
Experiential Learning Interventions and Healthy Eating Outcomes in Children: A Systematic Literature Review

 ,
,  , , ,
, , , 
 and
and 
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection
2.4. Data Extraction
2.5. Risk of Bias Appraisal
2.6. Data Synthesis and Analysis
3. Results
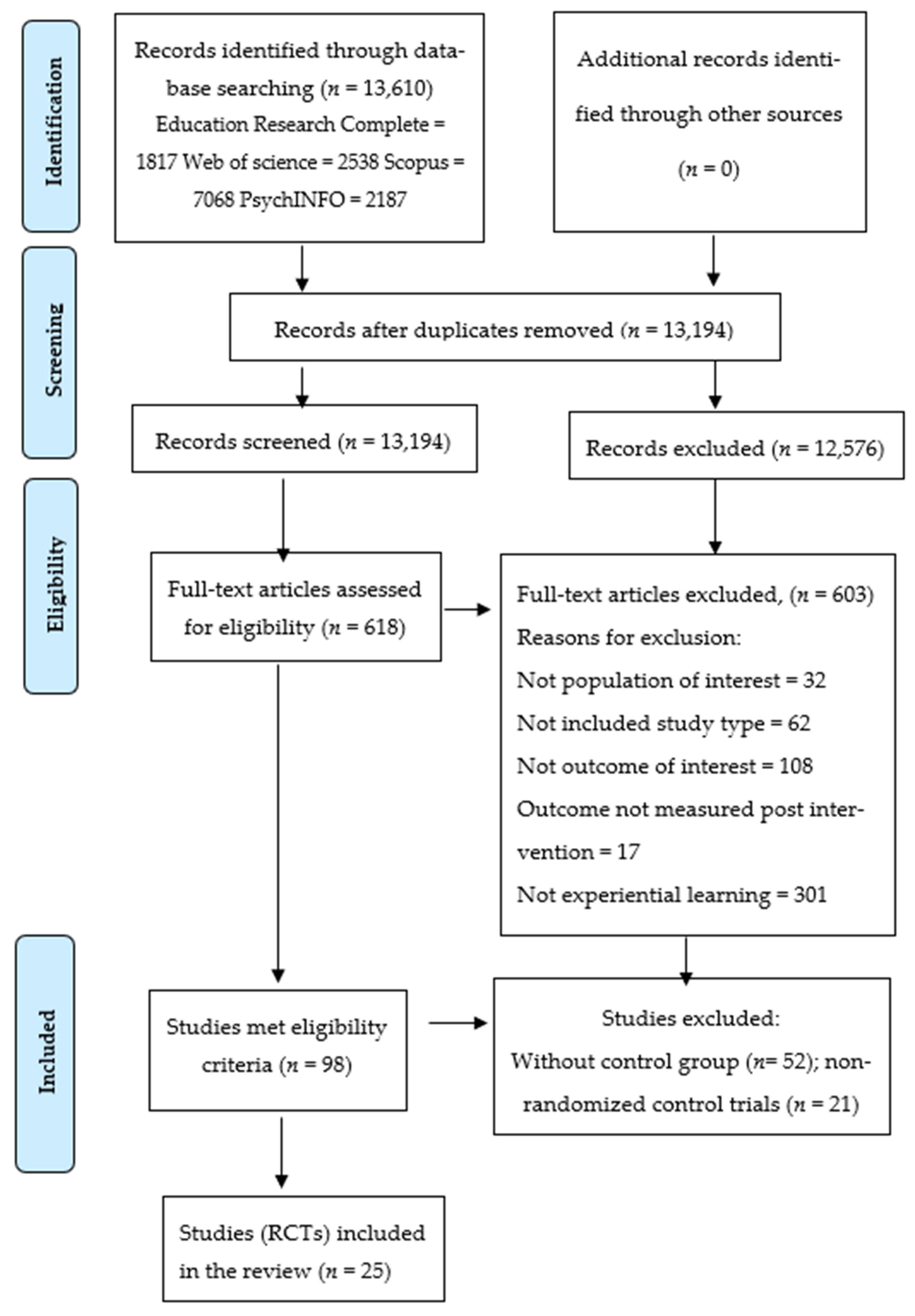
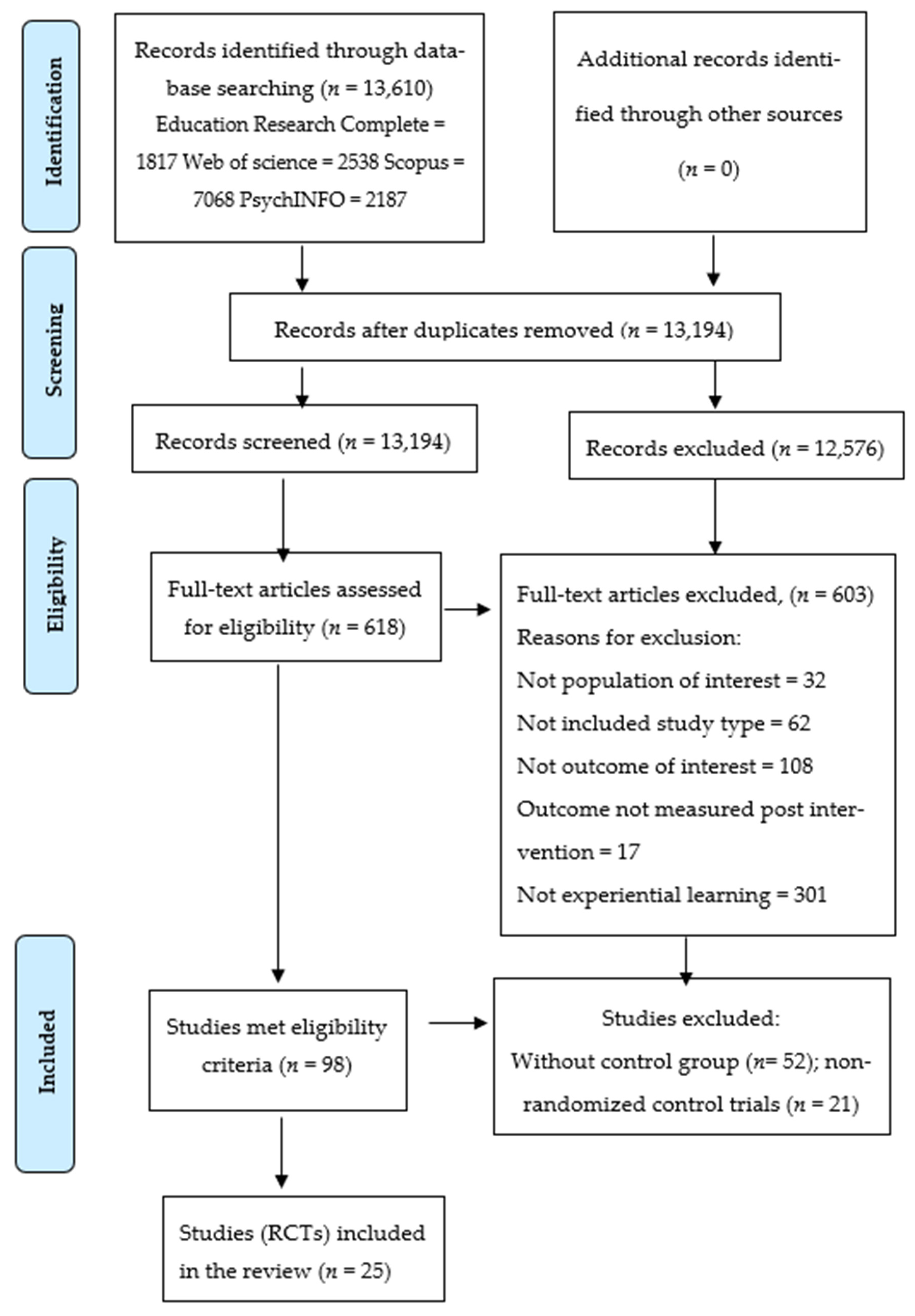
3.1. Study Selection
3.2. Study and Intervention Characteristics
3.3. Experiential Learning Activities
3.4. Intervention Effects
4. Discussion
4.1. Main Findings
4.2. Implications for Interventions
4.3. Implications for Future Research
4.4. Implications for Policy
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- National Cancer Control Indicators. Overweight and Obesity–Children and Young People. Available online: https://ncci.canceraustralia.gov.au/prevention/overweight-and-obesity/overweight-and-obesity-children-and-young-people (accessed on 25 January 2021).
- World Health Organization. Global Strategy on Diet, Physical Activity and Health: Childhood Overweight and Obesity. Available online: http://www.who.int/dietphysicalactivity/childhood/en/ (accessed on 15 February 2019).
- Kelly, A.S.; Barlow, S.E.; Rao, G.; Inge, T.H.; Hayman, L.L.; Steinberger, J.; Urbina, E.M.; Ewing, L.J.; Daniels, S.R. Severe obesity in children and adolescents: Identification, associated health risks, and treatment approaches: A scientific statement from the American Heart Association. Circulation 2013, 128, 1689–1712. [Google Scholar] [CrossRef]
- World Health Organisation. Why Does Childhood Overweight and Obesity Matter? Available online: https://www.who.int/dietphysicalactivity/childhood_consequences/en/ (accessed on 8 January 2021).
- Pulgaron, E.R.; Delamater, A.M. Obesity and type 2 diabetes in children: Epidemiology and treatment. Curr. Diabetes Rep. 2014, 14, 508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raj, M. Obesity and cardiovascular risk in children and adolescents. Indian J. Endocrinol. Metab. 2012, 16, 13. [Google Scholar] [CrossRef] [PubMed]
- Birch, L.L.; Anzman, S.L. Learning to eat in an obesogenic environment: A developmental systems perspective on childhood obesity. Child Dev. Perspect. 2010, 4, 138–143. [Google Scholar] [CrossRef]
- Lynch, C.; Kristjansdottir, A.G.; Te Velde, S.J.; Lien, N.; Roos, E.; Thorsdottir, I.; Krawinkel, M.; de Almeida, M.D.V.; Papadaki, A.; Ribic, C.H. Fruit and vegetable consumption in a sample of 11-year-old children in ten European countries–the PRO GREENS cross-sectional survey. Public Health Nutr. 2014, 17, 2436–2444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Australian Bureau of Statistics. Australian Health Survey: Users’ Guide, 2011–2013. Available online: http://www.ausstats.abs.gov.au/ausstats/subscriber.nsf/0/734DF823586D5AD9CA257B8E0014A387/$File/national%20nutrition%20and%20physical%20activity%20survey%202011-12%20questionnaire.pdf (accessed on 23 April 2019).
- Cockroft, J.; Durkin, M.; Masding, C.; Cade, J. Fruit and vegetable intakes in a sample of pre-school children participating in the ‘Five for All’project in Bradford. Public Health Nutr. 2005, 8, 861–869. [Google Scholar] [CrossRef] [Green Version]
- Yngve, A.; Wolf, A.; Poortvliet, E.; Elmadfa, I.; Brug, J.; Ehrenblad, B.; Franchini, B.; Haraldsdóttir, J.; Krølner, R.; Maes, L. Fruit and vegetable intake in a sample of 11-year-old children in 9 European countries: The Pro Children Cross-sectional Survey. Ann. Nutr. Metab. 2005, 49, 236–245. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Diet, Nutrition, and the Prevention of Chronic Diseases: Report of a Joint WHO/FAO Expert Consultation; World Health Organization: Geneva, Switzerland, 2003; Volume 916. [Google Scholar]
- Bannon, K.; Schwartz, M.B. Impact of nutrition messages on children’s food choice: Pilot study. Appetite 2006, 46, 124–129. [Google Scholar] [CrossRef]
- Mikkilä, V.; Räsänen, L.; Raitakari, O.; Pietinen, P.; Viikari, J. Consistent dietary patterns identified from childhood to adulthood: The cardiovascular risk in Young Finns Study. Br. J. Nutr. 2005, 93, 923–931. [Google Scholar] [CrossRef]
- Luque, V.; Escribano, J.; Closa-Monasterolo, R.; Zaragoza-Jordana, M.; Ferré, N.; Grote, V.; Koletzko, B.; Totzauer, M.; Verduci, E.; ReDionigi, A. Unhealthy dietary patterns established in infancy track to mid-childhood: The EU childhood obesity project. J. Nutr. 2018, 148, 752–759. [Google Scholar] [CrossRef]
- Movassagh, E.Z.; Baxter-Jones, A.D.; Kontulainen, S.; Whiting, S.J.; Vatanparast, H. Tracking dietary patterns over 20 years from childhood through adolescence into young adulthood: The Saskatchewan Pediatric Bone Mineral Accrual Study. Nutrients 2017, 9, 990. [Google Scholar] [CrossRef] [PubMed]
- Lioret, S.; McNaughton, S.; Spence, A.; Crawford, D.; Campbell, K. Tracking of dietary intakes in early childhood: The Melbourne InFANT Program. Eur. J. Clin. Nutr. 2013, 67, 275–281. [Google Scholar] [CrossRef] [PubMed]
- World Cancer Research Fund. NOURISHING Framework. Available online: https://www.wcrf.org/int/policy/policy-databases/nourishing-framework (accessed on 10 March 2021).
- Jarpe-Ratner, E.; Folkens, S.; Sharma, S.; Daro, D.; Edens, N.K. An experiential cooking and nutrition education program increases cooking self-efficacy and vegetable consumption in children in grades 3–8. J. Nutr. Educ. Behav. 2016, 48, 697–705.e1. [Google Scholar] [CrossRef] [Green Version]
- Parmer, S.M.; Salisbury-Glennon, J.; Shannon, D.; Struempler, B. School gardens: An experiential learning approach for a nutrition education program to increase fruit and vegetable knowledge, preference, and consumption among second-grade students. J. Nutr. Educ. Behav. 2009, 41, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Hersch, D.; Perdue, L.; Ambroz, T.; Boucher, J.L. Peer reviewed: The impact of cooking classes on food-related preferences, attitudes, and behaviors of school-aged children: A systematic review of the evidence, 2003–2014. Prev. Chronic Dis. 2014, 11, E193. [Google Scholar] [CrossRef] [PubMed]
- Dudley, D.; Cotton, W.; Peralta, L. Teaching approaches and strategies that promote healthy eating in primary school students: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savoie-Roskos, M.R.; Wengreen, H.; Durward, C. Increasing fruit and vegetable intake among children and youth through gardening-based interventions: A systematic review. J. Acad. Nutr. Diet. 2017, 117, 240–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muliasari, D.N. Promoting Critical Thinking through Children’s Experiential Learning. In Proceedings of the 3rd International Conference on Early Childhood Education (ICECE 2016), Bandung, Indonesia, 11–12 November 2016. [Google Scholar]
- Illeris, K. What do we actually mean by experiential learning? Hum. Resour. Dev. Rev. 2007, 6, 84–95. [Google Scholar] [CrossRef] [Green Version]
- DeCosta, P.; Møller, P.; Frøst, M.B.; Olsen, A. Changing children’s eating behaviour-A review of experimental research. Appetite 2017, 113, 327–357. [Google Scholar] [CrossRef]
- Kolb, D.A. Experiential Learning: Experience as the Source of Learning and Development; Pearson Education, Inc.: Hoboken, NJ, USA, 2014. [Google Scholar]
- Dewey, J. Experience and education. In The Educational Forum; Taylor & Francis Group: England, UK, 1986; Volume 50, pp. 241–252. [Google Scholar] [CrossRef]
- Beloglovsky, M.; Daly, L. Early Learning Theories Made Visible; Redleaf Press: St Paul, MN, USA, 2015. [Google Scholar]
- Charlton, K.; Comerford, T.; Deavin, N.; Walton, K. Characteristics of successful primary school based experiential nutrition programs: A Systematic Literature Review. Public Health Nutr. 2020, 24, 4642–4662. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ-Brit. Med. J. 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Ortega, A.; Bejarano, C.M.; Cushing, C.C.; Staggs, V.S.; Papa, A.E.; Steel, C.; Shook, R.P.; Sullivan, D.K.; Couch, S.C.; Conway, T.L. Differences in adolescent activity and dietary behaviors across home, school, and other locations warrant location-specific intervention approaches. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Sterne, J.A.; Savovic, J.; Page, M.J.; Hróbjartsson, A.; Boutron, I.; Reeves, B.; Eldridge, S. A revised tool for assessing risk of bias in randomized trials. Cochrane Database Syst. Rev. 2016, 10, 29–31. [Google Scholar]
- Sterne, J.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. Available online: https://sites.google.com/site/riskofbiastool/welcome/rob-2-0-tool/current-version-of-rob-2 (accessed on 23 April 2021).
- Cohen, J. A Power Primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Laurence Erlbaum: Mahwah, NJ, USA, 1988; pp. 19–74. [Google Scholar]
- Vereecken, C.; Huybrechts, I.; Van Houte, H.; Martens, V.; Wittebroodt, I.; Maes, L. Results from a dietary intervention study in preschools “Beastly Healthy at School”. Int. J. Public Health 2009, 54, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Witt, K.E.; Dunn, C. Increasing fruit and vegetable consumption among preschoolers: Evaluation of Color Me Healthy. J. Nutr. Educ. Behav. 2012, 44, 107–113. [Google Scholar] [CrossRef]
- Brouwer, R.J.N.; Neelon, S.E. Watch Me Grow: A garden-based pilot intervention to increase vegetable and fruit intake in preschoolers. BMC Public Health 2013, 13, 363. [Google Scholar]
- Martínez-Andrade, G.O.; Cespedes, E.M.; Rifas-Shiman, S.L.; Romero-Quechol, G.; González-Unzaga, M.A.; Benítez-Trejo, M.A.; Flores-Huerta, S.; Horan, C.; Haines, J.; Taveras, E.M. Feasibility and impact of Creciendo Sanos, a clinic-based pilot intervention to prevent obesity among preschool children in Mexico City. BMC Pediatrics 2014, 14, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dazeley, P.; Houston-Price, C. Exposure to foods’ non-taste sensory properties. A nursery intervention to increase children’s willingness to try fruit and vegetables. Appetite 2015, 84, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jisoo, H.; Bales, D.W.; Wallinga, C.R. Using Family Backpacks as a Tool to Involve Families in Teaching Young Children About Healthy Eating. Early Child. Educ. J. 2018, 46, 209. [Google Scholar]
- Perry, C.L.; Bishop, D.B.; Taylor, G.; Murray, D.M.; Mays, R.W.; Dudovitz, B.S.; Smyth, M.; Story, M. Changing fruit and vegetable consumption among children: The 5-a-Day Power Plus program in St. Paul, Minnesota. Am. J. Public Health 1998, 88, 603–609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bere, E.; Veierød, M.; Bjelland, M.; Klepp, K.I. Free school fruit—Sustained effect 1 year later. Health Educ. Res. 2005, 21, 268–275. [Google Scholar] [CrossRef] [Green Version]
- Bere, E.; Veierd, M.B.; Bjelland, M.; Klepp, K.-I. Outcome and process evaluation of a Norwegian school-randomized fruit and vegetable intervention: Fruits and Vegetables Make the Marks (FVMM). Health Educ. Res. 2006, 21, 267. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.-L.; Weiss, S.; Heyman, M.B.; Lustig, R.H. Efficacy of a child-centred and family-based program in promoting healthy weight and healthy behaviors in Chinese American children: A randomized controlled study. J. Public Health 2009, 32, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Fulkerson, J.A.; Rydell, S.; Kubik, M.Y.; Lytle, L.; Boutelle, K.; Story, M.; Neumark-Sztainer, D.; Dudovitz, B.; Garwick, A.J.O. Healthy Home Offerings via the Mealtime Environment (HOME): Feasibility, acceptability, and outcomes of a pilot study. Obesity 2010, 18, S69–S74. [Google Scholar] [CrossRef] [Green Version]
- Rosenkranz, R.R.; Behrens, T.K.; Dzewaltowski, D.A. A group-randomized controlled trial for health promotion in Girl Scouts: Healthier troops in a SNAP (Scouting Nutrition & Activity Program). BMC Public Health 2010, 10, 81. [Google Scholar]
- Keihner, A.J.; Meigs, R.; Sugerman, S.; Backman, D.; Garbolino, T.; Mitchell, P. The Power Play! Campaign’s School Idea & Resource Kits improve determinants of fruit and vegetable intake and physical activity among fourth-and fifth-grade children. J. Nutr. Educ. Behav. 2011, 43, S122–S129. [Google Scholar]
- Katz, D.L.; Katz, C.S.; Treu, J.A.; Reynolds, J.; Njike, V.; Walker, J.; Smith, E.; Michael, J. Teaching healthful food choices to elementary school students and their parents: The Nutrition Detectives™ program. J. Sch. Health 2011, 81, 21–28. [Google Scholar] [CrossRef]
- Wall, D.E.; Least, C.; Gromis, J.; Lohse, B. Nutrition education intervention improves vegetable-related attitude, self-efficacy, preference, and knowledge of fourth-grade students. J. Sch. Health 2012, 82, 37–43. [Google Scholar] [CrossRef]
- Brown, B.; Noonan, C.; Harris, K.J.; Parker, M.; Gaskill, S.; Ricci, C.; Cobbs, G.; Gress, S. Developing and piloting the journey to native youth health program in Northern Plains Indian communities. Diabetes Educ. 2013, 39, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Habib-Mourad, C.; Ghandour, L.A.; Moore, H.J.; Nabhani-Zeidan, M.; Adetayo, K.; Hwalla, N.; Summerbell, C. Promoting healthy eating and physical activity among school children: Findings from Health-E-PALS, the first pilot intervention from Lebanon. BMC Public Health 2014, 14, 940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, N.M.; Myers, B.M.; Todd, L.E.; Barale, K.; Gaolach, B.; Ferenz, G.; Aitken, M.; Henderson, C.R.; Tse, C.; Pattison, K.O. The effects of school gardens on children’s science knowledge: A randomized controlled trial of low-income elementary schools. Int. J. Sci. Educ. 2015, 37, 2858–2878. [Google Scholar] [CrossRef]
- Allirot, X.; da Quinta, N.; Chokupermal, K.; Urdaneta, E. Involving children in cooking activities: A potential strategy for directing food choices toward novel foods containing vegetables. Appetite 2016, 103, 285. [Google Scholar] [CrossRef] [PubMed]
- LaChausse, R.G. A clustered randomized controlled trial to determine impacts of the Harvest of the Month program. Health Educ. Res. 2017, 32, 375–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schreinemachers, P.; Bhattarai, D.R.; Subedi, G.D.; Acharya, T.P.; Chen, H.-P.; Yang, R.-Y.; Kashichhawa, N.K.; Dhungana, U.; Luther, G.C.; Mecozzi, M. Impact of school gardens in Nepal: A cluster randomised controlled trial. J. Dev. Eff. 2017, 9, 329–343. [Google Scholar] [CrossRef]
- Schreinemachers, P.; Rai, B.B.; Dorji, D.; Chen, H.-P.; Dukpa, T.; Thinley, N.; Sherpa, P.L.; Yang, R.-Y. School gardening in Bhutan: Evaluating outcomes and impact. Food Secur. 2017, 9, 635–648. [Google Scholar] [CrossRef] [Green Version]
- Keihner, A.; Rosen, N.; Wakimoto, P.; Goldstein, L.; Sugerman, S.; Hudes, M.; Ritchie, L.; McDevitt, K. Impact of California Children’s Power Play! Campaign on fruit and vegetable intake and physical activity among fourth-and fifth-grade students. Am. J. Health Promot. 2017, 31, 189–191. [Google Scholar] [CrossRef] [PubMed]
- Scherr, R.E.; Linnell, J.D.; Dharmar, M.; Beccarelli, L.M.; Bergman, J.J.; Briggs, M.; Brian, K.M.; Feenstra, G.; Hillhouse, J.C.; Keen, C.L.; et al. A multicomponent, school-based intervention, the Shaping Healthy Choices Program, improves nutrition-related outcomes. J. Nutr. Educ. Behav. 2017, 49, 368–379.e1. [Google Scholar] [CrossRef] [PubMed]
- Allirot, X.; Maiz, E.; Urdaneta, E. Shopping for food with children: A strategy for directing their choices toward novel foods containing vegetables. Appetite 2018, 120, 296. [Google Scholar] [CrossRef]
- Christian, M.S.; Evans, C.E.; Nykjaer, C.; Hancock, N.; Cade, J.E. Evaluation of the impact of a school gardening intervention on children’s fruit and vegetable intake: A randomised controlled trial. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 99. [Google Scholar] [CrossRef] [Green Version]
- Hutchinson, J.; Christian, M.S.; Evans, C.E.L.; Nykjaer, C.; Hancock, N.; Cade, J.E. Evaluation of the impact of school gardening interventions on children’s knowledge of and attitudes towards fruit and vegetables. A cluster randomised controlled trial. Appetite 2015, 91, 405–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gold, A.; Larson, M.; Tucker, J.; Strang, M. Classroom nutrition education combined with fruit and vegetable taste testing improves children’s dietary intake. J. Sch. Health 2017, 87, 106–113. [Google Scholar] [CrossRef]
- Ng, C.M.; Kaur, S.; Koo, H.C.; Mukhtar, F. Involvement of children in hands-on meal preparation and the associated nutrition outcomes: A scoping review. J. Hum. Nutr. Diet. 2021. [Google Scholar] [CrossRef] [PubMed]
- Minich, D.M. A review of the science of colorful, plant-based food and practical strategies for “eating the rainbow”. J. Nutr. Metab. 2019, 2019, 1–19. [Google Scholar] [CrossRef]
- Anderson, E.S.; Winett, R.A.; Wojcik, J.R. Self-regulation, self-efficacy, outcome expectations, and social support: Social cognitive theory and nutrition behavior. Ann. Behav. Med. 2007, 34, 304–312. [Google Scholar] [CrossRef]
- Bandura, A. Health promotion by social cognitive means. Health Educ. Behav. 2004, 31, 143–164. [Google Scholar] [CrossRef] [PubMed]
- Nicklaus, S. The role of food experiences during early childhood in food pleasure learning. Appetite 2016, 104, 3–9. [Google Scholar] [CrossRef]
- Houston-Price, C.; Butler, L.; Shiba, P. Visual exposure impacts on toddlers’ willingness to taste fruits and vegetables. Appetite 2009, 53, 450–453. [Google Scholar] [CrossRef]
- Gross, S.M.; Pollock, E.D.; Braun, B. Family influence: Key to fruit and vegetable consumption among fourth-and fifth-grade students. J. Nutr. Educ. Behav. 2010, 42, 235–241. [Google Scholar] [CrossRef]
- Micha, R.; Karageorgou, D.; Bakogianni, I.; Trichia, E.; Whitsel, L.P.; Story, M.; Penalvo, J.L.; Mozaffarian, D. Effectiveness of school food environment policies on children’s dietary behaviors: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0194555. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| PICO | Booleans | Search Terms |
|---|---|---|
| Population | “Child*” OR “Preschool” OR “Elementary school” OR “Elementary student” OR “Elementary education” OR “Grade 1” OR “Grade 2” OR “Grade 3” OR “Grade 4” OR “Grade 5” OR “Grade 6” OR “Kindergarten” OR “Primary education” OR “Primary school” OR “Early years” | |
| Intervention | AND | “Play-based learning” OR “Learning through play” OR “Experiential learning” OR “Learning centered play” OR “Student-centered learning” OR “Guided play” OR “Facilitated play” OR “Play-based education” OR “Play education” OR “Educati* Activ*” OR “Interactive learning” OR “Playful pedagogy” OR “Active learning” OR “Experiential education” OR “Experience-based learning” OR “Program*” OR “Intervention” OR “Workshop” OR “Promotion” OR “Project” |
| Outcome | AND | “Nutrition*” OR “Food” OR “Diet*” OR “Eating habits” OR “Fruit” OR “Vegetable” OR “Healthy eating” |
| Authors (Year) Country | Study Design/ Theory | Sample Size, Age/Grade Involved Parent | Setting, Duration, Experiential Learning Activity | Measures/ Tools | Results | Overall Risk of Bias |
|---|---|---|---|---|---|---|
| Studies conducted in a preschool setting (<5 years old children) | ||||||
| Vereecken et al., (2009) Belgium [38] | RCT IMP | N = 1063 2–3 years No | Preschools. Six months. Tasting food, role- modelling (story and characters) | Changes in consumption of fruit, vegetables, snacks (pastry, savoury snacks, and sweets) and drinks. Observations recorded by teachers and parent-reported using FFQ. | I > C for children’s fruit consumption (parental reported), due to an increase in fruit made available at school 0.11 (95 % CI: 0.00, 0.21) p < 0.044) and not due to an increase in fruit brought from home (intervention effect = –0.02 (95 % CI: −0.13, 0.08) p = 0.677). I = C for other food items (snacks, vegetables, and beverages). (↑ +) | High |
| Witt et al., (2012) U.S. [39] | CRCT NR | N = 268 4–5 years Yes | Preschool-based. Six weeks: 2 x 15-30min lessons + 1 imaginary trip per week. Fun, interactive activities, songs/music, colour, appeal to senses, role plays, healthful eating, food tasting | Weighed snack consumption of fruit and vegetables during childcare. 3-day food diary, FFQ. | I > C for all. Post-test: Fruit - d = 1.29, p < 0.001; vegetables - d = 0.90, p < 0.001 follow-up: Fruit - d = 0.68, p < 0.001; vegetables - 1.20, p < 0.001 (↑ +) | Some Concerns |
| Brouwer and Neelon, (2013) U.S. [40] | RCT NR | N = NR. (Average 19 children × 4 centres) 3–5 years. Yes | Child-care centres. Four-month gardening program to yield one crop per month and tasting produce. | Increase in no. of V & F provided to & consumed by children in childcare. Observation (meals and snacks). Recording (all foods/beverages served, consumed, and wasted). Nutritional value and food groupings (USDA MyPlate). | Post-intervention, Vegetable consumption, (mean intake) I (0.25 (1.10)) > C (−0.18 (0.52)). Fruit consumption, (mean intake) I (−0.33 (0.72)) < C (0.15 (0.25)). (↑ +) | High |
| Martínez-Andrade et al., (2014) U.S. [41] | CRCT CCM | N = 306 2–5 years No | Primary care clinics. Six weeks x 2 h. 90 min - nutrition education, 30 min- preparation and consumption of healthy foods, calculating the quantity of sugar/ fat in processed foods, creating shopping lists. | Parent-reported (three- and six-month follow-up). Dietary intake- Child FFQ | I > C for vegetable consumption: 6.3 servings/week, (95% CI, 1.8, 10.8) at 3 months. I = C for behaviour at 3 and 6 months. At 3-month sweet snacks (−3.9 servings/ week; 95% CI, −8.9, 1.1), sugar added to drinks (−2.2 Servings/week; 95% CI, −8.4, 4.1), and effects reduced at 6 months. (↑+ ↓-) | High |
| Dazeley and Houston-Price, (2015) England [42] | CRCT NR | N = 92 1–3 years No | Day-care nurseries. Once/ day x four weeks. Four activity sheets in total, each with three games specific to senses: sight, smell, touch or sound and activities such as drawing, colouring, storybooks nursery rhyme and taste testing. | Researchers recorded foods touched and tasted by children (video camera) and online coding. | I > C, children touched and tasted more of the vegetables to which they had been familiarised in their playtime activities than of a matched set of non-exposed foods t (53) = 2.05, p = 0.046). (↑ +) | Low |
| Jisoo et al., (2018) U.S. [43] | CRCT BET | N = 42 4–5 years Yes | Preschool & home. Family backpack (hands-on activities/supplies) distributed over 12 weeks. Children’s picture book, hands-on activities (1) “Mystery Bag,” math activity on F&V by touch; (2) “My Favourites’,” art activity on F&V by drawing (3) “Graphing F&V” | Parent-reported children’s fruit and vegetable consumption FFQ | I > C for children’s fruit and vegetable consumption. [t (21) = 2.49, p < 0.05 for fruits; t (21) = 3.92, p < 0.01 for vegetables]. (↑ +) | High |
| Studies conducted in the primary school and community setting (6 to 12 years old children) | ||||||
| Perry et al., (1998) U.S [44] | CRCT SLT | N = 441 Grades 4–5 No | Primary schools. Two curricula: “High 5” and “5 for 5,” Each included, 16 × 40–45-min classroom sessions, 2 × a week for eight weeks. Skill-building, problem-solving activities, snack preparation & taste testing. Curricula introduced; role models (comic books in High 5), adventure stories (5 for 5), competitions (eating fruits & vegetables). | Lunchroom observations and 24-h food recall measured food consumption. Parent telephone surveys and a health behaviour questionnaire (psychosocial factors). | Lunch observations: I > C for vegetable consumption in girls (Δ = 0, 26 servings, p < 0.05) than boys (Δ = 0, 04). 24-Hr recalls. I > C for servings of fruits & vegetables per 1000 kcal, and servings of fruit per 1000 kcal. Health Behaviour: Teacher perceived- I > C for eating, need to eat, reports of asking for, daily servings of fruits and vegetables. (↑ +) | High |
| Bere et al., (2005) Norway [45] | CRCT NR | N = 517 12–13 years Grade 6 Yes | School-based. Two school years; baseline to follow-up 1 = 8 months and follow-up 2= 20 months. Preparing fruit and vegetables (snacks), taste testing. | Self-reported fruit and vegetable intake (24-h fruit and vegetable recall). | I > C for fruit and vegetable intake at follow-up 1 and follow-up 2 (effect sizes = 0.6 and 0.5), p = 0.07) at school and all day. (↑ +) | High |
| Bere et al., (2006) Norway [46] | CRCT SCT | N = 369, 12–13 years Grade 6. No | School-based. One school year. Preparing fruit and vegetables (snacks), taste testing, information session, monitoring own fruit and vegetable intake for three days, self-assessment and goal setting for future intake. | Self-reported fruit and vegetable intake (24-h fruit and vegetable recall). | I = C for intake of fruit and vegetables eaten at school or all day, neither at follow-up 1 (22% versus 15% subscribers) nor follow-up 2 (15% versus 26% subscribers), p = (0.51, 0.76 0.41). (↑ +) | High |
| Chen et al., (2009) U.S [47] | RCT SCT | N = 67 8–10 years. Yes | Family-based. Once/ week for eight weeks, interactive fun activities (games & play), role-playing selecting healthy meals, food choices-high sugar, high-fat foods, interactive food preparation. Family component (two 2-h sessions) | Self-reported. Dietary intake of children (3-day food diary) and food choices (Health Behaviour Questionnaire) | I > C for the decrease in fat intake and increase vegetable and fruit intake. (p < 0.05) (↑ +) (↓−) | High |
| Fulkerson et al., (2010) U.S. [48] | RCT SCT | N = 44 8–10 years. Yes | Elementary School. Five × 90-min sessions, six months - interactive nutrition education, taste testing, cooking skill building, parent discussion groups, and hands-on meal preparation. | Child food preparation skill (Questionnaire). Home food availability/meal offering (Inventories). Dietary assessment (24-h diet recalls). | I > C for food preparation skill development (p < 0.001), consumption of fruits and vegetables (p < 0.08), and intakes of key nutrients (all p values < 0.05). (↑+) | High |
| Rosenkranz et al., (2010) U.S [49] | CRCT | N = 76, 9–12 years. No | Girl Scouts and home. Educational curriculum, FV snack preparation, role-playing, tasting of FV snacks, promotion of FV consumption and prohibition of SSB, candy over 4 months. | Troop leader health promotion behaviours and environmental opportunities for healthful eating in the troop meetings. | I > C for all. Opportunities for healthful eating (d= 210.8, p < 0.001), promotion of healthful eating (d = 18.14, p < 0.001). 1< C for discouraged healthful eating (p = 0.002) (↑+ ↓−) | Some Concerns |
| Keihner et al., (2011) U.S [50] | RCT SCT | N = 1154 8–12years Grades 4–5. No | Elementary schools. 10 × 50 min classroom-based nutrition education lessons (grade-specific) with activities including Fruit and Vegetable rap songs, serving size poster, and stickers over the eight weeks. | Pre/post surveys measured knowledge, outcome expectations, and self-efficacy (SE) using a questionnaire. | I > C for Fruit and Vegetable knowledge (4 items, p < 0.05 to p < 0.001); positive outcome expectations (fifth grade only, p <0.001); asking/shopping and eating Self Efficacy (p = 0.04 and p < 0.001). (↑ +) | Some Concerns |
| Katz et al., (2011) U.S [51] | CRCT SEM | N = 1180 7–9 years. Grades 2–4. Yes | Elementary School. Four × 20-min sessions over two school years. (Minilessons) on food choice and health, interactive activity/ hands-on ‘‘spying on food labels’’ game, emphasising healthy choice and summarising key points. | Nutrition Knowledge (food label literacy/ food choices) – a standardised test instrument. Dietary Pattern- Youth and Adolescent Questionnaire and (FFQ). | I > C for nutrition knowledge (p < 0.01). Grade 3 students showed the most improvement, 23% (p < 0.01). I = C for improvements in dietary patterns, in terms of total caloric, sodium, and total sugar intake (p > 0.05). (↑+ ↓−) | High |
| Wall et al., (2012) U.S [52] | CRCT NR | N = 1937 9 years Grade 4. No | Elementary school. Four lessons × 3–5 weeks of learner-centred activities; vegetable tastings, worksheets, handouts. | Food preference, attitude, and self-efficacy survey items (from SNAP-Ed intervention) | I > C for vegetable-related preference, attitude, self-efficacy, and knowledge (p < 0.001). (Intervention 1.56 ± 5.80); (control 0.08 ± 4.82). (↑ +) | Some Concerns |
| Brown et al., (2013) U.S [53] | CRCT SCT | N = 1619 11–14 years. Grades 4–8. No | School-based. Four lessons on calcium and osteoporosis. Prevention and taste-testing food items within two weeks over one academic year. | Interest in lessons, enjoyment of food tasting, eating attitude, tasting experience, new knowledge (21-item survey) | For all foods tasted, students who did not enjoy the food tasting were less interested in the lesson than students who did enjoy the food tasting (all p < 0.001). (↓−) | High |
| Habib-Mourad et al., (2014) Lebanon [54] | RCT SCT | N = 387 9–11 years. Grades 4–5. No | Primary school. 45 min classroom sessions per week for 12 weeks (10–15 min discussion on nutrition, 30 min - interactive activities (games, hands-on activities- posters, pamphlets, activity booklets, card & board games), food preparation. | Dietary habits, nutrition knowledge and self-efficacy (Questionnaire) | I > C for purchasing and consuming less chips and sugar sweetened beverage (SSB) (86% & 88%, p < 0.001) and knowledge and self-efficacy (+ 2.8 & +1.7, p < 0.001). (↓−) | High |
| Wells et al., (2015) U.S. [55] | RCT NR | N = 3061, 6–12 years, Grades 2, 4, & 5. No | Elementary school. 40 lessons x 60 min (20 for grade two to three, 20 for grade four to six/ week for two years (classroom & garden) Garden activities- planting, harvesting, and tasting as snacks. | Effect school gardens on children’s science knowledge (Nutritional Science Questionnaire) | I > C for science knowledge from wave 1 to waves 2, 3, 4 (p < 0.0001), and for dose response (p < 0.0001). (↑+) | High |
| Allirot et al., (2016) Spain [56] | RCT NR | N = 137 7–11 years. No | Primary school. Single session × 2 h. 1hr cooking workshop- preparing three food items/ chance to see, smell and touch taste ingredients. 1hr creative workshop- collage session (food images-fruits/ vegetables) creating portrait (cutting & gluing food images, making stories with (created characters), drawings (whiteboard), playing games (guessing & drawing). Food selection (familiar/unfamiliar), tasting. | Willingness to choose and taste unfamiliar foods/food intake estimation (Photographs). Liking of the food items (electronic 5-point facial scale) Subjective hunger and satiety (Bennet and Blisset’s “Teddy the Bear” hunger and satiety scale). | I > C for mean number of unfamiliar foods chosen per child (p = 0.037), for willingness to taste the unfamiliar foods (p = 0.011), liking for the whole afternoon snack (p = 0.034), for 2 of 3 unfamiliar foods and for 1 of 3 familiar foods (p < 0.05). I = C for overall food intake and hunger/satiety scores. (↑+ ↓−) | Some Concerns |
| LaChausse, (2017) U.S. [57] | CRCT NR | N = 275 Grades 4–6. No | Primary schools. Onex 30–40min session per month × four months.14 HOTM activities included fruit and vegetable tastings, student workbooks, storybooks related to a monthly fruit or vegetable, farm-to-school presentations, and cafeteria posters. | Self-reported. Eating behaviours (Youth Network Survey). Fruit (F) and vegetable (V) preferences (F/V Preferences Scale). Knowledge on F &V- (5 items from General Knowledge Survey). Self-Efficacy to i) Ask for F and V ii) to Prepare F and V iii) to Eat fruits and vegetables. | I = C for both: fruit consumption (b = 0.14, t = 0.89, p = 0.38), vegetable consumption (b = –0.17, t = –0.73, p = 0.47). I > C for fruit & vegetable preferences, (b = 3.41, t = 2.19, p = 0.04) I = C for knowledge of fruits and vegetables, (b = 0.13, t = 0.77, p = 0.45). Self-efficacy, I = C for all (to ask for, prepare and eat fruits and vegetables. (↑ +) | Some Concerns |
| Schreinemachers et al., (2017) Nepal [58] | CRCT NR | N = 1275 10–15 years. No | School-based. Two school years. Gardening lessons and hands-on practice (cultivation of nutrient-dense vegetables), lessons on gardening and promotional activities to reinforce lessons and strengthen impact by poster displays. | Awareness of fruit (F) & vegetables (V), knowledge about food & nutrition & sustainable agriculture, preferences & liking for F&V (structured questionnaire with (colour photos and multiple choice). F& V consumption (24-hr recall) | I > C for children’s awareness about F and V, knowledge on sustainable agriculture, food, nutrition and health and their stated preferences for eating fruit and vegetables (p < 0.01). I = C for improvements in F and V consumption or nutritional status. (↑ +) | High |
| Schreinemachers et al., (2017) Bhutan [59] | CRCT NR | N = 468 9–15 years Yes | School-based. One school year of gardening projects to cultivate nutrient-dense vegetables and weekly lessons on gardening/ nutrition. Promotional activities to reinforce the lessons (poster displays, poem displays on school boards, songs, nutrition charts, vegetable charts, pledges) | Awareness of fruit (F) & vegetables (V), knowledge about food & nutrition & sustainable agriculture, preferences/ liking for F and V (structured questionnaire with (colour photos and multiple choice). F and V consumption (24-h recall) | I > C, for children’s awareness of fruit & vegetables by 18.0 % (p < 0.01), their knowledge of sustainable agriculture by 15.2 % (p < 0.05), preferences for consuming fruit & vegetables by 9.5 % (p < 0.05), children’s probability of consuming vegetables the previous day, 11.7 % (p < 0.05) but I = C for number of different fruits or vegetables consumed. (↑ +) | High |
| Keihner et al., (2017) U.S. [60] | CRCT NR | N = 3463 8–12 years Grades 4–5. No | Elementary schools. 10 weeks of activities during/after school-weekly fruits &vegetable lessons, biweekly classroom promotions/taste tests; posters displayed in/around schools; weekly nutrition materials for parents. | Child reported fruit and vegetable (FV) intake using a 24-h food diary. | I < C for daily Fruit and Vegetable intake, (Mean difference in change between groups, 0.26 cups, p < 0.001) (↑ +) | Some Concerns |
| Scherr et al., (2017) U.S. [61] | CRCT SCT | N = 409 9–10 years Grade 4 Yes | Elementary school. Nutrition education, cooking demonstrations, school gardens, family newsletters, health fairs, salad bars, tasting over one school year. | Increase in nutrition knowledge (Nutrition Knowledge Questionnaire). Fruit and vegetable intake (FFQ). | I > C nutrition knowledge (mean d = 2.2; p < 0.001), total vegetable identification (mean d = 1.18; p < 0.001), vegetable preferences or reported fruit & vegetable intake, self-reported general or diet-related parenting practices. (↑+ ↓−) | High |
| Allirot et al., (2018) Spain [62] | CRCT NR | N = 86 8–10 years No | Primary school. Single session × 2 h. 1-h workshop- simulated purchasing of ingredients for the preparation of three unfamiliar foods and classifying them as per recipe: 1-h creative workshop—drawing a dish using vegetable or fruit, oral presentation, personal nutritional pyramid and playing guessing game: consumption of afternoon snack—from six food items. | Willingness to choose and taste unfamiliar foods/Food intake estimation (Photographs). Liking of food items (validated illustrative five-point facial scale). Subjective hunger and satiety (Bennet and Blisset’s “Teddy the Bear” hunger and satiety scale). | I > C for mean number of unfamiliar foods chosen per child (0.70 ± 0.14), (0.19 ± 0.07) (p = 0.003) and liking for 1 of 3 unfamiliar foods (p < 0.05). I = C for food intake estimation and levels of subjective appetite. (↑+ ↓−) | Some Concerns |
| Preschool-Aged Children | ||
| Study | Experiential Learning Activities | Mean Effect Size (Cohen’s d) |
| Outcome: Behaviour | ||
| Dazeley et al. (2015) [42] | Taste-testing, sensory evaluation, games, storybooks, creative/art activities | Healthy foods 0.13 |
| Jisoo et al. (2018) [43] | Games, storybooks, sensory evaluation creative/art activities | Healthy foods 0.12 |
| Vereecken et al. (2009) [38] | Taste-testing, role modelling | Healthy foods 0.01 |
| Unhealthy foods 0.03 | ||
| Martinez et al. (2014) [41] | Taste-testing, food preparation/cooking, calculations, creating shopping lists | Healthy foods −0.12 |
| Unhealthy foods −0.004 | ||
| Brouwer et al. (2013) [40] | Gardening, taste-testing | Healthy foods −0.04 |
| Outcome: Attitudes | ||
| Dazeley et al. (2015) [42] | Taste-testing, sensory evaluation, games, storybooks, creative/art activities | Healthy foods 0.23 |
| Outcome: Knowledge | ||
| Witt et al. (2012) [39] | Taste-testing, roleplays, games, songs | Insufficient reported data |
| Primary school-aged children | ||
| Study | Experiential learning activities | Mean effect size (Cohen’s d) |
| Outcome: Behaviour | ||
| Chen et al. (2010) [47] | Food preparation, role-playing, games | Healthy foods 1.31 |
| Unhealthy foods −0.05 | ||
| Scherr et al. (2017) [61] | Gardening, taste-testing | Healthy foods 0.9 |
| Unhealthy foods −0.66 | ||
| Allirot et al. (2016) [56] | Food preparation/cooking, taste-testing, games, sensory evaluation, creative art activities | Healthy foods 0.5 |
| Unhealthy foods 0.2 | ||
| Allirot et al. (2018) [62] | Food purchasing, food preparation/cooking, games, taste-testing, creative/art activities | Healthy foods −0.12 |
| Unhealthy foods 0.4 | ||
| Schreinemachers et al. (2017) [58] | Gardening | Healthy foods 0.3 |
| Brown et al. (2013) [53] | Taste-testing | Unhealthy foods 0.13 |
| Habib-Mourad et al. (2014) [54] | Food preparation/cooking, games | Healthy foods 0.12 |
| Unhealthy foods −0.13 | ||
| Schreinemachers et al. (2017) [59] | Gardening, songs, creative/art activities | Healthy foods 0.09 |
| LaChausse, (2017) [57] | Taste-testing, storybooks | Healthy foods 0.06 |
| Katz et al. (2011) [51] | Games | Healthy foods 0.06 |
| Unhealthy foods 0.07 | ||
| Fulkerson et al. (2010) [48] | Taste-testing, food preparation/cooking. | Healthy foods 0 |
| Rosenkranz et al. (2010) [49] | Taste-testing, food preparation/cooking, role-playing | Unhealthy foods 0.04 |
| Perry et al. (1998) [44] | Taste-testing, food preparation/cooking, taste-testing, storybook | Insufficient reported data |
| Bere et al. (2005) [45] | Food preparation, taste-testing | Insufficient reported data |
| Bere et al. (2006) [46] | Food preparation/cooking, taste-testing | Insufficient reported data |
| Keihner et al. (2017) [60] | Taste-testing | Insufficient reported data |
| Keihner et al. (2011) [50] | Songs | Insufficient reported data |
| Outcome: Attitudes | ||
| Schreinemachers et al. (2017) [58] | Gardening | Healthy foods 1.12 |
| Habib-Mourad et al. (2014) [54] | Food preparation/cooking, games | Healthy foods 0.8 |
| Rosenkranz et al. (2010) [49] | Food preparation/cooking, role-playing, taste-testing. | Healthy foods 0.7 |
| Chen et al. (2010) [47] | Food preparation/cooking, role-playing, games | Healthy foods 0.5 |
| Allirot et al. (2016) [56] | Food preparation/cooking, taste-testing, sensory evaluation, games, creative art activities | Healthy foods 0.3 |
| Unhealthy foods 0.3 | ||
| Wall et al. (2012) [52] | Taste-testing | Healthy foods 0.3 |
| Allirot et al. (2018) [62] | Food purchasing, food preparation/ cooking, taste-testing, games creative/art activities | Healthy foods 0.09 |
| Unhealthy foods 0.14 | ||
| LaChausse (2017) [57] | Taste-testing, storybooks | Healthy foods 0.04 |
| Outcome: Knowledge | ||
| Schreinemachers et al. (2017) [58] | Gardening | Healthy foods 1.43 |
| Habib-Mourad et al. (2014) [54] | Food preparation/cooking, games | Healthy foods 1.03 |
| Wall et al. (2012) [52] | Taste-testing | Healthy foods 1.03 |
| Brown et al. (2013) [53] | Taste-testing | Healthy foods 0.9 |
| Fulkerson et al. (2010) [48] | Food preparation/cooking, taste-testing. | Healthy foods 0.2 |
| Chen et al. (2010) [47] | Food preparation/cooking, role-playing, games | Healthy foods 0.2 |
| LaChausse (2017) [57] | Taste-testing, storybooks | Healthy foods 0 |
| Katz et al. (2011) [51] | Games | Healthy foods −0.14 |
| Wells et al. (2015) [55] | Gardening, taste-testing | Insufficient reported data |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Varman, S.D.; Cliff, D.P.; Jones, R.A.; Hammersley, M.L.; Zhang, Z.; Charlton, K.; Kelly, B. Experiential Learning Interventions and Healthy Eating Outcomes in Children: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2021, 18, 10824. https://doi.org/10.3390/ijerph182010824
Varman SD, Cliff DP, Jones RA, Hammersley ML, Zhang Z, Charlton K, Kelly B. Experiential Learning Interventions and Healthy Eating Outcomes in Children: A Systematic Literature Review. International Journal of Environmental Research and Public Health. 2021; 18(20):10824. https://doi.org/10.3390/ijerph182010824
Chicago/Turabian StyleVarman, Sumantla D., Dylan P. Cliff, Rachel A. Jones, Megan L. Hammersley, Zhiguang Zhang, Karen Charlton, and Bridget Kelly. 2021. "Experiential Learning Interventions and Healthy Eating Outcomes in Children: A Systematic Literature Review" International Journal of Environmental Research and Public Health 18, no. 20: 10824. https://doi.org/10.3390/ijerph182010824
APA StyleVarman, S. D., Cliff, D. P., Jones, R. A., Hammersley, M. L., Zhang, Z., Charlton, K., & Kelly, B. (2021). Experiential Learning Interventions and Healthy Eating Outcomes in Children: A Systematic Literature Review. International Journal of Environmental Research and Public Health, 18(20), 10824. https://doi.org/10.3390/ijerph182010824