Abstract
Earlier exposure to binge drinking and tobacco use is associated with higher odds of substance use disorders. Using national youth data from the PATH study, we prospectively estimate the age of initiating past 30-day use of (1) cigarettes, e-cigarettes, and binge drinking, and (2) cigarettes, cigarillos, and binge drinking. Cox proportional hazard models were used to estimate differences in the age of initiation by sex, race/ethnicity, and previous use of other tobacco products. By age 21, 4.4% (95% CI: 3.7–5.2) and 2.0% (95% CI: 1.2–2.8) of youth reported initiation of past 30-day use outcomes (1) and (2), respectively. After controlling for sex and previous use of other tobacco products, statistically significant differences in the age of initiation by race/ethnicity were found for each outcome: Hispanic and non-Hispanic Black youth were less likely than non-Hispanic White youth to initiate past 30-day use of both outcomes (1) and (2) at earlier ages. Although the initiation of both outcomes remained relatively low by age 21, these incidences represent 1.56 million and 700,000 youth, respectively. This study provides the public with evidence to identify the particular ages at which education campaigns may be most effective to prevent youth from initiating these three substances. Further research is needed to estimate the age of initiation of other dual tobacco use patterns with binge drinking.
1. Introduction
Tobacco and alcohol use are estimated to cause approximately 29% [1] and 5.5% [2] of cancer deaths in the U.S., respectively. Additionally, using both tobacco and alcohol further increases the risk of developing cancer. In fact, several studies show that the association between alcohol with oral and pharyngeal cancer was stronger among tobacco users, and that the joint effect of tobacco and alcohol on oral and pharyngeal cancer was not additive but multiplicative [3,4]. In addition, use of tobacco and alcohol increases the risk for adverse mental health outcomes [5,6,7,8,9]. Furthermore, the earlier people initiate tobacco and/or alcohol use, the higher the odds of developing a substance use disorder [10,11,12]. Given the greater health risk imposed by using both tobacco and alcohol, one important risk factor to consider for prevention is the age of initiation of these substances. In this manuscript, e-cigarettes are included as a tobacco product (TP) because e-cigarettes contain nicotine in the U.S. [13].
According to the 2019 National Youth Tobacco Survey (NYTS) data, e-cigarettes and cigar products were the most commonly used tobacco products among U.S. middle and high school students, with 20.0% and 5.3% middle and high school students using e-cigarettes and cigar products in the past 30-days, respectively [14]. Similarly, a previous report of the Population Assessment of Tobacco and Health (PATH) study from 2013–2016 among youth never tobacco users found that 4.7%, 6.4%, and 4.0% reported past 30-day cigarette, e-cigarette, or any cigar (cigarillos, filtered cigars, and traditional cigars) use, respectively, after one or two years of follow-up [15]. Among a nationally representative sample of youth who reported any TP use, a 2013–2014 PATH study reported the prevalence of the most common combinations of dual TP use as: 15% cigarettes and e-cigarettes and 10% cigarettes and cigarillos [16]. The same study also reported that among youth who had used any TP in the past 30-days, 43.0% reported using more than 1 TP in the past 30-days. Among these poly-tobacco users, cigarettes, e-cigarettes, and cigarillos were the most popular, with 71.4%, 53.7%, and 46.0% reporting the use of each TP [16]. Dual TP use is problematic, as it exposes youth to more tobacco toxicants than single-product use as seen in biomarker data studies [17,18], and a previous PATH study found dual TP use is associated with increased nicotine dependence [19]. Furthermore, dual use of cigarettes and e-cigarettes is associated with higher odds of cardiovascular disease than when each product is used alone [20].
A study using data from the 2017 National Survey on Drug Use and Health found that 5.3% of youth (aged 12–17) reported binge drinking in the past 30-days [21], which is a concern considering the reinforcing relationship between tobacco and alcohol, in which alcohol is primary trigger for initiation of tobacco use and relapse back to tobacco use after quit attempts [5,20,21]. Given that alcohol consumed in excessive amounts (i.e., binge drinking) and dual TP use are linked to long-term health consequences (i.e., heart diseases, stroke, cancer, and substance use disorders) [22,23,24], especially when youth start using these substances at younger ages, it is imperative to understand the age of initiation of the polysubstance use behavior of past 30-day dual TP use and binge drinking.
Sex differences in tobacco use have been reported in previous studies, with males reporting younger ages of initiation of cigarette, e-cigarette, and cigarillo use [25,26,27,28]. In addition, males are more likely to be dual and poly TP users [29]. Other studies have also found racial disparities in tobacco use patterns, with White youth reporting higher risk for all tobacco use patterns (i.e., mono, dual, and poly use) compared to their African American peers [30,31]. Similarly, sex and race/ethnicity group differences have been found in binge drinking, with male youth reporting higher rates of binge drinking than females [32], and White youth reporting higher rates of binge drinking than youth of other races/ethnicities [32].
The present paper prospectively estimates the age of initiation of two polysubstance use outcomes: past 30-day use of (i) cigarettes, e-cigarettes, and binge drinking, and past 30-day use of (ii) cigarettes, cigarillos, and binge drinking among youth (12–17 years old) in the PATH study who reported never use of these substances at their first wave of PATH participation (waves 1–4). Differences in the age of initiation of these two polysubstance use outcomes by sex and by race/ethnicity after controlling for the number of other TPs ever used were explored. Understanding the age of initiation of polysubstance use not only reinforces the importance of substance intervention at a young age, but also informs intervention and educational programs about possible differences by sex and by race/ethnicity.
2. Methods
2.1. Study Design and Participants
PATH is a nationally representative, longitudinal cohort study of US youth and adults that studies tobacco use behaviors, attitudes and beliefs, and tobacco-related health outcomes [33]. The target population of PATH consisted of individuals 12 years and older across the US, with 13,651 youth participating the study at wave 1 (September 2013 to December 2014). In addition, youth who were younger than 12 years old at wave 1 were considered “aged-up youth” when they turned 12 years old and were eligible to participate in the study in follow-up waves; 2091, 2045, 1694, and 4433 aged-up youth entered the PATH study at waves 2 (October 2014 to October 2015), 3 (October 2015 to October 2016), 4 (December 2016 to January 2018), and 5 (January 2018 to December 2019) respectively. Youth who turned 18 years old were invited to complete the adult measurements: 1915, 1907, and 1900 aged-up adults completed the adult questionnaire from waves 2 to 4 (October 2014 to January 2018), respectively. A sample of youth who reported never use of cigarettes, e-cigarettes, and cigarillos, and who did not binge drink in the past 30-days at their first wave of PATH participation (waves 1–4) were included using the restricted-use data [34]. Data from waves 2 to 5 were used to track outcomes for all participants. A total of 19,184 (representing 35,373,374 U.S. youth) constituted the sample. Informed oral consent was obtained from the parents of the youth and youth provided oral assent [33]. The Committee for the Protection of Human Subjects at the University of Texas Health Science Center at Houston provided IRB approval for this study with number HSC-SPH-17-0368.
2.2. Outcomes
Two polysubstance use outcomes were studied: the age of initiation of past 30-day use of (i) cigarettes, e-cigarettes, and binge drinking and the age of initiation of past 30 day use of (ii) cigarettes, cigarillos, and binge drinking. These polysubstance use outcomes are based on reporting past 30-day use of all three substances in the same PATH study wave. For each TP, PATH asked “In the past 30 days, have you smoked/used [TP], even one or two puffs/times?”. Response options included “yes”, “no”, and “don’t know”. Respondents who refused to answer or responded “don’t know” were considered missing. Among youth who reported past 30-day alcohol use, PATH also asked “On average, on those days you drank in the past 30 days, how many alcoholic drinks did you usually have each day? Count a drink as a can or bottle of beer; a wine cooler or a glass of wine, champagne, or sherry; a shot of liquor or a mixed drink or cocktail”. Boys who reported 3, 4, or 5+ drinks on days drank in the past 30 days were considered past 30-day binge drinkers for ages 12–13, 14–15, and 16–17 [35], respectively. Girls who reported 3+ drinks on days drank in the past 30 days were considered past 30-day binge drinkers [35]. Youth who answered “yes” to past 30-day cigarette use, past 30-day e-cigarette use and who reported past 30-day binge drinking in the same PATH wave were considered polysubstance users for outcome (i). Youth who answered “yes” to past 30-day cigarette use, past 30-day cigarillo use and who reported past 30-day binge drinking in the same PATH wave were considered polysubstance users for outcome (ii). Please note that cigarillo users include both blunt-only users (cigarillo users who remove the tobacco and replace it with marijuana) and those who used cigarillos as intended (see limitations section).
2.3. Other Tobacco Product Use
Youth may have used other tobacco products prior to initiation of each outcome. We considered other TPs, including hookah, smokeless tobacco, traditional cigars, and filtered cigars. Because of the low prevalence of use of each individual TP, we collapsed other TP use as 0 (never used other TPs) and 1+ (used at least one other TP). Youth who answered “Don’t know” to all TPs were considered missing. The number of other TPs ever used was calculated at youth’s first wave of PATH participation to ensure that the other TP use preceded each polysubstance use outcome.
2.4. Sex and Race/Ethnicity
The PATH study imputed self-reported participant sex by using the household information at wave 1 and categorized participants as boys and girls. The following categories measured self-reported participant race: White alone, Black alone, Asian alone, and other (including multiracial). Participants’ ethnicity was categorized as either Hispanic or non-Hispanic. In order to be comparable to the Surgeon General’s report [36], race and ethnicity were combined into four categories: non-Hispanic White, Hispanic, non-Hispanic Black, and non-Hispanic other (including, Asian and multiracial participants).
2.5. Age of Initiation of Polysubstance Use Outcomes
Two separate prospective estimations were conducted: (i) the age of initiation of past 30-day use of cigarettes, e-cigarettes, and binge drinking and (ii) the age of initiation of past 30-day use of cigarettes, cigarillos, and binge drinking. PATH provided the age of youth in years at each wave and the number of weeks between survey waves. We used participants’ age at their first wave of PATH participation (waves 1–4) and the number of weeks between survey waves (waves 2–5) until each past 30-day use outcome (i and ii) to estimate the lower and upper age bounds as an interval-censored age of initiation. For all participants, the lower age bound was the highest possible age a participant remained a non-polysubstance user for each outcome. The lower age bound was calculated as the sum of the age at the first wave of PATH participation and the number of weeks between survey waves until the latest wave where the participants reported non-use of all three substances in the past 30-days. For those who become users, the upper age bound was the highest possible age when youth first reported past 30-day use of each polysubstance use behavior (i and ii). The upper age bound was calculated as the sum of the age at their first wave of PATH participation and the number of weeks between survey waves until the first report of using all three substances in the past 30-days for each outcome. For youth who remained non-users of all three substances for each outcome, the upper age bound was censored.
2.6. Statistical Analysis
PATH uses a complex survey design, requiring the use of sampling weights and balanced repeated replicate weights with Fay’s correction factor of 0.3 [33,37]. Weighted summary statistics are provided. The distribution of the age of initiation for polysubstance use outcomes (i) and (ii) were estimated using weighted interval-censoring survival analysis [38]. The hazard function (and its 95% confidence intervals) for each polysubstance use outcome was estimated using the Turnbull non-parametric estimator [39], and are reported as cumulative incidence in percentages, which is presented in a figure. Weighted interval-censoring Cox proportional hazards regression models [40] were used to examine differences in the estimated age of initiation by sex and by race/ethnicity while controlling for ever use of other TPs. If there were statistically significant differences by sex or by race/ethnicity on the age of initiation of each polysubstance use outcome, weighted interval-censoring survival analyses were conducted stratified by sex or by race/ethnicity. There was very little missingness in PATH, and missing values are reported. All statistical analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC, USA).
3. Results
3.1. Sample Demographics
Demographic characteristics of PATH youth who had never used cigarettes, e-cigarettes, and cigarillos and had not binge drank in the past 30-days are reported in Table 1. Their average age was 13.6 years old, 55.2% entered the study at wave 1, 51% were males, and 23.4% were Hispanic. Among youth, 0.2%, 0.02%, 1.3%, and 0.7% have ever used traditional cigars, filtered cigars, hookah, or smokeless tobacco, respectively. Therefore, 2.2% had ever used any other TP.

Table 1.
Demographic characteristics of PATH ¥ youth (aged 12–17) never users at their first wave of participation.
3.2. Prospective Estimation of Age of Initiation of Past 30-Day Polysubstance Use Outcomes
Table 2 shows the distribution of the age of initiating past 30-day polysubstance use outcomes for the entire sample of youth. Initiation of both polysubstance use outcomes remained low for the ages that characterize youth (12–17 years). However, by age 21, 4.44% (95% CI: 3.72–5.16) of youth are estimated to initiate past 30-day use of cigarettes, e-cigarettes, and binge drinking, representing 1.57 million U.S. youth. By age 21, 1.98% (95% CI: 1.20–2.77) of youth are estimated to initiate past 30-day use of cigarettes, cigarillos, and binge drinking, representing over 700,000 U.S. youth.
Table 2.
Estimated hazard functions 1 (with 95% confidence intervals) of the age of initiation of each past 30-day polysubstance use outcome in PATH ¥ youth (2013–2019).
3.3. Crude and Adjusted Hazard Ratios of the Age of Initiation of Past 30-Day Polysubstance Use Outcomes
Table 3 presents the crude hazard ratios estimating differences in the age of initiation of each polysubstance use outcomes by sex, by race/ethnicity, and by ever use of other TPs. Table 3 also presents the adjusted hazard ratios (AHRs) estimating differences in the age of initiation of each polysubstance use outcome, while controlling for sex, race/ethnicity, and ever use of other TPs simultaneously. Hispanic youth were 43% less likely (AHR: 0.57; 95% CI: 0.41–0.80) and Non-Hispanic Black youth were 85% less likely (AHR: 0.15; 95% CI: 0.06–0.35) to initiate past 30-day use of cigarettes, e-cigarettes, and binge drinking at earlier ages compared to Non-Hispanic White youth. Hispanic youth were 48% (AHR: 0.52; 95% CI: 0.32–0.86) less likely, Non-Hispanic Black youth were 64% (AHR: 0.36; 95% CI: 0.14–0.91) less likely, and Non-Hispanic Other were 65% (AHR: 0.35; 95% CI: 0.13–0.96) less likely to initiate past 30-day use of cigarettes, cigarillos, and binge drinking at earlier ages compared to Non-Hispanic White youth. However, no statistical differences in initiating each past 30-day polysubstance use outcome were observed for sex in both crude and adjusted analyses.
Table 3.
Crude and adjusted hazard ratios (with 95% confidence intervals) for the age of initiation of past 30-day polysubstance use outcomes in PATH ¥ youth (2013–2019).
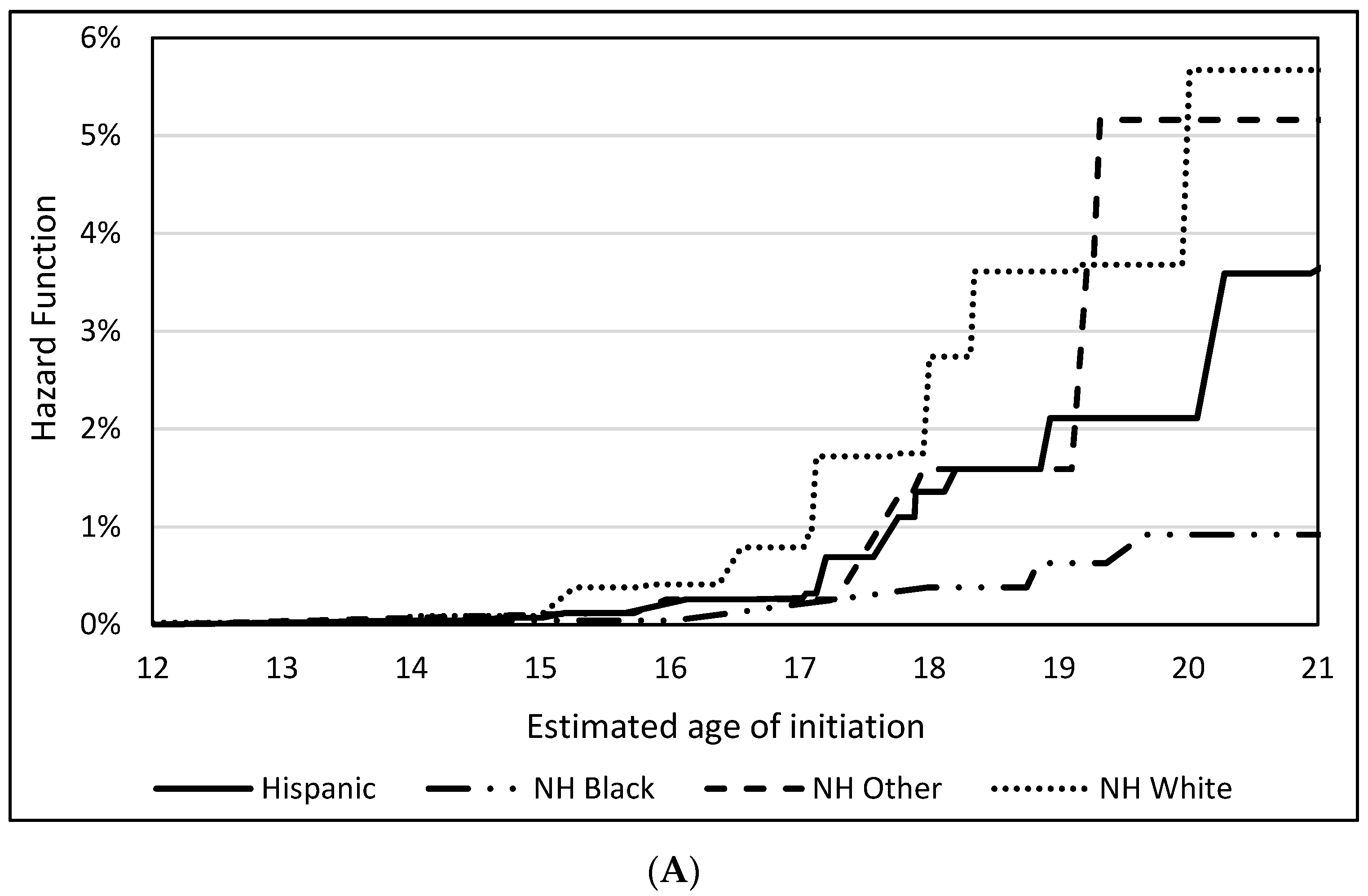
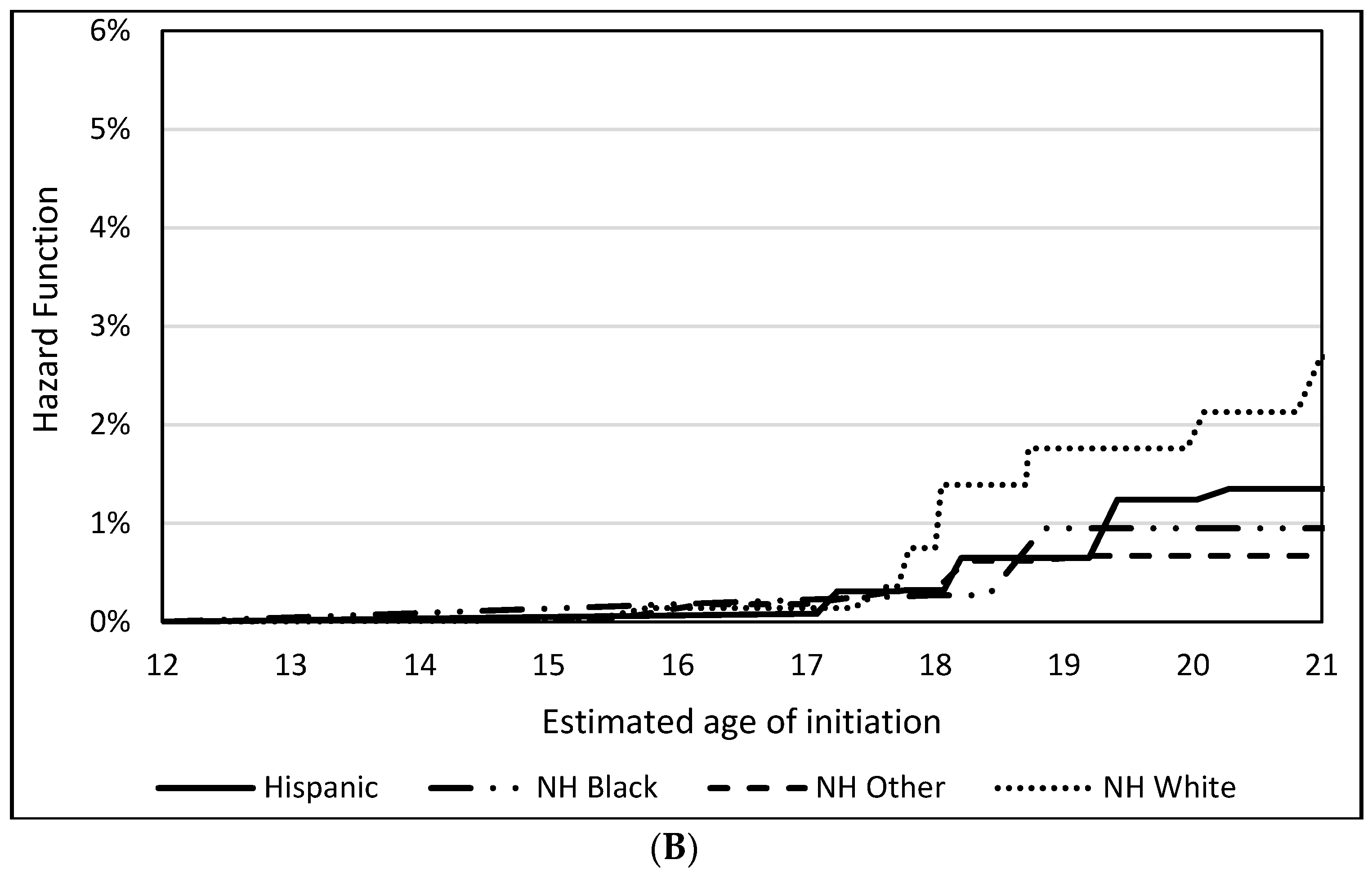
Figure 1 shows the hazard functions of the age of initiating each polysubstance use outcome stratified by race/ethnicity. Overall, Non-Hispanic White youth were estimated to initiate both past 30-day polysubstance use outcomes at earlier ages, only surpassed by Non-Hispanic Other youth between ages 19 and 20 for cigarettes, e-cigarettes, and binge drinking. However, by age 21, Non-Hispanic White youth were estimated to have the highest probability of initiation of past 30-day polysubstance use of cigarettes, e-cigarettes, and binge drinking (5.7%), followed by Non-Hispanic Other youth (5.2%), Hispanic youth (3.7%), and Non-Hispanic Black youth (0.9%). By age 21, 2.7% of Non-Hispanic White youth were estimated to initiate past 30-day polysubstance use of cigarettes, cigarillos, and binge drinking, followed by Hispanic youth (1.4%), Non-Hispanic Black youth (0.9%), and Non-Hispanic other youth (0.7%).
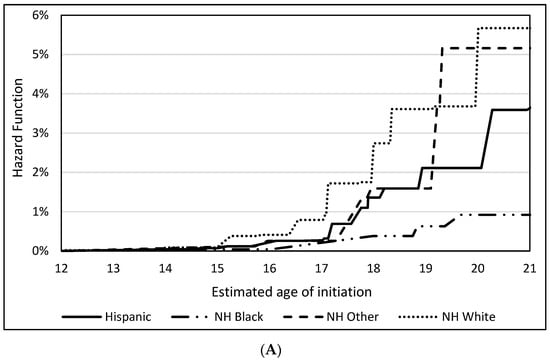
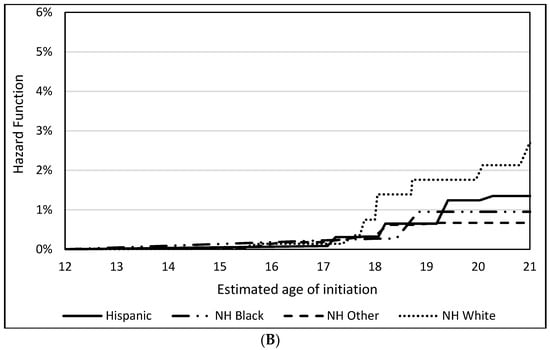
Figure 1.
Hazard functions of the age of initiation of past 30-day use of (A) cigarettes, e-cigarettes, and binge drinking and past 30-day use of (B) cigarettes, cigarillos, and binge drinking by race/ethnicity.
4. Discussion
This study is the first to prospectively estimate the age of initiation of past 30-day polysubstance use of cigarettes, e-cigarettes, and binge drinking, as well as the age of initiation of past 30-day polysubstance use of cigarettes, cigarillos, and binge drinking. Reporting past 30-day polysubstance use of three substances in the same wave of PATH is a risky behavior in youth and becomes even more problematic when this occurs at younger ages, despite the fact that it was illegal for youth to purchase TPs before 18 and alcohol before 21 years old. The Tobacco 21 Law went into effect in December 2019 [41], which did not affect our participants. While initiation of each polysubstance use outcome remained relatively low by age 20, the estimated percentages of initiation of past 30-day polysubstance use of cigarettes, e-cigarettes, and binge drinking represent over 1.56 million youth and past 30-day polysubstance use of cigarettes, cigarillos, and binge drinking represent over 700,000 youth, which is problematic. Adolescence represents a period of critical growth and development during which neurobiological, physical, emotional, and social changes occur in youth [42], and the use of these three substances has implications for these developments.
Our findings are similar to previous studies on the relationship between TP and alcohol use. The 2014 Monitoring the Future study reported the odds of initiating past 30-day alcohol use among those who were past 30-day poly-nicotine TP users as 19.7 (AOR: 13.6–28.5) for 8th and 10th graders and as 11.5 (AOR: 8.4–15.7) for 12th graders [43]. Our study prospectively followed-up never users while the previous study reported cross-sectional analyses which included users and non-users. Our study goes beyond this previous work by estimating the age when youth initiate past 30-day use of all three substances in the same PATH wave.
A study based on the 2003 National Youth Risk Behavior Survey that defined binge drinking as consuming more than five drinks in a row during the past 30-days found that among 12–20 year old respondents, 17.8% of 12–14 year olds, 28.9% of 15–17 year olds, and 38.7% of 18–20 year olds were binge drinkers [44]. Our results are similar to this study, finding that binge drinking is more common in 18+ year olds compared to 12–14 and 15–17 year olds [44]. This is concerning as a prior study suggests that binge drinking in late adolescence predicts binge drinking at ages 30–31 [45].
Our study found that Hispanic and Non-Hispanic Black youth had decreased risk of earlier ages of initiating past 30-day polysubstance use outcomes compared to Non-Hispanic White youth. This is consistent with the current literature finding that White high school students often report earlier initiation of alcohol use [32,46]. Similarly, data from nationally representative surveys found that Non-Hispanic White youth were more likely to initiate e-cigarette use, and had higher prevalence of exclusive, dual and poly tobacco use than youth of other racial/ethnic groups [47,48], which is in line with our findings. However, studies have not successfully documented possible reasons as to why this racial/ethnic difference occurs in e-cigarette use [49,50]. Future studies should investigate such factors to determine the reasons for this disparity. Our results found that Non-Hispanic Black youth are less likely to initiate past 30-day use of cigarettes, cigarillos, and binge drinking at earlier ages compared to Non-Hispanic White youth. In contrast, a recent study that found that Non-Hispanic White youth were less likely to initiate past 30-day use of cigarillos as a single TP at earlier ages than Non-Hispanic Black youth [25]. This inconsistency could arise from the confounding effects due to concurrent use of cigarettes and binge drinking, substances which studies have shown Non-Hispanic White youth initiate earlier [29,34,48].
Previous publications of PATH youth reported the age of initiation single TPs, including cigarettes [27], e-cigarettes [26], and cigar products [25], which found that males are more likely to initiate past 30-day use of cigarettes, e-cigarettes, or cigar products at earlier ages than females. This is contrary to our results where we did not observe differences in the age of initiating polysubstance use between males and females. The reasons for this are unclear and should be explored in future research, as other studies also have shown that males were more likely than females to engage in binge drinking [32] and that males are at higher risk of dual TP use compared to females [29].
There are many complications associated with dual tobacco use and binge drinking in youth, which are compounded the earlier that youth initiate use of these substances, such as drinking and driving [51], more frequent use of heroin and methamphetamines [51], risky sexual behavior [52], and alcohol poisoning [52], among others. A recent e-poster presentation at a 2021 Tobacco Regulatory Science meeting hosted by the National Institutes of Health argued for the necessity of communicating cancer risks associated with alcohol and tobacco use and showed that messages with images warning of the health risks of using both tobacco and alcohol are more effective than messages without images. This suggests that prevention and education programs that use messages containing images warning the health risks associated with using both tobacco and alcohol may be necessary [53].
Strengths of this study include the longitudinal prospective analysis of the age of initiation of past 30-day polysubstance use of three substances using a nationally representative sample across PATH waves 1–5. One of the limitations of our study is that we depended on self-reported data for the cigarette, e-cigarette, cigarillo, and binge drinking status to estimate the age of initiation. In addition, we use interval censoring survival analysis because asking participants the exact date they initiated all three substances is unrealistic. Another limitation is that due to the survey design of the cigar variables in PATH, it is not possible to separate blunt-only users. The variable that asks about blunt use asks about using traditional cigars, cigarillos, or filtered cigars as blunts in a single question. Then, past 30-day cigarillo use is asked without specifying if they are blunt users. However, considering that cigarillo users are still exposed to nicotine and tobacco toxicants even after replacing the tobacco in cigarillos with marijuana [54], the implications from this study should still stand.
5. Conclusions
In conclusion, this study prospectively estimates the age of initiating past 30-day use of (1) cigarettes, e-cigarettes, and binge drinking, and (2) cigarettes, cigarillos, and binge drinking, and identifies Non-Hispanic White youth as being at a higher risk of initiating the aforementioned polysubstance use at earlier ages in comparison to Hispanic youth or Non-Hispanic Black youth. This study provides interventionists and the public with evidence to identify the particular ages at which education campaigns may be most effective to prevent youth from initiating past 30-day polysubstance use and to target the specific racial/ethnic group that is the most vulnerable.
Author Contributions
Conceptualization, A.P. and B.C.; methodology, A.P. and B.C.; software, A.E.K.; validation, A.P. and A.E.K.; formal analysis, A.E.K., M.A.B. and B.C.; investigation, A.P., H.M.S.S., A.E.K. and M.A.B.; data curation, A.E.K.; writing—original draft preparation, A.P., A.E.K., M.A.B. and H.M.S.S.; writing—review and editing, A.P., A.E.K., M.A.B., H.M.S.S. and B.C.; supervision, A.P.; funding acquisition, A.P. All authors have read and agreed to the published version of the manuscript.
Funding
Funding for this study was provided by National Cancer Institute (NCI) and the FDA Center for Tobacco Products (CTP) Grant number [R01CA234205]. NCI and FDA Center for Tobacco Products had no role to in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
Institutional Review Board Statement
The University of Texas Health Center at Houston granted institutional review board approval (HSC-SPH-17-0368). This report followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for cohort studies.
Informed Consent Statement
Informed oral consent was obtained from the parents of the youth and youth provided oral assent.
Data Availability Statement
All the data from waves 1–5 are available from the Population Assessment of Tobacco and Health (PATH) Study [United States] Restricted-Use Files. Inter-university Consortium for Political and Social Research [distributor], https://doi.org/10.3886/ICPSR36231.v28, accessed on 20 November 2021. Researchers can apply for access to the restricted-use datasets from the Inter-university Consortium for Political and Social Research (ICPSR) at the University of Michigan. To access data in the Virtual Data Enclave (VDE), a Restricted Data Use Agreement (RDUA) must be established between the University of Michigan and the researcher’s institution. Data are provided via ICPSR’s VDE. For further information, please reference the VDE Guide to learn about the application process, about using the VDE, and how to request disclosure review of VDE output located here: https://www.icpsr.umich.edu/web/pages/NAHDAP/vde/index.html, accessed on 20 November 2021. Obtaining results using the restricted-use datasets requires a disclosure process with protocols set by ICPSR. When a researcher logs on to the VDE, a virtual machine is launched on the researcher’s own desktop but operates from a server at ICPSR. The virtual machine is isolated from the researcher’s physical desktop computer—users cannot download or upload files or parts of files from or to the VDE; print VDE contents to a printer; or email, copy, or otherwise move files in or out of the VDE computing environment, either accidentally or intentionally. Results are only disclosed by ICPSR after programs have been checked for accuracy and results have been replicated.
Conflicts of Interest
The authors declare no conflict of interest.
References
- National Cancer Institute at the National Institutes of Health. Cancer Causes and Prevention: Risk Factors: Tobacco. Available online: https://www.cancer.gov/about-cancer/causes-prevention/risk/tobacco (accessed on 27 March 2020).
- National Cancer Institute at the National Institutes of Health. Cancer Causes and Prevention: Risk Factors: Alcohol and Cancer Risk. Available online: https://www.cancer.gov/about-cancer/causes-prevention/risk/alcohol/alcohol-fact-sheet (accessed on 27 March 2020).
- Hashibe, M.; Brennan, P.; Chuang, S.C.; Boccia, S.; Castellsague, X.; Chen, C.; Curado, M.P.; Dal Maso, L.; Daudt, A.W.; Fabianova, E.; et al. Interaction between tobacco and alcohol use and the risk of head and neck cancer: Pooled analysis in the International Head and Neck Cancer Epidemiology Consortium. Cancer Epidemiol. Biomark. Prev. 2009, 18, 541–550. [Google Scholar] [CrossRef] [Green Version]
- Turati, F.; Garavello, W.; Tramacere, I.; Pelucchi, C.; Galeone, C.; Bagnardi, V.; Corrao, G.; Islami, F.; Fedirko, V.; Boffetta, P.; et al. A meta-analysis of alcohol drinking and oral and pharyngeal cancers: Results from subgroup analyses. Alcohol Alcohol. 2013, 48, 107–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohn, A.M.; Johnson, A.L.; Rose, S.W.; Pearson, J.L.; Villanti, A.C.; Stanton, C. Population-level patterns and mental health and substance use correlates of alcohol, marijuana, and tobacco use and co-use in US young adults and adults: Results from the population assessment for tobacco and health. Am. J. Addict. 2018, 27, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Nollen, N.L.; Ahluwalia, J.S.; Lei, Y.; Yu, Q.; Scheuermann, T.S.; Mayo, M.S. Adult Cigarette Smokers at Highest Risk for Concurrent Alternative Tobacco Product Use Among a Racially/Ethnically and Socioeconomically Diverse Sample. Nicotine Tob. Res. 2016, 18, 386–394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, G.; Mayer, M.E.; Barrington-Trimis, J.L.; McConnell, R.; Leventhal, A.M.; Krishnan-Sarin, S. Longitudinal associations between use and co-use of cigars and cigarettes: A pooled analysis of three adolescent cohorts. Drug Alcohol Depend. 2019, 201, 45–48. [Google Scholar] [CrossRef]
- Cho, J.; Goldenson, N.I.; Stone, M.D.; McConnell, R.; Barrington-Trimis, J.L.; Chou, C.P.; Sussman, S.Y.; Riggs, N.R.; Leventhal, A.M. Characterizing Polytobacco Use Trajectories and Their Associations with Substance Use and Mental Health Across Mid-Adolescence. Nicotine Tob. Res. 2018, 20, S31–S38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohn, A.; Cobb, C.O.; Niaura, R.S.; Richardson, A. The Other Combustible Products: Prevalence and Correlates of Little Cigar/Cigarillo Use Among Cigarette Smokers. Nicotine Tob. Res. 2015, 17, 1473–1481. [Google Scholar] [CrossRef] [PubMed]
- Shah, V.; Watson, J. Relationship between Substance Use and Socioeconomic Variables in Pennsylvania Adolescents: 2009–2017. Subst. Use Misuse 2020, 55, 1856–1866. [Google Scholar] [CrossRef] [PubMed]
- Kandel, D.; Kandel, E. The Gateway Hypothesis of substance abuse: Developmental, biological and societal perspectives. Acta Paediatr. 2015, 104, 130–137. [Google Scholar] [CrossRef]
- DuRant, R.H.; Smith, J.A.; Kreiter, S.R.; Krowchuk, D.P. The relationship between early age of onset of initial substance use and engaging in multiple health risk behaviors among young adolescents. Arch. Pediatr. Adolesc. Med. 1999, 153, 286–291. [Google Scholar] [CrossRef] [Green Version]
- U.S. Department of Health and Human Services, Office of the U.S Surgeon General, the U.S. Centers for Disease Control and Prevention and Office on Smoking and Health. Know the Risks: E-Cigarettes and Young People. Available online: https://e-cigarettes.surgeongeneral.gov/#:~:text=E%2Dcigarettes%20are%20considered%20tobacco,nicotine%2C%20which%20comes%20from%20tobacco) (accessed on 20 November 2021).
- Wang, T.W.; Gentzke, A.S.; Creamer, M.R.; Cullen, K.A.; Holder-Hayes, E.; Sawdey, M.D.; Anic, G.M.; Portnoy, D.B.; Hu, S.; Homa, D.M.; et al. Tobacco Product Use and Associated Factors among Middle and High School Students—United States, 2019. MMWR Surveill Summ. 2019, 68, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Stanton, C.A.; Sharma, E.; Seaman, E.L.; Kasza, K.A.; Edwards, K.C.; Halenar, M.J.; Taylor, K.A.; Day, H.; Anic, G.; Hull, L.C.; et al. Initiation of Any Tobacco and Five Tobacco Products across 3 Years among Youth, Young Adults and Adults in the USA: Findings from the PATH Study Waves 1–3 (2013–2016). Tob Control. 2020, 29, s178–s190. [Google Scholar] [CrossRef] [PubMed]
- Kasza, K.A.; Ambrose, B.K.; Conway, K.P.; Borek, N.; Taylor, K.; Goniewicz, M.L.; Cummings, K.M.; Sharma, E.; Pearson, J.L.; Green, V.R.; et al. Tobacco-Product Use by Adults and Youths in the United States in 2013 and 2014. N. Engl. J. Med. 2017, 376, 342–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, C.M.; Rostron, B.L.; Chang, J.T.; Corey, C.G.; Kimmel, H.L.; Sosnoff, C.S.; Goniewicz, M.L.; Edwards, K.C.; Hatsukami, D.K.; Wang, Y.; et al. Biomarkers of Exposure among U.S. Adult Cigar Smokers: Population Assessment of Tobacco and Health (PATH) Study Wave 1 (2013–2014). Cancer Epidemiol. Prev. Biomark. 2019, 28, 943–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Kettermann, A.; Rostron, B.L.; Day, H.R. Biomarkers of Exposure among U.S. Cigar Smokers: An Analysis of 1999-2012 National Health and Nutrition Examination Survey (NHANES) Data. Cancer Epidemiol. Prev. Biomark. 2014, 23, 2906–2915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snell, L.M.; Barnes, A.J.; Nicksic, N.E. A Longitudinal Analysis of Nicotine Dependence and Transitions from Dual Use of Cigarettes and Electronic Cigarettes: Evidence from Waves 1–3 of the PATH Study. J. Stud. Alcohol Drugs 2020, 81, 595–603. [Google Scholar] [CrossRef]
- Osei, A.D.; Mirbolouk, M.; Orimoloye, O.A.; Dzaye, O.; Uddin, S.M.I.; Benjamin, E.J.; Hall, M.E.; DeFilippis, A.P.; Stokes, A.; Bhatnagar, A.; et al. Association Between E-Cigarette Use and Cardiovascular Disease Among Never and Current Combustible-Cigarette Smokers. Am. J. Med. 2019, 132, 949–954.e942. [Google Scholar] [CrossRef]
- Quigley, J.; Committee on Substance, U.S.E. and Prevention. Alcohol Use by Youth. Pediatrics 2019, 144, e20191357. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Cigars: Health Effects. Available online: https://www.cdc.gov/tobacco/data_statistics/fact_sheets/tobacco_industry/cigars/index.htm#health-effects (accessed on 8 February 2021).
- Centers for Disease Control and Prevention. Smoking & Tobacco Use: Health Effects. Available online: https://www.cdc.gov/tobacco/basic_information/health_effects/index.htm#:~:text=Smoking%20causes%20cancer%2C%20heart%20disease,immune%20system%2C%20including%20rheumatoid%20arthritis (accessed on 10 February 2021).
- Centers for Disease Control and Prevention. Alcohol Use and Your Health. Available online: https://www.cdc.gov/alcohol/fact-sheets/alcohol-use.htm (accessed on 9 February 2021).
- Chen, B.; Sterling, K.L.; Bluestein, M.A.; Kuk, A.E.; Harrell, M.B.; Perry, C.L.; Pérez, A. Age of initiation of cigarillos, filtered cigars and/or traditional cigars among youth: Findings from the Population Assessment of Tobacco and Health (PATH) study, 2013–2017. PLoS ONE 2020, 15, e0243372. [Google Scholar] [CrossRef]
- Pérez, A.; Bluestein, M.; Chen, B.; Perry, C.L.; Harrell, M.B. Prospectively Estimating the Age of Initiation of E-cigarettes among U.S. youth: Findings from the Population Assessment of Tobacco and Health (PATH) Study, 2013–2017. J. Biom. Biostat. 2020, 11. [Google Scholar] [CrossRef]
- Pérez, A.; N’Hpang, R.S.; Callahan, E.; Bluestein, M.; Kuk, A.E.; Chen, B.; Perry, C.L.; Harrell, M.B. Age at Initiation of Cigarette Use in a Nationally Representative Sample of US Youth, 2013–2017. JAMA Netw. Open. 2021, 4, e210218. [Google Scholar] [CrossRef] [PubMed]
- Sharapova, S.; Reyes-Guzman, C.; Singh, T.; Phillips, E.; Marynak, K.L.; Agaku, I. Age of tobacco use initiation and association with current use and nicotine dependence among US middle and high school students, 2014–2016. Tob. Control 2020, 29, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; Gray, T.R.; Martinez, D.J.; Curry, L.E.; Horn, K.A. Risk Profiles of Youth Single, Dual, and Poly Tobacco Users. Nicotine Tob. Res. 2016, 18, 1614–1621. [Google Scholar] [CrossRef] [PubMed]
- Osman, A.; Kowitt, S.D.; Ranney, L.M.; Heck, C.; Goldstein, A.O. Trends and Racial Disparities in Mono, Dual, and Poly Use of Tobacco Products Among Youth. Nicotine Tob. Res. 2018, 20, S22–S30. [Google Scholar] [CrossRef] [PubMed]
- McCabe, S.E.; West, B.T.; Veliz, P.; Boyd, C.J. E-cigarette Use, Cigarette Smoking, Dual Use, and Problem Behaviors Among U.S. Adolescents: Results from a National Survey. J. Adolesc. Health 2017, 61, 155–162. [Google Scholar] [CrossRef]
- Patrick, M.E.; Schulenberg, J.E.; Martz, M.E.; Maggs, J.L.; O’Malley, P.M.; Johnston, L.D. Extreme binge drinking among 12th-grade students in the United States: Prevalence and predictors. JAMA Pediatr. 2013, 167, 1019–1025. [Google Scholar] [CrossRef] [Green Version]
- Hyland, A.; Ambrose, B.K.; Conway, K.P.; Borek, N.; Lambert, E.; Carusi, C.; Taylor, K.; Crosse, S.; Fong, G.T.; Cummings, K.M.; et al. Design and methods of the Population Assessment of Tobacco and Health (PATH) Study. Tob. Control 2017, 26, 371–378. [Google Scholar] [CrossRef]
- National Addiction & HIV Data Archive Program. Population Assessment of Tobacco and Health (PATH) Study [United States] Restricted-Use Files (ICPSR 36231). Inter-University Consortium for Political and Social Research [Distributor]. 2021. Available online: https://doi.org/10.3886/ICPSR36231.v26 (accessed on 28 July 2021).
- National Institute on Alcohol Abuse and Alcoholism. Underage Drinking. Available online: https://www.niaaa.nih.gov/publications/brochures-and-fact-sheets/underage-drinking (accessed on 30 March 2020).
- US Department of Health and Human Services. Preventing Tobacco Use among Youth and Young Adults: A Report of the Surgeon General; US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2012.
- Judkins, D.R. Fay’s method for variance estimation. J. Off. Stat. 1990, 6, 223–239. [Google Scholar]
- Royston, P.; Parmar, M.K. Flexible parametric proportional-hazards and proportional-odds models for censored survival data, with application to prognostic modelling and estimation of treatment effects. Stat. Med. 2002, 21, 2175–2197. [Google Scholar] [CrossRef]
- Goodall, R.L.; Dunn, D.T.; Babiker, A.G. Interval-censored survival time data: Confidence intervals for the non-parametric survivor function. Stat. Med. 2004, 23, 1131–1145. [Google Scholar] [CrossRef] [PubMed]
- Finkelstein, D.M. A proportional hazards model for interval-censored failure time data. Biometrics 1986, 42, 845–854. [Google Scholar] [CrossRef]
- U.S. Food & Drug Administration. Tobacco 21. Available online: https://www.fda.gov/tobacco-products/retail-sales-tobacco-products/tobacco-21 (accessed on 20 December 2020).
- Larsen, B.; Luna, B. Adolescence as a neurobiological critical period for the development of higher-order cognition. Neurosci. Biobehav. Rev. 2018, 94, 179–195. [Google Scholar] [CrossRef]
- Richter, L.; Pugh, B.S.; Smith, P.H.; Ball, S.A. The co-occurrence of nicotine and other substance use and addiction among youth and adults in the United States: Implications for research, practice, and policy. Am. J. Drug Alcohol Abus. 2017, 43, 132–145. [Google Scholar] [CrossRef]
- Miller, J.W.; Naimi, T.S.; Brewer, R.D.; Jones, S.E. Binge Drinking and Associated Health Risk Behaviors Among High School Students. Pediatrics 2007, 119, 76–85. [Google Scholar] [CrossRef]
- McCarty, C.A.; Ebel, B.E.; Garrison, M.M.; DiGiuseppe, D.L.; Christakis, D.A.; Rivara, F.P. Continuity of Binge and Harmful Drinking from Late Adolescence to Early Adulthood. Pediatrics 2004, 114, 714. [Google Scholar] [CrossRef]
- Terry-McElrath, Y.M.; Patrick, M.E. U.S. adolescent alcohol use by race/ethnicity: Consumption and perceived need to reduce/stop use. J. Ethn. Subst. Abus. 2020, 19, 3–27. [Google Scholar] [CrossRef]
- Cho, B.; Hirschtick, J.L.; Usidame, B.; Meza, R.; Mistry, R.; Land, S.R.; Levy, D.T.; Holford, T.; Fleischer, N.L. Sociodemographic Patterns of Exclusive, Dual, and Polytobacco Use Among U.S. High School Students: A Comparison of Three Nationally Representative Surveys. J. Adolesc. Health 2021, 68, 750–757. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Yu, B.; Wang, Y. Initiation of Electronic Cigarette Use by Age Among Youth in the U.S. Am. J. Prev. Med. 2017, 53, 396–399. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, J.P. Sensation seeking and adolescent e-cigarette use. J. Subst. Use 2021, 26, 542–548. [Google Scholar] [CrossRef]
- Tsai, J.; Walton, K.; Coleman, B.N.; Sharapova, S.R.; Johnson, S.E.; Kennedy, S.M.; Caraballo, R.S. Reasons for Electronic Cigarette Use Among Middle and High School Students—National Youth Tobacco Survey, United States, 2016. Morb. Mortal. Wkly. Rep. 2018, 67, 196–200. [Google Scholar] [CrossRef]
- D’Amico, E.J.; Metrik, J.; McCarthy, D.M.; Frissell, K.C.; Applebaum, M.; Brown, S.A. Progression into and out of binge drinking among high school students. Psychol. Addict. Behav. 2001, 15, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Substance Abuse and Health Services Administration. Report to Congress on the Prevention and Reduction of Underage Drinking; U.S. Department of Health and Human Services: Washington, DC, USA, 2012.
- Cox, M.; Jarman, K.L.; Kowitt, S.D.; Kong, A.Y.; Goldstein, A.O.; Ross, J.C.; Ranney, L.M. Dual Health Messages for Tobacco and Alcohol Co-Use. e-Poster presented at: Fall 2021 National Institute of Health Tobacco Regulatory Science Meeting. 2021. Available online: https://westat.confex.com/westat/trs21/general/eposterview.cgi?eposterid=88 (accessed on 20 October 2021).
- Peters, E.N.; Schauer, G.L.; Rosenberry, Z.R.; Pickworth, W.B. Does marijuana “blunt” smoking contribute to nicotine exposure?: Preliminary product testing of nicotine content in wrappers of cigars commonly used for blunt smoking. Drug Alcohol Depend. 2016, 168, 119–122. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).