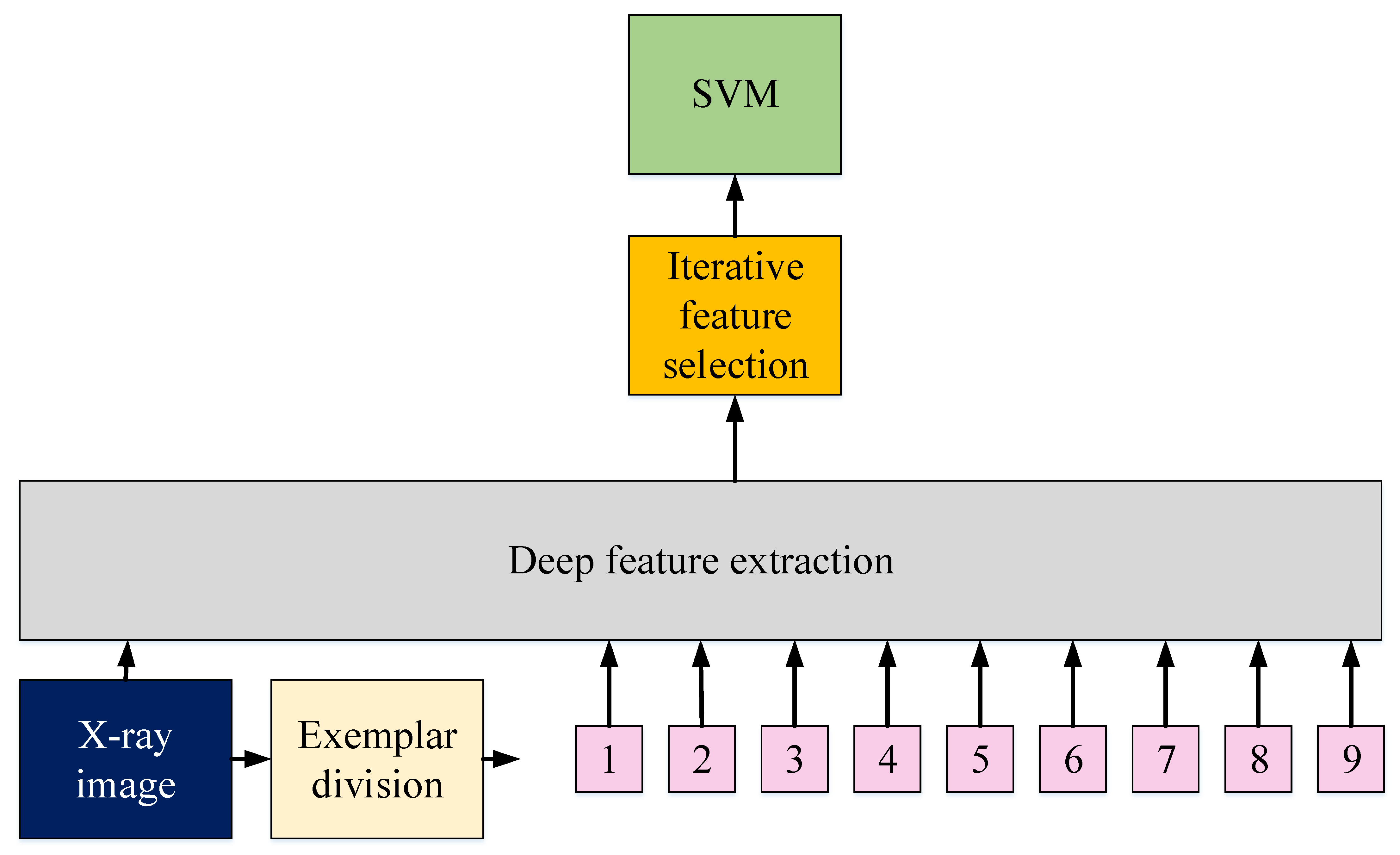
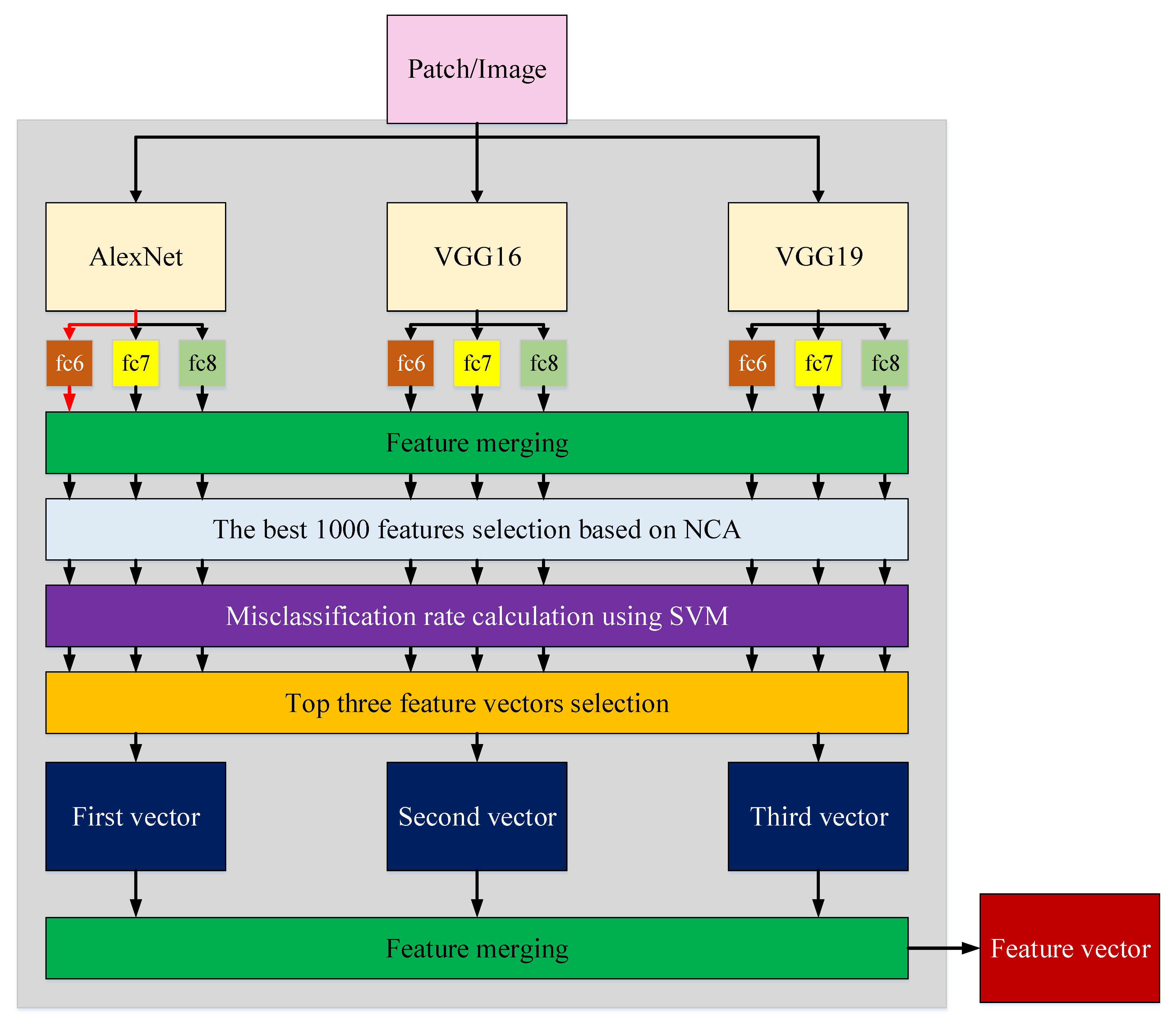
2.2.1. Deep Feature Extraction
2.2.2. Iterative Feature Selector
2.2.3. Classification
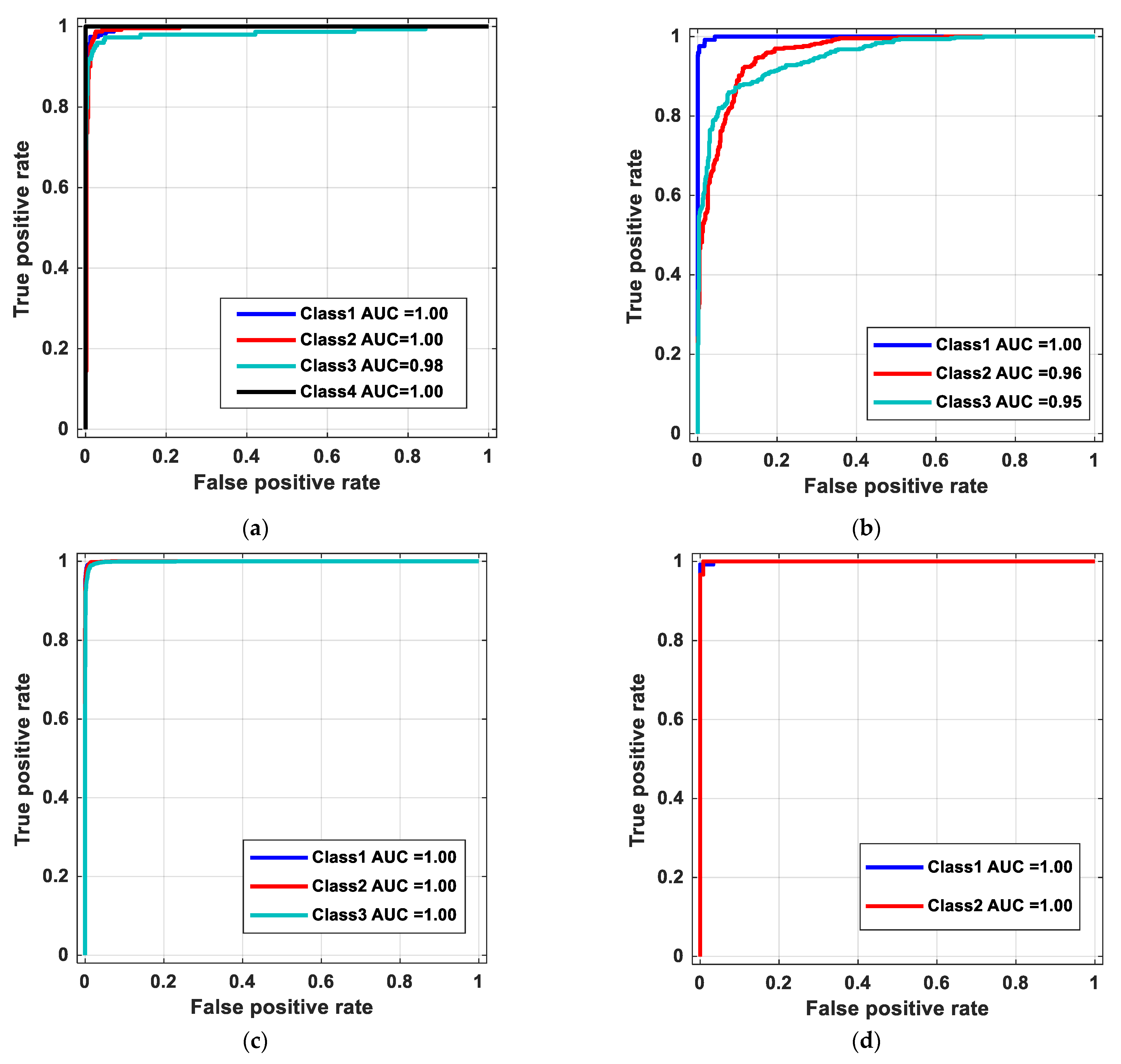
3. Results
4. Discussion
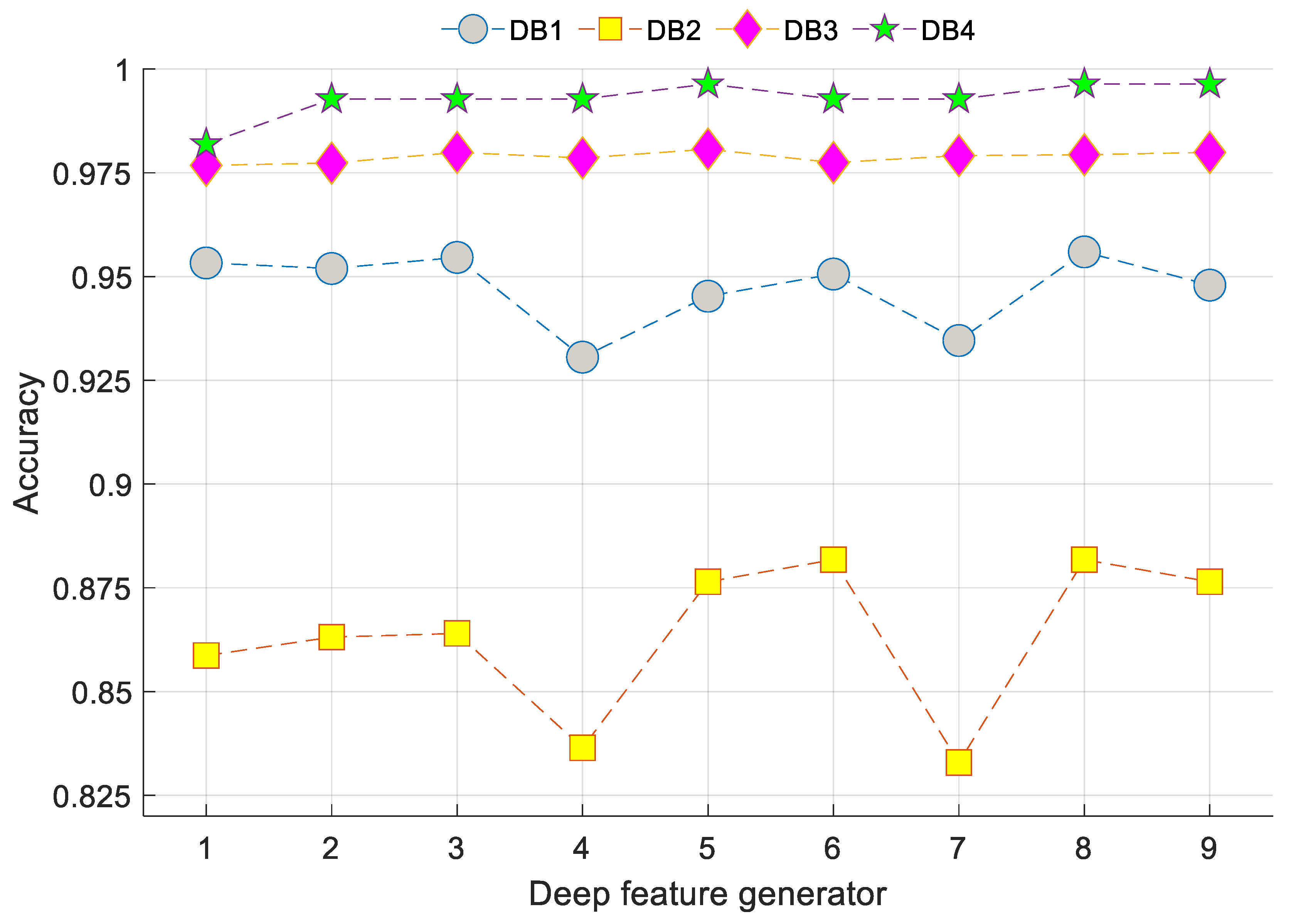
- A new deep feature generation architecture is presented using three pre-trained networks, and the proposed architecture can select the best feature generation model.
- This exemplar and cognitive deep feature generation model tested using four COVID-19 X-ray image databases and attained a high success rate on all databases, which justifies the universal success of this model.
- This model attained 97.60%, 89.96%, 98.84% and 99.64% accuracies using four databases (DB1, DB2, DB3 and DB4, respectively).
- Our method obtained the highest performance compared to other state-of-the-art works (see Table 9).
- The proposed method is a cognitive model because it can automatically select the best models, best features and most appropriate classifier.
- The proposed model yielded the highest classification performance using deep feature generators.
- The proposed model can detect COVID-19 and pneumonia accurately using X-ray images.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hu, S.; Gao, Y.; Niu, Z.; Jiang, Y.; Li, L.; Xiao, X.; Wang, M.; Fang, E.F.; Menpes-Smith, W.; Xia, J. Weakly supervised deep learning for COVID-19 infection detection and classification from ct images. IEEE Access 2020, 8, 118869–118883. [Google Scholar] [CrossRef]
- Waheed, A.; Goyal, M.; Gupta, D.; Khanna, A.; Al-Turjman, F.; Pinheiro, P.R. Covidgan: Data augmentation using auxiliary classifier gan for improved COVID-19 detection. IEEE Access 2020, 8, 91916–91923. [Google Scholar] [CrossRef] [PubMed]
- Cheong, K.H.; Jones, M.C. Introducing the 21st century’s New four horsemen of the coronapocalypse. BioEssays 2020, 42, 2000063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheong, K.H.; Wen, T.; Lai, J.W. Relieving Cost of Epidemic by Parrondo’s Paradox: A COVID-19 Case Study. Adv. Sci. 2020, 7, 2002324. [Google Scholar] [CrossRef]
- Lai, J.W.; Cheong, K.H. Superposition of COVID-19 waves, anticipating a sustained wave, and lessons for the future. BioEssays 2020, 42, 2000178. [Google Scholar] [CrossRef]
- Babajanyan, S.; Cheong, K.H. Age-structured SIR model and resource growth dynamics: A COVID-19 study. Nonlinear Dyn. 2021, 1–12. [Google Scholar]
- Alizadehsani, R.; Alizadeh Sani, Z.; Behjati, M.; Roshanzamir, Z.; Hussain, S.; Abedini, N.; Hasanzadeh, F.; Khosravi, A.; Shoeibi, A.; Roshanzamir, M. Risk factors prediction, clinical outcomes, and mortality in COVID-19 patients. J. Med. Virol. 2021, 93, 2307–2320. [Google Scholar] [CrossRef]
- Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/ (accessed on 1 June 2021).
- Jaiswal, A.; Gianchandani, N.; Singh, D.; Kumar, V.; Kaur, M. Classification of the COVID-19 infected patients using DenseNet201 based deep transfer learning. J. Biomol. Struct. Dyn. 2020, 1–8. [Google Scholar] [CrossRef]
- Wang, W.; Xu, Y.; Gao, R.; Lu, R.; Han, K.; Wu, G.; Tan, W. Detection of SARS-CoV-2 in different types of clinical specimens. JAMA 2020, 323, 1843–1844. [Google Scholar] [CrossRef] [Green Version]
- Abbas, A.; Abdelsamea, M.M.; Gaber, M.M. Classification of COVID-19 in chest X-ray images using DeTraC deep convolutional neural network. Appl. Intell. 2021, 51, 854–864. [Google Scholar] [CrossRef]
- Quintero, F.O.L.; Contreras-Reyes, J.E. Estimation for finite mixture of simplex models: Applications to biomedical data. Stat. Model. 2018, 18, 129–148. [Google Scholar] [CrossRef]
- Zhang, Z.; Shen, Y.; Wang, H.; Zhao, L.; Hu, D. High-resolution computed tomographic imaging disclosing COVID-19 pneumonia: A powerful tool in diagnosis. J. Infect. 2020, 81, 318. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Ai, L.; Lu, H.; Li, H. Clinical and imaging features of COVID-19. Radiol. Infect. Dis. 2020, 7, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Pereira, R.M.; Bertolini, D.; Teixeira, L.O.; Silla, C.N., Jr.; Costa, Y.M. COVID-19 identification in chest X-ray images on flat and hierarchical classification scenarios. Comput. Methods Programs Biomed. 2020, 194, 105532. [Google Scholar] [CrossRef]
- Punn, N.S.; Agarwal, S. Automated diagnosis of COVID-19 with limited posteroanterior chest X-ray images using fine-tuned deep neural networks. Appl. Intell. 2021, 51, 2689–2702. [Google Scholar] [CrossRef]
- Akilan, T.; Wu, Q.J.; Zhang, H. Effect of fusing features from multiple DCNN architectures in image classification. IET Image Process. 2018, 12, 1102–1110. [Google Scholar] [CrossRef]
- Ma, L.; Jiang, W.; Jie, Z.; Jiang, Y.-G.; Liu, W. Matching image and sentence with multi-faceted representations. IEEE Trans. Circuits Syst. Video Technol. 2019, 30, 2250–2261. [Google Scholar] [CrossRef]
- Zhang, W.; Wu, Q.J.; Yang, Y.; Akilan, T. Multimodel Feature Reinforcement Framework Using Moore-Penrose Inverse for Big Data Analysis. IEEE Trans. Neural Netw. Learn. Syst. 2020. [Google Scholar] [CrossRef] [PubMed]
- Huynh-The, T.; Hua, C.-H.; Kim, D.-S. Encoding pose features to images with data augmentation for 3-D action recognition. IEEE Trans. Ind. Inform. 2019, 16, 3100–3111. [Google Scholar] [CrossRef]
- Pahuja, G.; Nagabhushan, T. A comparative study of existing machine learning approaches for parkinson’s disease detection. IETE J. Res. 2021, 67, 4–14. [Google Scholar] [CrossRef]
- Deivasigamani, S.; Senthilpari, C.; Yong, W.H. Machine learning method based detection and diagnosis for epilepsy in EEG signal. J. Ambient Intell. Humaniz. Comput. 2021, 12, 4215–4221. [Google Scholar] [CrossRef]
- Tuncer, T.; Dogan, S.; Pławiak, P.; Acharya, U.R. Automated arrhythmia detection using novel hexadecimal local pattern and multilevel wavelet transform with ECG signals. Knowl. Based Syst. 2019, 186, 104923. [Google Scholar] [CrossRef]
- Tuncer, T.; Dogan, S.; Subasi, A. Surface EMG signal classification using ternary pattern and discrete wavelet transform based feature extraction for hand movement recognition. Biomed. Signal Process. Control 2020, 58, 101872. [Google Scholar] [CrossRef]
- Jahmunah, V.; Sudarshan, V.K.; Oh, S.L.; Gururajan, R.; Gururajan, R.; Zhou, X.; Tao, X.; Faust, O.; Ciaccio, E.J.; Ng, K.H. Future IoT tools for COVID-19 contact tracing and prediction: A review of the state-of-the-science. Int. J. Imaging Syst. Technol. 2021, 31, 455–471. [Google Scholar] [CrossRef] [PubMed]
- Sharifrazi, D.; Alizadehsani, R.; Roshanzamir, M.; Joloudari, J.H.; Shoeibi, A.; Jafari, M.; Hussain, S.; Sani, Z.A.; Hasanzadeh, F.; Khozeimeh, F. Fusion of convolution neural network, support vector machine and Sobel filter for accurate detection of COVID-19 patients using X-ray images. Biomed. Signal Process. Control 2021, 68, 102622. [Google Scholar] [CrossRef]
- Abdar, M.; Salari, S.; Qahremani, S.; Lam, H.-K.; Karray, F.; Hussain, S.; Khosravi, A.; Acharya, U.R.; Nahavandi, S. UncertaintyFuseNet: Robust Uncertainty-aware Hierarchical Feature Fusion with Ensemble Monte Carlo Dropout for COVID-19 Detection. arXiv 2021, arXiv:2105.08590. [Google Scholar]
- Wang, S.; Zha, Y.; Li, W.; Wu, Q.; Li, X.; Niu, M.; Wang, M.; Qiu, X.; Li, H.; Yu, H. A fully automatic deep learning system for COVID-19 diagnostic and prognostic analysis. Eur. Respir. J. 2020, 56, 2000775. [Google Scholar] [CrossRef] [PubMed]
- Jamshidi, M.; Lalbakhsh, A.; Talla, J.; Peroutka, Z.; Hadjilooei, F.; Lalbakhsh, P.; Jamshidi, M.; La Spada, L.; Mirmozafari, M.; Dehghani, M. Artificial intelligence and COVID-19: Deep learning approaches for diagnosis and treatment. IEEE Access 2020, 8, 109581–109595. [Google Scholar] [CrossRef] [PubMed]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. Adv. Neural Inf. Process. Syst. 2012, 25, 1097–1105. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Tuncer, T.; Dogan, S.; Özyurt, F.; Belhaouari, S.B.; Bensmail, H. Novel Multi Center and Threshold Ternary Pattern Based Method for Disease Detection Method Using Voice. IEEE Access 2020, 8, 84532–84540. [Google Scholar] [CrossRef]
- Vapnik, V. The support vector method of function estimation. In Nonlinear Modeling; Springer: Berlin, Germany, 1998; pp. 55–85. [Google Scholar]
- Vapnik, V. The Nature of Statistical Learning Theory; Springer Science & Business Media: Berlin, Germany, 2013. [Google Scholar]
- Narin, A.; Kaya, C.; Pamuk, Z. Automatic detection of coronavirus disease (COVID-19) using X-ray images and deep convolutional neural networks. Pattern Anal. Appl. 2021, 1–14. [Google Scholar] [CrossRef]
- Muhammad, G.; Hossain, M.S. COVID-19 and non-COVID-19 classification using multi-layers fusion from lung ultrasound images. Inf. Fusion 2021, 72, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Loey, M.; Smarandache, F.; Khalifa, N.E. Within the lack of chest COVID-19 X-ray dataset: A novel detection model based on GAN and deep transfer learning. Symmetry 2020, 12, 651. [Google Scholar] [CrossRef] [Green Version]
- Saad, W.; Shalaby, W.A.; Shokair, M.; Abd El-Samie, F.; Dessouky, M.; Abdellatef, E. COVID-19 classification using deep feature concatenation technique. J. Ambient Intell. Humaniz. Comput. 2021, 1–19. [Google Scholar] [CrossRef]
- Tuncer, T.; Dogan, S.; Ozyurt, F. An automated Residual Exemplar Local Binary Pattern and iterative ReliefF based COVID-19 detection method using chest X-ray image. Chemom. Intell. Lab. Syst. 2020, 203, 104054. [Google Scholar] [CrossRef]
- Sharma, V.; Dyreson, C. COVID-19 detection using residual attention network an artificial intelligence approach. arXiv 2020, arXiv:2006.16106. [Google Scholar]
- Jia, G.; Lam, H.-K.; Xu, Y. Classification of COVID-19 chest X-Ray and CT images using a type of dynamic CNN modification method. Comput. Biol. Med. 2021, 134, 104425. [Google Scholar] [CrossRef] [PubMed]
- Bassi, P.R.; Attux, R. A deep convolutional neural network for COVID-19 detection using chest X-rays. Res. Biomed. Eng. 2021, 1–10. [Google Scholar]
- Goldberger, J.; Hinton, G.E.; Roweis, S.; Salakhutdinov, R.R. Neighbourhood components analysis. Adv. Neural Inf. Process. Syst. 2004, 17, 513–520. [Google Scholar]
- Dosovitskiy, A.; Beyer, L.; Kolesnikov, A.; Weissenborn, D.; Zhai, X.; Unterthiner, T.; Dehghani, M.; Minderer, M.; Heigold, G.; Gelly, S. An image is worth 16x16 words: Transformers for image recognition at scale. arXiv 2020, arXiv:2010.11929. [Google Scholar]
- Shoeibi, A.; Khodatars, M.; Alizadehsani, R.; Ghassemi, N.; Jafari, M.; Moridian, P.; Khadem, A.; Sadeghi, D.; Hussain, S.; Zare, A. Automated detection and forecasting of COVID-19 using deep learning techniques: A review. arXiv 2020, arXiv:2007.10785. [Google Scholar]
- Kermany, D.; Zhang, K.; Goldbaum, M. Large Dataset of Labeled Optical Coherence Tomography (OCT) and Chest X-ray Images. Available online: https://data.mendeley.com/datasets/rscbjbr9sj/3 (accessed on 1 April 2021).
- Kermany, D.S.; Goldbaum, M.; Cai, W.; Valentim, C.C.; Liang, H.; Baxter, S.L.; McKeown, A.; Yang, G.; Wu, X.; Yan, F. Identifying medical diagnoses and treatable diseases by image-based deep learning. Cell 2018, 172, 1122–1131.e1129. [Google Scholar] [CrossRef] [PubMed]
- Ozturk, T.; Talo, M.; Yildirim, E.A.; Baloglu, U.B.; Yildirim, O.; Acharya, U.R. Automated detection of COVID-19 cases using deep neural networks with X-ray images. Comput. Biol. Med. 2020, 121, 103792. [Google Scholar] [CrossRef]
- Github. COVID-19. Available online: https://github.com/muhammedtalo/COVID-19 (accessed on 14 March 2021).
- Github. COVID Chestxray Dataset. Available online: https://github.com/ieee8023/covid-chestxray-dataset/tree/master/images (accessed on 14 March 2021).
- Rahman, T. COVID-19 Radiography Database. Available online: https://www.kaggle.com/tawsifurrahman/covid19-radiography-database (accessed on 21 April 2021).
- Chowdhury, M.E.; Rahman, T.; Khandakar, A.; Mazhar, R.; Kadir, M.A.; Mahbub, Z.B.; Islam, K.R.; Khan, M.S.; Iqbal, A.; Al Emadi, N. Can AI help in screening viral and COVID-19 pneumonia? IEEE Access 2020, 8, 132665–132676. [Google Scholar] [CrossRef]
- Rahman, T.; Khandakar, A.; Qiblawey, Y.; Tahir, A.; Kiranyaz, S.; Kashem, S.B.A.; Islam, M.T.; Al Maadeed, S.; Zughaier, S.M.; Khan, M.S. Exploring the effect of image enhancement techniques on COVID-19 detection using chest X-ray images. Comput. Biol. Med. 2021, 132, 104319. [Google Scholar] [CrossRef]
- Murugan, R.; Goel, T. E-DiCoNet: Extreme learning machine based classifier for diagnosis of COVID-19 using deep convolutional network. J. Ambient Intell. Humaniz. Comput. 2021, 1–12. [Google Scholar] [CrossRef]
- Gilanie, G.; Bajwa, U.I.; Waraich, M.M.; Asghar, M.; Kousar, R.; Kashif, A.; Aslam, R.S.; Qasim, M.M.; Rafique, H. Coronavirus (COVID-19) detection from chest radiology images using convolutional neural networks. Biomed. Signal Process. Control 2021, 66, 102490. [Google Scholar] [CrossRef]
- Pandit, M.K.; Banday, S.A.; Naaz, R.; Chishti, M.A. Automatic detection of COVID-19 from chest radiographs using deep learning. Radiography 2021, 27, 483–489. [Google Scholar] [CrossRef]
- Nigam, B.; Nigam, A.; Jain, R.; Dodia, S.; Arora, N.; Annappa, B. COVID-19: Automatic detection from X-ray images by utilizing deep learning methods. Expert Syst. Appl. 2021, 176, 114883. [Google Scholar] [CrossRef]
- Hussain, E.; Hasan, M.; Rahman, M.A.; Lee, I.; Tamanna, T.; Parvez, M.Z. CoroDet: A deep learning based classification for COVID-19 detection using chest X-ray images. Chaos Solitons Fractals 2021, 142, 110495. [Google Scholar] [CrossRef] [PubMed]
- Shi, W.; Tong, L.; Zhu, Y.; Wang, M.D. COVID-19 Automatic Diagnosis with Radiographic Imaging: Explainable AttentionTransfer Deep Neural Networks. IEEE J. Biomed. Health Inform. 2021, 25, 2376–2387. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, H.; Ghosh, S.; Dhar, A.; Obaidullah, S.M.; Santosh, K.; Roy, K. Deep neural network to detect COVID-19: One architecture for both CT Scans and Chest X-rays. Appl. Intell. 2021, 51, 2777–2789. [Google Scholar] [CrossRef]
- Sitaula, C.; Hossain, M.B. Attention-based VGG-16 model for COVID-19 chest X-ray image classification. Appl. Intell. 2021, 51, 2850–2863. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hyperparameter | Value |
|---|---|
| Multiclass method | One-vs.-One, One-vs.-All |
| Box constraint level | [0.001–1000] |
| Kernel | Cubic, Quadratic, Linear, Gaussian |
| Standardise | False, True |
| Hyperparameter | Tuned Parameters for the DB1 | Tuned Parameters for the DB2 | Tuned Parameters for the DB3 |
|---|---|---|---|
| Multiclass method | One-vs.-One | One-vs.-All | One-vs.-All |
| Kernel | Linear | Gaussian | Cubic |
| Box constraint | 999.30 | 2 | 1 |
| Standardise | False | True | True |
| Actual Class | Predicted Class | |||
|---|---|---|---|---|
| Normal | Bacterial Pneumonia | Virus Pneumonia | COVID-19 | |
| Normal | 227 | 4 | 3 | 0 |
| Bacterial Pneumonia | 3 | 238 | 1 | 0 |
| Viral Pneumonia | 3 | 4 | 141 | 0 |
| COVID-19 | 0 | 0 | 0 | 125 |
| Recall (%) | 97.01 | 98.35 | 95.27 | 100 |
| Precision (%) | 97.42 | 96.75 | 97.24 | 100 |
| F1-score (%) | 97.22 | 97.54 | 96.25 | 100 |
| Actual Class | Predicted Class | ||
|---|---|---|---|
| COVID-19 | Healthy | Pneumonia | |
| COVID-19 | 120 | 0 | 5 |
| Healthy | 1 | 457 | 42 |
| Pneumonia | 0 | 65 | 432 |
| Recall (%) | 96 | 91.40 | 87 |
| Precision (%) | 99.17 | 87.55 | 90.25 |
| F1-score (%) | 97.56 | 89.43 | 88.59 |
| Actual Class | Predicted Class | ||
|---|---|---|---|
| COVID-19 | Pneumonia | Healthy | |
| COVID-19 | 3586 | 2 | 28 |
| Pneumonia | 2 | 1318 | 25 |
| Healthy | 28 | 19 | 3953 |
| Recall (%) | 99.17 | 97.99 | 98.82 |
| Precision (%) | 99.17 | 98.43 | 98.68 |
| F1-score (%) | 99.17 | 98.21 | 98.75 |
| Actual Class | Predicted Class | |
|---|---|---|
| COVID-19 | Healthy | |
| COVID-19 | 126 | 1 |
| Healthy | 0 | 150 |
| Recall (%) | 99.21 | 100 |
| Precision (%) | 100 | 99.33 |
| F1-score (%) | 99.60 | 99.66 |
| Overall Results | DB1 | DB2 | DB3 | DB4 |
|---|---|---|---|---|
| Accuracy (%) | 97.60 | 89.96 | 98.84 | 99.64 |
| Unweighted average recall (%) | 97.66 | 91.47 | 98.66 | 99.61 |
| Precision (%) | 97.85 | 92.32 | 98.76 | 99.80 |
| F1 score (%) | 97.75 | 91.86 | 98.71 | 99.63 |
| Network | Number | Fully Connected Layer |
|---|---|---|
| AlexNet | 1 | fc8 |
| 2 | fc7 | |
| 3 | fc6 | |
| VGG16 | 4 | fc8 |
| 5 | fc7 | |
| 6 | fc6 | |
| VGG19 | 7 | fc8 |
| 8 | fc7 | |
| 9 | fc6 |
| Study | Method | Classifier | Split Ratio | Number of Class/Type | Number of Cases | Results (%) |
|---|---|---|---|---|---|---|
| Murugan and Goel [54] | Convolutional neural networks (ResNet50) | Softmax | 70:30 | 3/Chest X-ray | 900 COVID-19 900 Pneumonia 900 Normal | Acc: 94.07 Sen: 98.15 Spe: 91.48 Rec: 85.21 Pre: 98.15 F1: 91.22 |
| Gilanie et al. [55] | Convolutional neural networks | Softmax | 60:20:20 | Chest radiology | 1066 COVID-19 7021 Pneumonia 7021 Normal | Acc: 96.68 Spe: 95.65 Sen: 96.24 |
| Pandit et al. [56] | Convolutional neural networks (VGG-16) | Softmax | 70:30 | 1. 2/Chest radiographs 2. 3/Chest radiographs | 1. 224 COVID-19 504 Healthy 2. 224 COVID-19 700 Pneumonia 504 Healthy | Acc: 1. 96.00 2. 92.53 |
| Nigam et al. [57] | Convolutional neural networks (EfficientNet) | Softmax | 70:20:10 | 3/Chest X-ray | 795 COVID-19 795 Normal 711 Others | Acc: 93.48 |
| Hussain et al. [58] | Convolutional neural networks (CoroDet) | Softmax | 5-fold cross validation | 1. 2/Chest X-ray 2. 3/Chest X-ray 3. 4/Chest X-ray | 1. 500 COVID-19 800 Normal 2. 500 COVID-19 800 Normal 800 Pneumonia—bacterial 3. 500 COVID-19 800 Normal 400 Pneumonia—bacterial 400 Pneumonia—viral | Acc: 1. 99.10 2. 94.20 3. 91.20 |
| Ozturk et al. [48] | Deep neural networks | Darknet-19 | 5-fold cross validation | 3/Chest X-ray | 125 COVID-19 500 Pneumonia 500 No Findings | Acc: 87.02 Sen: 92.18 Spe: 89.96 |
| Shi et al. [59] | Deep neural networks | Deep neural networks | 70:20:10 | 1. 3/Chest CT images 2. 3/Chest X-ray | 1. 349 COVID-19 384 Normal 304 CAP 2. 450 COVID-19 1800 Normal 1837 CAP | Acc: 1. 87.98 2. 93.44 |
| Mukherjee et al. [60] | Convolutional neural network, Deep neural network | Softmax | 10-fold cross validation | 2/Computed Tomography and Chest X-ray | 336 COVID-19 336 non-COVID-19 | Acc: 96.28 Sen: 97.92 Spe: 94.64 Pre: 94.81 F1: 96.34 |
| Sitaula and Hossain [61] | Convolutional neural networks | FC-layers, and Softmax | 70:30 | 1. 3/Chest X-ray 2. 4/Chest X-ray 3. 5/Chest X-ray | Database1: 125 COVID-19 125 No findings 125 Pneumonia Database2: 320 COVID-19 320 Normal 320 Pneumonia Bacterial 320 Pneumonia Viral Database3: 320 COVID-19 320 Normal 320 Pneumonia Bacterial 320 Pneumonia Viral 320 No findings | Acc: 1. 79.58 2. 85.43 3. 87.49 |
| Our method | Exemplar COVID-19FclNet9 | Support vector machine | 10-fold cross validation | 4/Chest X-ray | 234 Control 242 Bacterial Pneumonias 148 Viral pneumonias 125 COVID-19 | Acc: 97.60 |
| 3/Chest X-ray | 125 COVID-19 500 Pneumonia 500 Control | Acc: 89.96 | ||||
| 3/ Chest X-ray | 3616 COVID-19 1345 Pneumonia 4000 Control | Acc: 98.84 | ||||
| 2/Chest X-ray | 127 COVID-19 150 Normal | Acc: 99.64 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barua, P.D.; Muhammad Gowdh, N.F.; Rahmat, K.; Ramli, N.; Ng, W.L.; Chan, W.Y.; Kuluozturk, M.; Dogan, S.; Baygin, M.; Yaman, O.; et al. Automatic COVID-19 Detection Using Exemplar Hybrid Deep Features with X-ray Images. Int. J. Environ. Res. Public Health 2021, 18, 8052. https://doi.org/10.3390/ijerph18158052
Barua PD, Muhammad Gowdh NF, Rahmat K, Ramli N, Ng WL, Chan WY, Kuluozturk M, Dogan S, Baygin M, Yaman O, et al. Automatic COVID-19 Detection Using Exemplar Hybrid Deep Features with X-ray Images. International Journal of Environmental Research and Public Health. 2021; 18(15):8052. https://doi.org/10.3390/ijerph18158052
Chicago/Turabian StyleBarua, Prabal Datta, Nadia Fareeda Muhammad Gowdh, Kartini Rahmat, Norlisah Ramli, Wei Lin Ng, Wai Yee Chan, Mutlu Kuluozturk, Sengul Dogan, Mehmet Baygin, Orhan Yaman, and et al. 2021. "Automatic COVID-19 Detection Using Exemplar Hybrid Deep Features with X-ray Images" International Journal of Environmental Research and Public Health 18, no. 15: 8052. https://doi.org/10.3390/ijerph18158052
APA StyleBarua, P. D., Muhammad Gowdh, N. F., Rahmat, K., Ramli, N., Ng, W. L., Chan, W. Y., Kuluozturk, M., Dogan, S., Baygin, M., Yaman, O., Tuncer, T., Wen, T., Cheong, K. H., & Acharya, U. R. (2021). Automatic COVID-19 Detection Using Exemplar Hybrid Deep Features with X-ray Images. International Journal of Environmental Research and Public Health, 18(15), 8052. https://doi.org/10.3390/ijerph18158052