
Ambient Cumulative PM2.5 Exposure and the Risk of Lung Cancer Incidence and Mortality: A Retrospective Cohort Study

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Source
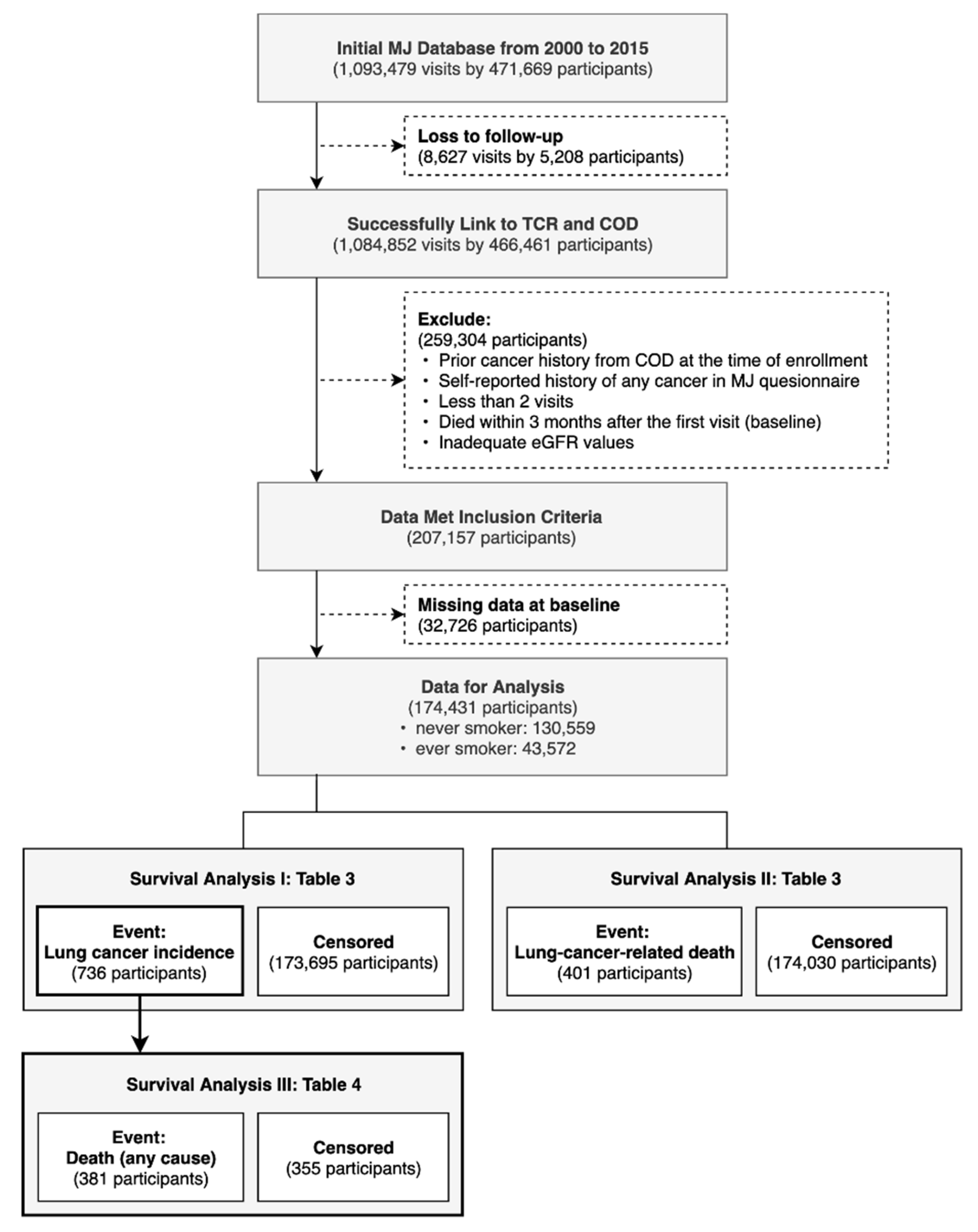
2.2. Selection of Study Population
2.3. Endpoints
2.4. Definition of Variables
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA A Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health and Welfare. Cause of Death Statistics. Available online: https://www.mohw.gov.tw/lp-4650-2.html (accessed on 3 May 2021).
- Giovino, G.A. Epidemiology of tobacco use in the United States. Oncogene 2002, 21, 7326–7340. [Google Scholar] [CrossRef] [Green Version]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer Incidence and Mortality Worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef]
- Couraud, S.; Debieuvre, D.; Moreau, L.; Dumont, P.; Margery, J.; Quoix, E.; Duvert, B.; Cellerin, L.; Baize, N.; Taviot, B.; et al. No impact of passive smoke on the somatic profile of lung cancers in never-smokers. Eur. Respir. J. 2015, 45, 1415–1425. [Google Scholar] [CrossRef] [Green Version]
- Toh, C.-K.; Gao, F.; Lim, W.-T.; Leong, S.-S.; Fong, K.-W.; Yap, S.-P.; Hsu, A.A.; Eng, P.; Koong, H.-N.; Thirugnanam, A.; et al. Never-Smokers with Lung Cancer: Epidemiologic Evidence of a Distinct Disease Entity. J. Clin. Oncol. 2006, 24, 2245–2251. [Google Scholar] [CrossRef] [PubMed]
- Pallis, A.G.; Syrigos, K.N. Lung cancer in never smokers: Disease characteristics and risk factors. Crit. Rev. Oncol. Hematol. 2013, 88, 494–503. [Google Scholar] [CrossRef]
- Bell, D.W.; Brannigan, B.W.; Matsuo, K.; Finkelstein, D.M.; Sordella, R.; Settleman, J.; Mitsudomi, T.; Haber, D.A. Increased Prevalence of EGFR-Mutant Lung Cancer in Women and in East Asian Populations: Analysis of Estrogen-Related Polymorphisms. Clin. Cancer Res. 2008, 14, 4079–4084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tseng, C.-H.; Tsuang, B.-J.; Chiang, C.-J.; Ku, K.-C.; Tseng, J.-S.; Yang, T.-Y.; Hsu, K.-H.; Chen, K.-C.; Yu, S.-L.; Lee, W.-C.; et al. The Relationship between Air Pollution and Lung Cancer in Nonsmokers in Taiwan. J. Thorac. Oncol. 2019, 14, 784–792. [Google Scholar] [CrossRef]
- Turner, M.C.; Krewski, D.; Pope, C.A., III; Chen, Y.; Gapstur, S.M.; Thun, M.J. Long-term ambient fine particulate matter air pollution and lung cancer in a large cohort of never-smokers. Am. J. Respir. Crit. Care Med. 2011, 184, 1374–1381. [Google Scholar] [CrossRef]
- Hamra, G.B.; Guha, N.; Cohen, A.; Laden, F.; Raaschou-Nielsen, O.; Samet, J.M.; Vineis, P.; Forastiere, F.; Saldiva, P.; Yorifuji, T. Outdoor particulate matter exposure and lung cancer: A systematic review and meta-analysis. Environ. Health Perspect. 2014, 122, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olsson, A.C.; Gustavsson, P.; Kromhout, H.; Peters, S.; Vermeulen, R.; Brüske, I.; Pesch, B.; Siemiatycki, J.; Pintos, J.; Brüning, T.; et al. Exposure to Diesel Motor Exhaust and Lung Cancer Risk in a Pooled Analysis from Case-Control Studies in Europe and Canada. Am. J. Respir. Crit. Care Med. 2011, 183, 941–948. [Google Scholar] [CrossRef] [Green Version]
- Yorifuji, T.; Kashima, S.; Tsuda, T.; Ishikawa-Takata, K.; Ohta, T.; Tsuruta, K.-I.; Doi, H. Long-term exposure to traffic-related air pollution and the risk of death from hemorrhagic stroke and lung cancer in Shizuoka, Japan. Sci. Total Environ. 2013, 443, 397–402. [Google Scholar] [CrossRef]
- Huang, F.; Pan, B.; Wu, J.; Chen, E.; Chen, L. Relationship between exposure to PM2.5 and lung cancer incidence and mortality: A meta-analysis. Oncotarget 2017, 8, 43322–43331. [Google Scholar] [CrossRef] [Green Version]
- Ito, Y.; Wakai, K.; Suzuki, K.; Ozasa, K.; Watanabe, Y.; Seki, N.; Ando, M.; Nishino, Y.; Kondo, T.; Ohno, Y.; et al. Lung Cancer Mortality and Serum Levels of Carotenoids, Retinol, Tocopherols, and Folic Acid in Men and Women: A Case-Control Study Nested in the JACC Study. J. Epidemiol. 2005, 15, S140–S149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lei, Y.; Cai, W.; Chen, Y.; Du, Y.-X. Some lifestyle factors in human lung cancer: A case-control study of 792 lung cancer cases. Lung Cancer 1996, 14, S121–S136. [Google Scholar] [CrossRef]
- Gao, Y. Risk factors for lung cancer among nonsmokers with emphasis on lifestyle factors. Lung Cancer 1996, 14, S39–S45. [Google Scholar] [CrossRef]
- Blumberg, J. The Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study in Finland. Nutr. Rev. 2009, 52, 242–245. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Tsai, S.P.; Tsao, C.K.; Chiu, M.L.; Tsai, M.K.; Lu, P.J.; Lee, J.H.; Chen, C.H.; Wen, C.; Chang, S.-S.; et al. Cohort Profile: The Taiwan MJ Cohort: Half a million Chinese with repeated health surveillance data. Int. J. Epidemiol. 2017, 46, 1744–1744g. [Google Scholar] [CrossRef]
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D.R.; the Modification of Diet in Renal Disease Study Group. A More Accurate Method to Estimate Glomerular Filtration Rate from Serum Creatinine: A New Prediction Equation. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef]
- Mok, Y.; Ballew, S.H.; Sang, Y.; Coresh, J.; Joshu, C.E.; Platz, E.A.; Matsushita, K. Albuminuria, Kidney Function, and Cancer Risk in the Community. Am. J. Epidemiol. 2020, 189, 942–950. [Google Scholar] [CrossRef] [PubMed]
- Chuang, Y.-H.; Lin, I.-F.; Lao, X.Q.; Lin, C.; Chan, T.-C. The Association between Renal Function Decline and the Incidence of Urothelial Carcinoma: A 16-year Retrospective Cohort Study in Taiwan. Eur. Urol. Open Sci. 2021, 27, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Grunnet, M.; Sorensen, J. Carcinoembryonic antigen (CEA) as tumor marker in lung cancer. Lung Cancer 2012, 76, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Li, Y.; Yuan, Z.; Lau, A.; Li, C.; Fung, J. Using satellite remote sensing data to estimate the high-resolution distribution of ground-level PM2.5. Remote Sens. Environ. 2015, 156, 117–128. [Google Scholar] [CrossRef]
- Zhang, Z.; Chang, L.-Y.; Lau, A.K.H.; Chan, T.-C.; Chuang, Y.C.; Chan, J.; Lin, C.; Jiang, W.K.; Dear, K.; Zee, B.C.-Y.; et al. Satellite-based estimates of long-term exposure to fine particulate matter are associated with C-reactive protein in 30,034 Taiwanese adults. Int. J. Epidemiol. 2017, 46, 1126–1136. [Google Scholar] [CrossRef] [PubMed]
- Yun, Y.D.; Back, J.H.; Ghang, H.; Jee, S.H.; Kim, Y.; Lee, S.M.; Samet, J.M.; Lee, K.S. Hazard Ratio of Smoking on Lung Cancer in Korea According to Histological Type and Gender. Lung 2015, 194, 281–289. [Google Scholar] [CrossRef]
- Khuder, S.A. Effect of cigarette smoking on major histological types of lung cancer: A meta-analysis. Lung Cancer 2001, 31, 139–148. [Google Scholar] [CrossRef]
- Ghazipura, M.; Garshick, E.; Cromar, K. Ambient PM 2.5 exposure and risk of lung cancer incidence in North America and Europe. Environ. Res. Commun. 2019, 1, 015004. [Google Scholar] [CrossRef]
- Raaschou-Nielsen, O.; Andersen, Z.J.; Beelen, R.; Samoli, E.; Stafoggia, M.; Weinmayr, G.; Hoffmann, B.; Fischer, P.; Nieuwenhuijsen, M.J.; Brunekreef, B.; et al. Air pollution and lung cancer incidence in 17 European cohorts: Prospective analyses from the European Study of Cohorts for Air Pollution Effects (ESCAPE). Lancet Oncol. 2013, 14, 813–822. [Google Scholar] [CrossRef]
- Li, R.; Zhou, R.; Zhang, J. Function of PM2.5 in the pathogenesis of lung cancer and chronic airway inflammatory diseases (Review). Oncol. Lett. 2018, 15, 7506–7514. [Google Scholar] [CrossRef] [Green Version]
- Lipfert, F.W.; Wyzga, R.E. Longitudinal relationships between lung cancer mortality rates, smoking, and ambient air quality: A comprehensive review and analysis. Crit. Rev. Toxicol. 2019, 49, 790–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slezakova, K.; Castro, D.; Pereira, M.; Morais, S.; Delerue-Matos, C.; Alvim-Ferraz, M. Influence of tobacco smoke on carcinogenic PAH composition in indoor PM10 and PM2.5. Atmos. Environ. 2009, 43, 6376–6382. [Google Scholar] [CrossRef] [Green Version]
- WHO. Global Strategy on Diet, Physical Activity and Health. Available online: http://www.who.int/dietphysicalactivity/fruit/en/ (accessed on 10 May 2021).
- Aune, D.; Giovannucci, E.; Boffetta, P.; Fadnes, L.T.; Keum, N.N.; Norat, T.; Greenwood, D.C.; Riboli, E.; Vatten, L.J.; Tonstad, S. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality—A systematic review and dose-response meta-analysis of prospective studies. Int. J. Epidemiol. 2017, 46, 1029–1056. [Google Scholar] [CrossRef] [PubMed]
- Druesne-Pecollo, N.; Latino-Martel, P.; Norat, T.; Barrandon, E.; Bertrais, S.; Galan, P.; Hercberg, S. Beta-carotene supplementation and cancer risk: A systematic review and metaanalysis of randomized controlled trials. Int. J. Cancer 2009, 127, 172–184. [Google Scholar] [CrossRef] [PubMed]
- Vieira, A.R.; Abar, L.; Vingeliene, S.; Chan, D.S.M.; Aune, D.; Navarro-Rosenblatt, D.; Stevens, C.; Greenwood, D.; Norat, T. Fruits, vegetables and lung cancer risk: A systematic review and meta-analysis. Ann. Oncol. 2016, 27, 81–96. [Google Scholar] [CrossRef] [PubMed]
- Cheng, F.-Y.; Hsu, C.-H. Long-term variations in PM2.5 concentrations under changing meteorological conditions in Taiwan. Sci. Rep. 2019, 9, 6635. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Event of Interest | Overall (N = 174,431) | LC Incidence | LC-Related Mortality | ||||
|---|---|---|---|---|---|---|---|
| Variables | Non LC (N = 173,695) | LC (N = 736) | p-Value | Survivor (N = 174,030) | LC-Related Death (N = 401) | p-Value | |
| Age (years), mean ± SD | 39.02 ± 12.95 | 38.95 ± 12.92 | 54.96 ± 12.32 | <0.001 | 38.97 ± 12.92 | 59.08 ± 12.05 | <0.001 |
| Female, N (%) | 87,722 (50.29) | 87,363 (50.30) | 359 (48.78) | 0.411 | 87,563 (50.31) | 159 (39.65) | <0.001 |
| Education level, N (%) | |||||||
| High school or lower | 68,233 (39.12) | 67,735 (39.00) | 498 (67.66) | <0.001 | 67,931 (39.03) | 302 (75.31) | <0.001 |
| College or higher | 106,198 (60.88) | 105,960(61.00) | 238 (32.34) | 106,099 (60.97) | 99 (24.69) | ||
| Body mass index (kg/m2), mean ± SD | 22.91 ± 3.60 | 22.90 ± 3.60 | 23.39 ± 3.31 | <0.001 | 22.90 ± 3.60 | 23.53 ± 3.40 | <0.001 |
| <18.5 | 16,147 (9.26) | 16,111 (9.28) | 36 (4.89) | <0.001 | 16,128 (9.27) | 19 (4.74) | 0.005 |
| 18.5–23.9 | 97,271 (55.76) | 96,853 (55.76) | 418 (56.79) | 97,052 (55.77) | 219 (54.61) | ||
| 24–27.9 | 46,721 (26.78) | 46,501 (26.77) | 220 (29.89) | (26.77) | 128 (31.92) | ||
| ≥28 | 14,292 (8.19) | 14,230 (8.19) | 62 (8.42) | 14,257 (8.19) | 35 (8.73) | ||
| eGFR (mL/min/1.73 m2), mean ± SD, N (%) | 86.41 ± 17.83 | 86.45 ± 17.82 | 77.31 ± 15.91 | <0.001 | 86.44 ± 17.82 | 74.44 ± 15.50 | <0.001 |
| ≥ 90 | 64,333 (36.88) | 64,187 (36.95) | 146 (19.84) | <0.001 | 64,268 (36.93) | 65 (16.21) | <0.001 |
| 60–89 | 105,042 (60.22) | 104,530 (60.18) | 512 (69.57) | 104,771 (60.20) | 271 (67.58) | ||
| 45–59 | 4471 (2.56) | 4403 (2.53) | 68 (9.24) | 4415 (2.54) | 56 (13.97) | ||
| <45 | 585 (0.34) | 575 (0.33) | 10 (1.36) | 576 (0.33) | 9 (2.24) | ||
| eGFR annual decline ≥5 | 20,385 (11.69) | 20,310 (11.69) | 75 (10.19) | 0.205 | 20,346 (11.69) | 39 (9.73) | 0.221 |
| CEA (mg/dL), mean ± SD a | 1.46 ± 1.18 | 1.45 ± 1.45 | 2.33 ± 3.21 | <0.001 | 1.45 ± 1.17 | 2.87 ± 4.43 | <0.001 |
| Family history of LC, N (%) | 9160 (5.25) | 9101 (5.24) | 59 (8.02) | <0.001 | 9136 (5.25) | 24 (5.99) | 0.510 |
| Comorbidities, N (%) | |||||||
| Hypertension | 12,106 (6.94) | 11,970 (6.89) | 136 (18.48) | <0.001 | 12,019 (6.91) | 87 (21.70) | <0.001 |
| Diabetic mellitus | 7084 (4.06) | 7020 (4.04) | 64 (8.70) | <0.001 | 7035 (4.04) | 49 (12.22) | <0.001 |
| CVD | 4754 (2.73) | 4696 (2.70) | 58 (7.88) | <0.001 | 4710 (2.71) | 44 (10.97) | <0.001 |
| CVA | 478 (0.27) | 471 (0.27) | 7 (0.95) | 0.005 | 471 (0.27) | 7 (1.75) | <0.001 |
| Lifestyle behaviors, N (%) | |||||||
| Smoking status | |||||||
| Never smoker | 130,559 (74.85) | 130,091 (74.90) | 468 (63.59) | <0.001 | 130,344 (74.90) | 215 (53.62) | <0.001 |
| Ever smoker | 43,872 (25.15) | 43,604 (25.10) | 268 (36.41) | 43,686 (25.10) | 186 (46.39) | ||
| Fruit/vegetable ≥ 2 servings per day | 164,115 (94.09) | 163,430 (94.09) | 685 (93.07) | 0.242 | 163,744 (94.09) | 371 (92.52) | 0.183 |
| PM2.5 exposure (μg/m3), median ± IQR, N(%) b | 21.45 ± 6.95 | 21.45 ± 6.95 | 20.20 ± 6.45 | <0.001 | 21.45 ± 6.95 | 20.00 ± 6.40 | <0.001 |
| <17.95 | 43,693 (25.05) | 43,503 (25.05) | 190 (25.82) | 43,572 (25.04) | 121 (30.17) | ||
| 17.95 ≤ PM2.5 < 21.45 | 43,671 (25.04) | 43,413 (24.99) | 258 (35.05) | 43,532 (25.01) | 139 (34.66) | ||
| 21.45 ≤ PM2.5 < 24.9 | 43,272 (24.81) | 43,119 (24.82) | 153 (20.79) | 43,194 (24.82) | 78 (19.45) | ||
| ≥24.9 | 43,795 (25.11) | 43,660 (25.14) | 135 (18.34) | 43,732 (25.13) | 63 (15.71) | ||
| Follow-up time (years) c, median ± IQR | 12.29 ± 6.25 c | 12.29 ± 6.24 | 8.71 ± 6.00 | <0.001 | 12.29 ± 6.25 | 9.43 ± 5.35 | <0.001 |
| Type of LC diagnosis, N(%) d | <0.001 | ||||||
| Small-cell | 33 (0.02) | 33 (4.48) | 9 (0.01) | 24 (5.99) | |||
| Adenocarcinoma | 525 (0.30) | 525 (71.33) | 305 (0.18) | 220 (54.86) | |||
| Squamous cell | 76 (0.04) | 76 (10.33) | 26 (0.01) | 50 (12.47) | |||
| Others | 102 (0.06) | 102 (13.86) | 39 (0.02) | 63 (15.71) | |||
| Variable | Overall (n = 736) | Never Smoker (n = 468) | Ever Smoker (n = 268) | p-Value |
|---|---|---|---|---|
| Age (years), mean ± SD | 54.96 ±12.32 | 53.31 ± 12.05 | 57.85 ± 12.28 | <0.001 |
| Female, N(%) | 359 (48.78) | 333 (71.15) | 26 (9.70) | <0.001 |
| Education level, N(%) | <0.001 | |||
| High school or lower | 498 (67.66) | 291 (62.18) | 207 (77.24) | |
| College or higher | 238 (32.34) | 177 (37.82) | 61 (22.76) | |
| Body mass index (kg/m2), N(%) | 0.621 | |||
| <18.5 | 36 (4.89) | 23 (4.91) | 13 (4.85) | |
| 18.5–23.9 | 418 (56.79) | 274 (58.55) | 144 (53.73) | |
| 24–27.9 | 220 (29.89) | 133 (28.42) | 87 (32.46) | |
| ≥28 | 62 (8.42) | 38 (8.12) | 24 (8.96) | |
| eGFR (mL/min/1.73 m2), N(%) | 0.021 | |||
| ≥90 | 146 (19.84) | 103 (22.01) | 43 (16.04) | |
| 60–89 | 512 (69.57) | 326 (69.66) | 186 (69.40) | |
| 45–59 | 68 (9.24) | 35 (7.48) | 33 (12.31) | |
| <45 | 10 (1.36) | 4 (0.85) | 6 (2.24) | |
| eGFR annual decline ≥5 (mL/min/1.73 m2), N(%) | 75 (10.19) | 50 (10.68) | 25 (9.33) | 0.559 |
| CEA a (mg/dL), mean ± SD | 2.33 ± 3.21 | 1.89 ± 3.67 | 3.10 ± 1.97 | <0.001 |
| Family history of LC, N(%) | 59 (8.02) | 36 (7.69) | 23 (8.58) | 0.669 |
| Comorbidities, N(%) | ||||
| Hypertension | 136 (18.48) | 83 (17.74) | 53 (19.78) | 0.492 |
| Diabetic mellitus | 64 (8.70) | 34 (7.26) | 30 (11.19) | 0.069 |
| CVD | 58 (7.88) | 38 (8.12) | 20 (7.46) | 0.750 |
| CVA | 7 (0.95) | 3 (0.64) | 4 (1.49) | 0.252 |
| Fruit/vegetable ≥ 2 servings per day, N(%) | 685 (93.07) | 451 (96.37) | 234 (87.31) | <0.001 |
| PM2.5 exposure (μg/m3), median ± IQR, N(%) b | 20.20 ± 6.45 | 20.30 ± 6.24 | 20.00 ± 7.77 | 0.012 |
| <17.95 | 190 (25.82) | 106 (22.65) | 84 (31.34) | |
| 17.95 ≤ PM2.5 < 21.45 | 258 (35.05) | 164 (35.04) | 94 (35.07) | |
| 21.45 ≤ PM2.5 < 24.9 | 153 (20.79) | 106 (22.65) | 47 (17.54) | |
| ≥24.9 | 135 (18.34) | 92 (19.66) | 43 (16.04) | |
| Time to event (years), median ± IQR | 8.71 ± 6.00 | 8.55 ± 6.55 | 8.93 ± 5.36 | 0.631 |
| Types of LC diagnosis, N(%) c | <0.001 | |||
| Small-cell | 33 (0.02) | 4 (0.85) | 29 (10.82) | |
| Adenocarcinoma | 525 (0.30) | 385 (82.26) | 140 (52.24) | |
| Squamous cell | 76 (0.04) | 20 (4.27) | 56 (20.90) | |
| Others | 102 (0.06) | 59 (12.61) | 43 (16.04) | |
| All-cause death, N(%) | 381 (51.77) | 206 (44.02) | 175 (65.30) | <0.001 |
| Event of Interest | LC Incidence | LC-Related Mortality | ||||||
|---|---|---|---|---|---|---|---|---|
| Never Smokers (N = 130,559; LC = 468) | Ever Smokers (N = 43,872; LC = 268) | Never Smokers (N = 130,559; Death = 215) | Ever Smokers (N = 43,872; Death = 186) | |||||
| Variables | aHR (95%CI) | p-Value | aHR (95%CI) | p-Value | aHR (95%CI) | p-Value | aHR (95%CI) | p-Value |
| Age ≥ 50 | 5.26 (4.16, 6.65) | <0.001 | 6.98 (5.09, 9.59) | <0.001 | 7.33 (5.05, 10.64) | <0.001 | 10.98 (7.09, 17.01) | <0.001 |
| Female | 1.33 (1.07, 1.64) | 0.009 | 0.89 (0.59, 1.35) | 0.577 | 1.14 (0.84, 1.54) | 0.403 | 0.61 (0.34, 1.11) | 0.105 |
| Lower education level | 1.05 (0.84, 1.31) | 0.653 | 1.86 (1.37, 2.54) | <0.001 | 1.15 (0.82, 1.61) | 0.422 | 2.33 (1.54, 3.53) | <0.001 |
| Body-mass index (kg/m2) | ||||||||
| 18.5–23.9 | ref. | ref. | ref. | ref. | ||||
| <18.5 | 0.77 (0.50, 1.18) | 0.232 | 1.22 (0.69, 2.17) | 0.493 | 1.02 (0.54, 1.91) | 0.954 | 1.25 (0.60, 2.58) | 0.553 |
| 24–27.9 | 0.80 (0.64, 0.99) | 0.040 | 0.74 (0.56, 0.97) | 0.027 | 0.72 (0.53, 0.99) | 0.042 | 0.81 (0.59, 1.12) | 0.198 |
| ≥28 | 0.72 (0.51, 1.03) | 0.075 | 0.72 (0.47, 1.12) | 0.150 | 0.60 (0.35, 1.01) | 0.054 | 0.77 (0.45, 1.30) | 0.320 |
| eGFR (mL/min/1.73 m2) | ||||||||
| ≥90 | ref. | ref. | ref. | ref. | ||||
| 60–89 | 1.58 (1.25, 2.00) | <0.001 | 1.33 (0.93, 1.89) | 0.117 | 1.88 (1.28, 2.77) | 0.001 | 1.10 (0.71, 1.68) | 0.676 |
| 45–59 | 1.85 (1.23, 2.79) | 0.003 | 1.87 (1.15, 3.06) | 0.012 | 3.13 (1.81, 5.40) | <0.001 | 1.92 (1.11, 3.33) | 0.020 |
| <45 | 1.47 (0.54, 4.06) | 0.453 | 2.49 (1.03, 6.02) | 0.043 | 2.37 (0.71, 7.85) | 0.160 | 2.82 (1.13, 7.05) | 0.026 |
| eGFR annual decline ≥ 5 | 1.28 (0.94, 1.73) | 0.117 | 1.27 (0.83, 1.96) | 0.269 | 1.26 (0.79, 2.02) | 0.327 | 1.36 (0.82, 2.27) | 0.236 |
| CEA(mg/dL), per increment | 1.06 (1.04, 1.08) | <0.001 | 1.16 (1.11, 1.22) | <0.001 | 1.07 (1.05, 1.09) | <0.001 | 1.19 (1.13, 1.25) | <0.001 |
| Family history of LC | 1.68 (1.20, 2.37) | <0.001 | 1.73 (1.12, 2.65) | 0.013 | 1.45 (0.84, 2.49) | 0.184 | 1.07 (0.56, 2.02) | 0.844 |
| Fruit/vegetable ≥ 2 servings per day | 1.12 (0.69, 1.82) | 0.648 | 0.68 (0.47, 0.97) | 0.034 | 0.92 (0.47, 1.80) | 0.813 | 0.76 (0.48, 1.20) | 0.241 |
| PM2.5 exposure (μg/m3) a, per 10 increment | 1.32 (1.12, 1.56) | 0.001 | 1.04 (0.86, 1.27) | 0.666 | 1.28 (1.01, 1.63) | 0.043 | 0.96 (0.76, 1.20) | 0.714 |
| HTN | 1.17 (0.90, 1.52) | 0.256 | 1.25 (0.90, 1.74) | 0.190 | 1.17 (0.81, 1.68) | 0.402 | 1.10 (0.74, 1.61) | 0.638 |
| DM | 0.92 (0.64, 1.33) | 0.663 | 0.99 (0.67, 1.47) | 0.948 | 1.35 (0.87, 2.09) | 0.176 | 0.99 (0.63, 1.54) | 0.954 |
| CVA | 1.00 (0.32, 3.15) | 0.996 | 1.14 (0.42, 3.12) | 0.793 | 1.13 (0.28, 4.60) | 0.867 | 1.72 (0.69, 4.27) | 0.243 |
| CVD | 1.37 (0.96, 1.94) | 0.079 | 1.14 (0.71, 1.83) | 0.594 | 1.70 (1.09, 2.64) | 0.019 | 1.42 (0.86, 2.34) | 0.166 |
| Never Smoker a (N = 323; Death = 161) | Ever Smoker (N = 192; Death = 131) | |||
|---|---|---|---|---|
| Variable | aHR (95%CI) | p-Value | aHR (95%CI) | p-Value |
| Age at diagnosis of LC | 1.03 (1.01, 1.04) | <0.001 | 1.03 (1.01, 1.05) | 0.001 |
| Female (ref. male) | 0.67 (0.47, 0.95) | 0.024 | 1.04 (0.57, 1.92) | 0.891 |
| Lower education level (ref. college or higher) | 0.79 (0.55, 1.14) | 0.210 | 1.03 (0.61, 1.74) | 0.907 |
| Cancer stage b III and IV (ref. I and II) | 6.09 (3.87, 9.57) | <0.001 | 7.48 (4.15, 13.48) | <0.001 |
| Cancer type c non-adeno(ref. adenocarcinoma) | 2.55 (1.73, 3.75) | <0.001 | 1.29 (0.90, 1.86) | 0.165 |
| PM2.5 exposure d, per 10 increment, μg/m3 | 1.09 (0.83, 1.44) | 0.534 | 0.82 (0.62, 1.08) | 0.154 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, H.-L.; Chuang, Y.-H.; Lin, T.-H.; Lin, C.; Chen, Y.-H.; Hung, J.-Y.; Chan, T.-C. Ambient Cumulative PM2.5 Exposure and the Risk of Lung Cancer Incidence and Mortality: A Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 12400. https://doi.org/10.3390/ijerph182312400
Huang H-L, Chuang Y-H, Lin T-H, Lin C, Chen Y-H, Hung J-Y, Chan T-C. Ambient Cumulative PM2.5 Exposure and the Risk of Lung Cancer Incidence and Mortality: A Retrospective Cohort Study. International Journal of Environmental Research and Public Health. 2021; 18(23):12400. https://doi.org/10.3390/ijerph182312400
Chicago/Turabian StyleHuang, Hung-Ling, Yung-Hsin Chuang, Tzu-Hsuan Lin, Changqing Lin, Yen-Hsu Chen, Jen-Yu Hung, and Ta-Chien Chan. 2021. "Ambient Cumulative PM2.5 Exposure and the Risk of Lung Cancer Incidence and Mortality: A Retrospective Cohort Study" International Journal of Environmental Research and Public Health 18, no. 23: 12400. https://doi.org/10.3390/ijerph182312400
APA StyleHuang, H.-L., Chuang, Y.-H., Lin, T.-H., Lin, C., Chen, Y.-H., Hung, J.-Y., & Chan, T.-C. (2021). Ambient Cumulative PM2.5 Exposure and the Risk of Lung Cancer Incidence and Mortality: A Retrospective Cohort Study. International Journal of Environmental Research and Public Health, 18(23), 12400. https://doi.org/10.3390/ijerph182312400