1. Introduction
In 2020, the World Health Organization (WHO) declared a “public health emergency of international concern (PHEIC)” due to the worldwide spread of coronavirus disease-19 (COVID-19), declaring the situation a “pandemic” [
1]. Despite government measures to contain COVID-19 outbreaks, more than 198 million confirmed cases and more than 4.2 million deaths have occurred worldwide as of the end of July 2021, and 42,000 new deaths and three million new cases of COVID-19 are being reported each day [
2]. In addition, the dramatic changes and threats brought about by the COVID-19 pandemic have had a profound impact on mental as well as physical health. Although many previous clinical studies have been conducted worldwide to develop a vaccine for COVID-19, its impact on mental health and related services has been largely underestimated [
3,
4]. Given the increasing number of mental health problems associated with physical illness, systematic investigations in these areas are necessary to understand the extent of the issue and apply therapeutic and preventive strategies [
5,
6].
According to a recent study, over 25% of the population in China has experienced severe symptoms related to anxiety and stress due to unexpected and unusual situations and fears caused by COVID-19 [
7]. A study of Korean adults reported that after the COVID-19 outbreak in Korea, 42.8%, 36.1%, and 23.6% of the individuals reported experiences of depression, anxiety, and stress, respectively [
8]. Moreover, in the case of the United Kingdom, a study on mental health after the onset of the COVID-19 pandemic showed an increase in mental health problems in 10.3% and 16.4% of men and women, respectively [
9]. Adolescents in particular have encountered mental health concerns such as anxiety, depression, and obsessive–compulsive disorder due to the continuous stress imposed by COVID-19 [
6,
10,
11]. Current evidence suggests that these mental health areas are closely related to physical activity, which is known to be effective in maintaining and improving mental health [
12]. Indeed, physical activity in adolescents not only affects health treatment and outcomes (e.g., bone density, physical activity in adulthood), but also relieves symptoms of psychological tension such as stress, depression, and anxiety [
13]. In other words, the data suggest that there is a significant correlation between sports activity and stress levels in adolescents.
Stress exhibits a well-known association with self-regulation. Self-regulation is a mental and behavioral process that results in conformity with the self-concept and personal goals by putting one’s self-concept into action, modifying one’s behavior, or changing the external environment [
14]. In adolescence, the ability to control impulses and carefully plan, solve, and evaluate problems related to oneself becomes necessary. Research has indicated that self-regulation is related to the process of resource depletion [
15]. Intentional efforts to increase flexibility and adaptability to the environment by controlling oneself are processes that consume limited resources. Due to the limited nature of self-regulation described in terms of the strength model or ego depletion, those who continue to self-regulate beyond limitations experience fatigue, resulting in a failure to self-regulate [
16]. Accordingly, further research is required to identify the variables that prevent failure of self-regulation due to fatigue, such as skill, motivation, fatigue, self-efficacy, emotion, and personality variables [
17].
Therefore, when examining the relationship between self-regulation and stress, it is necessary to investigate the control variables that can prevent fatigue of self-regulation, enable self-regulation, and consequently reduce stress. Optimism, which can be considered a moderator variable, is a belief that good things will happen in one’s life [
18], and it is a concept that reflects positive and hopeful emotions for the future. Positive emotions have the effect of offsetting negative emotions [
19], and positive emotions resulting from an optimistic attitude can attenuate negative emotions and fatigue associated with self-regulation. In fact, studies have reported that optimism positively affects stress and plays a key role in improving self-regulation [
20]. In addition, optimism allows self-regulation to continue even in difficult situations [
21]. Therefore, optimism is thought to not only affect stress, but also the influence of self-regulation on stress.
As noted above, previous research has demonstrated a positive relationship between participation in physical activity and self-regulation. In addition, participation in physical activity, optimism, and self-regulation exert a negative effect on stress. However, these studies have only examined partial relationships between the factors, such as the relationship between physical activity and self-regulation [
22] or that between self-regulation and stress [
23]. This is limited in that it does not provide information regarding the comprehensive structural relationships between participation in physical activity, optimism/pessimism, self-regulation, and stress. In addition, very few studies have measured the stress of adolescents arising from the special circumstances of COVID-19. For example, it is difficult to directly participate in physical activities due to pandemic-related measures such as social distancing, restrictions on the use of schools and external sports facilities, conversion of physical education classes to the online format, and restrictions on watching sports in person. Given this situation, the number of studies investigating measures that can help alleviate “COVID-19-related stress” among adolescents remains insufficient.
Therefore, in this study, we empirically investigated the relationships between participation in sports, optimism/pessimism, self-regulation, and coronavirus-related stress among adolescents. Specifically, we aimed to provide practical information that can minimize stress among adolescents in the context of COVID-19. To achieve this goal, the following research hypotheses were established based on previous studies and various theories. First, we hypothesized that there would be differences in sports participation, optimism, pessimism, self-regulation, and coronavirus-related stress according to sex, school level, frequency of physical activity participation per week, amount of time spent engaged in physical activity, and duration of physical activity participation (Hypothesis 1). Second, that sports participation would positively/negatively affect optimism, pessimism, self-regulation, and coronavirus-related stress (Hypothesis 2). Third, that optimism and pessimism would positively/negatively affect self-regulation and coronavirus-related stress (Hypothesis 3). Fourth, that self-regulation would exert a negative effect on coronavirus-related stress (Hypothesis 4).
4. Discussion
This study investigated the relationships between participation in sports, optimism/pessimism, self-regulation, and coronavirus-related stress among Korean adolescents in the context of the COVID-19 pandemic. First, there were significant differences in each variable according to demographic characteristics. Specifically, for all the sub-variables of sports participation, scores were significantly higher among the male students than among the female students. Scores for the pessimism variable were significantly lower among the male students than among the female students, while those for optimism were significantly higher among the male students than among the female students. Scores for self-regulation were significantly higher for the male students than for the female students, while those for coronavirus-related stress were significantly lower among the male students than among the female students. These results are consistent with those of Shevlin et al. [
34] and Lee [
29] who reported similar results for middle and high school students. However, given that Qi et al. [
35] reported no sex differences in stress due to COVID-19, follow-up studies are required.
No significant differences in the variables related to sports participation, optimism, or self-regulation ability were observed according to school level. In terms of coronavirus-related stress, scores for the compulsive category were significantly lower among the middle school students than among the high school students. The finding that there is no difference in physical activity participation between middle school students and high school students is inconsistent with some previous studies [
36,
37]. The school curriculum significantly affects the physical activity of adolescents [
36]; however, due to COVID-19, the students were not engaged in the physical activity typically performed at school (physical education time, sports club time). This may explain the similarity in the level of physical activity participation between the middle school students and the high school students, as similar findings have been reported for situations in which physical activity is restricted, such as prohibition of the use of sports facilities in schools [
29].
In addition, higher levels of physical activity (frequency, intensity, and duration), were associated with higher scores for sports participation, optimism, and self-regulation and with lower scores for pessimism and coronavirus-related stress. These results are in line with those of Koo and Lee [
38] who reported that participation in a physical activity-based recreation program had a positive effect on optimism in terms of frequency, intensity, and duration. In addition, according to the study by Qi et al. [
35] which found a negative correlation between the level of physical activity and coronavirus-related stress, individuals who engaged in regular physical activity had higher levels of self-esteem, optimism, and happiness than those who were not physically active. Cekin [
39] further highlighted this possibility, in support of the findings presented herein. In particular, Kybartas et al. [
40] reported that moderate-intensity physical activity is not correlated with improvements in self-regulation, although correlations were observed for high-intensity physical activity. This is very similar to the results of this study, in which differences between each variable occurred only for high-intensity and long-term physical activity.
The findings presented herein indicate that sports participation had a positive effect on optimism and a negative effect on pessimism in Korean adolescents. Pavey et al. [
41] observed a significant relationship between physical activity and optimism in young and middle-aged women, supporting the results reported herein. Thus, evidence suggests that physical activity plays an important role in creating a positive cognitive attitude toward the future [
39] and that social and environmental changes should be initiated to promote physical activity among adolescents.
Sports participation had a statistically significant positive effect on self-regulation in Korean adolescents. This result is related to the finding that physical activity impacts the formation of a positive self-concept [
22]. In addition, it is in line with the finding that the students who engaged in physical activity less frequently and were passive when engaged in physical activity were more prone to psychological problems such as depression and anxiety [
42].
Sports participation exerted a statistically significant negative effect on coronavirus-related stress. Vogel et al. [
43] reported that the participants who engaged in physical activity experienced lower levels of coronavirus-related stress than the inactive participants using stress-relieving strategies such as talking or playing with friends and family, exercising outdoors, and listening to music. This is consistent with the results of this study. These results are also consistent with a previous study on Chinese adolescents with similar environmental and physical conditions as those of Korean adolescents. As a result, physiological exercise helped alleviate negative emotions. Further, it has been shown that negative emotions may be alleviated more significantly with weekly physical activity of 2500 metabolic equivalents of energy [
44].
Optimism exerted a positive effect on self-regulation, while pessimism exerted a negative effect on self-regulation. This result is in accordance with the previous finding [
21] that optimistic individuals can engage in self-regulation for a longer period of time. Thus, when self-regulation ability is high, individuals can continue to perform tasks that require persistence for a longer duration. In addition, optimism plays an important role in sustaining and enhancing self-regulation [
20,
45,
46,
47], which is in agreement with the results reported herein. As such, optimistic people are more likely to engage in many goals simultaneously, and this characteristic increases their chances of achieving them in the long run. On the other hand, some studies have reported that optimistic individuals may struggle with conflicting goals in the short term [
48]. Based on the results of previous studies, it can be inferred that adolescents with high optimism can handle stress well because of their high self-regulation ability. However, personally dealing with continuous stress during adolescence may lead to the accumulation of latent stress and cause greater conflict. Therefore, it is important to think about ways to increase the ability to overcome stress through appropriate physical activity rather than through simply avoiding stress.
The results reported herein also indicated that optimism exerts a negative effect on coronavirus-related stress, while pessimism exerts a positive effect on coronavirus-related stress, consistent with previous findings [
18,
48]. These results are also consistent with those of Reed [
49] who investigated the mediating role of optimism between stress and life satisfaction. This suggests that people with higher levels of coronavirus-related stress are more likely to view psychological problems with more pessimism and less optimism. This may explain how stress can lead to greater pessimism and how low optimism can result in greater psychological problems [
50,
51,
52,
53]. Additionally, the beneficial effects of high levels of optimism and low levels of pessimism suggest the need to think about ways to develop optimism as it can aid individuals in overcoming coronavirus-related stress and attenuate psychological symptoms. In this study, self-regulation exerted a negative effect on coronavirus-related stress. This result is consistent with the finding that self-regulation style has a negative effect on stress [
54,
55]. In other words, self-regulation that relies on strategies that are in harmony with the self can help to reduce coronavirus-related stress.
This study had some limitations. In this work, meaningful results were derived by setting the degree of sports participation, optimism and pessimism, and self-regulation as variables that can affect coronavirus-related stress. However, diverse variables can influence coronavirus-related stress, many of which may not have been included in this study. Therefore, a multidimensional analysis that includes additional variables with the potential to impact coronavirus-related stress is required. Second, only Korean adolescents were assessed in this study; therefore, it would not be appropriate to generalize the study results to other ethnicities. Future studies should perform these assessments in populations that reflect the various characteristics of different ethnicities.


 self-regulation ability”, which had the highest correlation, was 0.491, which was lower than the AVEs for optimism (0.547) and pessimism (0.588). Thus, discriminant validity between the variables was secured.
self-regulation ability”, which had the highest correlation, was 0.491, which was lower than the AVEs for optimism (0.547) and pessimism (0.588). Thus, discriminant validity between the variables was secured.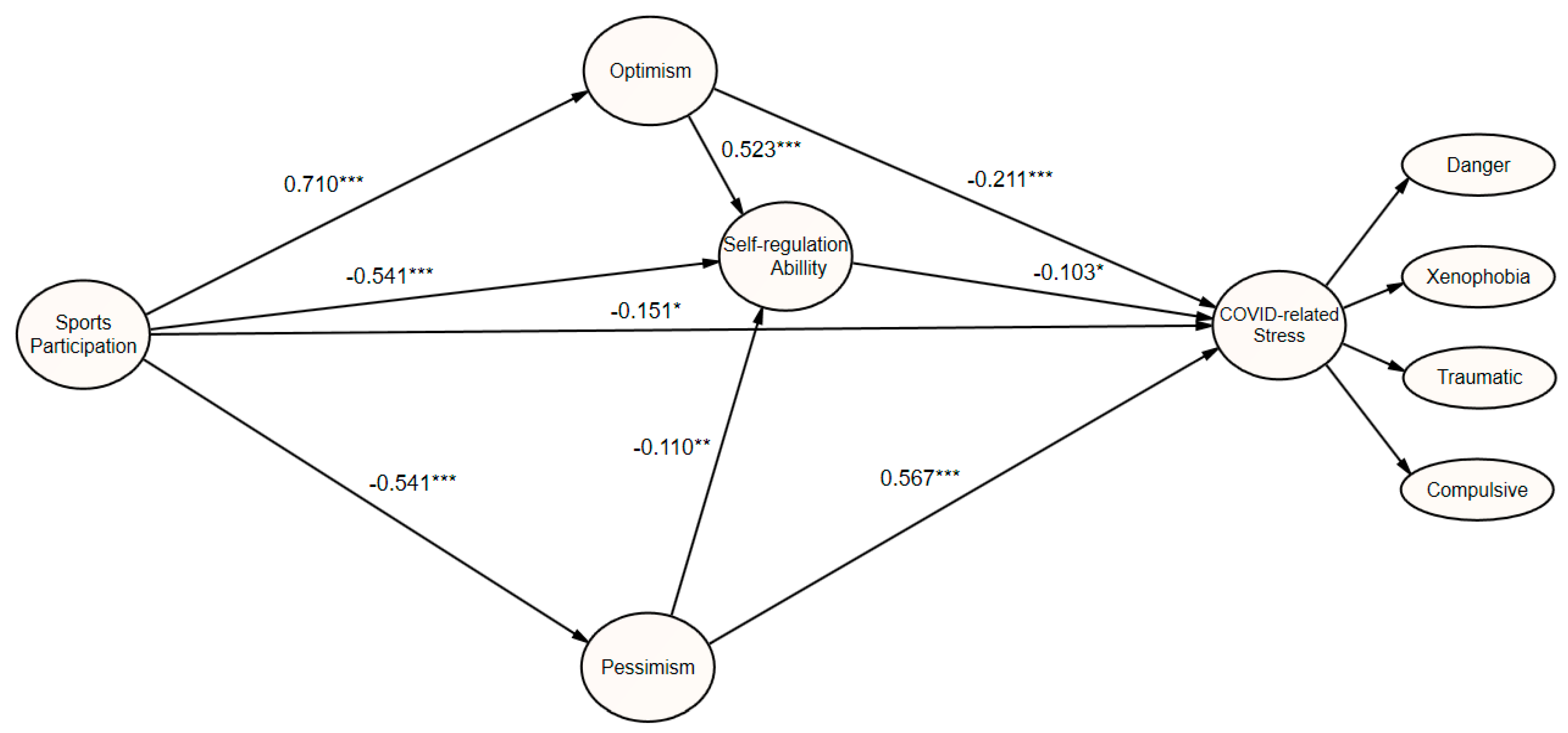

{kind=link}