Abstract
Introduction: Engagement and co-production in healthcare research and innovation are crucial for delivering person-centred interventions in underserved communities, but the knowledge of effective strategies to target this population is still vague, limiting the provision of person-centred care. Our research aimed to identify essential knowledge to foster engagement and co-production. Materials and Methods: A meta-synthesis research design was used to compile existing qualitative research papers on health communication, engagement, and empowerment in vulnerable groups in high-income countries (HICs) from 2008 to 2018. A total of 23 papers were selected and analysed. Results: ‘Design and recruitment’ and ‘engagement and co-production’ thematic areas are presented considering the factors related to researcher–communities attunement and the strategical plans for conducting research. The insights are discussed in light of the literature. Long-term alliances, sustainable structures, and strengthened bonds are critical factors for producing real long-term change, empowering persons and communities, and paving the way to person-centred care. Conclusions: The enhancement of the recruitment, involvement, and empowerment of traditionally disengaged communities and individuals depends on the awareness and analysis of social determinants, power differentials and specific tactics, and the capacity of researchers and individuals to apply all these principles in real-world practice.
1. Introduction
Co-production and engagement of individuals and communities are critical for designing person-centred care, and they are even more crucial if the service users are socially vulnerable groups (e.g., traditionally discriminated or marginalised minorities, including racialised groups, deprived communities, or sexual minorities, among others). Vulnerability is understood as the result of specific socio-economic, demographic, cultural, institutional, spatial, and environmental contexts [1] encompassing the susceptibility to hazards, and then, the diminished capacity to cope and/or to adapt. Thus, “vulnerability” is opposed to “resilience”, or the capacity of social, economic, and environmental systems for coping with hazardous events, disturbances, and adverse events, being able to respond and to maintain, transform, or adapt their basic functions, identities, or structures [2].
Traditionally discriminated, marginalised, or excluded communities are considered vulnerable in this article: the historical power imbalance might diminish the ability of these communities and individuals to cope with adverse events due to structural reasons. Other vulnerability conditions that are included are: (i) rural areas, due to their partial isolation and lack of access to key results [3,4,5,6]; (ii) youngest and oldest persons, due to ageism [7,8]; (iii) persons with diagnosis of mental disorders and people with disabilities, due to structural discrimination (mentalism and ableism), stigma, stereotypes, and problems in accessing regular healthcare [9]; and (iv) impoverished persons and communities, also excluded or at higher risk of social exclusion due to systemic determinants [10]. Considering an intersectional perspective, all these disparities potentially leading to marginalisation, exclusion, and discrimination are acquired in the social interaction and reproduced in such a way that various forms of inequalities operate together, exacerbating each other [11,12].
Besides, this study differentiates between hard-to-reach, hidden, and disengaged populations. Hard-to-reach are those groups that are difficult to involve due to their physical, geographical, socio-economic, or socio-cultural situation. Hidden populations are persons who do not wish to be found (e.g., irregular migrants or drug users) [13], whereas disengaged refers to persons or communities not actively involved or considered in the research, co-design of interventions, or even health education programmes (their degree of reluctance may vary, and refers only to a lack of participation).
Considering the above, co-production and engagement present three challenges in health research and participatory research for person-centred care. Firstly, how to raise the recruitment and participation of disengaged and hard-to-reach communities [14]. Secondly, to which extent research could empower or, on the contrary, disempower individuals and communities [15]. Thirdly, how to engage them, paying attention to social determinants, specific difficulties, and power imbalances within the research context [16].
The community-centric approach, as well as individual and community engagement and empowerment, will be further examined to establish the foundation for obtaining knowledge about the recruitment, retainment, alliance-building, and co-production processes:
The community-centric approach is an integrative process to overcome the limitations of traditional research and biomedical models—such as the immutability of individual risk factors or the restrictive focus—by considering the bio-psycho-social perspective [15]. Community-centric approaches can unveil factors that may condition the acceptance of public health campaigns or behavioural change. Consequently, engagement and empowerment are central concepts.
Engagement is widely used in the literature to refer to the community aiming to reach a long-term alliance [17]. The engagement is related to health outcomes for communities and individuals. It is suggested that involving patients as partners in the long term facilitates patient-centred care delivery [18], helping to ensure that research efforts address relevant clinical questions, through the co-design of the agenda, leading to more adequate research design, which may imply to involve community stakeholders [19]. Community engagement includes patients and service users participating in research and healthcare innovation. It entails a long-term involvement (co-production) and alliance at the community level as a whole, implying a multi-stakeholder approach [20,21,22]. Patients’ knowledge, health conditions, beliefs, and experiences impact their decisions to be engaged in interventions and initiatives and, most likely, in research projects [23]. At the individual level, engagement infers the involvement and active participation of an individual in the therapeutical or research process integrating information, professional advice, personal needs and preferences, and their own competencies and abilities in managing their own health [24]. It may also involve a medium- and long-term sustainable relationship with feasible changes at the behavioural level, specifically in self-caring and self-management of health. Moreover, it contributes to the maintenance of health-promotion initiatives by fostering its sustainability over time [25].
Empowerment was understood in this study by considering three key elements: (i) counter-hegemonic rupture; (ii) advocacy; and (iii) locus of control. At the community/social level, empowerment sometimes involves a rupture of the hegemonic order—or the status quo—in which counter-hegemonic forces/groups dispute their own rights, and thus power, in conflict with the ruling elite/s. This notion, related to the rights and collective identity of discriminated minorities (e.g., ethnic minorities), implies deeper and substantial changes in the societal and systemic order itself [15,26]. At the community level, empowerment as advocacy aims at raising the capacity of individuals and communities to control their circumstances through exercising power framed in collective and collaborative efforts. In other words, and specifically applied to health promotion, it implies ‘identity, knowledge and understanding, personal control, personal decision-making, and enabling other patients’ [27]. Finally, empowerment could have a more individualistic meaning, involving both a sense of agency and locus of control [28]; and also in terms of ‘informed patient’ or ‘reflexive consumer’.
The meta-synthesis, based on the meta-ethnography approach sustained by Noblit and Hare [29]—but with some adaptations to effectively cover, relate, compare, and inter-translate the very large sample of studies further detailed in the section on Materials and Methods—has been extensively used for health, social care, and person-centred care research; in particular, for examining the complex relations between a vast range of social and environmental determinants. The meta-synthesis is a systematic review of primary qualitative studies that also aims at building middle-range theory for constructing new frameworks to inform policies, research, and clinical or assistance practice. It applies to multi-faceted health and social care issues by developing new frameworks, comprising health services, policy analysis, strategies, programme and intervention insights, experiences, and social and systemic determinants [30,31]. It was utilised for acquiring knowledge on decision making and patient–provider communication [28], programmes addressed to women with substance use problems [32], studies of exercise programmes for older persons [33], the exploration of the person-centred care concept [34], the experience of disease and the ethnicity [35], or the peer-based support [36].
This study aimed at unveiling the key mechanisms for conducting research under participatory, inclusive approaches involving vulnerable groups through a critical revision of the current qualitative evidence collected in real research project settings. The specific objectives were: (i) to identify key factors to foster recruitment and engagement; and (ii) to improve co-production processes involving vulnerable groups (including hard-to-reach, hidden, and disengaged populations) to support communities in fostering their empowerment at a collective level.
2. Materials and Methods
This research summed up the partial results of a meta-synthesis using a sample of 102 studies, including journal articles, PhD theses, and master’s degree dissertations. All studies included in the present article were scientific peer-reviewed articles.
2.1. Search Strategy
The literature search was conducted in the University of Valencia database (Trobes) and Google Scholar. Trobes includes the Cochrane Library, SCOPUS, Web of Science, Journal Citation Reports, M3edLine, Proquest Central, and Proquest Dissertations and Theses, among others, and can be found at https://trobes.uv.es/ (accessed on 22 November 2021). Google Scholar was used to find peer-reviewed grey literature, avoiding publication bias. The following keywords were used in both databases:
- Qualitative study
- Health communication
- Recruitment
- Empowerment
- Engagement
- Chronic
- Long-term condition
- Participation
- Vulnerable
- Recruitment
- Hard-to-reach
2.2. Selection Process and Eligibility Criteria
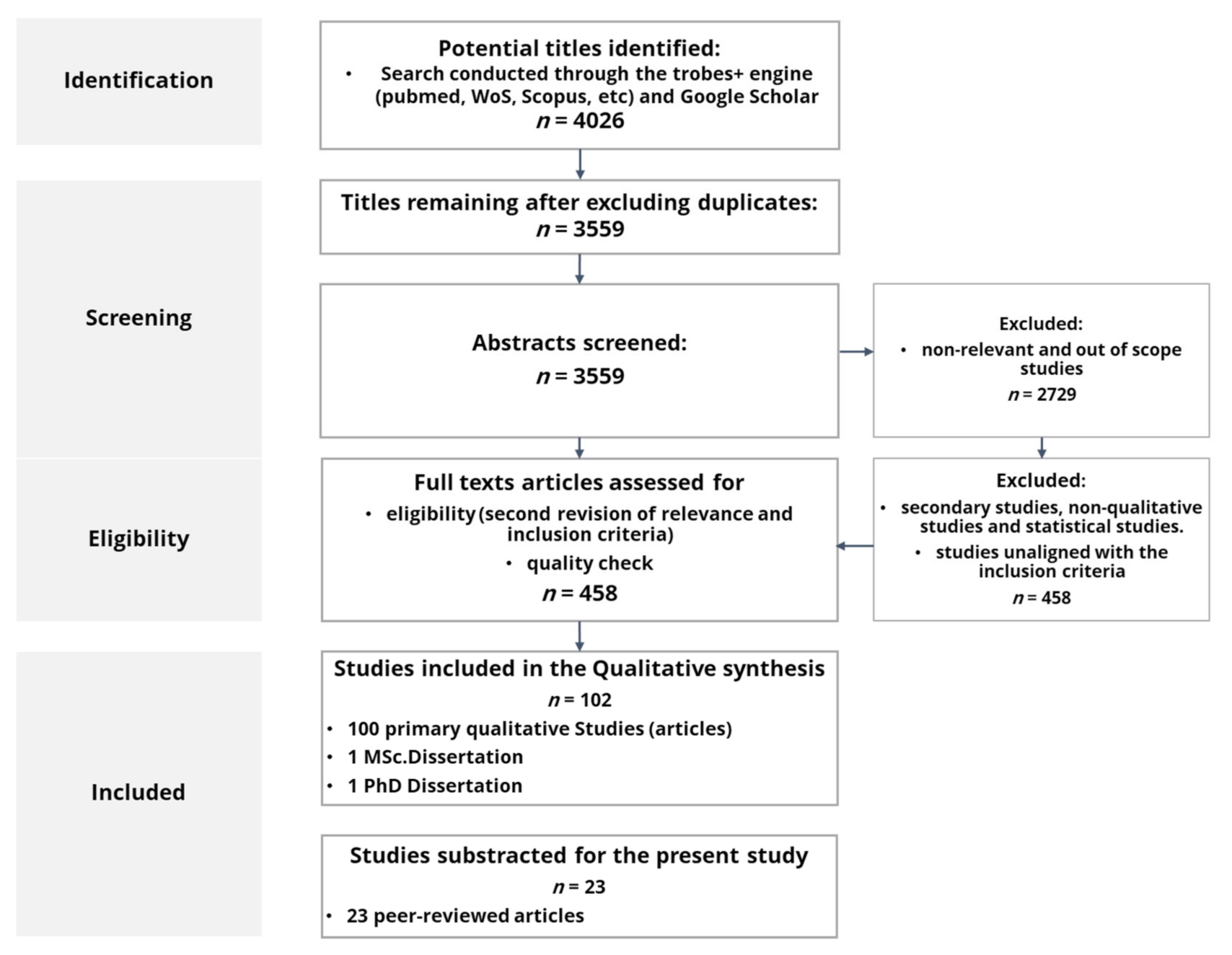
As Figure 1 details, initial results showed 4026 references (3559 after deleting duplicates; 2729 after deleting irrelevant and non-related results) from 2008 to 2018, comprising the period of the economic and financial crisis. Since financial crises imply limited resources devoted to health promotion, investigating how to foster health communication, literacy, self-management, empowerment, and co-production in a period of crisis has a clear intrinsic interest.
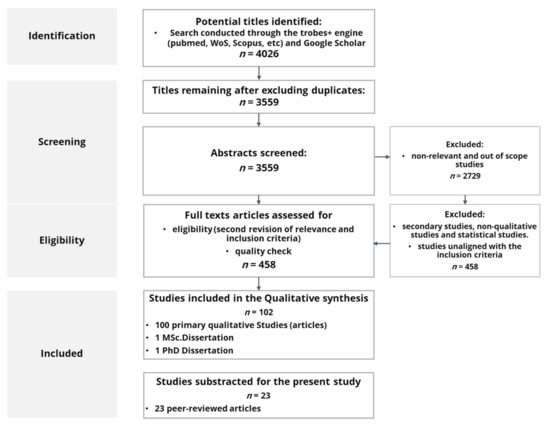
Figure 1.
Search strategy and result diagram.
Papers meeting the exclusion criteria were excluded from the analysis (see Table 1). As a result, 458 studies were scanned and assessed for the final selection, considering the inclusion criteria and the quality control through the Critical Skills Programme (CASP) questionnaire for qualitative research papers. Finally, 102 studies meeting all inclusion criteria and rated as excellent (CASP ≥ 8) were included in the final sample.

Table 1.
Inclusion and exclusion criteria.
2.3. Data Extraction and Analysis
PDFs (full texts of each article) were downloaded. Both the full paper as well as the section on Results were coded and analysed using MAXQDA (Verbi®® v2018–2020) following a meta-synthesis method [29] based on the grounded theory. The grounded theory analysis is based on the lack of predefinition of the themes extracted: the rationale for this innovative approach is that the widely used principles of grounded theory could be applied to a large meta-synthesis in order to ensure that all meanings and metaphors are well captured, but at the same time, the structure of the information is comprehensive but still manageable in order to generate lines of argument and new models and implications for practice. Specifically, the grounded theory approach facilitated that codes and themes arising from the information and the materials were effectively related to each other, and then inter-translated and compared. The qualitative data was tagged according to those repeated ideas and emerging iterative concepts, following an inductive reasoning led by the materials themselves in order to generate the core lines of argument, and then middle-range theories [37].
The analysis was conducted on 102 selected studies. Among them, 23 studies were directly related to the following codes: ‘recruitment for research’, ‘participating in research’ and ‘researching in the community’. Papers selected are cited within the Appendix B.
2.4. Characteristics of the Papers Selected for the Meta-Synthesis
Table 2 presents the studies’ characteristics.
Table 2.
Studies included, characteristics, and ethical considerations.
The sample analysed in the 23 studies selected covered qualitative data from 786 individuals. However, the figures behind the data remain unclear, since some research papers conducted a participatory observation of very large samples. The sample remains unclear because the audience of these meetings cannot be easily specified. Besides, 37 reports were included by the researchers, as well as 16 visits to stakeholders, and 10 organisations were studied.
The composition of the meta-sample was as follows:
- 160 healthcare professionals (HCPs) (28 females, 2 males, and 120 non-specified);
- 196 healthcare and social workers (e.g., managers, researchers, social workers, community workers, key informants, business and public administration officers, and policy specialists);
- 3 caregivers/relatives;
- 17 patient representatives;
- 356 patients (195 females, 161 males; 79 non-specified).
It is worth noting that some studies included the general population and a vast range of healthcare users with different socio-economic and socio-cultural backgrounds—that may also entail traditionally discriminated persons and communities. These studies were included due to their conceptual richness and the inclusion of patients from all backgrounds. Table 3 sums up the sampled studies.
Table 3.
Thematic coverage and sample of the papers included in the meta-synthesis.
3. Results and Discussion
Twenty-three (23) papers matching the theme ‘Research’ were identified. The papers were related to:
- Designing and recruiting in research and healthcare innovation for person-centred care. This theme covered the first stages, from the design to the recruitment of individuals and leaders in the community, and how the plan itself, the participation, and the methods used during these phases could contribute to the improvement of the subsequent stages.
- Engagement and co-production as a means for empowering persons and communities. This covered the research and co-production conduction and how to engage individuals and engagement; thus, phases covered were implementation and, if applicable, evaluation, until the end of each study.
In addition, two analytic themes were used for classifying the information: facilitators and barriers. The constructed items also were classified as factors linked to ‘community–researchers attunement’ and ‘comprehensiveness of the strategic plans’. Each item contained into these two categories was re-interpreted and summarised to capture the key idea behind the statements analysed to make them operative for constructing middle-range theories (full quotations are shown in the complementary materials).
3.1. Analysis of Design & Recruitment Factors
Table 4 summarises the key facilitators and barriers (sources are quoted in lowercase letters to facilitate the distinction between the papers comprising the sample, cited in the Appendix B, and the general sources referenced).
Table 4.
Facilitators and barriers during design and recruitment.
As facilitators, the texts analysed emphasised the importance of preparing the information with adequate and tailored content and format, adapted to the community to be reached during the design and recruitment phases (l)(m)(q)(t). It may also imply the cultural adequacy of materials, contents, and means used for their engagement. Enough information needs to be provided, always in an understandable way (l)(m)(q)(t). Community leaders and civil society organisations (CSOs) should be involved, and they can be essential to lead the recruitment, retention, designing of information materials, and dissemination of resources or the assessment procedures (q)(s)(t). It is also relevant to include in the design process an adequate budget planning, as long as the involvement of communities may imply a different allocation of resources compared with traditional methods (l)(p)(t).
The emerged topics show that a real concern, knowledge, and interest in the community is important during this phase (l)(p)(q). To plan how to establish trust and rapport with the participants and, if needed, leaders, is key to ensure their short- and medium-term retainment (b)(i)(p)(r)(t). The qualitative data also reflect that during the recruitment, it is essential to clarify how the study meets the community needs and preferences (g)(x), and to ensure the relevance by finding practical applications of the research and/or its outcomes (p)(x), In some cases, health education or enhancement of this type of literacy should be provided (g)(x). Questionnaires and tools, if not standardised, may need to be adapted, including the terms, language, and jargon (g). To facilitate recruitment, the research and co-production process should be designed with individuals in a flexible way, ensuring adaptability of schedules, meetings, questionnaires, and any other research resource. (i)(q).
The improvement of the cultural competencies and openness of the researchers (g)(x) has been mentioned as a requirement. In particular, the study (x) includes the confidence in narratives (of the community members) and the acknowledgement of their contributions. Once more, trust in researchers appears as a key factor (x)(v).
Scepticism and mistrust are significant barriers to accessing the sample (p)(v)(x)(c), and the difficulty for reaching and engaging the right persons for the recruitment (q). However, in early stages, the main barriers are given by individual factors, such as a lack of self-confidence (d)(q), feeling triggered by sensitive issues (i), or being afraid about legal consequences (c). The lack of information fosters distrust and imbalance of power (t). Fear to disclose private information also appears (i) and, from the side of patients or community organisations, fear of worsening the current stigmatisation of some persons (p). Lastly, the distrust in some communities limits the recruitment scope (v). Other barriers to consider, depending on the group/s targeted, are a disproportionate vulnerability to punitive legal/policy consequences (the fear of persecution may prevent persons and groups from participating (c)), the fear of being further demonised or stigmatised (p), or the previous reluctance to seek medical care (g).
Administrative barriers, highlighting the socio-political environment, are based on the conflicts around the definition of the research agenda, appearing early in the design, even during the proposal stages (p)(t): the lack of resources and the excessive workload to meet specific patients’ and communities’ needs may be an additional source of conflicting agendas (b)(l)(m)(q). These may also prevent the implementation of interventions, programmes, or research projects (b)(l).
3.2. Analysis of Engagement and Co-Production Factors
Facilitators and barriers emerging from the texts’ interpretation concerning the engagement and co-production processes are summarised in Table 5.
Table 5.
Facilitators and barriers during the engagement of participants and the co-production process.
Concerning the key elements found relevant in the analysed papers for the engagement and co-production with vulnerable groups in health research, the most important facilitators were the active involvement of healthcare professionals (j)(p)(q)(r)(s), the early involvement in the process of researching and innovating (p)(q)(s)(x), the community and the leadership’s trust in the researchers (c)(o)(p)(r)(t)(v)(x), and the provision of feedback and recognition of the contributors’ role, even by acknowledging the co-ownership if possible (l)(s)(u)(v). One of the most important facilitators was to offer a long-term perspective: firstly, by developing community structures, which often involves a meaningful co-ownership (g)(p)(q); secondly, by acknowledging their contributions (l)(s)(u)(v); thirdly, by ensuring financial transparency (m); and fourthly, by offering long-term support by the research entity to the community or advocacy group (l)(p). Another facilitator mentioned was the sensitivity and confidentiality of the process, a requirement to encourage patients to participate in the discussions and feel confident to talk and explain their views (l)(q)(r)(s)(v)(e). To build trust and rapport among participants, community stakeholders, leaders (if any), and researchers is crucial for retaining persons (p)(s)(x)(c).
The researchers′ cultural and linguistic competencies were also essential. Terms should be adapted during the meetings, as well as in materials, questionnaires, or any other resource provided (l)(p)(x). The researchers′ characteristics were considered relevant: their expertise, availability, and social skills, as well as the reputation of their institution and the resources available, matter in engaging and co-producing with vulnerable groups in research (p)(v).
Critical barriers also were identified in the qualitative research, with special relevance of the lack of trust in the researcher (c)(o)(p)(r)(t)(v)(x), which might be mutual (c)(o)(p)(t). In addition, tokenism and technocratic approaches appeared to prevent adequate engagement and co-production processes (a)(f)(k)(l)(p)(q)(t). Communication problems were also emphasised in various studies (i)(k)(l)(p)(q). The issues reported included paternalistic communication, and dismission or rejection of experiential knowledge as subjective, private, and irrelevant (k); researchers also might have problems in communicating well with patients, being misunderstood (l). In (p) and (l), jargon and non-emotional communication (e.g., a researcher dispassionately talking about his disease), and feeling ignored or unable to contribute to the project (l), including feeling disqualified and not listened to (q), were addressed.
Again, conflicting agendas between communities, researchers, and/or research institutions also play a limiting role in the successful engagement of communities and vulnerable individuals (k)(o)(p)(f). Moreover, the greater complexity of participative approaches in research, such as the co-production, is seen as a barrier. Finally, an additional barrier for the researchers to implement these approaches was their potential perception of lack of rigour, mainly due to two main pre-conceptions: firstly, the perceived lack of knowledge of the community in the scientific and/or health-specific topic (the community contributors are laypersons) (j)(k)(l)(p); and secondly, the involvement of the vulnerable groups could be understood as a loss of neutrality (p)(q)(s).
3.3. Discussion
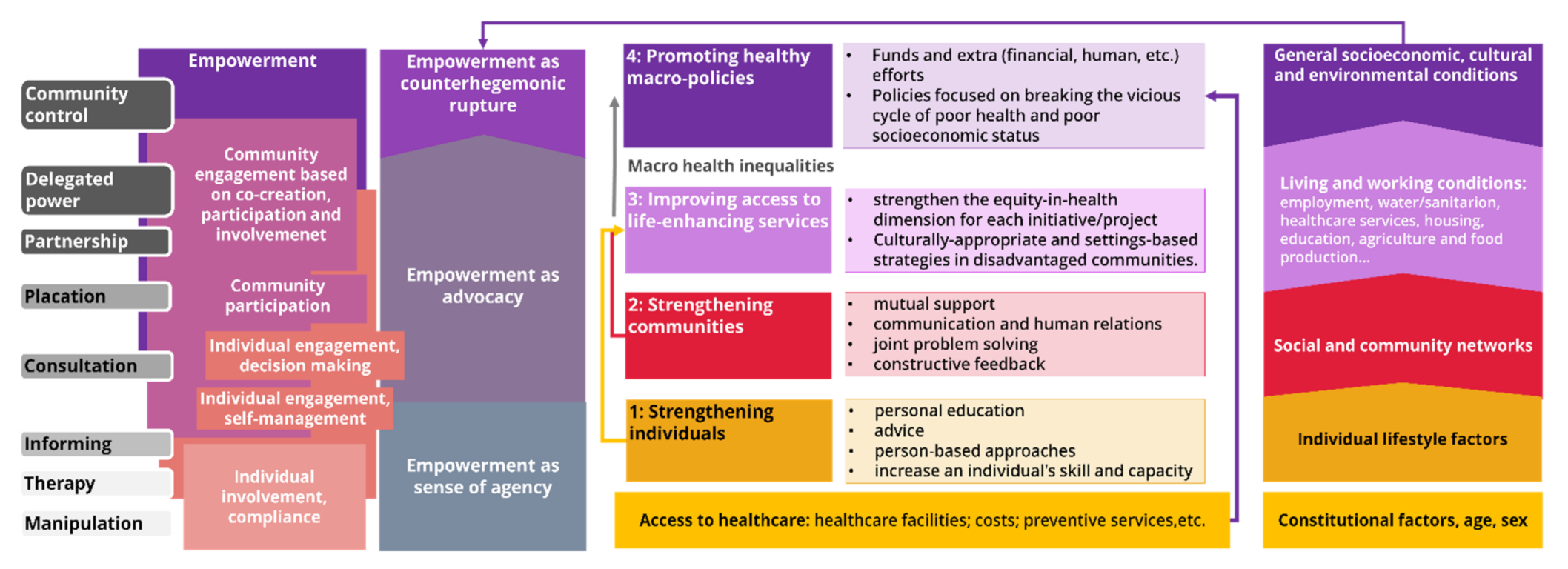
This study identified several facilitators and barriers when promoting engagement and co-production of vulnerable communities to participate in health research and innovation. Since this study targeted the academic community, the Community-Engaged Dissemination and Implementation (CEDI) framework of domains and competencies [41] was also integrated within the discussion and, most importantly, in the generation of models. Besides, the social determinants of health, as characterised by Dahlgren and Whitehead [16,42], for researching and intervening in the community [42] were taken into account. The consideration of social determinants of health determines a typology and process for tackling social inequalities in health research, care and innovation [28]. Concerning participation, the classic Ladder of Citizen Participation [43] also is integrated jointly with more modern approaches for planning and executing patients and public engagement. Appendix A (Figure A1). Graphically shows the relations between ladders of participation [43], community engagement, empowerment, and typologies of health research and health interventions in light of health disparities [16,42].
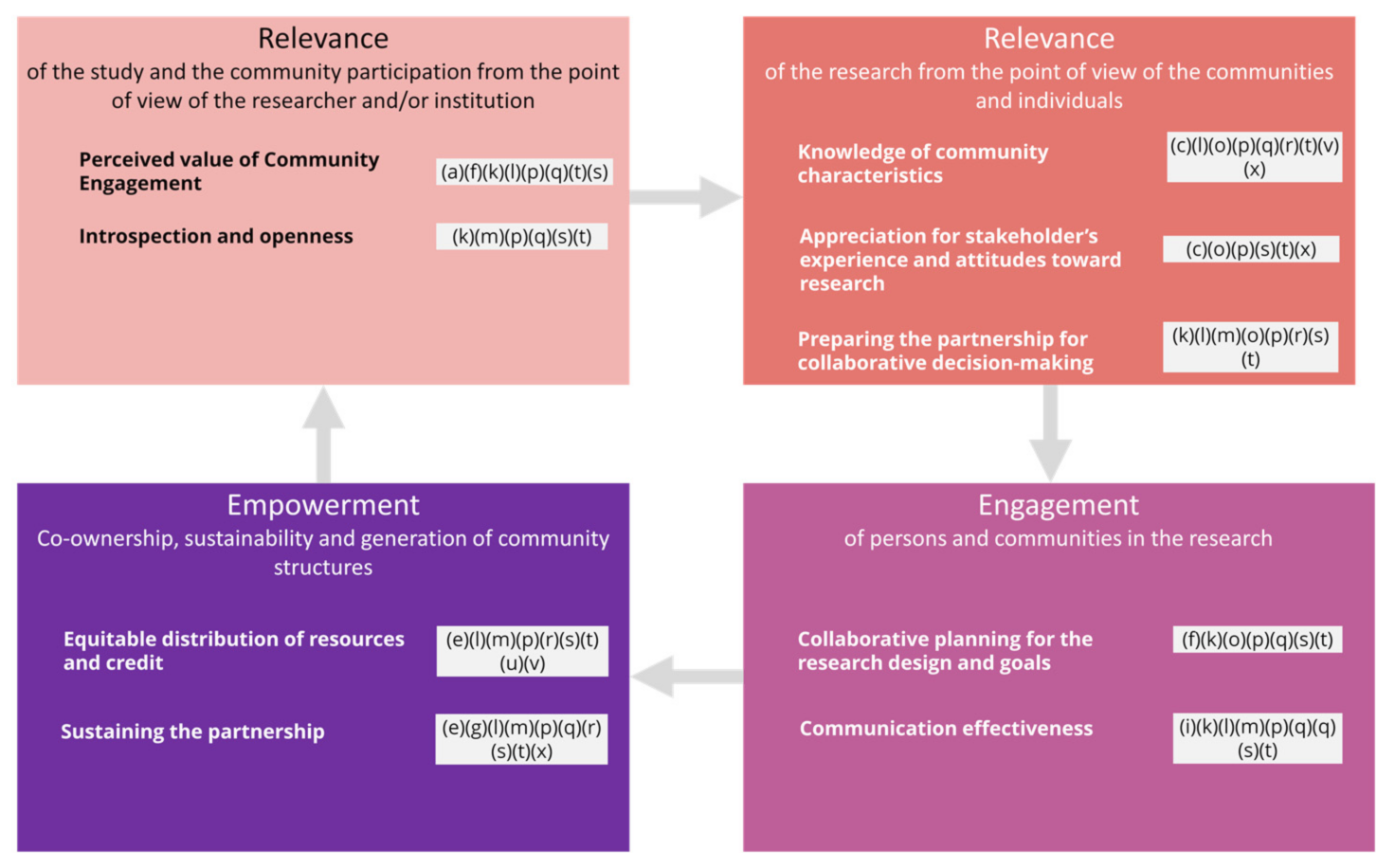
A summary of this meta-synthesis and of the themes that have emerged is presented, aligned with the CEDI model, as well as the main topics of this study: engagement and empowerment through person-centred health research, innovation, and co-production (Figure 2). In particular, nine domains divided into 40 competencies comprised the CEDI model. These domains were reinterpreted within the most important constructs of this research: relevance (affecting the design and the recruitment and considered from the perspectives of researchers and the views from the communities–five domains), engagement (of communities and/or persons–two domains), and empowerment (which mostly involves co-production with the communities–two domains). Our findings as coded from the papers analysed were discussed accordingly (see Figure 2).
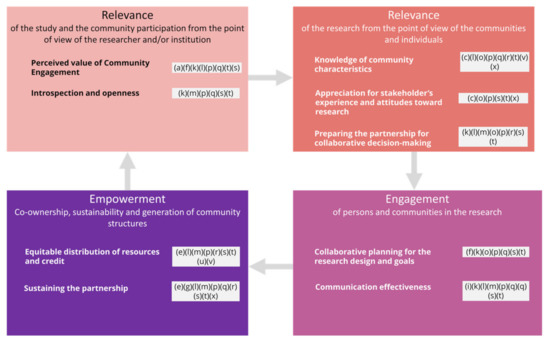
Figure 2.
Results discussed in light of the CEDI model.
Firstly, concerning the first CEDI domain; i.e., the researchers’ attitude towards the community engagement role in research, the analysis revealed the importance of showing sincere concern and interest in the community (p), with an open-minded, interested, and listening attitude shown by the research team (p). Non-participative traditional approaches are still sustained by the academic and healthcare entities involved in research and innovation. Usually, the process of participation is understood as a process of delivering information and then consultation [44], rather than establishing a more profound relationship and engaging in co-production processes. Sometimes, researchers may want too much control without considering the community organisations as co-owners, leading to reluctancy and making it more difficult to reach these traditionally reluctant communities (p). In addition, technocratic approaches and tokenism are barriers to researching the community, even for recruiting persons [44], as seen in (a)(f)(k)(l)(p)(q)(t), since these approaches represent a negative attitude concerning their capacities and/or skills to actively contribute to health research. The extensive training in quantitative analysis and manuscript writing skills dedicated to community members may be a barrier to the implementation of participatory processes in research [45]. In parallel, the researchers’ perception of lack of rigour (j)(k)(l)(p) or lack of neutrality (p)(q)(s) in co-production processes were also identified as barriers for engaging communities in research.
Secondly, the introspection and openness of the researcher—and thus their ability to examine their preconceptions, self-reflection about their own cultural backgrounds, and pre-conceived notions about communities—while practising cultural humility was also found in this meta-synthesis. Community contributors and individuals may struggle in the research and how it potentially contributes to a further stereotyping or marginalisation (p) or even exploitation (t). The marginalisation of experiential knowledge sustained by the participants and community members sustained in the power imbalance must be considered (k)(p)(t). Conflicting realities between communities, even cultures, may arise that also are related to the requirements and duties of all parties involved (m). For instance, communities might not understand the scientific ‘rhythms’ (m), or culturally and linguistically diverse groups would prefer to engage with a researcher from their own community (o). Structural determinants should be integrated within the research and clinical knowledge, practices, and analysis to avoid revictimization, discrimination, and stigmas. In addition, the ‘cultural trauma’ could be addressed: analysis should be periodically conducted through multi-disciplinary meetings; the research and clinical staff should be committed and aware of these structural determinants; and the wider community needs to be involved [46]. During the research design phase, the active involvement of individuals and communities led to more relevant objectives and person-centred care, integrated solutions, or, at smaller scales, user-friendly and understandable information, culturally-tailored interactions, or a richer interpretation of data; it may also enhance the dissemination of results [19].
Third, the knowledge of the community is crucial. The relationship with the community and the cultural awareness of the research team are also key elements (q)(s). The participation of a vast range of actors, a real power-sharing collaboration in co-production and partnership, bidirectional learning, inclusion within the research protocol, and intercultural competency, especially for underserved populations [47]. The role of patients and stakeholders seems to be critical for identifying patient-centred research agendas, priorities, inputs on research design, and strategies for increasing the participation and retention in trials [48].
When approaching hard-to-reach, hidden, or disengaged populations, mistrust appears (p)(v). Researchers may need access to a very specific sample through community leaders, who might be fearful of the consequences that giving access may have. There are not universally adopted strategies for recruiting. Most of them are focused on engendering patients and focused on individuals, while researchers working with minorities highlight the importance of involving the community as a whole [49]
The level of communitarian disengagement appears in (c)(o)(p)(r)(t)(v)(x). To overcome these difficulties, a collaborative reflection embracing a sense of team ethos and community cohesion is required [5]. However, even when designing and executing a flawless protocol for ensuring co-production and community empowerment, to conduct participatory research does not lead to equal participation and cannot break the power imbalance between community members [19]. Participatory research and, specifically, CBPR is effective: (i) in increasing the participation of racial and ethnic minority subjects in research. It also showed to be a powerful tool for diminishing health disparities, determined by the involvement and the degree of engagement by communities; and (ii) for validating effective interventions among under-represented populations [45].
It is crucial to determine how to keep persons motivated to raise retention and engagement. Motivations should be based on advocacy (q). However, there is a lack of standard reporting guidelines and guidance regarding engagement of stakeholders and patients, as well as information on how to identify and recruit participants [48].
The disconnection between the community and the research entity (m)(p) must be prevented for an effective co-production process, and this is particularly important regarding transparency (p)(t). This disconnection might be produced because researchers or institutions are ‘outside of the orbit’ of the community, or if a new programme derived from the research is introduced into the quotidian practice of community workers and community boards (p), among other reasons. The recruitment of participants conducted by community members and leaders increases the recruitment rates and the retainment during the participatory research process [45].
Researchers must be willing to share knowledge with the community to learn about the community and the stakeholders involved, mapping representativeness, leaders, relationships, historical events, power dynamics, or customs to perform a realistic needs assessment focused on them and their priorities [44,45,50,51]. This appeared in (l)(p)(q). To know the community by showing real interest is key before selecting which means would work [13]: for instance, knowledge sharing activities with the communities are critical to ensure a truly participatory approach [45,51]. The role of patients and stakeholders seems to be critical for identifying patient-centred research agendas, priorities, and inputs on research design and strategies for increasing the participation and retention in trials [48]. Well-balanced and equalitarian partnerships in research involve users in all stages and focus on experiential knowledge and mutual learning, with openness and respectful attitudes from both sides [52]. Community empowerment may consist of skill-building, priority setting, action plans’ strategical design and implementation, evaluation, managing budgets or raising funds, or making local management decisions [50].
At the individual level, to directly appeal to patients’ empowerment or participatory methods and co-creation frameworks would help to maximise the recruitment (q)(v).
Fourthly, the appreciation of the communities and individuals’ experiences is essential. The fear of further marginalisation appeared in (o)(p)(t), and trust of community key stakeholders and leaders was emphasised in (p)(s)(x)(c). In this concern, negative previous experiences in research have an impact on their attitudes, and therefore in their involvement in research processes (p)(t)(x).
The fifth domain is to prepare the researchers–community partnership for a collaborative effort, thereby facilitating dialogue, coordination, and decision making. To integrate the formal and informal processes in the community for decision-making, collaboratively outlining the priorities and obtaining the commitment of organisations and leaders for the co-production process is crucial. These factors were mentioned in (r)(s)(t). Researchers should share results while focusing on contextual issues and avoiding re-stigmatisation of service users (p)(x). Both communities and patients need to be heard, valued, and seen (u). In the case of disengaged and highly stigmatised communities, two additional factors are essential for conducting ethical and safe research: (i) to build rapport; and (ii) to consolidate meaningful and safe relationships with the research team (c). A broad range of parties involved is required, including, but not restricted to, community leaders, advocates, community health workers, individuals, health professionals, public administration officers, and service users (e.g., patients). These groups should be carefully defined before designing the strategy for disseminating and implementing the co-production processes [20,22,47]. Activities for sustaining the community engagement should be demarcated as well, and these should include plans far beyond the mere passive receptiveness of information. It is also crucial to share results and provide relevant outcomes, considering their practical application or their potential for generating new resources in the community studied (g)(p)(x).
The multi-stakeholder approach (l), the need for putting in place formal agreements (m), to raise the potential for dialogue and shifting thinking in all parties involved (e), and collaborative efforts and transparency (m) were confirmed as facilitators of the recruitment in this meta-synthesis. Research showed that the motivation and disposition of community members to take part and engage in participatory processes were personal and professional growth, recognition and respect, sense of ownership and sense of confidence, development of leadership skills, knowledge acquisition, concurrence with prevalent cultural norms, appropriateness of the participatory process with local environment and needs, and perceived or experienced beneficial outcomes [50].
The co-production can minimise the power imbalances between researchers, communities, and institutions [44,48,50], as shown in (p)(r)(s)(t). The engagement and outcomes related to participation seemed to be greater for researchers willing to conduct their studies under a multi-disciplinary approach (s). This implied sharing results as soon as possible with community members (p)(r)(t) and providing ownership to communities themselves (r)(t).
All these factors under the fifth domain were also related to the sixth domain, which is the collaborative planning for the research design and goals. The involvement of the populations in the design phase [44,48] since the early beginning (l)(p)(q), as well as the importance of a jointly defined research agenda, were key facilitators (k)(o)(p)(f).
Seventh, the communication effectiveness is related to a clear presentation of ideas, listening attitude, and culturally sensitive and plain language. Our research showed the importance of the information being specifically prepared for the community, culturally tailored, from the design phase (l)(m)(q)(s)(t), using adequate terms (g)(p)(q); and how unclear information (t), jargon (q), or language barriers are problematic in these participative research processes. In sum, communication problems appeared as major barriers for researching involving vulnerable persons (i)(k)(l)(p)(q). Thus, sensitive communication when addressing the problems faced by participants and/or by communities is needed: communication problems in this regard arose as an important barrier [44].
The eighth factor is the equitable distribution of resources and credit, including financial resources, resource distribution, and role in media coverage and scientific publications. Planning how to share results (p)(r)(t) and provide ownership (l)(r)(s)(t)(u)(v) appeared. In addition, budget and resources were mentioned (r)(e), as well as financial transparency (m). In this regard, it is worth mentioning that collection, interpretation, and exchange and co-ownership of data are very complex issues that could be discussed in terms of the consequences of these processes for the groups themselves. Data gathering may be detrimental to deprived or marginalised communities. Besides, the indicators may be culturally inadequate, the stakeholders may be under-represented or disregarded, and the results are sometimes inaccessible for them [15,27].
Lastly, the ninth domain is the long-term relationship, sustaining the partnership and integrating the capacity building, the long-term funding, the self-sustainability of research and healthcare innovation projects and programmes, and the commitment of devoting time and efforts to addressing stakeholder needs beyond the research [52]. Long-term financial and organisational support (l)(p) appeared jointly with results sharing (q)(s)(t). Both factors seem to be linked to the dependency on funds by patient organisations (l) and the lack of long-term engagement of researchers perceived by the community (m). Organisational commitment and policies, budget, resources, time, and training (r)(e) are important for preventing a negative sense of exploitation (p)(t)(x) or abandonment (o). To overcome these difficulties and perceptions, structures to sustain the communities’ empowerment in the long-term could be provided (g)(p)(x) while also considering the sharing of resources (p)(t) and raising policies and organisational commitment for ensuring the persons’ participation (r)(e).
The goal of our study was to provide sound knowledge for research into person-centred care by empowering deprived communities to be part of research and innovation in health and social care. To achieve this empowerment, we must integrate the lessons learned and the findings exposed in these results, as well as the ladders of participation [43] and the typology of actions on health inequalities [42].
3.3.1. Implications for Practice
The implementation of co-production methods during the entire research process could offer a more tailored process and a more successful recruitment, raising the recruitment and retainment of traditionally disengaged communities. It is needed to engage participants, advocacy entities, and groups in the long term.
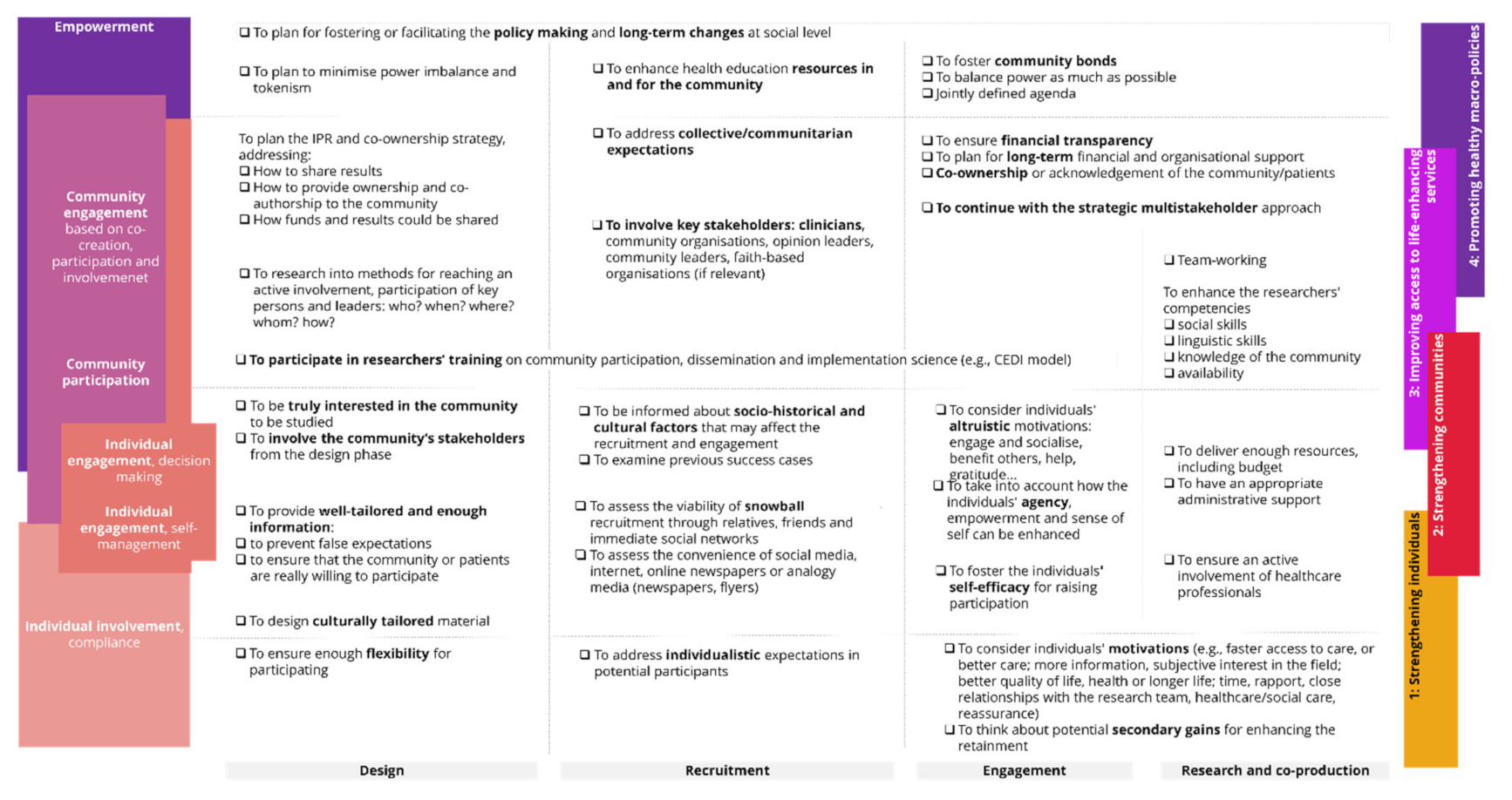
The checklist in Figure 3 summarises our findings translated into best practices, divided into the phases of the design and execution of a person-centred co-production.
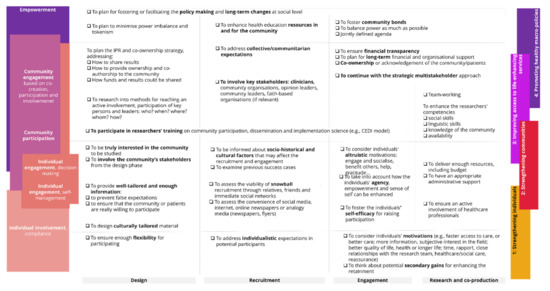
Figure 3.
Checklist to promote community empowerment and individuals′ engagement in research for person-centred care.
The role of the research and the co-production for studied communities depends on their capacity to produce a real and long-term change that translates into meaningful empowerment of persons and communities, therefore paving the way to more efficient person-centred care. There are some important considerations when fostering person-centred care through the engagement and empowerment of individuals and communities.
On the one hand, at the individual level, to offer flexibility and to foster self-efficacy to ensure safety and confidentiality are key aspects. During the co-production, to engage participants, raise their confidence, adapt terms, and overcome the tokenism are essential to empowering vulnerable persons. Likewise, to prepare appropriate information addressed at individuals and communities to be involved, founded on a sound knowledge of the community, is needed. On the other hand, at the community level, it is required to consider the disengagement, the need for structures, and long-term alliances to empower communities at practical and real levels. Vital factors include tackling the power imbalance during the early stages, involving health professionals and key stakeholders during the execution of co-creation processes, and building trust. Trust and acknowledgement of community contributors are decisive during the design and recruitment stages, as well as during the execution phases. The acknowledgement of their contributions, even co-ownership (whenever possible or pertinent), should be considered.
3.3.2. Limitations and Strengths
The great amount of literature reviewed, together with the qualitative perspective selected to analyse the discourse of key persons involved in the research, constituted a strength of the current research. Qualitative research allowed us to obtain a vast range of information about the participants’ perspectives, solutions proposed, assumptions, beliefs, strengths, and structural problems in their own terms, which is crucial for designing well-tailored interventions attending to the targeted audiences’ narratives. Likewise, the integrative perspective and the focus on the individuals’ agency and the community empowerment for focusing the engagement was a meaningful strength of our study. The innovative methodology for analysing a vast amount of data through the integration of grounded theory principles were used, although the general structure was a meta-synthesis due to the huge number of papers and dissertations (102 in total; 23 of them were included in this study) included in the general dissertation. The innovative approach allowed us not to lose important information by: (i) facilitating the extraction of key thematic areas arising from the information; and (ii) not attaching to a single framework (e.g., the CEDI) delimiting the codes and the analysis of the information, but facilitating the comparison and the analysis with the literature.
The study also had some limitations that relied on the non-exhaustiveness of the literature sample included. As a matter of fact, this research was a part of a larger meta-synthesis not entirely focused on research and co-production, but strongly linked to these topics. Conversely, the ‘partial’ nature ensured its integration into a wider frame, joining key themes on health communication and patient and community participation: decision making, self-management of health, or counselling were jointly treated in a comprehensive viewpoint, which supposed a great added value in terms of integrative perspectives able to inform practice.
Further research will be conducted on the prioritisation of factors and on the validation of the checklist and best practices extracted. The outputs will be tested in real research settings through qualitative research to validate and prioritise those that would be specifically needed for person-centred care. The research results will be disseminated to health and social care professional and workers in plain language.
4. Conclusions
This qualitative study reviewed and showed the experiences of researchers, patients, and communities, as well as other relevant stakeholders, such as public administration officers. The knowledge captured in these experiences allowed us to identify facilitators and barriers, as well as provide best practices for conducting a culturally tailored and empowering co-production in research and healthcare innovation. Three challenges were addressed in the study design: (i) how to raise the recruitment of the disengaged; (ii) the potential for empowering persons and communities through research and/or co-production; and (iii) the engagement of deprived and disengaged groups in light of the social determinants of health. The co-production during all research phases offered a well-tailored process, and successful recruitment of participants and key stakeholders. The safety of the participants, the confidentiality of the information, and the awareness of power imbalances—both between researchers and communities and among participants—during the research was critical from the point of view of the effectiveness, engagement, and ethics of the study during its entire lifecycle. When designing innovation and/or interventions involving vulnerable communities, socio-economic and cultural settings and systemic co-determinants should be integrated within the co-production process. Collective empowerment depends on the access to basic services (among others, healthcare) and the material circumstances, equitable societal structures (policies, budget and funds, and approach and focus of the measures undertaken by decision makers), and structural determinants (again, socio-economic, cultural, and environmental conditions co-determining health inequalities at a macro level). Co-production processes could be approached for raising the individuals′ self-efficacy, skills, and access to services; the advocacy capacities of the community and civil society players; and for supporting long-term changes and promoting healthier policies able to change current vicious cycles of poverty and poor health outcomes. To collaborate with communities and to sustain or, at least, not interfere in the creation of sustainable structures and bonds will result in meaningful empowerment and an enhanced sense of agency of all participants.
Author Contributions
All authors actively contributed to the present research paper: B.V.A. was the principal researcher, supported in the design and the revision of the papers included by E.D.F. and M.F.G. M.F.S. actively collaborated in the extraction of conclusions and the synthesis of the research. Both E.D.F. and M.F.S. contributed to revising the style and readiness of the research article. All authors have read and agreed to the published version of the manuscript.
Funding
These results are part of wider research supported by the regional government through the Valencia Agency of Innovation (AVI) under grant INNTAL31/19/001, project COMSALUD (estrategias de alto impacto en COMunicación de la SALUD e implementación de proyectos socio-sanitarios con grupos psicosocialmente vulnerables—High-impact strategies in health communication and in implementing socially relevant health interventions with psycho-social vulnerable groups).
Institutional Review Board Statement
This research was a review article and did not involve human and/or animal subjects. The study was conducted ethically and responsibly in full compliance with the eligible standards of integrity and relevance of the research and, specifically for review works, acknowledgement of all primary sources consulted and revised.
Informed Consent Statement
Not applicable.
Data Availability Statement
Concerning availability of data, all tables with excerpts and verbatim quotations extracted from studies sampled are available as complementary materials at https://roderic.uv.es/handle/10550/77735, accessed on 22 November 2021, deposited in the Institutional Repository of the University of Valencia Roderic (roderic.uv.es, accessed on the 22 November 2021).
Acknowledgments
The present study was supported by the company Senior Europa S.L.–Kveloce I + D + i and its entire staff, including the administrative and technical personnel and their contribution to the research and innovation activities within the company. The authors also acknowledge and recognize the work and effort devoted by the director of the present Ph.D. dissertation, Jorge Garcés Ferrer.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A. The Relation between Ladders of Participation, Typology of Intervention and Research, Social Determinants of Health, Engagement, and Empowerment
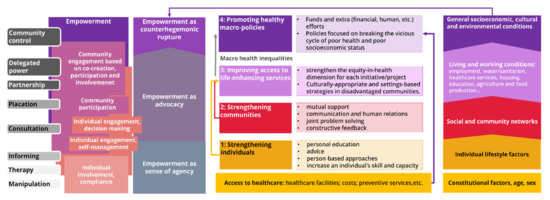
Figure A1.
Scheme reflecting the relation between the ladders of participation, the typology of the intervention and the social determinants of health in light of the communities’ engagement and empowerment. Prepared by the authors based on [16,42,43].
Figure A1.
Scheme reflecting the relation between the ladders of participation, the typology of the intervention and the social determinants of health in light of the communities’ engagement and empowerment. Prepared by the authors based on [16,42,43].
Appendix B. Studies Included in the Sample
- Greenhalgh T, Hinder S, Stramer K, Bratan T, Russell J. Adoption, non-adoption, and abandonment of a personal electronic health record: case study of HealthSpace. BMJ [Internet]. 2010;341(7782):1091.
- Caine V, Mill J, O’Brien K, Solomon P, Worthington C, Dykeman M, et al. Implementation Process of a Canadian Community-based Nurse Mentorship Intervention in HIV Care. Journal of the Association of Nurses in AIDS Care [Internet]. 2016;27(3):274–84. Available from: https://doi.org/10.1016/j.jana.2015.11.001.
- Goldenberg SM, Brouwer KC, Jimenez TR, Miranda SM, Mindt MR. Enhancing the ethical conduct of HIV research with migrant sex workers: Human rights, policy, and social contextual influences. PLoS ONE [Internet]. 2016;11(5):e0155048. Available from: https://doi.org/10.1371/journal.pone.0155048.
- Nota I, ssaert CHC, Taal E, van de Laar MAFJ. Arthritis patients’ motives for (not) wanting to be involved in medical decision-making and the factors that hinder or promote patient involvement. Clinical rheumatology [Internet]. 2016 2014;35(5):1225–35. Available from: https://dx.doi.org/10.1007/s10067-014-2820-y.
- Rivas C, Taylor S, Abbott S, Clarke A, Griffiths C, Roberts CM, et al. Perceptions of changes in practice following peer review in the National Chronic Obstructive Pulmonary Disease Resources and Outcomes Project. International journal of health care quality assurance [Internet]. 2012;25(2):91–105. Available from: https:///doi.org/10.1108/09526861211198263/full/html.
- Bess KD, Prilleltensky I, Perkins DD, Collins LV. Participatory Organizational Change in Community-Based Health and Human Services: From Tokenism to Political Engagement. American Journal of Community Psychology [Internet]. 2009;43(1):134–48. Available from: https://doi.org/10.1007/s10464-008-9222-8.
- Ekundayo OT, Tataw DB. Prostate cancer risk factors, care utilization and policy options. Focus group findings from an engagement with an African American urban community. American Journal of Health Studies [Internet]. 2012;27(1):32. Available from: https://www.researchgate.net/publication/237091071_PROSTATE_CANCER_RISK_FACTORS_CARE_UTILIZATION_AND_POLICY_OPTIONS_FOCUS_GROUP_FINDINGS_FROM_AN_ENGAGEMENT_WITH_AN_AFRICAN_AMERICAN_URBAN_COMMUNITY.
- Locock L, Smith L. Personal benefit, or benefiting others? Deciding whether to take part in clinical trials. Clinical Trials [Internet]. 2011;8(1):85–93. Available from: https://doi.org/10.1177/1740774510392257.
- Cook C. Email interviewing: generating data with a vulnerable population. Journal of advanced nursing [Internet]. 2012;68(6):1330–9. Available from: https://doi.org/10.1111/j.1365-2648.2011.05843.x.
- Carlisle K, Farmer J, Taylor J, Larkins S, Evans R. Evaluating community participation: A comparison of participatory approaches in the planning and implementation of new primary health-care services in northern Australia. The International Journal of Health Planning and Management [Internet]. 2018 [cited 2018 Apr 20];0(0). Available from: https://doi.org/10.1002/hpm.2523.
- Brooks F. Nursing and public participation in health: An ethnographic study of a patient council. International journal of nursing studies [Internet]. 2008;45(1):3–13. Available from: https://doi.org/10.1016/j.ijnurstu.2006.08.012.
- de Wit MPT, Abma TA, Loon MK, Collins S, Kirwan J. Facilitating and inhibiting factors for long-term involvement of patients at outcome conferences–lessons learnt from a decade of collaboration in OMERACT: a qualitative study. BMJ Open [Internet]. 2013;3(8):e003311. Available from: https://doi.org/10.1136/bmjopen-2013-003311.
- Kraemer Diaz AE, Spears Johnson CR, Arcury TA. Perceptions That Influence the Maintenance of Scientific Integrity in Community-Based Participatory Research. Health Educ Behav [Internet]. 2015 Jun [cited 2019 Oct 31];42(3):393–401. Available from: https://doi.org/10.1177/1090198114560016.
- Holmberg C, Whitehouse K, Daly M, McCaskill-Stevens W. Gaining control over breast cancer risk: Transforming vulnerability, uncertainty, and the future through clinical trial participation–a qualitative study. Sociology of health & illness [Internet]. 2015;37(8):1373–87. Available from: https://doi.org/10.1111/1467-9566.12307.
- Bailey KC, DeGrace BW, Arnold S. Partnering to understand: An investigation of health disparity in the communities surrounding a university health sciences center. Journal of allied health [Internet]. 2014;43(1):3–11. Available from: https://pubmed.ncbi.nlm.nih.gov/24598894/.
- Pinto RM. Community Perspectives on Factors That Influence Collaboration in Public Health Research. Health Education & Behavior [Internet]. 2009;36(5):930–47. Available from: https://doi.org/10.1177/1090198108328328.
- Buck D, Gamble C, Dudley L, Preston J, Hanley B, Williamson PR, et al. From plans to actions in patient and public involvement: Qualitative study of documented plans and the accounts of researchers and patients sampled from a cohort of clinical trials. BMJ Open [Internet]. 2014;4(12):e006400. Available from: https://doi.org/10.1136/bmjopen-2014-006400.
- Robinson N, Lorenc A. ‘No one wants to be the face of Herpes London’: a qualitative study of the challenges of engaging patients and the public in sexual and reproductive health and HIV/AIDS services. Health Expect [Internet]. 2015 Apr [cited 2019 Oct 31];18(2):221–32. Available from: https://doi.org/10.1111/hex.12024.
- Abma TA, Pittens CACM, Visse M, Elberse JE, Broerse JEW. Patient involvement in research programming and implementation. Health Expectations [Internet]. 2015;18(6):2449–64. Available from: https://doi.org/10.1111/hex.12213.
- Safo S, Cunningham C, Beckman A, Haughton L, Starrels JL. ‘A place at the table:’ a qualitative analysis of community board members’ experiences with academic HIV/AIDS research. BMC medical research methodology [Internet]. 2016;16:80. Available from: https://doi.org/10.1186/s12874-016-0181-8.
- Rise MB, Solbjør M, Lara MC, Westerlund H, Grimstad H, Steinsbekk A. Same description, different values. How service users and providers define patient and public involvement in health care. Health Expectations [Internet]. 2013;16(3):266–76. Available from: https://doi.org/10.1111/j.1369-7625.2011.00713.x.
- James DCS, Harville C, Efunbumi O, Babazadeh I, Ali S. “You Have to Approach Us Right”: A Qualitative Framework Analysis for Recruiting African Americans Into mHealth Research. Health Education & Behavior [Internet]. 2017;44(5):781–90. Available from: https://doi.org/10.1177/1090198117727324.
- Young C, Tong A, Sherriff S, Kalucy D, Fernando P, Muthayya S, et al. Building better research partnerships by understanding how Aboriginal health communities perceive and use data: a semistructured interview study. BMJ OPEN [Internet]. 2016;6(4):e010792. Available from: https://doi.org/10.1136/bmjopen-2015-010792.
References
- Kuhlicke, C.; Scolobig, A.; Tapsell, S.; Steinführer, A.; Marchi, B.D. Contextualizing social vulnerability: Findings from case studies across Europe. Nat. Hazards 2011, 58, 789–810. [Google Scholar] [CrossRef]
- Smith, K.R.; Woodward, A.; Campbell-Lendrum, D.; Chadee, D.D.; Honda, Y.; Liu, Q.; Olwoch, J.M.; Revich, B.; Sauerborn, R. Chapter 11. Human health: Impacts, Adaptation, and Co-Benefits. In Climate Change 2014: Impacts, Adaptation, and Vulnerability. Part A: Global and Sectoral Aspects; Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; Field, C.B., Barros, V.R., Dokken, D.J., Mach, K.J., Mastrandrea, M.D., Bilir, T.E., Chatterjee, M., Ebi, K.L., Estrada, Y.O., Genova, R.C., et al., Eds.; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2014. [Google Scholar] [CrossRef] [Green Version]
- Delea, S.; Buckley, C.; Hanrahan, A.; McGreal, G.; Desmond, D.; McHugh, S. Management of diabetic foot disease and amputation in the Irish health system: A qualitative study of patients’ attitudes and experiences with health services. BMC Health Serv. Res. 2015, 15, 251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, J.; Bukulatjpi, S.; Sharma, S.; Davis, J.; Johnston, V. “Only your blood can tell the story”—A qualitative research study using semi-structured interviews to explore the hepatitis B related knowledge, perceptions and experiences of remote dwelling Indigenous Australians and their health care providers in northern Australia. BMC Public Health 2014, 14, 1233. [Google Scholar] [CrossRef]
- DiGiacomo, M.; Green, A.; Rodrigues, E.; Mulligan, K.; Davidson, P.M. Developing a gender-based approach to chronic conditions and women’s health: A qualitative investigation of community-dwelling women and service provider perspectives. BMC Womens Health 2015, 15, 105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gien, L.; Porr, C.; Parsons, K.; John’s, S.; Allison, J. Challenges in Self-Management of type 2 Diabetes Mellitus (T2DM) in a Rural Community of Eastern Canada. Perspectives 2017, 39, 6–15. Available online: https://www.proquest.com/openview/b4e689a558dd37e78a117b7eb3b315f7/1?pq-origsite=gscholar&cbl=2026736 (accessed on 22 November 2021).
- Chrisler, J.C.; Barney, A.; Palatino, B. Ageism can be Hazardous to Women’s Health: Ageism, Sexism, and Stereotypes of Older Women in the Healthcare System. J. Soc. Issues 2016, 72, 86–104. [Google Scholar] [CrossRef]
- Schroyen, S.; Adam, S.; Marquet, M.; Jerusalem, G.; Thiel, S.; Giraudet, A.-L.; Missotten, P. Communication of healthcare professionals: Is there ageism? Eur. J. Cancer Care 2018, 27, e12780. [Google Scholar] [CrossRef]
- Nario-Redmond, M.R.; Kemerling, A.A.; Silverman, A. Hostile, Benevolent, and Ambivalent Ableism: Contemporary Manifestations. J. Soc. Issues 2019, 75, 726–756. [Google Scholar] [CrossRef] [Green Version]
- Cortina Orts, A. Aporofobia, el Rechazo al Pobre: Un Desafío para la Democracia, 1st ed.; Ediciones Paidós: Barcelona, Spain, 2017; p. 196. [Google Scholar]
- Cooper, B. Intersectionality. In The Oxford Handbook of Feminist Theory; Oxford University Press: Oxford, UK, 2016. [Google Scholar] [CrossRef]
- Crenshaw, K. On Intersectionality: Essential Writings; New Press: New York, NY, USA, 2019. [Google Scholar]
- Shaghaghi, A.; Bhopal, R.S.; Sheikh, A. Approaches to Recruiting ‘Hard-To-Reach’ Populations into Research: A Review of the Literature. Health Promot. Perspect. 2011, 1, 86–94. [Google Scholar] [CrossRef]
- Gemmill, R.; Williams, A.C.; Cooke, L.; Grant, M. Challenges and strategies for recruitment and retention of vulnerable research participants: Promoting the benefits of participation. Appl. Nurs. Res. 2012, 25, 101–107. [Google Scholar] [CrossRef] [Green Version]
- O’Campo, P.; Dunn, J.R. (Eds.) Rethinking Social Epidemiology: Towards a Science of Change; Springer: Dordrecht, The Netherlands, 2012. [Google Scholar] [CrossRef]
- Dahlgren, G.; Whitehead, M. European Strategies for Tackling Social Inequities in Health: Levelling Up Part 2; WHO Regional Office for Europe: Copenhagen, Denmark, 2007; p. 149. Available online: http://www.euro.who.int/__data/assets/pdf_file/0018/103824/E89384.pdf (accessed on 22 November 2021).
- Holt, C.L.; Chambers, D.A. Opportunities and challenges in conducting community-engaged dissemination/implementation research. Transl. Behav. Med. 2017, 7, 389–392. [Google Scholar] [CrossRef] [Green Version]
- Lawrence, M.; Kinn, S. Defining and measuring patient-centred care: An example from a mixed-methods systematic review of the stroke literature. Health Expect. 2012, 15, 295–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brett, J.; Staniszewska, S.; Mockford, C.; Herron-Marx, S.; Hughes, J.; Tysall, C.; Suleman, R. Mapping the impact of patient and public involvement on health and social care research: A systematic review. Health Expect. 2014, 17, 637–650. [Google Scholar] [CrossRef]
- Tiwari, R.; Stephens, J.; Hooper, R. Mission rehabilitation—A community-centric approach to Aboriginal healing. Australian Aborig. Stud. 2019, 2, 19–33. Available online: https://www.researchgate.net/publication/337829607_Mission_rehabilitation_-_a_community-centric_approach_to_Aboriginal_healing_-_Tiwari_Stephens_Hooper (accessed on 22 November 2021).
- Ivory, V.; O’Donnell, K.; McFarlane, P. Enhancing liveability through community-centric approaches to asset management and affordable digital tools. In Proceedings of the WEC2019: World Engineers Convention 2019, Melbourne, Australia, 20–22 November 2019; ISBN 9781925627251. [Google Scholar]
- Rendalls, S.; Spigelman, A.D.; Goodwin, C.; Daniel, N. Health service engagement with consumers and community in Australia for issue: Engagement and accountability with your community. Int. J. Health Gov. 2019, 24, 274–283. [Google Scholar] [CrossRef]
- Vaismoradi, M.; Jordan, S.; Kangasniemi, M. Patient participation in patient safety and nursing input—A systematic review. J. Clin. Nurs. 2015, 24, 627–639. [Google Scholar] [CrossRef] [Green Version]
- Flournoy, M.W. Organizational Barriers to and Facilitators of Patient Engagement Processes for Persons Living with HIV/AIDS: A Case Study Analysis of an Oral Health Services Program. Ph.D. Thesis, University of South Carolina, Columbia, SC, USA, 2011. Available online: https://search.proquest.com/docview/921496802?pq-origsite=summon (accessed on 22 November 2021).
- Hanson, H.M.; Salmoni, A.W.; Volpe, R. Defining Program Sustainability: Differing Views of Stakeholders. Can. J. Public Health 2009, 100, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Griffin, G. Empowerment. In A Dictionary of Gender Studies; Oxford University Press: Oxford, UK, 2017; Available online: https://www.oxfordreference.com/view/10.1093/acref/9780191834837.001.0001/acref-9780191834837-e-104 (accessed on 22 November 2021).
- Small, N.; Bower, P.; Chew-Graham, C.A.; Whalley, D.; Protheroe, J. Patient empowerment in long-term conditions: Development and preliminary testing of a new measure. BMC Health Serv. Res. 2013, 13, 263. [Google Scholar] [CrossRef] [Green Version]
- Edwards, M.; Davies, M.; Edwards, A. What are the external influences on information exchange and shared decision-making in healthcare consultations: A meta-synthesis of the literature. Patient Educ. Couns. 2009, 75, 37–52. [Google Scholar] [CrossRef]
- Noblit, G.W.; Hare, R.D. Chapter 5: Meta-Ethnography: Synthesizing Qualitative Studies. Counterpoints 1999, 44, 93–123. [Google Scholar]
- Sandelowski, M.; Docherty, S.; Emden, C. Qualitative metasynthesis: Issues and techniques. Res. Nurs. Health 1997, 20, 365–371. [Google Scholar] [CrossRef]
- Bondas, T.; Hall, E.O.C. Challenges in Approaching Metasynthesis Research. Qual. Health Res. 2007, 17, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Sword, W.; Jack, S.; Niccols, A.; Milligan, K.; Henderson, J.; Thabane, L. Integrated programs for women with substance use issues and their children: A qualitative meta-synthesis of processes and outcomes. Harm Reduct. J. 2009, 6, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devereux-Fitzgerald, A.; Powell, R.; Dewhurst, A.; French, D.P. The acceptability of physical activity interventions to older adults: A systematic review and meta-synthesis. Soc. Sci. Med. 2016, 158, 14–23. [Google Scholar] [CrossRef]
- McCormack, B.; Karlsson, B.; Dewing, J.; Lerdal, A. Exploring person-centredness: A qualitative meta-synthesis of four studies. Scand. J. Caring Sci. 2010, 24, 620–634. [Google Scholar] [CrossRef]
- Rivas, C.; Matheson, L.; Nayoan, J.; Glaser, A.; Gavin, A.; Wright, P.; Wagland, R.; Watson, E. Ethnicity and the prostate cancer experience: A qualitative metasynthesis. Psycho-Oncology 2016, 25, 1147–1156. [Google Scholar] [CrossRef] [PubMed]
- MacLellan, J.; Surey, J.; Abubakar, I.; Stagg, H.R. Peer support workers in health: A qualitative metasynthesis of their experiences. PLoS ONE 2015, 10, e0141122. [Google Scholar] [CrossRef] [Green Version]
- Charmaz, K.; Belgrave, L.L. Grounded Theory. In The Blackwell Encyclopedia of Sociology; American Cancer Society: Atlanta, GA, USA, 2015. [Google Scholar] [CrossRef]
- Verbakel, E.; Tamlagsrønning, S.; Winstone, L.; Fjær, E.L.; Eikemo, T.A. Informal care in Europe: Findings from the European Social Survey (2014) special module on the social determinants of health. Eur. J. Public Health 2017, 27 (Suppl. 1), 90–95. [Google Scholar] [CrossRef]
- Sharma, N.; Chakrabarti, S.; Grover, S. Gender differences in caregiving among family—Caregivers of people with mental illnesses. World J. Psychiatry 2016, 6, 7. [Google Scholar] [CrossRef]
- Jang, S.-N.; Avendano, M.; Kawachi, I. Informal Caregiving Patterns in Korea and European Countries: A Cross-National Comparison. Asian Nurs. Res. 2012, 6, 19–26. [Google Scholar] [CrossRef] [Green Version]
- Shea, C.M.; Young, T.L.; Powell, B.J.; Rohweder, C.; Enga, Z.K.; Scott, J.E.; Carter-Edwards, L.; Corbie-Smith, G. Researcher readiness for participating in community-engaged dissemination and implementation research: A conceptual framework of core competencies. Transl. Behav. Med. 2017, 7, 393–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitehead, M. A typology of actions to tackle social inequalities in health. J. Epidemiol. Community Health 2007, 61, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Arnstein, S.R. A Ladder of Citizen Participation. J. Am. Inst. Plan. 1969, 35, 216–224. [Google Scholar] [CrossRef] [Green Version]
- Gagnon, M.-P.; Desmartis, M.; Gagnon, J.; St-Pierre, M.; Gauvin, F.-P.; Rhainds, M.; Lepage-Savary, D.; Coulombe, M.; Dipankui, M.T.; Légaré, F. Introducing the patient’s perspective in hospital health technology assessment (HTA): The views of HTA producers, hospital managers and patients. Health Expect. 2014, 17, 888–900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nueces, D.L.; Hacker, K.; DiGirolamo, A.; Hicks, L.S. A Systematic Review of Community-Based Participatory Research to Enhance Clinical Trials in Racial and Ethnic Minority Groups. Health Serv. Res. 2012, 47, 1363–1386. [Google Scholar] [CrossRef] [Green Version]
- Browne, A.J.; Varcoe, C.M.; Wong, S.T.; Smye, V.L.; Lavoie, J.; Littlejohn, D.; Tu, D.; Godwin, O.; Krause, M.; Khan, K.B.; et al. Closing the health equity gap: Evidence-based strategies for primary health care organizations. Int. J. Equity Health 2012, 11, 59. [Google Scholar] [CrossRef] [Green Version]
- Cyril, S.; Smith, B.J.; Possamai-Inesedy, A.; Renzaho, A.M.N. Exploring the role of community engagement in improving the health of disadvantaged populations: A systematic review. Glob. Health Action 2015, 8, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Forsythe, L.P.; Szydlowski, V.; Murad, M.H.; Ip, S.; Wang, Z.; Elraiyah, T.A.; Fleurence, R.; Hickam, D.H. A Systematic Review of Approaches for Engaging Patients for Research on Rare Diseases. J. Gen. Intern. Med. 2014, 29, 788–800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newington, L.; Metcalfe, A. Researchers’ and Clinicians’ Perceptions of Recruiting Participants to Clinical Research: A Thematic Meta-Synthesis. J. Clin. Med. Res. 2014, 6, 162–172. [Google Scholar] [CrossRef] [Green Version]
- George, A.S.; Mehra, V.; Scott, K.; Sriram, V. Community participation in health systems research: A systematic review assessing the state of research, the nature of interventions involved and the features of engagement with communities. PLoS ONE 2015, 10, e0141091. [Google Scholar] [CrossRef] [Green Version]
- Shippee, N.D.; Garces, J.P.D.; Lopez, G.J.P.; Wang, Z.; Elraiyah, T.A.; Nabhan, M.; Brito, J.P.; Boehmer, K.; Hasan, R.; Firwana, B.; et al. Patient and service user engagement in research: A systematic review and synthesized framework. Health Expect. 2015, 18, 1151–1166. [Google Scholar] [CrossRef] [Green Version]
- Abma, T.A.; Nierse, C.J.; Widdershoven, G.A.M. Patients as partners in responsive research: Methodological notions for collaborations in mixed research teams. Qual. Health Res. 2009, 19, 401–415. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).