
Diversity Competency and Access to Healthcare in Hospitals in Croatia, Germany, Poland, and Slovenia

 , , ,
, , ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
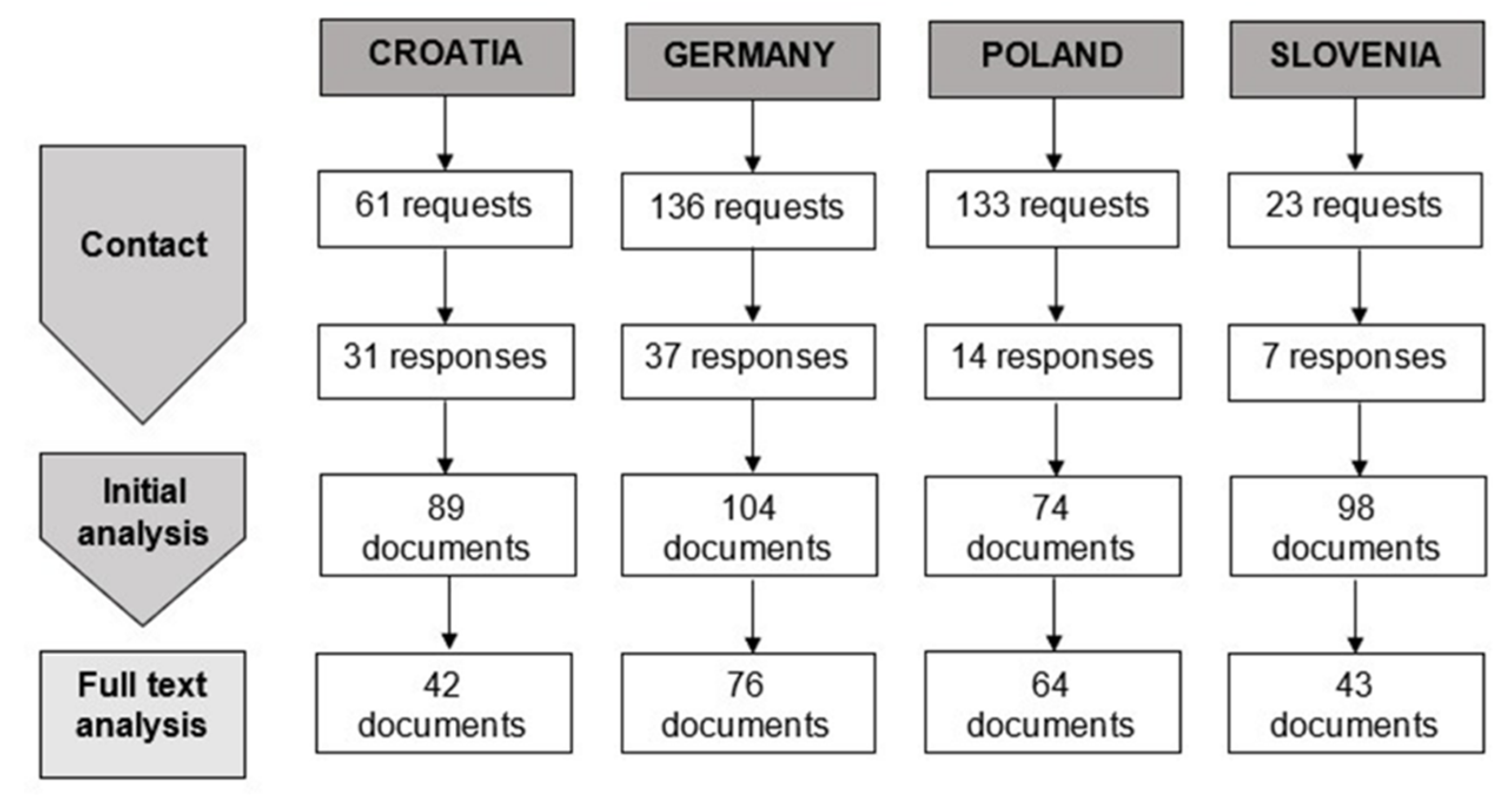
2.1. Procedure
2.2. Materials
2.3. Analysis
3. Results
3.1. General Anti-Discrimination Statements
3.2. Ethnicity, Race, and Culture
3.3. Religion and Belief
3.4. Gender, Gender Identity, and Sexual Orientation
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Satinsky, E.; Fuhr, D.C.; Woodward, A.; Sondorp, E.; Roberts, B. Mental Health Care Utilisation and Access among Refugees and Asylum Seekers in Europe: A Systematic Review. Health Policy 2019, 123, 851–863. [Google Scholar] [CrossRef]
- Rivenbark, J.G.; Ichou, M. Discrimination in Healthcare as a Barrier to Care: Experiences of Socially Disadvantaged Populations in France from a Nationally Representative Survey. BMC Public Health 2020, 20, 31. [Google Scholar] [CrossRef] [Green Version]
- Heise, L.; Greene, M.E.; Opper, N.; Stavropoulou, M.; Harper, C.; Nascimento, M.; Zewdie, D.; Darmstadt, G.L.; Greene, M.E.; Hawkes, S.; et al. Gender Inequality and Restrictive Gender Norms: Framing the Challenges to Health. Lancet 2019, 393, 2440–2454. [Google Scholar] [CrossRef]
- Orzechowski, M.; Nowak, M.; Bielińska, K.; Chowaniec, A.; Doričić, R.; Ramšak, M.; Łuków, P.; Muzur, A.; Zupanič-Slavec, Z.; Steger, F. Social Diversity and Access to Healthcare in Europe: How Does European Union’s Legislation Prevent from Discrimination in Healthcare? BMC Public Health 2020, 20, 1399. [Google Scholar] [CrossRef] [PubMed]
- Alizadeh, S.; Chavan, M. Cultural Competence Dimensions and Outcomes: A Systematic Review of the Literature. Health Soc. Care Community 2016, 24, e117–e130. [Google Scholar] [CrossRef] [Green Version]
- Nair, L.; Adetayo, O.A. Cultural Competence and Ethnic Diversity in Healthcare. Plast. Reconstr. Surg.-Glob. Open 2019, 7, e2219. [Google Scholar] [CrossRef]
- Brach, C.; Fraserirector, I. Can Cultural Competency Reduce Racial and Ethnic Health Disparities? A Review and Conceptual Model. Med. Care Res. Rev. 2000, 57, 181–217. [Google Scholar] [CrossRef]
- National Quality Forum. A Comprehensive Framework and Preferred Practices for Measuring and Reporting Cultural Competency 2009. Available online: https://www.qualityforum.org/Publications/2009/04/A_Comprehensive_Framework_and_Preferred_Practices_for_Measuring_and_Reporting_Cultural_Competency.aspx (accessed on 20 March 2021).
- Butler, M.; McCreedy, E.; Schwer, N.; Burgess, D.; Call, K.; Przedworski, J.; Rosser, S.; Larson, S.; Allen, M.; Fu, S.; et al. Improving Cultural Competence to Reduce Health Disparities; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2016; p. 170. [Google Scholar]
- Foronda, C.L. A Concept Analysis of Cultural Sensitivity. J. Transcult. Nurs. 2008, 19, 207–212. [Google Scholar] [CrossRef]
- Carpenter-Song, E.A.; Schwallie, M.N.; Longhofer, J. Cultural Competence Reexamined: Critique and Directions for the Future. Psychiatr. Serv. 2007, 58, 1362–1365. [Google Scholar] [CrossRef]
- Tayab, A.; Narushima, M. “Here for the Residents”: A Case Study of Cultural Competence of Personal Support Workers in a Long-Term Care Home. J. Transcult. Nurs. 2015, 26, 146–156. [Google Scholar] [CrossRef]
- Tucker, C.M.; Arthur, T.M.; Roncoroni, J.; Wall, W.; Sanchez, J. Patient-Centered, Culturally Sensitive Health Care. Am. J. Lifestyle Med. 2015, 9, 63–77. [Google Scholar] [CrossRef]
- May, S.; Potia, T.A. An Evaluation of Cultural Competency Training on Perceived Patient Adherence. Eur. J. Physiother. 2013, 15, 2–10. [Google Scholar] [CrossRef]
- Majumdar, B.; Browne, G.; Roberts, J.; Carpio, B. Effects of Cultural Sensitivity Training on Health Care Provider Attitudes and Patient Outcomes. J. Nurs. Scholarsh. 2004, 36, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Henderson, S.; Horne, M.; Hills, R.; Kendall, E. Cultural Competence in Healthcare in the Community: A Concept Analysis. Health Soc. Care Community 2018, 26, 590–603. [Google Scholar] [CrossRef]
- Weech-Maldonado, R.; Dreachslin, J.L.; Epané, J.P.; Gail, J.; Gupta, S.; Wainio, J.A. Hospital Cultural Competency as a Systematic Organizational Intervention: Key Findings from the National Center for Healthcare Leadership Diversity Demonstration Project. Health Care Manag. Rev. 2018, 43, 30–41. [Google Scholar] [CrossRef] [PubMed]
- Weech-Maldonado, R.; Elliott, M.; Pradhan, R.; Schiller, C.; Hall, A.; Hays, R.D. Can Hospital Cultural Competency Reduce Disparities in Patient Experiences with Care? Med. Care 2012, 50, S48–S55. [Google Scholar] [CrossRef] [Green Version]
- Anderson, L.M.; Scrimshaw, S.C.; Fullilove, M.T.; Fielding, J.E.; Normand, J. Culturally Competent Healthcare Systems: A Systematic Review. Am. J. Prev. Med. 2003, 24, 68–79. [Google Scholar] [CrossRef]
- Paez, K.A.; Allen, J.K.; Carson, K.A.; Cooper, L.A. Provider and Clinic Cultural Competence in a Primary Care Setting. Soc. Sci. Med. 2008, 66, 1204–1216. [Google Scholar] [CrossRef] [Green Version]
- Frusti, D.K.; Niesen, K.M.; Campion, J.K. Creating a Culturally Competent Organization: Use of the Diversity Competency Model. JONA J. Nurs. Adm. 2003, 33, 31–38. [Google Scholar] [CrossRef]
- Balcazar, F.E.; Suarez-Balcazar, Y.; Taylor-Ritzler, T. Cultural Competence: Development of a Conceptual Framework. Disabil. Rehabil. 2009, 31, 1153–1160. [Google Scholar] [CrossRef] [PubMed]
- Pinder, R.J.; Ferguson, J.; Møller, H. Minority Ethnicity Patient Satisfaction and Experience: Results of the National Cancer Patient Experience Survey in England. BMJ Open 2016, 6, e011938. [Google Scholar] [CrossRef] [Green Version]
- Hölzel, L.P.; Ries, Z.; Kriston, L.; Dirmaier, J.; Zill, J.M.; Rummel-Kluge, C.; Niebling, W.; Bermejo, I.; Härter, M. Effects of Culture-Sensitive Adaptation of Patient Information Material on Usefulness in Migrants: A Multicentre, Blinded Randomised Controlled Trial. BMJ Open 2016, 6, e012008. [Google Scholar] [CrossRef]
- Scott, J.; Marshall, G. A Dictionary of Sociology, 3rd ed.; Scott, J., Marshall, G., Eds.; Oxford University Press: Oxford, UK; New York, NY, USA, 2009; p. 183. [Google Scholar]
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content Analysis and Thematic Analysis: Implications for Conducting a Qualitative Descriptive Study: Qualitative Descriptive Study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Nybell, L.M.; Gray, S.S. Race, Place, Space: Meanings of Cultural Competence in Three Child Welfare Agencies. Soc. Work. 2004, 49, 17–26. [Google Scholar] [CrossRef] [PubMed]
- McCalman, J.; Jongen, C.; Bainbridge, R. Organisational Systems’ Approaches to Improving Cultural Competence in Healthcare: A Systematic Scoping Review of the Literature. Int. J. Equity Health 2017, 16, 78. [Google Scholar] [CrossRef]
- Noe, T.D.; Kaufman, C.E.; Kaufmann, L.J.; Brooks, E.; Shore, J.H. Providing Culturally Competent Services for American Indian and Alaska Native Veterans to Reduce Health Care Disparities. Am. J. Public Health 2014, 104, S548–S554. [Google Scholar] [CrossRef] [Green Version]
- Freeman, T.; Edwards, T.; Baum, F.; Lawless, A.; Jolley, G.; Javanparast, S.; Francis, T. Cultural Respect Strategies in Australian Aboriginal Primary Health Care Services: Beyond Education and Training of Practitioners. Aust. N. Z. J. Public Health 2014, 38, 355–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiaffino, M.K.; Ruiz, M.; Yakuta, M.; Contreras, A.; Akhavan, S.; Prince, B.; Weech-Maldonado, R. Culturally and Linguistically Appropriate Hospital Services Reduce Medicare Length of Stay. Ethn. Dis. 2020, 30, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Clarke, S.K.; Jaffe, J.; Mutch, R. Overcoming Communication Barriers in Refugee Health Care. Pediatric Clin. N. Am. 2019, 66, 669–686. [Google Scholar] [CrossRef]
- Chiarenza, A.; Dauvrin, M.; Chiesa, V.; Baatout, S.; Verrept, H. Supporting Access to Healthcare for Refugees and Migrants in European Countries under Particular Migratory Pressure. BMC Health Serv. Res. 2019, 19, 513. [Google Scholar] [CrossRef] [Green Version]
- Fang, M.L.; Sixsmith, J.; Lawthom, R.; Mountian, I.; Shahrin, A. Experiencing ‘Pathologized Presence and Normalized Absence’; Understanding Health Related Experiences and Access to Health Care among Iraqi and Somali Asylum Seekers, Refugees and Persons without Legal Status. BMC Public Health 2015, 15, 923. [Google Scholar] [CrossRef]
- Jongen, C.; McCalman, J.; Bainbridge, R. Health Workforce Cultural Competency Interventions: A Systematic Scoping Review. BMC Health Serv. Res. 2018, 18, 232. [Google Scholar] [CrossRef]
- Thackrah, R.D.; Thompson, S.C. Confronting Uncomfortable Truths: Receptivity and Resistance to Aboriginal Content in Midwifery Education. Contemp. Nurse 2013, 46, 113–122. [Google Scholar] [CrossRef]
- Macapagal, K.; Bhatia, R.; Greene, G.J. Differences in Healthcare Access, Use, and Experiences Within a Community Sample of Racially Diverse Lesbian, Gay, Bisexual, Transgender, and Questioning Emerging Adults. LGBT Health 2016, 3, 434–442. [Google Scholar] [CrossRef] [Green Version]
- Fredriksen-Goldsen, K.I.; Hoy-Ellis, C.P.; Goldsen, J.; Emlet, C.A.; Hooyman, N.R. Creating a Vision for the Future: Key Competencies and Strategies for Culturally Competent Practice with Lesbian, Gay, Bisexual, and Transgender (LGBT) Older Adults in the Health and Human Services. J. Gerontol. Soc. Work. 2014, 57, 80–107. [Google Scholar] [CrossRef]
- Liaw, S.-T.; Hasan, I.; Wade, V.; Canalese, R.; Kelaher, M.; Lau, P.; Harris, M. Improving Cultural Respect to Improve Aboriginal Health in General Practice: A Multi-Methods and Multi-Perspective Pragmatic Study. Aust. Fam. Phys. 2015, 44, 387–392. [Google Scholar] [CrossRef]
- Lieu, T.A.; Finkelstein, J.A.; Lozano, P.; Capra, A.M.; Chi, F.W.; Jensvold, N.; Quesenberry, C.P.; Farber, H.J. Cultural Competence Policies and Other Predictors of Asthma Care Quality for Medicaid-Insured Children. Pediatrics 2004, 114, E102–E110. [Google Scholar] [CrossRef] [Green Version]
- Henderson, S.; Kendall, E.; See, L. The Effectiveness of Culturally Appropriate Interventions to Manage or Prevent Chronic Disease in Culturally and Linguistically Diverse Communities: A Systematic Literature Review. Health Soc. Care Community 2011, 19, 225–249. [Google Scholar] [CrossRef]
- Bischoff, A.; Perneger, T.V.; Bovier, P.A.; Loutan, L.; Stalder, H. Improving Communication between Physicians and Patients Who Speak a Foreign Language. Br. J. Gen. Pract 2003, 53, 541–546. [Google Scholar]
- Schim, S.M.; Doorenbos, A.Z.; Borse, N.N. Enhancing Cultural Competence among Hospice Staff. Am. J. Hosp. Palliat. Care 2006, 23, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Chevannes, M. Issues in Educating Health Professionals to Meet the Diverse Needs of Patients and Other Service Users from Ethnic Minority Groups. J. Adv. Nurs. 2002, 39, 290–298. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, E.A.; Shepard, D.S.; Suaya, J.A.; Stone, E.-L. Overcoming Language Barriers in Health Care: Costs and Benefits of Interpreter Services. Am. J. Public Health 2004, 94, 866–869. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, C.; Motlib, J.; Azad, A.; Ramsay, J.; Eldridge, S.; Feder, G.; Khanam, R.; Munni, R.; Garrett, M.; Turner, A.; et al. Randomised Controlled Trial of a Lay-Led Self-Management Programme for Bangladeshi Patients with Chronic Disease. Br. J. Gen. Pract. 2005, 55, 831–837. [Google Scholar]
- Corkery, E.; Palmer, C.; Foley, M.E.; Schechter, C.B.; Frisher, L.; Roman, S.H. Effect of a Bicultural Community Health Worker on Completion of Diabetes Education in a Hispanic Population. Diabetes Care 1997, 20, 254–257. [Google Scholar] [CrossRef] [PubMed]
- Gary, T.L.; Bone, L.R.; Hill, M.N.; Levine, D.M.; McGuire, M.; Saudek, C.; Brancati, F.L. Randomized Controlled Trial of the Effects of Nurse Case Manager and Community Health Worker Interventions on Risk Factors for Diabetes-Related Complications in Urban African Americans. Prev. Med. 2003, 37, 23–32. [Google Scholar] [CrossRef]


{kind=link}
| Croatia | Germany | Poland | Slovenia | |
|---|---|---|---|---|
| University clinics | 5 | 21 | 20 | 2 |
| General and specialized hospitals | 56 | 115 | 108 | 21 |
| Confessional carrier | 1 | 41 | 5 | - |
| Non-confessional carrier | 60 | 95 | 128 | 23 |
| Anti-Discrimination Statements | ||
|---|---|---|
| Anti-discrimination as a guiding principle | Anti-discrimination provisions for employees | Croatia, Germany, Poland, Slovenia |
| Prohibition of discrimination on grounds of race, ethnic origin, nationality, religion or belief, gender and gender identity, sexual orientation, disability, age, political views, or social status | Germany, Poland | |
| Indirect mention of anti-discrimination | Equal access to healthcare for all social groups Equal right of everyone to quality healthcare | Croatia, Poland Slovenia |
| Equal treatment of all co-workers and patients Key principles | Poland, Slovenia | |
| Ethnicity, Race, and Culture | ||
|---|---|---|
| Language barriers | ‘Interpreter pool’ from among the employees of the institution or interpreting services | Germany, Poland, Slovenia |
| Possibility of involvement of interpreters from other institutions | Poland, Slovenia | |
| Lists of official interpreters | Croatia | |
| Improvement of access for ethnic or cultural minority groups | Support for migrant patients through administrative procedures | Germany |
| Training for employees concerning medico-ethical challenges in interactions with patients | Germany, Slovenia | |
| Integration of foreign workers into the hospital’s staff | Recognition of various backgrounds and experiences of foreign workers. | Germany |
| Religion and Belief | ||||
|---|---|---|---|---|
| Pastoral care | Access to clergy | On the regular basis | Pastoral care for the members of the Roman Catholic Church | Poland, Slovenia |
| On request | Provision of the pastoral care for members of religious communities | Germany, Poland Slovenia | ||
| Space dedicated for religious practices | Religious rites in a hospital chapel for members of the Roman Catholic faith | Croatia, Poland, Slovenia | ||
| Possibility of ritual rites in a hospital chapel/dedicated space for members of other religious communities | Slovenia, Poland | |||
| Religious services provided | Masses in hospital chapels, confession opportunities | Croatia, Germany, Poland, Slovenia | ||
| Respect for customs and practices | Diet | Halal diet | Croatia, Germany | |
| Other | A possibility of religious accompaniment of the dying patient | Germany, Poland | ||
| Meeting religiously motivated need | Jehovah’s Witnesses —blood transfusion | Acting according to professional standards and no obligation to respect refusal of blood transfusion | Croatia | |
| Respect of the patient’s will and explicit informed consent regarding refusal of blood transfusion | Germany | |||
| Male circumcision | Necessity for religious identity and religious socialization of the child for Jews and Muslims | Germany | ||
| Possibility of male circumcision as a self-pay service | Slovenia | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doričić, R.; Orzechowski, M.; Nowak, M.; Tutić Grokša, I.; Bielińska, K.; Chowaniec, A.; Ramšak, M.; Łuków, P.; Muzur, A.; Zupanič-Slavec, Z.; et al. Diversity Competency and Access to Healthcare in Hospitals in Croatia, Germany, Poland, and Slovenia. Int. J. Environ. Res. Public Health 2021, 18, 11847. https://doi.org/10.3390/ijerph182211847
Doričić R, Orzechowski M, Nowak M, Tutić Grokša I, Bielińska K, Chowaniec A, Ramšak M, Łuków P, Muzur A, Zupanič-Slavec Z, et al. Diversity Competency and Access to Healthcare in Hospitals in Croatia, Germany, Poland, and Slovenia. International Journal of Environmental Research and Public Health. 2021; 18(22):11847. https://doi.org/10.3390/ijerph182211847
Chicago/Turabian StyleDoričić, Robert, Marcin Orzechowski, Marianne Nowak, Ivana Tutić Grokša, Katarzyna Bielińska, Anna Chowaniec, Mojca Ramšak, Paweł Łuków, Amir Muzur, Zvonka Zupanič-Slavec, and et al. 2021. "Diversity Competency and Access to Healthcare in Hospitals in Croatia, Germany, Poland, and Slovenia" International Journal of Environmental Research and Public Health 18, no. 22: 11847. https://doi.org/10.3390/ijerph182211847