
Knowledge, Attitude, Practices and Viewpoints of Undergraduate University Students towards Self-Medication: An Institution-Based Study in Riyadh

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Study Tool
2.3. Validity and Reliability of Study Tool
2.4. Sampling Method and Sample Size
2.5. Data Collection
2.6. Data Processing and Analysis
3. Results
3.1. Demographic Information
3.2. Student’s Level of Knowledge towards SM
3.3. Student’s Attitude towards SM
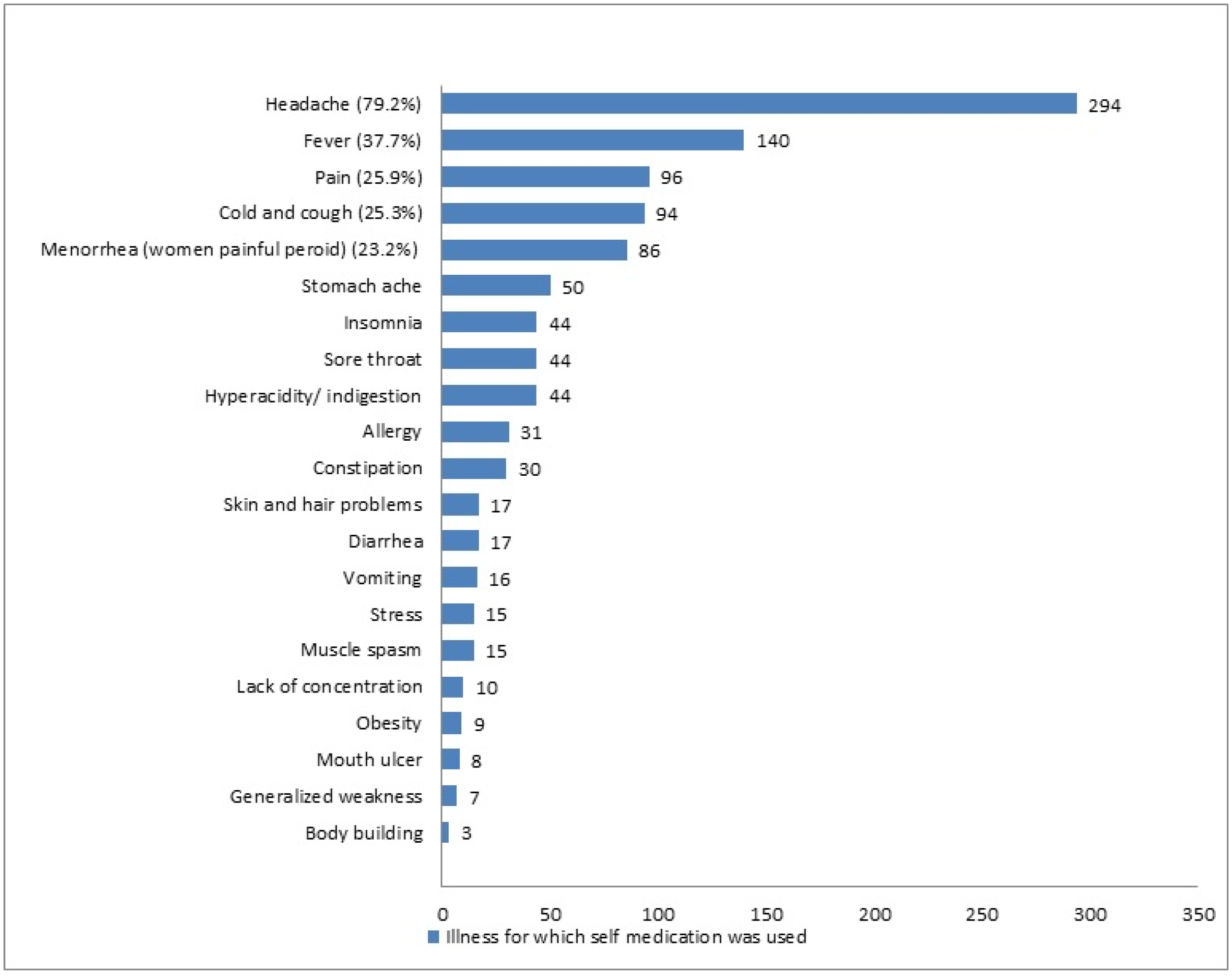
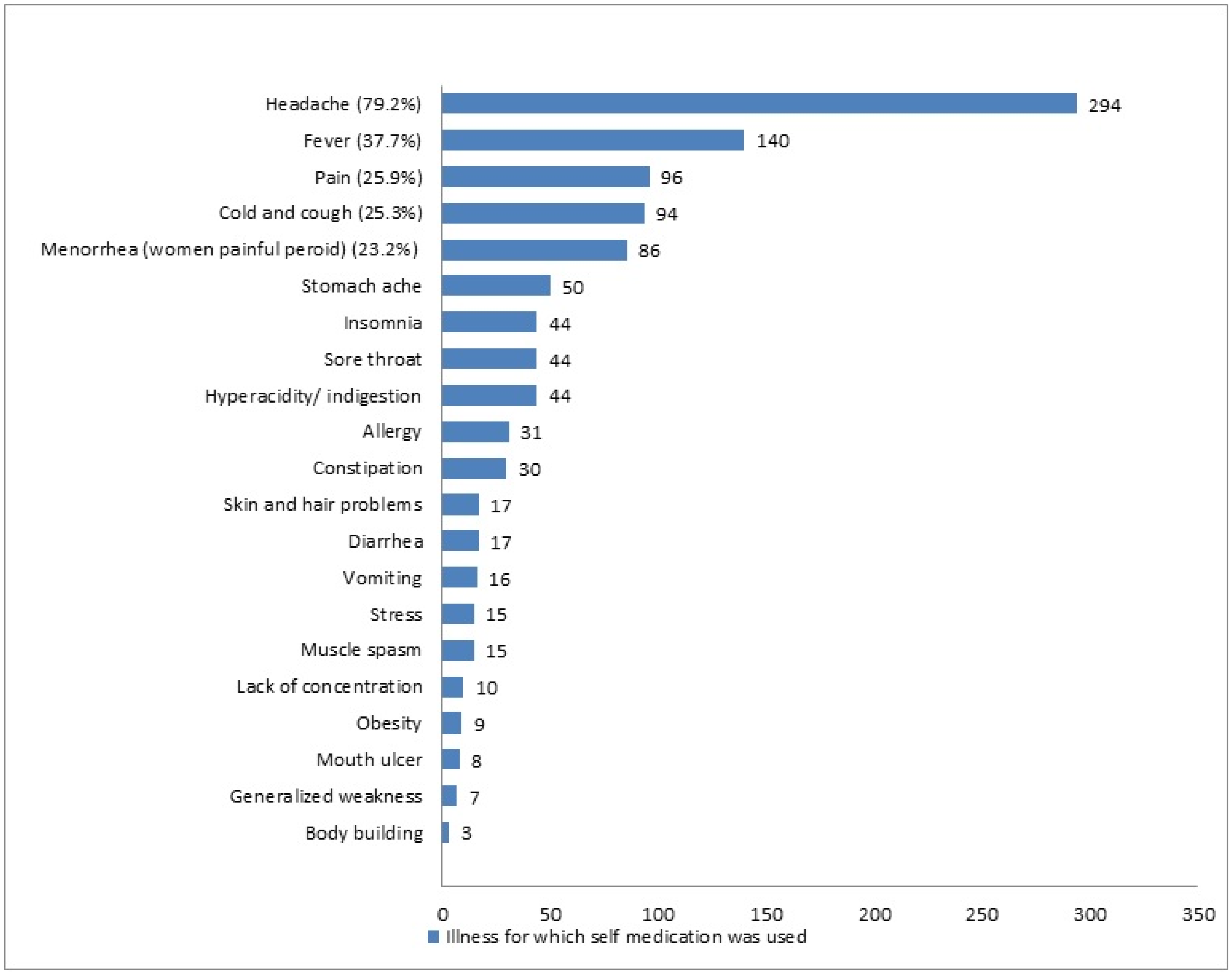
3.4. Self-Medication (SM) Practice
3.5. Information and Place of Obtaining the Drugs for SM
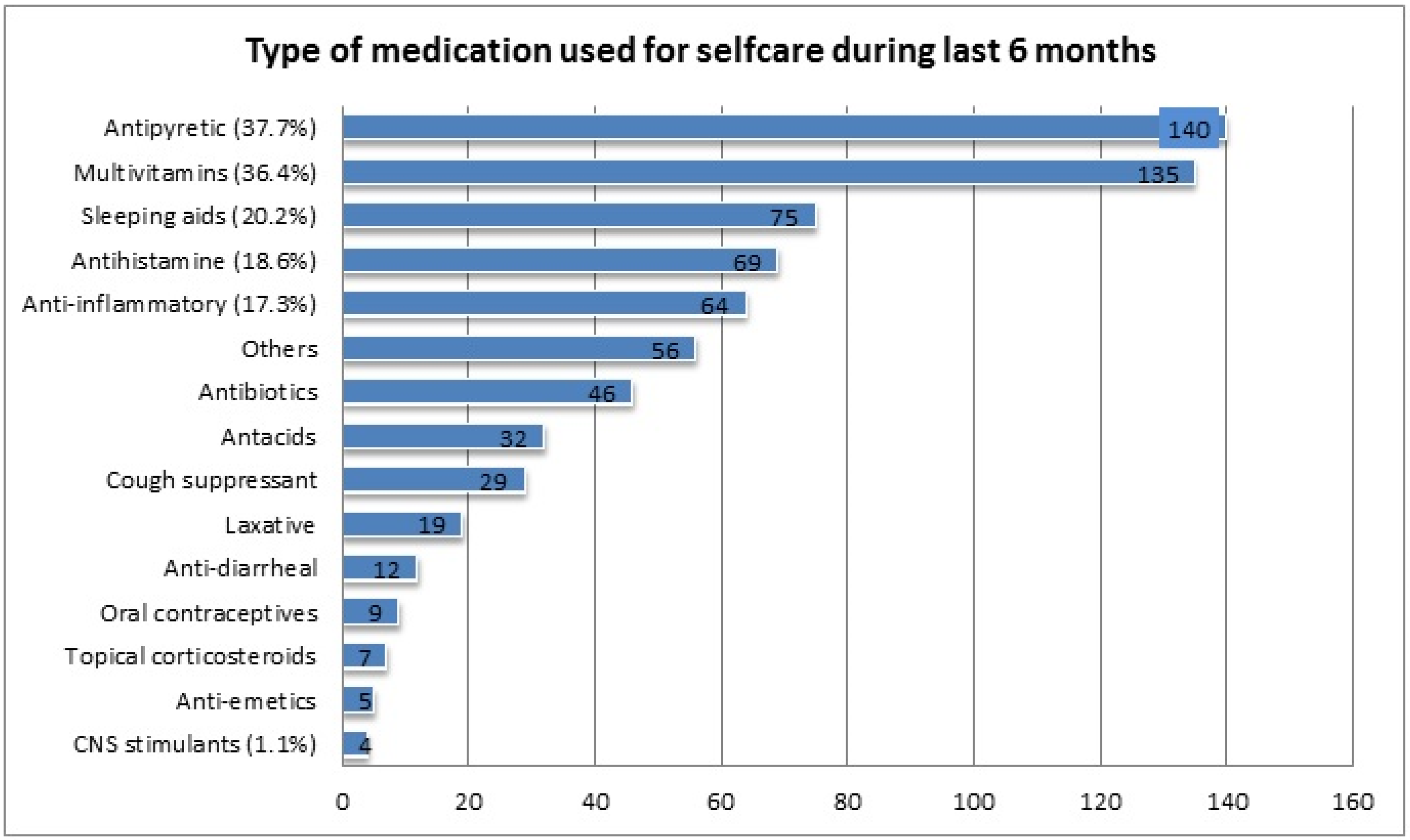
3.6. Medications Used for SM
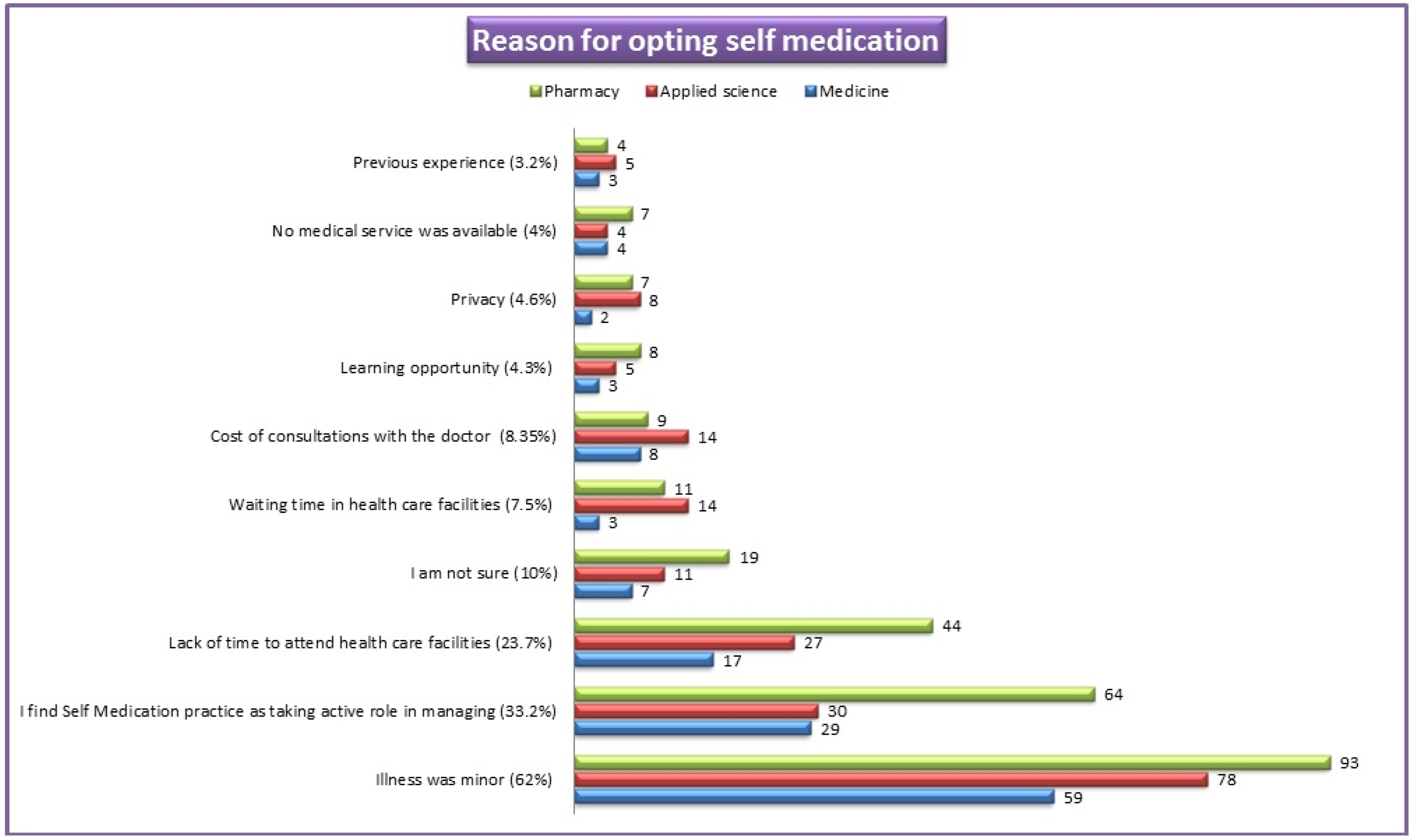
3.7. Reasons for Opting SM Practice
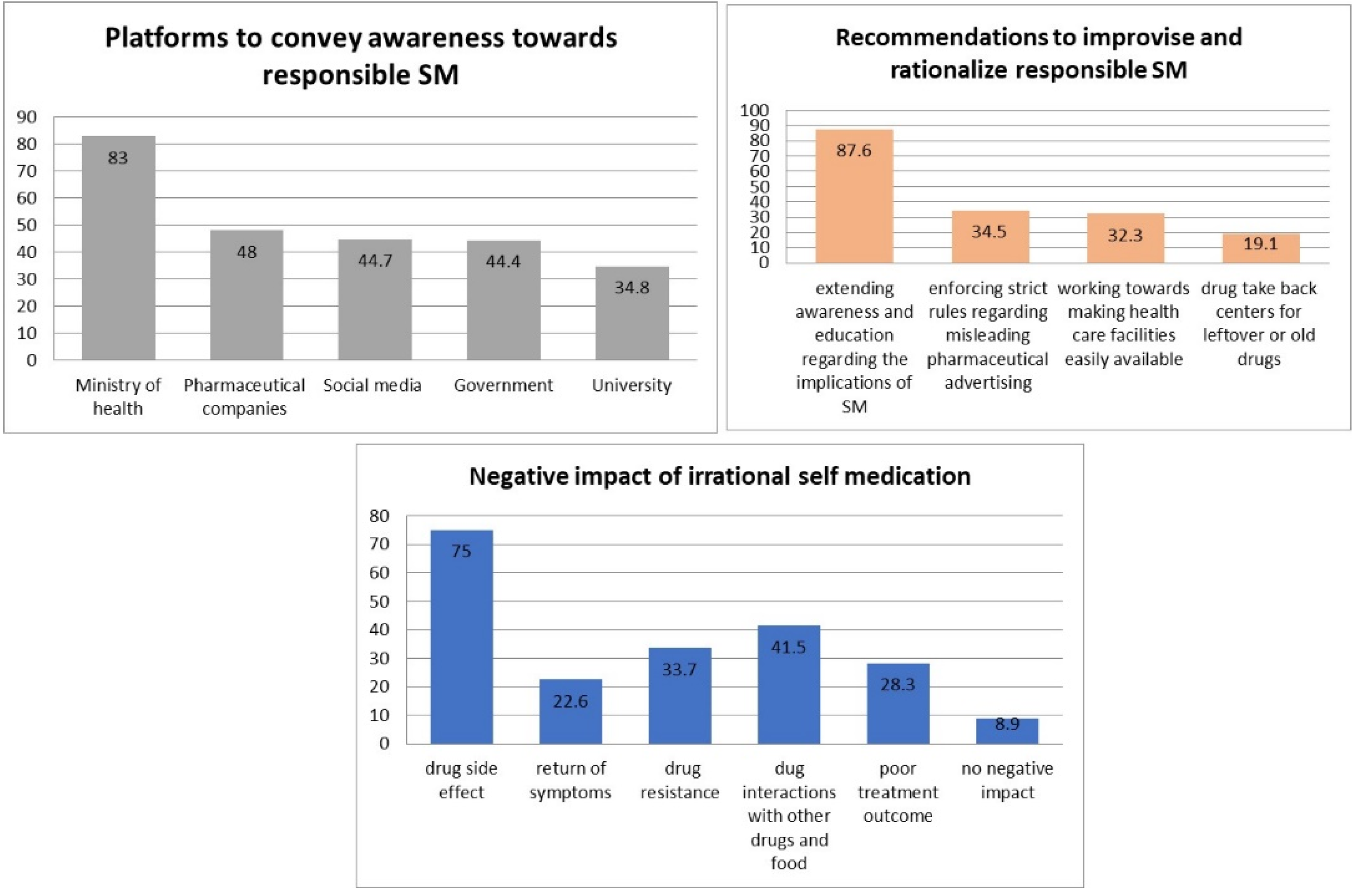
3.8. Negative Impact of Irrational SM
3.9. Awareness towards Responsible SM
3.10. Correlation between Knowledge and Attitude
3.11. Factors Influencing Self-Medication Practice
3.12. Factors Affecting Student’s Knowledge and Attitude Regarding SM
4. Discussion
4.1. Strengths and Limitations
4.2. Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| SM | Self-medication |
| UM | AlMaarefa University |
| OTC | Over-the-counter |
| GPA | Grade Percentage Average |
| BMI | Body Mass Index |
References
- Kayalvizhi, S.; Senapathi, R. Evaluation of the perception, attitude and practice of self-medication among business students in 3 select Cities, South India. Int. J. Enterp. Innov. Manag. Stud. 2010, 1, 40–44. [Google Scholar]
- WHO. Guidelines for the Regulatory Assessment of Medicinal Products for Use in Self-Medication. WHO Drug Information. 2000. Available online: https://apps.who.int/iris/handle/10665/66154 (accessed on 27 June 2021).
- Bennadi, D. Self-medication: A current challenge. J. Basic Clin. Pharm. 2014, 5, 19. [Google Scholar] [CrossRef] [PubMed]
- Makeen, H.A.; Albarraq, A.A.; Banji, O.J.F.; Taymour, S.; Meraya, A.; Alqhatani, S.; Banji, D. Knowledge, attitudes, and practices toward self-medication in a rural population in south-western Saudi Arabia. Saudi J. Health Sci. 2019, 8, 54–59. [Google Scholar]
- Ocan, M.; Obuku, E.A.; Bwanga, F.; Akena, D.; Richard, S.; Ogwal-Okeng, J.; Obua, C. Household antimicrobial self-medication: A systematic review and meta-analysis of the burden, risk factors and outcomes in developing countries. BMC Public Health 2015, 15, 742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phalke, V.D.; Phalke, D.B.; Durgawale, P.M. Self-medication practices in rural maharashtra. Indian J. Community Med. 2006, 31, 34–35. [Google Scholar] [CrossRef]
- Shveta, S.; Jagmohan, S. A study of self-medication pattern in Punjab. Indian J. Pharm. Pract. 2011, 4, 43–48. [Google Scholar]
- Joshi, M.C.; Shalini, A.S.; Agarwal, S. A questionnaire based study of self-medication practices among young population. Res. J. Pharm. Biol. Chem. Sci. 2011, 2, 761–766. [Google Scholar]
- Albusalih, F.A.; Naqvi, A.A.; Ahmad, R.; Ahmad, N. Prevalence of self- medication among students of pharmacy and medicine colleges of a public sector university in dammam city, Saudi Arabia. Pharmacy 2017, 5, 51. [Google Scholar] [CrossRef] [Green Version]
- Albasheer, O.B.; Mahfouz, M.S.; Masmali, B.M.; Ageeli, R.A.; Majrashi, A.M.; Hakami, A.N.; Hakami, Z.H.; Hakami, A.A.; Douf, T.A. Self-medication practice among undergraduate medical students of a saudi tertiary institution. Trop. J. Pharm. Res. 2016, 15, 2253–2259. [Google Scholar] [CrossRef] [Green Version]
- Mustafa, O.M.; Rohra, D.K. Patterns and determinants of self-medication among university students in Saudi Arabia. J. Pharm. Health Serv. Res. 2017, 8, 177–185. [Google Scholar] [CrossRef]
- Alshahrani, S.M.; Alavudeen, S.S.; Alakhali, K.M.; Al-Worafi, Y.M.; Bahamdan, A.K.; Vigneshwaran, E. Self-medication among king khalid university students, Saudi Arabia. Risk Manag. Healthc. Policy 2019, 12, 243–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saeed, M.S.; Alkhoshaiban, A.S.; Al-Worafi, A.; Long, C.M. Perception of self-medication among university students in Saudi Arabia. Arch. Pharm. Pract. 2014, 5, 149–152. [Google Scholar]
- Al Flaiti, M.; Al Badi, K.; Hakami, W.O.; Khan, S.A. Evaluation of self-medication practices in acute diseases among university students in Oman. J. Acute Dis. 2014, 3, 249–252. [Google Scholar] [CrossRef] [Green Version]
- Lukovic, J.A.; Miletic, V.; Pekmezovic, T.; Trajkovic, G.; Ratkovic, N.; Aleksic, D.; Grgurevic, A. Self-medication practices and risk factors for self-medication among medical students in belgrade, Serbia. PLoS ONE 2014, 9, e114644. [Google Scholar]
- Helal, R.M.; Abou-ElWafa, H.S. Self-medication in university students from the city of mansoura, Egypt. J. Environ. Public Health 2017, 2017, 9145193. [Google Scholar] [CrossRef]
- Alves, R.F.; Precioso, J.; Becoña, E. Knowledge, attitudes and practice of self-medication among university students in Portugal: A cross-sectional study. Nord. Alcohol Drugs 2021, 38, 50–65. [Google Scholar] [CrossRef]
- Paula Martins, A.; da Costa Miranda, A.; Mendes, Z.; Soares, M.A.; Ferreira, P.; Nogueira, A. Self- medication in a Portuguese urban population: A prevalence study. Pharmacoepidemiol. Drug Saf. 2002, 11, 409–414. [Google Scholar] [CrossRef]
- Montastruc, J.L.; Bondon-Guitton, E.; Abadie, D.; Lacroix, I.; Berreni, A.; Pugnet, G.; Durrieu, G.; Sailler, L.; Giroud, J.-P.; Damase-Michel, C.; et al. Pharmacovigilance, risks and adverse effects of self-medication. Therapies 2016, 71, 257–262. [Google Scholar] [CrossRef]
- Ugalmugle, S.; Swain, R. Over-the-Counter Drugs Market Size by Product; Global Market Insights: Selbyville, DE, USA, 2021; p. 135. Available online: https://www.gminsights.com/industry-analysis/over-the-counter-otc-drugs-market (accessed on 27 June 2021).
- Asdaq, B. Prevalence of stress and its associated factors among students of al- maarefa colleges of riyadh, Saudi Arabia: A comparative cross-sectional study. Asian J. Pharm. 2018, 12, S698. [Google Scholar]
- AlFadeel, M.A.; Shaban, A.E.; Neyaz, B.Y.; AlAli, H.S.; Neyaz, S.Y.; Alkhrissi, N.M.; Alahmari, M.S.; Sweed, W.K.; Alhajri, N.T.; Almoumen, A.M.; et al. Consumption of caffeine and its perceived effect among staff and students of medicine at Almaarefa University, Saudi Arabia. Int. J. Med. Dev. Ctries 2020, 4, 1112–1115. [Google Scholar]
- Al-Mutairi, A.S.; Rahhal, S.A.; Al-Abdullah, M.S.; Al-Ibrahim, Z.H.; Al-Mutairi, M.B.; Shafaay, R.A.; Alanazi, R.A.; Al-Mshel, H.A.; Moqbel, H.M.; Al-Habshan, N.A. Sleep and academic performance among female students in al-maarefa colleges. Egypt J. Hosp. Med. 2018, 73, 6828–6837. [Google Scholar] [CrossRef]
- Marwa, K.I.; AlKthiri, H.A.; Shicker, H.I.; Neyaz, B.Y.; Ali, A.H.A.; Albalawi, H.A.; Alhilal, S.H. Impact of distance learning during COVID-19 on the anxiety of college students of almaarefa university. Int. J. Med. Dev. Ctries. 2020, 4, 1844–1846. [Google Scholar] [CrossRef]
- Charan, J.; Biswas, T. How to calculate sample size for different study designs in medical research? Indian J. Psychol. Med. 2013, 35, 121–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, F.R.; Trivedi, P.K. Economics of self-medication: Theory and evidence. Health Econ. 2003, 12, 721–739. [Google Scholar] [CrossRef] [PubMed]
- Seam, O.R.; Bhatta, R.; Saha, B.L.; Das, A.; Hossain, M.; Uddin, S.M.N.; Karmakar, P.; Choudhuri, S.K.; Sattar, M.M. Assessing the perceptions and practice of self-medication among Bangladeshi undergraduate pharmacy students. Pharmacy 2018, 6, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashemzaei, M.; Afshari, M.; Koohkan, Z.; Bazi, A.; Rezaee, R.; Tabrizian, K. Knowledge, attitude, and practice of pharmacy and medical students regarding self-medication, a study in zabol university of medical sciences; sistan and baluchestan province in south-east of Iran. BMC Med. Educ. 2021, 49, 21. [Google Scholar]
- Kumar, N.; Kanchan, T.; Unnikrishnan, B.; Rekha, T.; Mithra, P.; Kulkarni, V.; Papanna, M.K.; Holla, R.; Uppal, S. Perceptions and practices of self-medication among medical students in coastal south India. PLoS ONE 2013, 8, e72247. [Google Scholar] [CrossRef]
- Sawalha., A.F. Assessment of self-medication practice among university students in Palestine: Therapeutic and toxicity implications. J. Nat. Stud. 2015, 15, 267–282. [Google Scholar]
- Aljaouni, M.E.; Hafiz, A.A.; Alalawi, H.H.; Alahmadi, G.M.; AlKhawaja, I. Self-medication practice among medical and non-medical students at taibah university, madinah, Saudi Arabia. Int. J. Acad. Sci. Res. 2015, 3, 54–65. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Variable | Demographic Characteristics (%) | Adequacy of Knowledge (n = 371) | Adequacy of Attitude (n = 371) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Good (%) | Moderate (%) | Poor (%) | p Value | Positive (%) | Neutral (%) | Negative (%) | p Value | |||
| Colleges | Pharmacy | 153 (41.2) | 70 (18.9) | 68 (18.3) | 15 (4) | 0.001 * | 81 (21.8) | 69 (18.6) | 3 (0.8) | 0.639 |
| Medicine | 88 (23.7) | 27 (7.3) | 48 (12.9) | 13 (3.5) | 37 (10) | 46 (12.4) | 5 (1.3) | |||
| Applied Sciences | 130 (35.1) | 26 (7) | 57 (15.4) | 47 (12.7) | 60 (16.2) | 63 (17) | 7 (1.9) | |||
| Age | <20 years | 30 (8.1) | 2 (0.5) | 16 (4.3) | 12 (3.2) | 0.001 * | 10 (2.7) | 18 (4.9) | 2 (0.5) | 0.083 |
| 20–25 years | 262 (70.6) | 84 (22.6) | 129 (34.8) | 49 (13.2) | 122 (32.9) | 134 (36.1) | 6 (1.6) | |||
| >25 years | 79 (21.3) | 37 (10) | 28 (7.5) | 14 (3.8) | 46 (12.4) | 26 (7) | 7 (1.9) | |||
| Nationality | Saudi | 286 (77.1) | 110 (29.6) | 122 (32.9) | 54 (14.6) | 0.017 * | 144 (38.8) | 129 (34.8) | 13 (3.5) | 0.130 |
| Non-Saudi | 85 (22.9) | 13 (3.5) | 51 (13.7) | 21 (5.7) | 34 (9.2) | 49 (13.2) | 2 (0.5) | |||
| Student situation | Full time student | 291 (78.4) | 88 (23.7) | 146 (39.4) | 57 (15.4) | 0.006 * | 146 (39.4) | 138 (37.2) | 7 (1.9) | 0.006 * |
| Working student | 80 (21.6) | 35 (9.4) | 27 (7.3) | 18 (4.9) | 32 (8.6) | 40 (10.8) | 8 (2.2) | |||
| Family member in health sector | Yes | 218 (58.8) | 83 (22.4) | 103 (27.8) | 32 (8.6) | 0.02 * | 108 (29.1) | 99 (26.7) | 11 (3) | 0.896 |
| No | 153 (41.2) | 40 (10.8) | 70 (18.9) | 43 (11.6) | 70 (18.9) | 79 (21.3) | 4 (1.1) | |||
| Gender | Male | 143 (38.5) | 53 (14.3) | 53 (14.3) | 37 (10) | 0.051 | 57 (15.4) | 77 (20.8) | 9 (2.4) | 0.019 * |
| Female | 228 (61.5) | 70 (18.9) | 120 (32.3) | 38 (10.2) | 121 (32.6) | 101 (27.2) | 6 (1.6) | |||
| Study level/phase | Level 1–2 | 42 (11.3) | 9 (2.4) | 21 (5.7) | 12 (3.2) | 0.001 * | 18 (4.9) | 23 (6.2) | 1 (0.3) | 0.006 * |
| Level 3–4 | 102 (27.5) | 16 (4.3) | 48 (12.9) | 38 (10.2) | 48 (12.9) | 43 (11.6) | 11 (3) | |||
| Level 5–6 | 83 (22.4) | 26 (7) | 46 (12.4) | 11 (3) | 43 (11.6) | 39 (10.5) | 1 (0.3) | |||
| Level 7–8 | 71 (19.1) | 39 (10.5) | 26 (7) | 6 (1.6) | 24 (6.5) | 47 (12.7) | zero | |||
| Level 9–10 | 43 (11.6) | 23 (6.2) | 17 (4.6) | 3 (0.8) | 31 (8.4) | 12 (3.2) | zero | |||
| Level 11–12 | 20 (5.4) | 9 (2.4) | 9 (2.4) | 2 (0.5) | 10 (2.7) | 9 (2.4) | 1 (0.3) | |||
| Internship students | 10 (2.7) | 1 (0.3) | 6 (1.6) | 3 (0.8) | 4 (1.1) | 5 (1.3) | 1 (0.3) | |||
| GPA | 1–2 | 31 (8.4) | 8 (2.2) | 15 (4) | 8 (2.2) | 0.509 | 20 (5.4) | 11 (3) | zero | 0.291 |
| 2–3 | 154 (41.5) | 63 (17) | 62 (16.7) | 29 (7.8) | 67 (18.1) | 82 (22.1) | 5 (1.3) | |||
| 3–4 | 186 (50.1) | 52 (14) | 96 (25.9) | 38 (10.2) | 91 (24.5) | 85 (22.9) | 10 (2.7) | |||
| BMI | Below 18.5 | 35 (9.43) | 7 (1.9) | 17 (4.6) | 11 (3) | 0.023 * | 26 (7) | 9 (2.42) | zero | 0.388 |
| 18.5 to 24.9 | 200 (53.9) | 77 (20.8) | 92 (24.8) | 31 (8.4) | 132 (35.6) | 62 (16.7) | 6 (1.6) | |||
| 25 to 29.9 | 93 (25.1) | 20 (5.4) | 47 (12.7) | 26 (7) | 59 (15.9) | 27 (7.3) | 7 (1.9) | |||
| 30 and above | 43 (11.6) | 19 (5.1) | 17 (4.6) | 7 (1.9) | 31 (8.4) | 10 (2.7) | 2 (0.53) | |||
| Residential status | Living with family | 299 (80.6) | 93 (25.1) | 141 (38) | 65 (17.5) | 0.424 | 137 (36.9) | 155 (41.8) | 7 (1.9) | 0.001 * |
| University accommodation | 10 (2.7) | 3 (0.8) | 7 (1.9) | zero | 10 (2.7) | zero | zero | |||
| Non-university accommodation | 62 (16.7) | 27 (7.3) | 25 (6.7) | 10 (2.7) | 31 (8.4) | 23 (6.2) | 8 (2.2) | |||
| Marital status | Single | 324 (87.3) | 102 (27.5) | 155 (41.8) | 67 (18.1) | 0.775 | 159 (42.9) | 155 (41.8) | 10 (2.7) | 0.009 * |
| Married | 41 (11.1) | 18 (4.9) | 15 (4) | 8 (2.2) | 18 (4.9) | 18 (4.9) | 5 (1.3) | |||
| Divorced/separated | 6 (1.6) | 3 (0.8) | 3 (0.8) | zero | 1 (0.3) | 5 (1.3) | zero | |||
| Presence of long term/chronic disease | No | 324 (87.3) | 95 (25.6) | 159 (42.9) | 70 (18.9) | 0.804 | 151 (40.7) | 160 (43.1) | 13 (3.5) | 0.053 |
| Yes | 47 (12.7) | 28 (7.5) | 14 (3.8) | 5 (1.3) | 27 (7.3) | 18 (4.9) | 2 (0.5) | |||
| Demographic Variable | Mean Knowledge Score (7-Point Scale) | Mean Attitude Score (20-Point Scale) | |
| Colleges | Pharmacy | 5.18 | 16.72 |
| Medicine | 4.81 | 16.04 | |
| Applied Sciences | 4.1 | 16.3 | |
| Age | <20 years | 3.7 | 15.96 |
| 20–25 years | 4.69 | 16.37 | |
| >25 years | 5.17 | 16.73 | |
| Nationality | Saudi | 4.83 | 16.51 |
| Non-Saudi | 4.3 | 16.1 | |
| Student situation | Full time student | 4.65 | 16.51 |
| Working student | 4.93 | 16.06 | |
| Family member in health sector | Yes | 4.94 | 16.41 |
| No | 4.39 | 16.41 | |
| Gender | Male | 4.66 | 16.1 |
| Female | 4.75 | 16.6 | |
| Study level/phase | Level 1–2 | 4.21 | 16.11 |
| Level 3–4 | 3.99 | 16.02 | |
| Level 5–6 | 4.85 | 16.66 | |
| Level 7–8 | 5.5 | 16.29 | |
| Level 9–10 | 5.27 | 17.3 | |
| Level 11–12 | 5.1 | 16.5 | |
| Internship students | 4.3 | 16.5 | |
| GPA | 1–2 | 4.45 | 17.45 |
| 2–3 | 4.85 | 16.25 | |
| 3–4 | 4.64 | 16.37 | |
| BMI | Below 18.5 | 4.24 | 16.48 |
| 18.5 to 24.9 | 4.93 | 16.47 | |
| 25 to 29.9 | 4.4 | 16.26 | |
| 30 and above | 4.73 | 16.46 | |
| Residential status | Living with family | 4.63 | 16.4 |
| University accommodation | 5 | 17.7 | |
| Non-university accommodation | 5.06 | 16.27 | |
| Marital status | Single | 4.66 | 16.42 |
| Married | 5.02 | 16.36 | |
| Divorced/separated | 5.33 | 16.5 | |
| Presence of long term/chronic disease | No | 4.6 | 16.34 |
| Yes | 5.51 | 16.89 | |
| Self-Medication Practice Information | Sample (N) | Percentage |
|---|---|---|
| During the last six months did you self-medicate yourself? | ||
| Yes | 206 | 55.5 |
| No | 165 | 44.5 |
| Frequency of practice (I used self-medication drug) | ||
| During last month | 126 | 34.0 |
| During the last three months | 80 | 21.6 |
| During the last six months | 165 | 44.5 |
| Place of obtaining the medication for self-use | ||
| Pharmacy store | 347 | 93.53 |
| Family/friends | 60 | 16.17 |
| Supermarket | 20 | 5.39 |
| Internet/online | 27 | 7.27 |
| Source of drug information | ||
| Previous prescription | 150 | 40.43 |
| Friends/relatives | 50 | 13.47 |
| Media | 25 | 6.73 |
| Internet | 110 | 29.64 |
| Parent | 30 | 8.08 |
| Academic knowledge and book | 200 | 53.9 |
| Other | 33 | 8.89 |
| Practice of Self-Medication During Last Six Months | p-Value | Cremer’s V | Odds Ratio (Risk Estimate) | |||||
|---|---|---|---|---|---|---|---|---|
| Category | Subgroup | 95% confidence interval | ||||||
| No (%) | Yes (%) | 0.011 * | 0.132 | Value | Lower | Upper | ||
| Family member working in health sector? | ||||||||
| Yes | 85 (22.9) | 133 (35.8) | 0.583 | 0.384 | 0.886 | |||
| No | 80 (21.6) | 73 (19.7) | ||||||
| Do you suffer from any long term/chronic disease? | Yes | 12 (3.2) | 35 (9.4) | 0.005 * | 0.145 | 2.610 | 1.308 | 5.208 |
| No | 153 (41.2) | 171 (46.1) | ||||||
| Colleges | Pharmacy | 58 (15.63) | 95 (25.60) | 0.033 * | 0.111 | 0.633 | 0.416 | 0.965 |
| Medicine & Applied Sciences | 107 (28.8) | 111 (29.9) | ||||||
| Gender | Male | 63 (17) | 80 (21.6) | 0.898 | 0.007 | 0.973 | 0.639 | 1.482 |
| Female | 102 (27.5) | 126 (34) | ||||||
| Nationality | Saudi | 130 (35) | 156 (42) | 0.486 | 0.036 | 1.190 | 0.729 | 1.945 |
| Non-Saudi | 35 (9.4) | 50 (13.5) | ||||||
| Student situation | Full time student | 127 (34.2) | 164 (44) | 0.539 | 0.032 | 0.856 | 0.521 | 1.406 |
| Working student | 38 (10.2) | 42 (11.3) | ||||||
| Independent Variable | Regression Coefficient β | Standard Error | Standardized Regression Coefficient β | t | p-Value |
|---|---|---|---|---|---|
| Constant term | 18.756 | 1.129 | --- | 16.616 | 0.000 |
| College | −0.687 | 0.164 | −0.212 | −4.189 | 0.000 |
| Nationality | −0.851 | 0.336 | −0.127 | −2.534 | 0.012 |
| Age | 0.967 | 0.284 | 0.180 | 3.400 | 0.001 |
| Gender | 1.111 | 0.292 | 0.191 | 3.801 | 0.000 |
| Level of study | 0.254 | 0.096 | 0.135 | 2.641 | 0.009 |
| Do you suffer from any long term/chronic disease? | 0.123 | 0.051 | 0.115 | 2.394 | 0.017 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mannasaheb, B.A.; Al-Yamani, M.J.; Alajlan, S.A.; Alqahtani, L.M.; Alsuhimi, S.E.; Almuzaini, R.I.; Albaqawi, A.F.; Alshareef, Z.M. Knowledge, Attitude, Practices and Viewpoints of Undergraduate University Students towards Self-Medication: An Institution-Based Study in Riyadh. Int. J. Environ. Res. Public Health 2021, 18, 8545. https://doi.org/10.3390/ijerph18168545
Mannasaheb BA, Al-Yamani MJ, Alajlan SA, Alqahtani LM, Alsuhimi SE, Almuzaini RI, Albaqawi AF, Alshareef ZM. Knowledge, Attitude, Practices and Viewpoints of Undergraduate University Students towards Self-Medication: An Institution-Based Study in Riyadh. International Journal of Environmental Research and Public Health. 2021; 18(16):8545. https://doi.org/10.3390/ijerph18168545
Chicago/Turabian StyleMannasaheb, Basheerahmed Abdulaziz, Mohammed Jaber Al-Yamani, Sarah Abdulrahman Alajlan, Lamyaa Munahi Alqahtani, Shrouq Eid Alsuhimi, Razan Ibrahim Almuzaini, Abeer Fahad Albaqawi, and Zahaa Majed Alshareef. 2021. "Knowledge, Attitude, Practices and Viewpoints of Undergraduate University Students towards Self-Medication: An Institution-Based Study in Riyadh" International Journal of Environmental Research and Public Health 18, no. 16: 8545. https://doi.org/10.3390/ijerph18168545
APA StyleMannasaheb, B. A., Al-Yamani, M. J., Alajlan, S. A., Alqahtani, L. M., Alsuhimi, S. E., Almuzaini, R. I., Albaqawi, A. F., & Alshareef, Z. M. (2021). Knowledge, Attitude, Practices and Viewpoints of Undergraduate University Students towards Self-Medication: An Institution-Based Study in Riyadh. International Journal of Environmental Research and Public Health, 18(16), 8545. https://doi.org/10.3390/ijerph18168545