
Examining and Promoting Sleep Health in the Undergraduate Classroom: A Mixed-Methods Approach



 ,
, 
Abstract
1. Introduction
1.1. Sleep Disturbances in College Students
1.2. Sleep Health in College Students
1.3. Sleep Interventions for College Students—Self-Determination Theory
2. Current Study
3. Methods
3.1. Participants
3.2. Measures
Sleep Health
3.3. Procedure
Sleep and Self-Determination Intervention
4. Data Analytic Plan
4.1. Quantitative Methods
4.2. Qualitative Methods
5. Reflexivity
6. Results
6.1. Aim 1: Describe Sleep Health in an Introductory Psychology Undergraduate College Sample
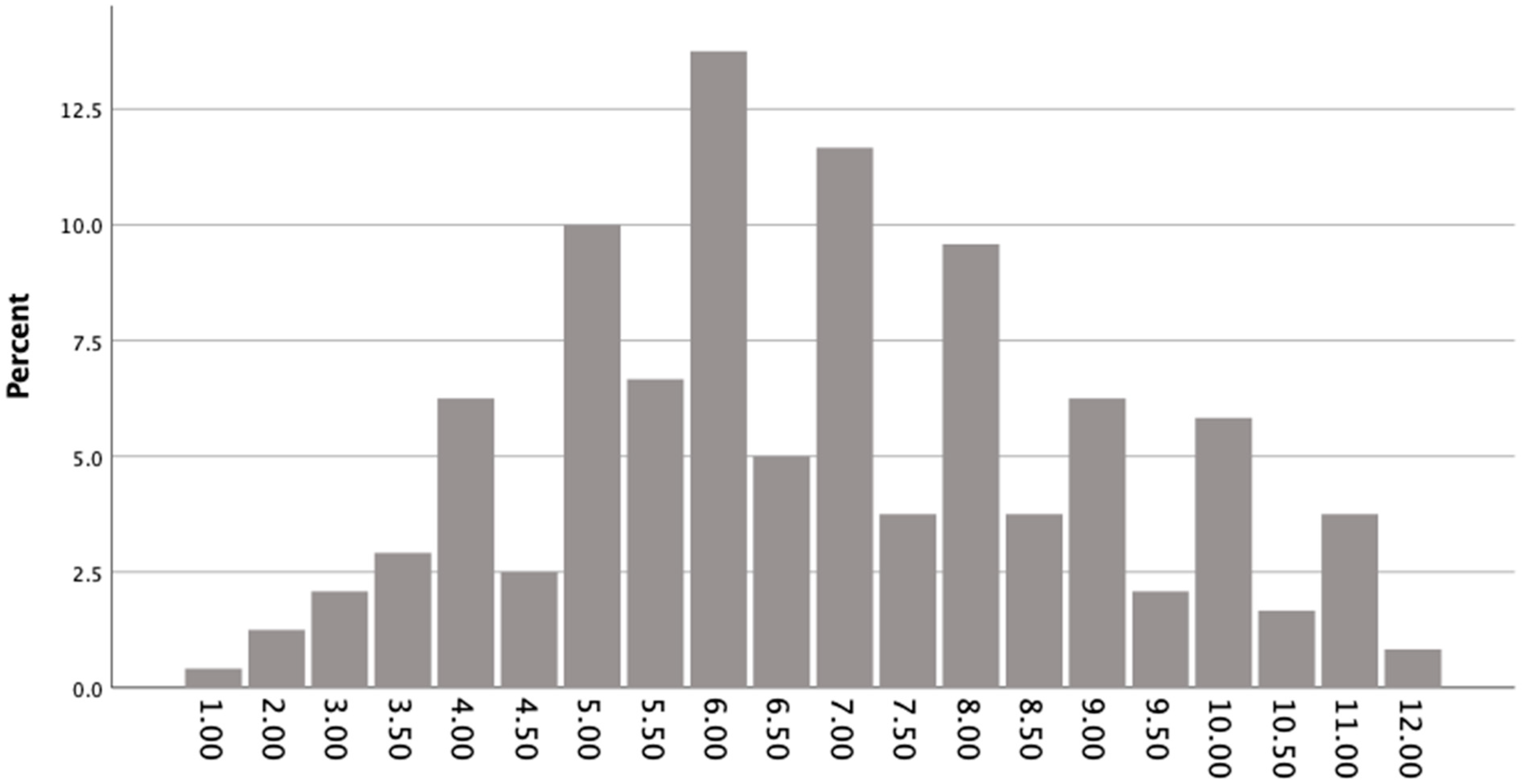
6.1.1. Quantitative Results
6.1.2. Qualitative Results
6.1.3. Integration of Quantitative and Qualitative Results
6.2. Aim 2: Describe and Evaluate the Effectiveness of a Self-Determination Intervention to Improve Sleep Health an Undergraduate College Sample
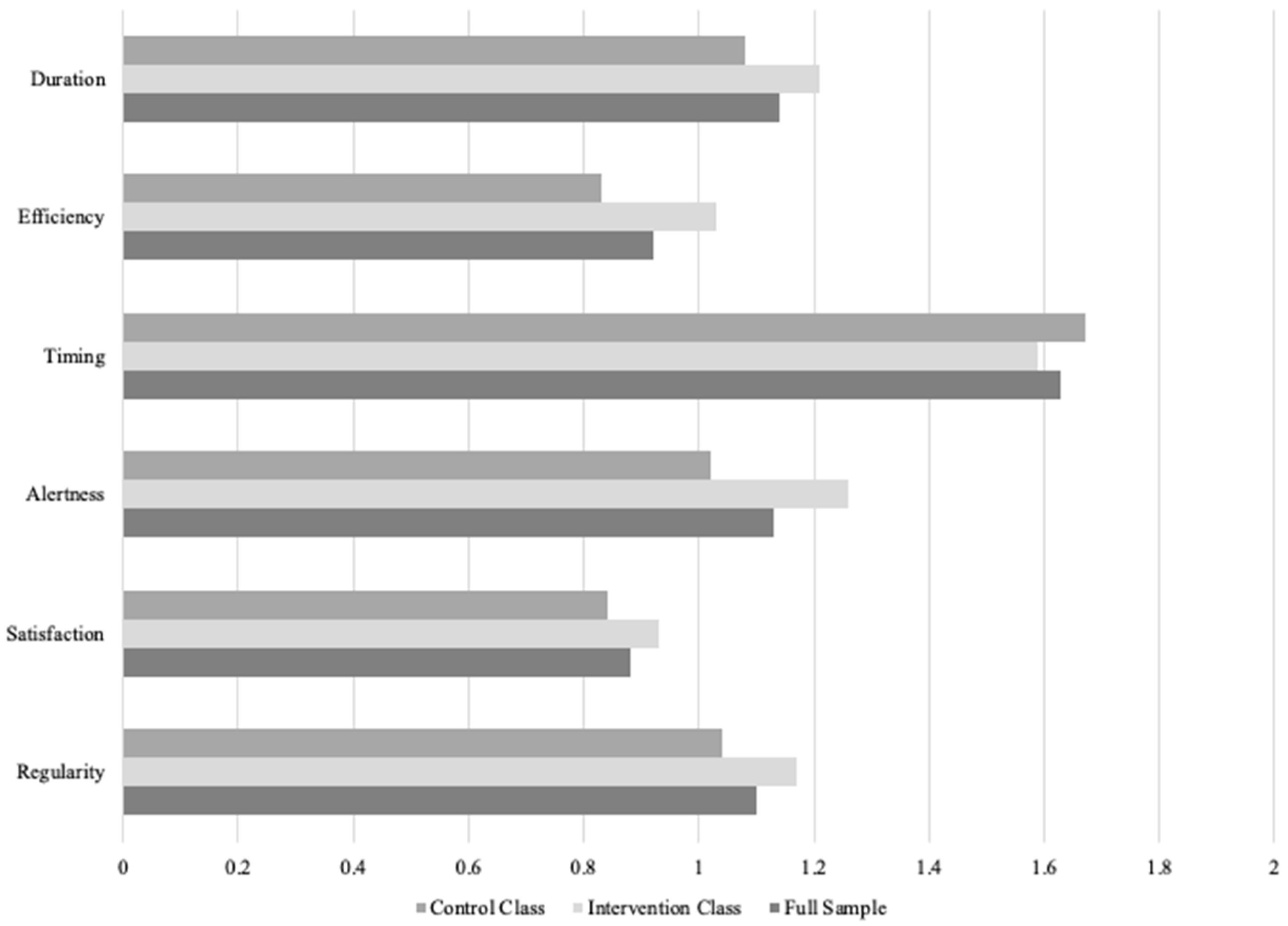
6.2.1. Quantitative Results
6.2.2. Qualitative Results
6.2.3. Integration of Quantitative and Qualitative Results
7. Discussion
7.1. Overview of Results
7.2. Theoretical and Clinical Implications
7.3. Limitations and Future Directions
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Berger, R. Now I see it, now I don’t: Researcher’s position and reflexivity in qualitative research. Qual. Res. 2015, 15, 219–234. [Google Scholar] [CrossRef]
- American Psychological Association. (n.d.). APA Introductory Psychology Initiative (IPI) Student Learning Outcomes for Introductory Psychology; American Psychological Association: Washington, DC, USA, 2021. [Google Scholar]
- Barber, L.K.; Cucalon, M.S. Modifying the Sleep Treatment Education Program for Students to include technology use (STEPS-TECH): Intervention effects on objective and subjective sleep outcomes. Stress Health 2017, 33, 684–690. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.P.; Jarrett, M.A.; Luebbe, A.M.; Garner, A.A.; Burns, G.L.; Kofler, M.J. Sleep in a large, multi-university sample of college students: Sleep problem prevalence, sex differences, and mental health correlates. Sleep Health 2018, 4, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis. Qual. Res. Sport Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Buboltz, W.C.; Brown, F.; Soper, B. Sleep habits and patterns of college students: A preliminary study. J. Am. Coll. Health 2001, 50, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J. Sleep health: Can we define it? Does it matter? Sleep 2014, 37, 9–17. [Google Scholar] [CrossRef]
- Campbell, R.; Vansteenkiste, M.; Delesie, L.M.; Mariman, A.N.; Soenens, B.; Tobback, E.; Van der Kaap-Deeder, J.; Vogelaers, D.P. Examining the role of psychological need satisfaction in sleep: A Self-Determination Theory perspective. Personal. Individ. Differ. 2015, 77, 199–204. [Google Scholar] [CrossRef]
- Clarke, V.; Braun, V. Thematic analysis. In Encyclopaedia of Quality of Life and Well-Being Research; Michalos, A.C., Ed.; Springer: Dordrecht, The Netherlands, 2014; pp. 6626–6628. [Google Scholar]
- Deci, E.L.; Ryan, R.M. Self-determination theory: A macrotheory of human motivation, development, and health. Can. Psychol./Psychol. Can. 2008, 49, 182–185. [Google Scholar] [CrossRef]
- Friedrich, A.; Schlarb, A.A. Let’s talk about sleep: A systematic review of psychological interventions to improve sleep in college students. J. Sleep. Res. 2018, 27, 4–22. [Google Scholar] [CrossRef]
- Griggs, S.; Conley, S.; Batten, J.; Grey, M. A systematic review and meta-analysis of behavioral sleep interventions for adolescents and emerging adults. Sleep Med. Rev. 2020, 54, 101356. [Google Scholar] [CrossRef]
- Franco, E.; Coterón, J. The Effects of a Physical Education Intervention to Support the Satisfaction of Basic Psychological Needs on the Motivation and Intentions to Be Physically Active. J. Hum. Kinet. 2017, 59, 5–15. [Google Scholar] [CrossRef]
- Gardner, P.; Kerridge, K. Everybody present: Exploring the use of an in-class meditation intervention to promote positive mental health among university students. Can. J. Community Ment. Health 2019, 38, 9–21. [Google Scholar] [CrossRef]
- Grandner, M.A.; Gallagher, R.A.L.; Gooneratne, N.S. The use of technology at night: Impact on sleep and health. J. Clin. Sleep Med. JCSM 2013, 9, 1301–1302. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Gurung, R.A.R.; Hackathorn, J.; Enns, C.; Frantz, S.; Cacioppo, J.T.; Loop, T.; Freeman, J.E. Strengthening introductory psychology: A new model for teaching the introductory course. Am. Psychol. 2016, 71, 112–124. [Google Scholar] [CrossRef] [PubMed]
- Hale, L.; Troxel, W.; Buysse, D.J. Sleep health: An opportunity for public health to address health equity. Annu. Rev. Public Health 2020, 41, 81–99. [Google Scholar] [CrossRef]
- Hublin, C.; Partinen, M.; Koskenvuo, M.; Kaprio, J. Heritability and Mortality Risk of Insomnia-Related Symptoms: A Genetic Epidemiologic Study in a Population-Based Twin Cohort. Sleep 2011, 34, 957–964. [Google Scholar] [CrossRef] [PubMed]
- Koydemir, S.; Sun-Selışık, Z.E. Well-being on campus: Testing the effectiveness of an online strengths-based intervention for first year college students. Br. J. Guid. Couns. 2016, 44, 434–446. [Google Scholar] [CrossRef]
- Lazard, L.; McAvoy, J. Doing reflexivity in psychological research—What’s the point? What’s the practice? Qual. Res. Psychol. 2020, 17, 159–177. [Google Scholar] [CrossRef]
- Levenson, J.C.; Miller, E.; Hafer, B.L.; Reidell, M.F.; Buysse, D.J.; Franzen, P.L. Pilot study of a sleep health promotion program for college students. Sleep Health 2016, 2, 167–174. [Google Scholar] [CrossRef]
- Lund, H.G.; Reider, B.D.; Whiting, A.B.; Prichard, J.R. Sleep Patterns and Predictors of Disturbed Sleep in a Large Population of College Students. J. Adolesc. Health 2010, 46, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Nebes, R.D.; Buysse, D.J.; Halligan, E.M.; Houck, P.R.; Monk, T.H. Self-Reported Sleep Quality Predicts Poor Cognitive Performance in Healthy Older Adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2009, 64B, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Neuendorf, K.A. Content analysis and thematic analysis. In Advanced Research Methods for Applied Psychology; Routledge: Abingdon, UK, 2018. [Google Scholar]
- Orzech, K.M.; Salafsky, D.B.; Hamilton, L.A. The State of Sleep Among College Students at a Large Public University. J. Am. Coll. Health 2011, 59, 612–619. [Google Scholar] [CrossRef] [PubMed]
- Ravyts, S.G.; Dzierzewski, J.M.; Perez, E.; Donovan, E.K.; Dautovich, N.D. Sleep Health as Measured by RU SATED: A Psychometric Evaluation. Behav. Sleep Med. 2021, 19, 48–56. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Self-Determination Theory and the Facilitation of Intrinsic Motivation, Social Development and Well-Being. Am. Psychol. 2000, 55, 68. [Google Scholar] [CrossRef]
- Schut, H.A.; Stam, H.J. Goals in rehabilitation teamwork. Disabil. Rehabil. 1994, 16, 223–226. [Google Scholar] [CrossRef]
- Springer, J.B.; Lamborn, S.D.; Pollard, D.M. Maintaining Physical Activity over Time: The Importance of Basic Psychological Need Satisfaction in Developing the Physically Active Self. Am. J. Health Promot. 2013, 27, 284–293. [Google Scholar] [CrossRef]
- Tang, M.; Wang, D.; Guerrien, A. A systematic review and meta-analysis on basic psychological need satisfaction, motivation, and well-being in later life: Contributions of self-determination theory. PsyCh J. 2020, 9, 5–33. [Google Scholar] [CrossRef]
- Taylor, D.J.; Gardner, C.E.; Bramoweth, A.D.; Williams, J.M.; Roane, B.M.; Grieser, E.A.; Tatum, J.I. Insomnia and Mental Health in College Students. Behav. Sleep Med. 2011, 9, 107–116. [Google Scholar] [CrossRef]
- Verstuyf, J.; Patrick, H.; Vansteenkiste, M.; Teixeira, P.J. Motivational dynamics of eating regulation: A self-determination theory perspective. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 21. [Google Scholar] [CrossRef]
- Vidic, Z.; Cherup, N. Mindfulness in classroom: Effect of a mindfulness-based relaxation class on college students’ stress, resilience, self-efficacy and perfectionism. Coll. Stud. J. 2019, 53, 130–142. [Google Scholar]
- Wittmann, M.; Dinich, J.; Merrow, M.; Roenneberg, T. Social Jetlag: Misalignment of Biological and Social Time. Chronobiol. Int. 2006, 23, 497–509. [Google Scholar] [CrossRef] [PubMed]
- Foulkes, L.; McMillan, D.; Gregory, A.M. A bad night’s sleep on campus: An interview study of first-year university students with poor sleep quality. Sleep Health 2019, 5, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, M.H.; Bos, S.C.; Soares, M.J.; Marques, M.; Pereira, A.T.; Maia, B.; Gomes, A.A.; Macedo, A. Longitudinal study on perfectionism and sleep disturbance. World J. Biol. Psychiatry 2010, 11, 476–485. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.M.; Robertson, G.C.; Dyson, R.B. Prospective Relationship Between Poor Sleep and Substance-Related Problems in a National Sample of Adolescents. Alcohol. Clin. Exp. Res. 2015, 39, 355–362. [Google Scholar] [CrossRef]
- Zhai, L.; Zhang, H.; Zhang, D. Sleep Duration and Depression among Adults: A Meta-Analysis of Prospective Studies: Research Article: Sleep Duration and Depression. Depress. Anxiety 2015, 32, 664–670. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Psychological Needs in Self-Determination Theory | Intervention |
|---|---|
| Competence | “There are probably a lot of things you’re already doing well regarding your sleep habits. If you think about it, you have come this far because you’re doing something right! Your personal strengths and knowledge about yourself as an individual will make you successful in achieving goals related to improving your sleep habits. What is something you already do well regarding your sleep habits?” |
| Autonomy | Review SMART goal setting |
| “Brainstorm three areas where you might want to make SMART goals to improve your sleep. You could focus on an area of sleep that you are already doing well in or an area of sleep that you are struggling. Some examples of areas to work on could be: regular bed/wake times, getting 7-9 h of sleep, limiting technology in bed, etc.” | |
| “You are the most knowledgeable about what you do well, what you need, and your specific context. Out of the three areas you listed, choose which area you would like to focus on changing. Write a SMART goal for this chosen area.” | |
| Relatedness | “Discuss with a class partner which SMART goal you chose. What do you anticipate could make completing that goal difficult? Brainstorm solutions to possible barriers with a partner.” |
| Question 1: What is Something You Already Do Well Regarding Your Sleep Habits? | ||
|---|---|---|
| Theme | Representative Response | % of Sample |
| Rhythmicity/Timing of Wake and Sleep | “Something that I already do well regarding sleep habits is that I sleep and wake up around the same time everyday.” | 24.21% |
| Prioritizing Sleep Duration | “I get the suggested amount of sleep for my age every night.” | 22.14% |
| General Sleep Timing | “I try to go to sleep no later than 1am, that’s my stopping point.” | 11.43% |
| Tech Hygiene | “I don’t look at my phone before going to sleep as the blue light emitted from a cell phone can make it hard to go to sleep and keep me up longer.” | 10.71% |
| Sleep Hygiene | “I don’t drink caffeine towards the end of the day.” | 7.86% |
| Bedtime Routine | “I have a nightly routine that helps prepare my body and mind for rest.” | 7.14% |
| Other (monitoring, substances) | “Take melatonin to fall asleep faster/easier.” | 7.14% |
| Daytime Activities | “I always try to do my homework early so that I am not up late at night working on it.” | 3.57% |
| Stimulus Control | “Something I already do well regarding my sleep habits is sleep when sleepy. When I get really tired I just head to bed and shlump.” | 2.86% |
| Creating an Environment Conducive to Sleep | “I sleep with two fans on and have many pillows and blankets in my comfy bed.” | 2.86% |
| Question 2: Brainstorm Three Areas That You Might Want to Make SMART Goals to Improve Your Sleep. | ||
|---|---|---|
| Theme | Representative Response | % of Sample |
| Sleep Hygiene | “quit smoking right before bed. no naps, makes me less tired when bedtime actually hits.” | 20.92% |
| Consistent Sleep Schedule | “I would like to get 7-9 h of sleep on the daily to feel fully awake and aware in the morning.” | 17.57% |
| Tech Hygiene | “The last goal that I would like to make would be to limit my technology usage before bed. When I lay down to go to bed, I normally stay awake for another 30ish minutes going through my phone which I know is very bad for sleep hygiene, so I would like to fix this.” | 17.15% |
| Stimulus Control | “sleeping when sleepy, I have this habit of fighting my sleep during the day when I know I need some shut-eye.” | 15.48% |
| Sleep Duration | “The first area I would like to work on is the amount of time I sleep. I would like to get at least 8 h a night but that’s asking a lot” | 8.37% |
| Daytime Activities | “Lastly I want to work on keeping my daytime routine the same since being in college everyday is not the same so I would like to work on that.” | 8.37% |
| Other (substances, earlier wake/sleep time) | “I also need to avoid alcohol as I’m unable to sleep at all without it and that’s super unhealthy!” | 5.86% |
| Bedtime Routine | “I also want to come up with a sleep ritual for before I go to bed, maybe it could improve the quality of my sleep.” | 3.35% |
| Monitoring | “Keeping a sleep diary.” | 1.67% |
| Strategic Napping | “I take a lot of naps during the day, I could cut back on those for better sleep at night.” | 1.26% |
| Question 3: Out of the Three Areas You Listed, Choose Which Area You Would Like to Focus On Changing? Write a SMART Goal for This Chosen Area. | ||
|---|---|---|
| Theme | Representative Response | % of Sample |
| Sleep Hygiene | “I will not nap in between my classes on Wednesdays (my busiest days) for the next two weeks and see how this impacts my sleeping habits/productivity” | 22.22% |
| Tech Hygiene | “I will put my phone and computer away 15 min before bed at night. Instead of using social media and technology before bed I will pick up reading as a better way to clear my mind at night.” | 19.44% |
| Stimulus Control | “I will do my homework only at my desk and leave my bed for relaxation and sleep purposes only for the next two weeks so that I can test if I am able to get better sleep as a result.” | 14.81% |
| Sleep Timing | “I will sleep between 10:30-12 on weekdays and before 2 on weekends for the rest of the semester.” | 12.04% |
| Regular Sleep Schedule | “I will go to bed and wake up at the same time for the next 2 weeks.” | 11.11% |
| Daytime Routine | “I will work out every day to help me feel more tired.” | 8.33% |
| Other (wake time adjustment, finding new spaces for daily tasks) | “Mainly I would like to fix the amount of time I spend in my bedroom. I don’t think that it is conducive to getting work done and it makes it harder to get to sleep when I need to be sleeping. My goal would be to change this behavior by establishing other locations that I can get my homework done and if I want to spend time watching television and relaxing during the day I should change that space as well.” | 5.56% |
| Bedtime Routine | “I will practice relaxing stretches 15 min before going to bed each night for the next 4 weeks.” | 3.70% |
| Prioritizing Sleep Duration | “I will strive to get at least 8 h of sleep.” | 2.78% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dautovich, N.D.; MacPherson, A.R.; Ghose, S.M.; Williams, C.M.; Reid, M.P.; Sabet, S.M.; Soto, P.; Jones, S.C.T.; Dzierzewski, J.M. Examining and Promoting Sleep Health in the Undergraduate Classroom: A Mixed-Methods Approach. Int. J. Environ. Res. Public Health 2021, 18, 12297. https://doi.org/10.3390/ijerph182312297
Dautovich ND, MacPherson AR, Ghose SM, Williams CM, Reid MP, Sabet SM, Soto P, Jones SCT, Dzierzewski JM. Examining and Promoting Sleep Health in the Undergraduate Classroom: A Mixed-Methods Approach. International Journal of Environmental Research and Public Health. 2021; 18(23):12297. https://doi.org/10.3390/ijerph182312297
Chicago/Turabian StyleDautovich, Natalie D., Ashley R. MacPherson, Sarah M. Ghose, Claire M. Williams, Morgan P. Reid, Sahar M. Sabet, Pablo Soto, Shawn C. T. Jones, and Joseph M. Dzierzewski. 2021. "Examining and Promoting Sleep Health in the Undergraduate Classroom: A Mixed-Methods Approach" International Journal of Environmental Research and Public Health 18, no. 23: 12297. https://doi.org/10.3390/ijerph182312297
APA StyleDautovich, N. D., MacPherson, A. R., Ghose, S. M., Williams, C. M., Reid, M. P., Sabet, S. M., Soto, P., Jones, S. C. T., & Dzierzewski, J. M. (2021). Examining and Promoting Sleep Health in the Undergraduate Classroom: A Mixed-Methods Approach. International Journal of Environmental Research and Public Health, 18(23), 12297. https://doi.org/10.3390/ijerph182312297