
Systematic Review of Cost-Effectiveness of Injury Prevention Interventions in Soccer—Evidence Why Health Agencies Should Address It


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction
2.4. Quality Assessment
3. Results
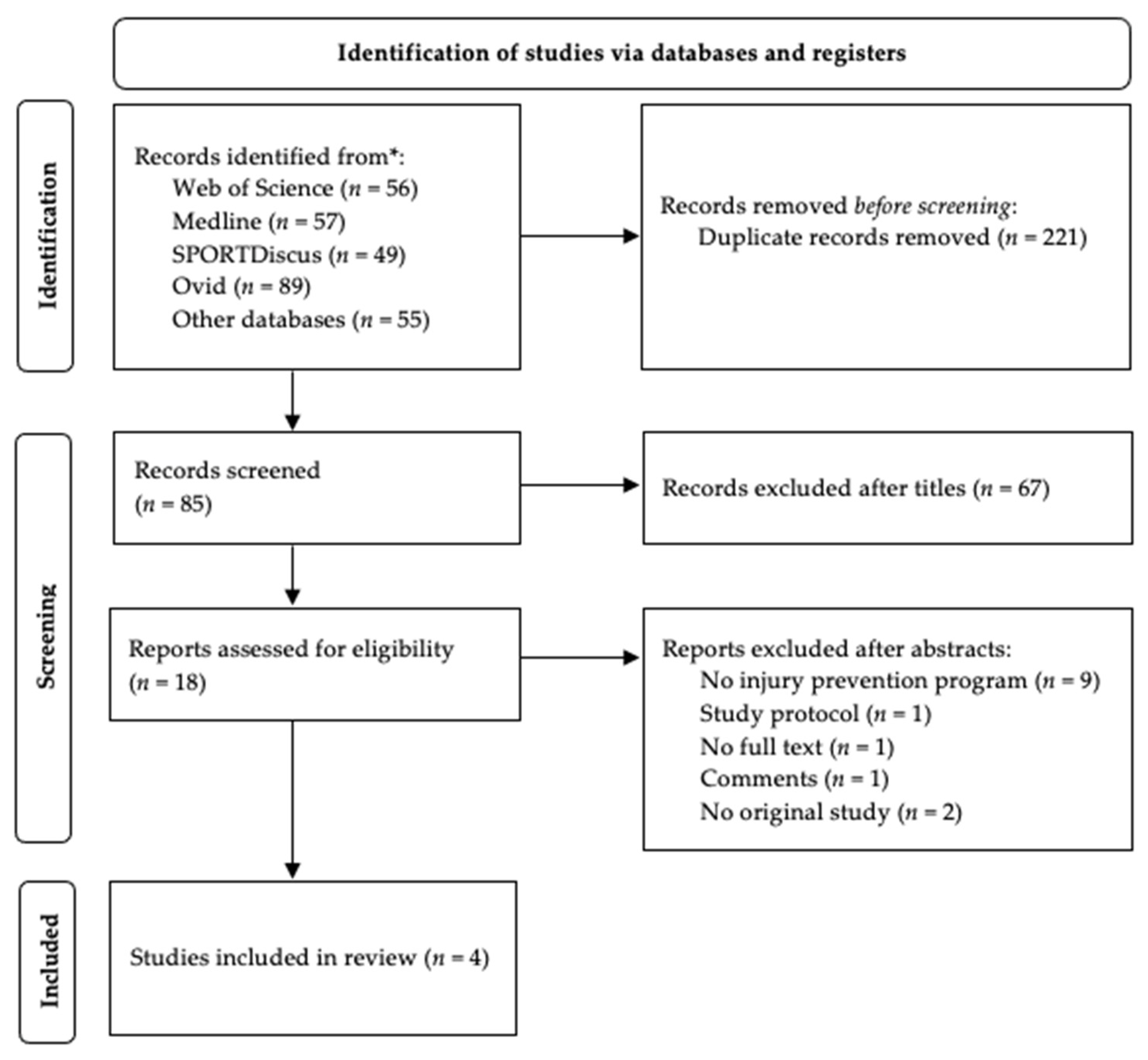
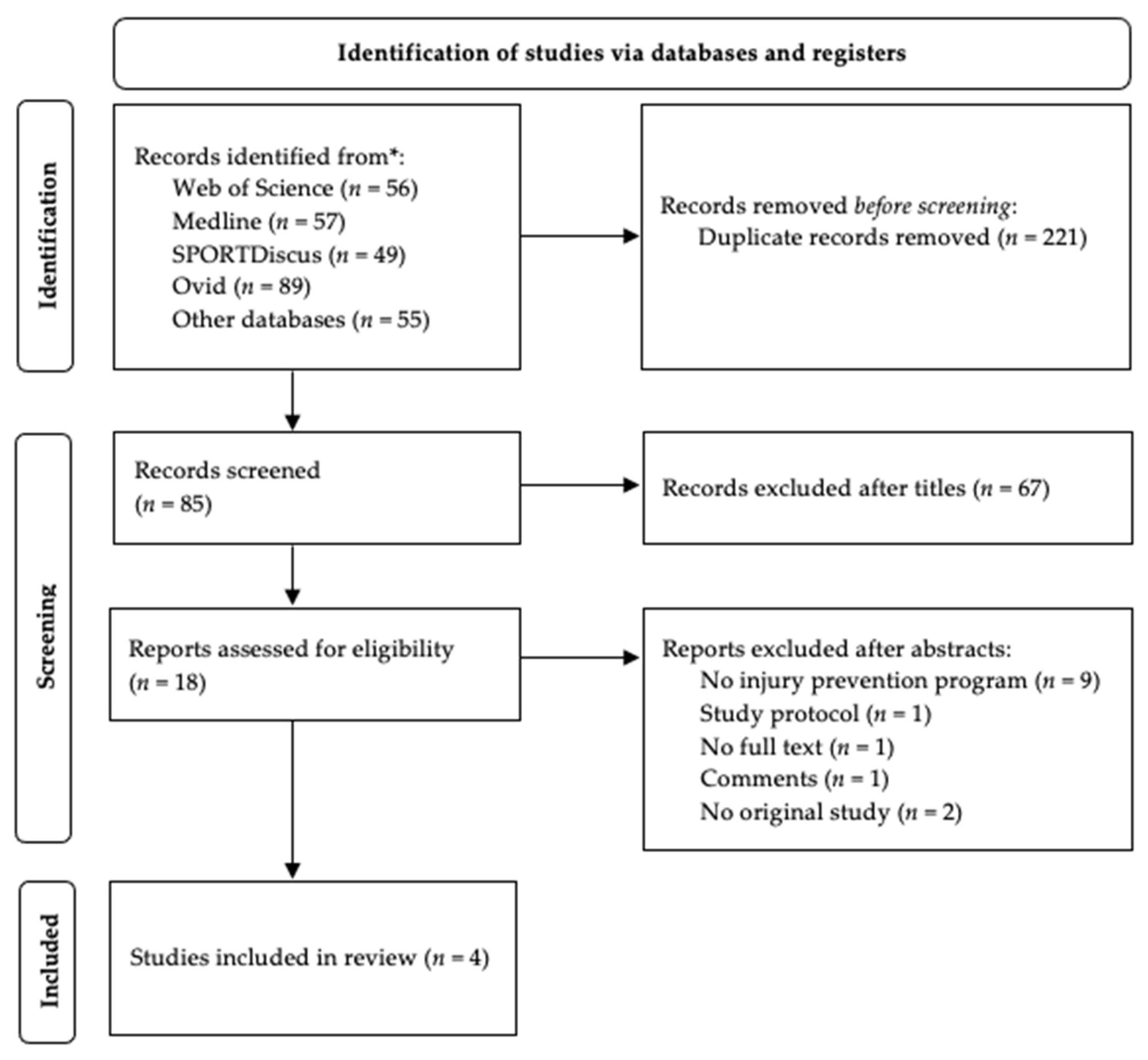
3.1. Literature Search
3.2. Study Description
3.3. Assessing the Quality of Economic Evaluation
3.4. Costs
3.5. Injury Prevention Programs Costs
3.6. Injury Prevention Interventions and Their Incremental Cost-Effectiveness Ratio
3.7. Cost-Effectiveness Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Räisänen, A.M.; Parkkari, J.; Karhola, L.; Rimpelä, A. Adolescent physical activity-related injuries in sports club, school sports and other leisure time physical activities. Cogent Med. 2016, 3, 1260786. [Google Scholar] [CrossRef]
- Verhagen, E.; van Tulder, M.; Van Der Beek, A.; Bouter, L.; Van Mechelen, W. An economic evaluation of a proprioceptive balance board training programme for the prevention of ankle sprains in volleyball. Br. J. Sports Med. 2005, 39, 111–115. [Google Scholar] [CrossRef]
- Krist, M.R.; van Beijsterveldt, A.M.; Backx, F.J.; de Wit, G.A. Preventive exercises reduced injury-related costs among adult male amateur soccer players: A cluster-randomised trial. J. Physiother. 2013, 59, 15–23. [Google Scholar] [CrossRef] [Green Version]
- Rössler, R.; Verhagen, E.; Rommers, N.; Dvorak, J.; Junge, A.; Lichtenstein, E.; Donath, L.; Faude, O. Comparison of the ‘11+ Kids’ injury prevention programme and a regular warmup in children’s football (soccer): A cost effectiveness analysis. Br. J. Sports Med. 2019, 53, 309–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lauersen, J.B.; Andersen, T.E.; Andersen, L.B. Strength training as superior, dose-dependent and safe prevention of acute and overuse sports injuries: A systematic review, qualitative analysis and meta-analysis. Br. J. Sports Med. 2018, 52, 1557–1563. [Google Scholar] [CrossRef] [Green Version]
- Åman, M.; Forssblad, M.; Larsén, K. Incidence and body location of reported acute sport injuries in seven sports using a national insurance database. Scand. J. Med. Sci. Sports 2018, 28, 1147–1158. [Google Scholar] [CrossRef] [PubMed]
- Verhagen, E.A.L.M. Costing an Injury Prevention Program in Amateur Adult Soccer. Clin. J. Sport Med. 2013, 23, 500–501. [Google Scholar] [CrossRef] [PubMed]
- Barengo, N.C.; Meneses-Echávez, J.F.; Ramírez-Vélez, R.; Cohen, D.D.; Tovar, G.; Bautista, J.E.C. The impact of the FIFA 11+ training program on injury prevention in football players: A systematic review. Int. J. Environ. Res. Public Health 2014, 11, 11986–12000. [Google Scholar] [CrossRef] [Green Version]
- Al Attar, W.S.A.; Alshehri, M.A. A meta-analysis of meta-analyses of the effectiveness of FIFA injury prevention programs in soccer. Scand. J. Med. Sci. Sports 2019, 29, 1846–1855. [Google Scholar] [CrossRef]
- Silvers-Granelli, H.J.; Bizzini, M.; Arundale, A.; Mandelbaum, B.R.; Snyder-Mackler, L. Does the FIFA 11+ Injury Prevention Program Reduce the Incidence of ACL Injury in Male Soccer Players? Clin. Orthop. Relat. Res. 2017, 475, 2447–2455. [Google Scholar] [CrossRef]
- Neto, M.G.; Conceição, C.S.; Brasileiro, A.J.A.D.L.; De Sousa, C.S.; Carvalho, V.; De Jesus, F.L.A. Effects of the FIFA 11 training program on injury prevention and performance in football players: A systematic review and meta-analysis. Clin. Rehabil. 2017, 31, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Rössler, R.; Donath, L.; Bizzini, M.; Faude, O. A new injury prevention programme for children’s football—FIFA 11+ Kids—Can improve motor performance: A cluster-randomised controlled trial. J. Sports Sci. 2016, 34, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Windt, J.; Ekstrand, J.; Khan, K.M.; McCall, A.; Zumbo, B.D. Does player unavailability affect football teams’ match physical outputs? A two-season study of the UEFA champions league. J. Sci. Med. Sport. 2018, 21, 525–532. [Google Scholar] [CrossRef]
- Finch, C.F. Getting sports injury prevention on to public health agendas-addressing the shortfalls in current information sources. Br. J. Sports Med. 2012, 46, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Michael, F.; Drummond, M.J.S.; Claxton, K.; Stoddart, G.L.; Torrance, G.W. Methods for The Economic Evaluation of Health Care; Oxford University Press: Oxford, UK, 2015; p. 464. [Google Scholar]
- Davis, J.C.; Robertson, M.C.; Ashe, M.C.; Liu-Ambrose, T.; Khan, K.M.; Marra, C.A. Does a home-based strength and balance programme in people aged > or = 80 years provide the best value for money to prevent falls? A systematic review of economic evaluations of falls prevention interventions. Br. J. Sports Med. 2010, 44, 80–89. [Google Scholar] [CrossRef]
- Winser, S.J.; Chan, H.T.F.; Ho, L.; Chung, L.S.; Ching, L.T.; Felix, T.K.L.; Kannan, P. Dosage for cost-effective exercise-based falls prevention programs for older people: A systematic review of economic evaluations. Ann. Phys. Rehabil. Med. 2020, 63, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Bramer, W.M.; Rethlefsen, M.L.; Kleijnen, J.; Franco, O.H. Optimal database combinations for literature searches in systematic reviews: A prospective exploratory study. Syst. Rev. 2017, 6, 245. [Google Scholar] [CrossRef]
- Nouni-Garcia, R.; Asensio-Garcia, M.R.; Orozco-Beltran, D.; Lopez-Pineda, A.; Gil-Guillén, V.F.; Quesada, J.A.; Casas, R.C.B.; Carratala-Munuera, C. The FIFA 11 programme reduces the costs associated with ankle and hamstring injuries in amateur Spanish football players: A retrospective cohort study. Eur. J. Sport Sci. 2019, 19, 1150–1156. [Google Scholar] [CrossRef] [PubMed]
- Marshall, D.A.; Lopatina, E.; Lacny, S.; Emery, C.A. Economic impact study: Neuromuscular training reduces the burden of injuries and costs compared to standard warm-up in youth soccer. Br. J. Sports Med. 2016, 50, 1388–1393. [Google Scholar] [CrossRef]
- Doran, C.M. Economic evaluation of interventions to treat opiate dependence: A review of the evidence. Pharmacoeconomics 2008, 26, 371–393. [Google Scholar] [CrossRef] [PubMed]
- Edmunds, K.; Ling, R.; Shakeshaft, A.; Doran, C.; Searles, A. Systematic review of economic evaluations of interventions for high risk young people. BMC Health Serv. Res. 2018, 18, 660. [Google Scholar] [CrossRef] [PubMed]
- Polinder, S.; Segui-Gomez, M.; Toet, H.; Belt, E.; Sethi, D.; Racioppi, F.; van Beeck, E.F. Systematic review and quality assessment of economic evaluation studies of injury prevention. Accid. Anal. Prev. 2012, 45, 211–221. [Google Scholar] [CrossRef]
- Bizzini, J.D.M. Football Injury Prevention. In Football Traumatology; Springer: Berlin/Heidelberg, Germany, 2015; pp. 35–46. [Google Scholar]
- Woods, S.E.; Diehl, J.; Zabat, E.; Daggy, M.; Engel, A.; Okragly, R. Is it cost-effective to require recreational ice hockey players to wear face protection? South. Med. J. 2008, 101, 991–995. [Google Scholar] [CrossRef] [PubMed]
- Michaels-Igbokwe, C.; Lee, R.; Marshall, D.A.; Currie, G. Economic evaluations of strategies to prevent sports and recreational injury among children and adolescents: A systematic review. Inj. Prev. J. Int. Soc. Child Adolesc. Inj. Prev. 2019, 25, 340–347. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Database | Research Platform | Search Strategy |
|---|---|---|
| Web of Science * | Web of Science Platform | TS = (“return of investment” OR ROI OR “cost benefit” OR cost * OR “cost effectiv *” OR cost-effectiv *) AND TS = (football OR soccer) AND TS = (injury AND prevention) |
| Medline (EBSCOhost) ** | EBSCOhost Research Platform | AB = (“return of investment” OR ROI OR “cost benefit” OR cost * OR “cost effectiv *” OR cost-effectiv *) AND AB = (football OR soccer) AND AB = (injury AND prevention) |
| SPORTDiscus with full text ** | ||
| Academic Search Ultimate ** | ||
| Health Source: Nursing/Academic Edition ** | ||
| OpenDissertations ** | ||
| Teacher Reference Center ** | ||
| MasterFILE Premier ** | ||
| Business Source Ultimate ** | ||
| Ovid MEDLINE(R) ALL *** | Ovid Research Platform | (“return of investment” OR ROI OR “cost benefit” or cost * OR “cost effectiv *” OR cost-effectiv *).ab,kw,ot,sy,ti AND (football OR soccer).ab,kw,ot,sy,ti AND (injury AND prevention).ab,kw,ot,sy,ti |
| Scheme | Study Design | Participant | Intervention | Comparator | Time Frame | Injury Definition | Outcomes | Perspective, Type of Currency, Time Period Costs were Measured | Sensitivity Analysis | Discounting, Time Horizon |
|---|---|---|---|---|---|---|---|---|---|---|
| Nouni-Garcia et al. 2019 [20] | Retrospective cohort study | Male amateur players aged 18–40 years INT: n = 42 CON: n = 42 | The “FIFA 11” intervention, 2× week | Usual training | Two soccer seasons | All time-loss lateral ankle ligament and hamstring injuries that had occurred during training sessions and competitions | mean total cost per player for the two seasons | Not provided, EUR, 2008–2021 | No | Not applicable |
| Krist et al. 2013 [3] | Cluster RCT | Male amateur players aged 18–40 years INT: n = 223 CON: n = 233 | “The11” injury prevention program during the warm-up (10 exercises and advice regarding fair play) 2 or 3× week for 33 weeks | Regular warm-up exercises, which usually consists of running exercises, dynamic and static stretching, and sprinting. | Soccer season | Physical complaint sustained by a participant that resulted from a soccer training session or soccer match, irrespective of the need for medical attention or time lost from soccer activities | intervention costs costs associated with the implementation of the preventive exercises costs of productivity losses due to absence from work ICER | Societal, EUR, 2009 | One-way using a range of estimates of cost items for injury prevention program | Not applicable 1 year |
| Marshall et al. 2016 [21] | Cluster RCT | male and female, ages 13–18 years INT: n = 380 CON: n = 364 | Fifteen-minute neuromuscular training in intervention group including 10 min of neuromuscular training components (e.g., strength, agility, balance) and 5 min of aerobic and dynamic stretching components, in addition to a 15 min home-based balance training (on a wobble board). | Standard of practice 15 min warm-up routine including aerobic, static stretching and dynamic stretching components and a home program, including only stretching components | Indoor soccer season + 6 months following the end of the season INT: h = 24,051 h of athlete participation CON: h = 23,597 h of athlete participation | Soccer-related injuries that required medical attention resulted in the inability to complete a session or in time loss from play | cost of injuries/1000 player hours cost of injuries/100 players mean cost per injury intervention costs ICER | Not stated, $, 2006–2007 | A sensitivity analysis was conducted in which the intervention costs (wobble boards and training session) were excluded from the total cost for the training group | Not applicable 1 year |
| Rössler et al. 2018 [4] | Cluster RCT | boys and girls, aged 7–12 years INT: n = 614, aged 11 (1.2) CON: n = 388 aged 10.6(1.1) | The “11+ Kids”, fifteen-minute injury prevention program at the beginning of each training session throughout the season | Regular warm-up program | Soccer season from August to June INT: h = 43,777 h of athlete participation CON: h = 32,596 h of athlete participation | Any soccer-related injuries that resulted in at least one of the following: (a) inability to complete the current match or training session and/or (b) absence from subsequent training sessions or matches and/or (c) injury requiring medical attention. | direct healthcare costs intervention costs intervention costs per player costs of a nationwide implementation of “11+ Kids” in Switzerland mean cost per player cost of injuries/1000 h of soccer ICER | Societal, EUR, 2014–2015 | Sensitivity analysis was performer by cutting the respective time period (exposure time and injury events) in the CON group at the beginning of the season | Not applicable 1 year |
| Criteria | Rössler 2018 | Marshall 2016 | Krist 2013 | Nouni-Garcia 2019 |
|---|---|---|---|---|
| yes | yes | yes | yes |
| yes | yes | yes | yes |
| yes | yes | yes | yes |
| yes | yes | yes | yes |
| yes | yes | yes | yes |
| yes | yes | yes | yes |
| yes | yes | yes | no |
| yes | yes | yes | no |
| yes | yes | yes | no |
| yes | yes | yes | yes |
| Total score | Good | Good | Good | Average |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grygorowicz, M.; Wiernicka, M.; Wiernicka, M. Systematic Review of Cost-Effectiveness of Injury Prevention Interventions in Soccer—Evidence Why Health Agencies Should Address It. Int. J. Environ. Res. Public Health 2021, 18, 11901. https://doi.org/10.3390/ijerph182211901
Grygorowicz M, Wiernicka M, Wiernicka M. Systematic Review of Cost-Effectiveness of Injury Prevention Interventions in Soccer—Evidence Why Health Agencies Should Address It. International Journal of Environmental Research and Public Health. 2021; 18(22):11901. https://doi.org/10.3390/ijerph182211901
Chicago/Turabian StyleGrygorowicz, Monika, Martyna Wiernicka, and Marzena Wiernicka. 2021. "Systematic Review of Cost-Effectiveness of Injury Prevention Interventions in Soccer—Evidence Why Health Agencies Should Address It" International Journal of Environmental Research and Public Health 18, no. 22: 11901. https://doi.org/10.3390/ijerph182211901
APA StyleGrygorowicz, M., Wiernicka, M., & Wiernicka, M. (2021). Systematic Review of Cost-Effectiveness of Injury Prevention Interventions in Soccer—Evidence Why Health Agencies Should Address It. International Journal of Environmental Research and Public Health, 18(22), 11901. https://doi.org/10.3390/ijerph182211901