
Inconvenience of Living Place Affects Individual HbA1c Level in a Rural Area in Japan: Shimane CoHRE Study

Abstract
:1. Introduction
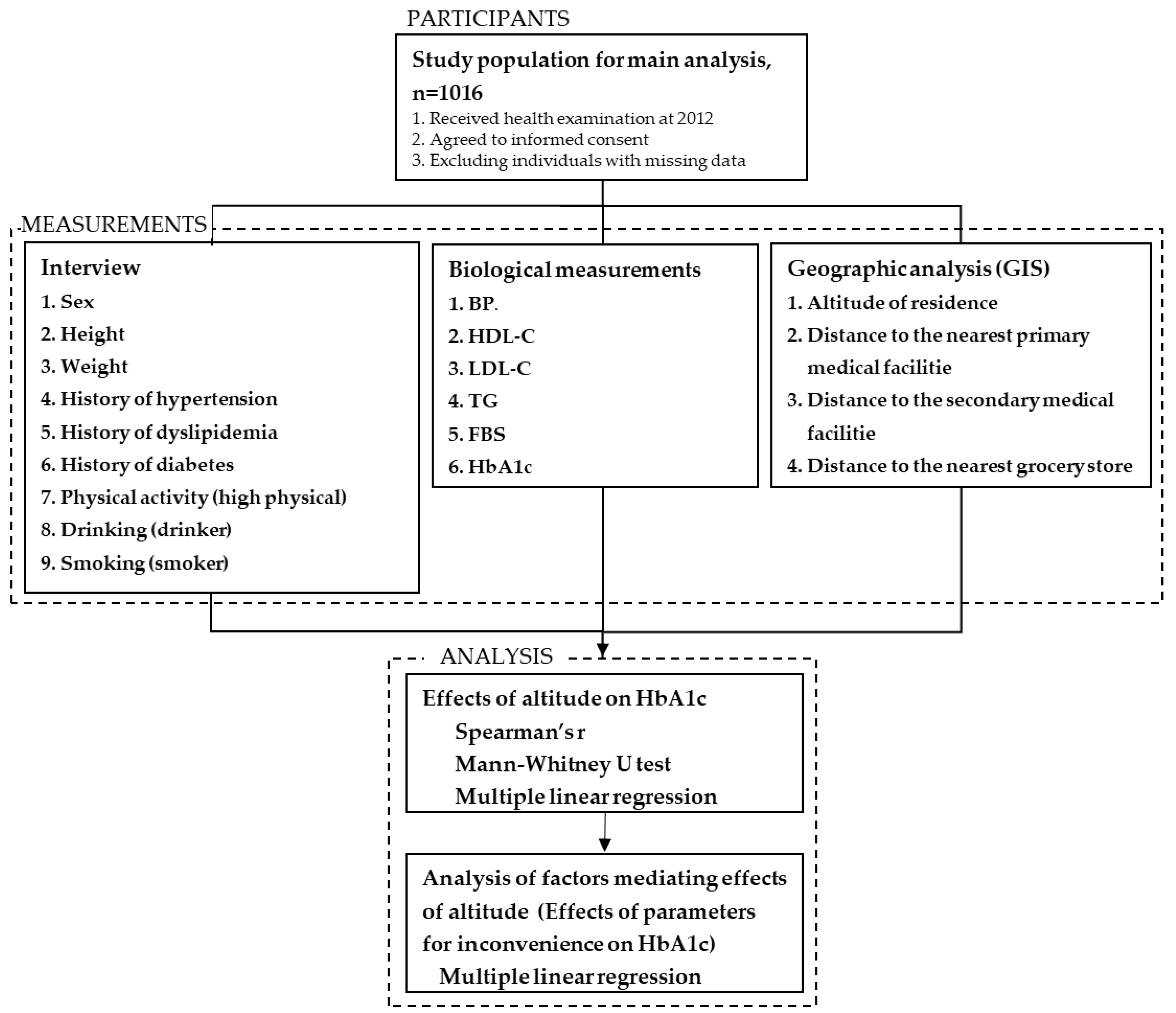
2. Materials and Methods
2.1. Participants
2.2. Measurements
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Report on Diabetes. 2016. Available online: http://apps.who.int/iris/bitstream/handle/10665/204871/9789241565257_eng.pdf?sequence=1&isAllowed=y (accessed on 31 August 2018).
- Ministry of Health, Labor and Welfare. Section of the National Health and Nutrition Survey. 2018. Available online: https://www.mhlw.go.jp/file/04-Houdouhappyou-10904750-Kenkoukyoku-Gantaisakukenkouzoushinka/kekkagaiyou_7.pdf (accessed on 31 August 2018).
- World Health Organization. Diabetes. 2020. Available online: https://www.who.int/health-topics/diabetes#tab=tab_1 (accessed on 3 June 2020).
- Ogurtsova, K.; da Rocha Fernandes, J.D.; Huang, Y.; Linnenkamp, U.; Guariguata, L.; Cho, N.H.; Cavan, D.; Shaw, J.; Makaroff, L.E. IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res. Clin. Pract. 2017, 128, 40–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deshpande, A.D.; Harris-Hayes, M.; Schootman, M. Epidemiology of Diabetes and Diabetes-Related Complications. Phys. Ther. 2008, 88, 1254–1264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.; Ding, Y.; Tanaka, Y.; Zhang, W. Risk factors contributing to type 2 diabetes and recent advances in the treatment and prevention. Int. J. Med. Sci. 2014, 11, 1185–1200. [Google Scholar] [CrossRef] [Green Version]
- International Diabetes Federation. IDF Diabetes Atlas 9th Edition 2019. 2019. Available online: https://idf.org/e-library/epidemiology-research/diabetes-atlas/159-idf-diabetes-atlas-ninth-edition-2019.html (accessed on 8 May 2020).
- Mezuk, B.; Li, X.; Cederin, K.; Rice, K.; Sundquist, J.; Sundquist, K. Beyond Access: Characteristics of the Food Environment and Risk of Diabetes. Am. J. Epidemiol. 2016, 183, 1129–1137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morland, B.K.; Evenson, R.K. Obesity prevalence and the local food environment. Health Place 2009, 15, 491–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dendup, T.; Feng, X.; Clingan, S.; Astell-Burt, T. Environmental Risk Factors for Developing Type 2 Diabetes Mellitus: A Systematic Review. Int. J. Environ. Res. Public Health 2018, 15, 78. [Google Scholar] [CrossRef] [Green Version]
- Schobersberger, W.; Schmid, P.; Lechleitner, M.; Von Duvillard, S.P.; Hortnagl, H.; Gunga, H.C.; Klingler, A.; Fries, D.; Kirsch, K.; Spiesberger, R.; et al. Austrian Moderate Altitude Study 2000 (AMAS 2000):The effects of moderate altitude (1700 m) on cardiovascular and metabolic variables in patients with metabolic syndrome. Eur. J. Appl. Physiol. 2003, 88, 506–514. [Google Scholar] [CrossRef]
- Lee, W.C.; Chen, J.J.; Ho, H.Y.; Hou, C.W.; Liang, M.P.; Shen, Y.W.; Kuo, G.H. Short-term altitude mountain living improves glycemic control. High. Alt. Med. Biol. 2003, 4, 81–91. [Google Scholar] [CrossRef]
- Kelly, K.R.; Williamson, D.L.; Fealy, C.E.; Kriz, D.A.; Krishnan, R.K.; Huang, H.; Ahn, J.; Loomis, J.L.; Kirwan, J.P. Acute altitude-induced hypoxia suppresses plasma glucose and leptin in healthy humans. Metabolism 2010, 59, 200–205. [Google Scholar] [CrossRef] [Green Version]
- Hamano, T.; Kimura, Y.; Takeda, M.; Yamasaki, M.; Nabika, T.; Shiwaku, K. Is Location Associated with High Risk of Hypertension? Shimane COHRE Study. Am. J. Hypertens. 2012, 25, 784–788. [Google Scholar] [CrossRef] [Green Version]
- Ferdaus, S.I.; Kohno, K.; Hamano, T.; Takeda, M.; Yamasaki, M.; Isomura, M.; Shiwaku, K.; Nabika, T. Altitudes of residential areas affect salt intake in a rural area in Japan: A Shimane CoHRE Study. Hypertens. Res. 2015, 38, 895–898. [Google Scholar] [CrossRef] [PubMed]
- Yamasaki, M.; Yano, S.; Takeda, M.; Abe, T.; Hamano, T.; Nabika, T.; Shiwaku, K. Prevalence of lifestyle-related chronic disease among agricultural and non-agricultural workers in rural areas of Japan: The Shimane CoHRE study. J. Rural. Med. 2020, 15, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohno, K.; Niihara, H.; Hamano, T.; Takeda, M.; Nakagawa, Y.; Shiwaku, K.; Zöller, B.; Nabika, T.; Li, X.; Sundquist, K.; et al. J-curve Association Between Alcohol Intake and Varicose Veins in Japan: The Shimane CoHRE Study. J. Dermatol. 2019, 46, 902–906. [Google Scholar] [CrossRef] [PubMed]
- Hamano, T.; Takeda, M.; Sundquist, K.; Nabika, T. Geographic elevation, car driving, and depression among elderly residents in rural areas: Shimane CoHRE Study. Int. J. Environ. Res. Public Health 2016, 13, 738. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Takeda, M.; Hamano, T.; Kijima, T.; Yamasaki, M.; Isomura, M.; Yano, S.; Shiwaku, K.; Nabika, T. Effect of salt intake on blood pressure in patients receiving antihypertensive therapy: Shimane CoHRE Study. Eur. J. Intern. Med. 2016, 28, 70–73. [Google Scholar] [CrossRef]
- Wada, M.; Yano, S.; Hamano, T.; Nabika, T.; Kumakura, S. Effect of serum cholesterol on insulin secretory capacity: Shimane CoHRE Study. PLoS ONE 2016, 11, e0149452. [Google Scholar] [CrossRef] [Green Version]
- Takeda, M.; Hamano, T.; Kohno, K.; Yano, S.; Shiwaku, K.; Nabika, T. Association between geographic elevation, bone status, and exercise habits: The Shimane CoHRE Study. Int. J. Environ. Res. Public Health 2015, 12, 7392–7399. [Google Scholar] [CrossRef] [Green Version]
- Yano, S.; Nagai, A.; Isomura, M.; Yamasaki, M.; Kijima, T.; Takeda, M.; Hamano, T.; Nabika, T. Relationship between blood myostatin levels and kidney function: Shimane CoHRE Study. PLoS ONE 2015, 10, e0141035. [Google Scholar] [CrossRef]
- Hamano, T.; Onoda, K.; Takeda, M.; Sundquist, K.; Yamaguchi, S.; Nabika, T. Geographic Elevation and Cognitive Function Among Elderly Residents in Rural Mountainous Areas: Shimane CoHRE Study. Int J. Environ. Res. Public Health 2015, 12, 13365–13371. [Google Scholar] [CrossRef] [Green Version]
- Hamano, T.; Tominaga, K.; Takeda, M.; Sundquist, K.; Nabika, T. Accessible Transportation, Geographic Elevation, and Masticatory Ability Among Elderly Residents of a Rural Area. Int. J. Environ. Res. Public Health 2015, 12, 7199–7207. [Google Scholar] [CrossRef] [Green Version]
- Mortimer, E.A., Jr.; Monson, R.R.; MacMahon, B. Reduction in mortality from coronary heart disease in men residing at high altitude. N. Engl. J. Med. 1977, 296, 581–585. [Google Scholar] [CrossRef] [PubMed]
- Aryal, N.; Weatherall, M.; Bhatta, Y.K.D.; Mann, S. Blood pressure and hypertension in people living at high altitude in Nepal. Hypertens. Res. 2019, 42, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Villanueva, K.; Knuiman, M.; Koohsari, M.J.; Hickey, S.; Foster, S.; Badland, H.; Nathan, A.; Bull, F.C.; Giles-Corti, B. People living in hilly residential areas in metropolitan Perth have less diabetes: Spurious association or important environmental determinant? Int. J. Health Geogr. 2013, 12, 59. [Google Scholar] [CrossRef] [Green Version]
- Fujiwara, T.; Takamoto, I.; Amemiya, A.; Hanazato, M.; Suzuki, N.; Nagamine, Y.; Sasaki, Y.; Tani, Y.; Yazawa, A.; Inoue, Y.; et al. Is a hilly neighborhood environment associated with diabetes mellitus among older people? results from the JAGES 2010 study. Soc. Sci. Med. 2017, 182, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Ferrer, H.B.; Cooper, A.; Audrey, S. Associations of mode of travel to work with physical activity, and individual, interpersonal, organizational, and environmental characteristics. J. Transp. Health 2018, 9, 45–55. [Google Scholar] [CrossRef]
- Takeda, M.; Hamano, T.; Kimura, Y.; Yamasaki, M.; Shiwaku, K. Factors Relating Utilization of Health Care Facilities in Rural Mountainous Region. J. Jpn. Assoc. Rural Med. 2014, 62, 929–940. [Google Scholar]
- Okuyama, K.; Akai, K.; Kijima, T.; Abe, T.; Isomura, M.; Nabika, T. Effect of Geographic Accessibility to Primary Care on Treatment Status of Hypertension. PLoS ONE 2019, 14, e0213098. [Google Scholar] [CrossRef]
- Ministry of Health, Labor and Welfare. Guidelines for Building a Medical System for Diabetes. 2017. Available online: https://www.mhlw.go.jp/file/06-Seisakujouhou-10800000-Iseikyoku/0000159904.pdf (accessed on 30 July 2020).
- Spence, J.C.; Cutumisu, N.; Edwards, J.; Raine, K.D.; Smoyer-Tomic, K. Relation between local food environments and obesity among adults. BMC Public Health 2009, 9, 192. [Google Scholar] [CrossRef] [Green Version]
- Choi, Y.; Suzuki, T. A Study on Shopping Behaviors for Groceries and Awareness on Convenience of Elderly People. Pap. City Plan. 2012, 47, 271–276. [Google Scholar]
- Hanibuchi, T.; Kondo, K.; Nakaya, T.; Nakade, M.; Ojima, T.; Hirai, H.; Kawachi, I. Neighborhood Food Environment and Body Mass Index Among Japanese Older Adults: Results from the Aichi Gerontological Evaluation Study (AGES). Int. J. Health Geogr. 2011, 10, 43. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Quartile 1 | Quartile 2 | Quartile 3 | Quartile 4 | p | Effect Size | |
|---|---|---|---|---|---|---|
| Number | 262 | 247 | 250 | 257 | ||
| Altitude, m | 38 (38, 39) | 53 (52, 54) | 123 (118, 128) | 304 (294, 314) | p < 0.001 | - |
| Age, years | 71 (70, 72) | 70 * vs. 4 (69, 71) | 70 (69, 71) | 71 (70, 72) | 0.01 | 0.011 b |
| Sex, % male | 37.4 | 38.1 | 41.6 | 41.6 | 0.65 | 0.04 c |
| BMI, kg/m2 | 22.2 (21.8, 22.6) | 22.2 (21.8, 22.7) | 21.9 (21.5, 22.2) | 22.5 (22.2, 22.9) | 0.09 | 0.006 b |
| SBP, mmHg | 129 (127, 131) | 128 (126, 130) | 127 (125, 129) | 128 (126, 130) | 0.78 | 0.001 b |
| DBP, mmHg | 77 (76, 79) | 78 (76, 79) | 76 (75, 78) | 77 (76, 79) | 0.49 | 0.002 b |
| Antihypertensive drug, % yes | 35.9 | 32.8 | 38.4 | 43.6 | 0.08 | 0.081 c |
| HDL-C, mg/dL | 66 (64, 68) | 64 (62, 66) | 66 (64, 68) | 63 (61, 65) | 0.14 | 0.005 b |
| LDL-C, mg/dL | 123 (119, 126) | 124 (120, 127) | 118 (115, 122) | 121 (118, 125) | 0.17 | 0.005 b |
| TG a, mg/dL | 85.4 (81.3, 89.7) | 89.1 (84.3, 94.2) | 83.7 (79.5, 88.1) | 83.4 (79.3, 87.8) | 0.26 | 0.004 b |
| Antihyperlipidemic drug, % yes | 23.3 | 17.8 | 18.8 | 21.4 | 0.41 | 0.054 c |
| HbA1c a, % | 5.32 (5.27, 5.37) | 5.35 (5.30, 5.41) | 5.39 (5.33, 5.44) | 5.48 * vs. 1, 2 (5.43, 5.54) | p < 0.001 | 0.019 b |
| Antidiabetic drugs, % yes | 4.6 | 3.6 | 5.6 | 5.4 | 0.72 | 0.036 c |
| Activity, % high activity | 47.3 | 46.6 | 48.0 | 50.6 | 0.82 | 0.03 c |
| Drinking, % yes | 44.7 | 42.3 | 54.0 | 47.7 | 0.05 | 0.087 c |
| Smoking, % yes | 5.3 | 6.5 | 4.0 | 5.4 | 0.67 | 0.039 c |
| Driving, % yes | 67.9 | 72.0 | 76.8 | 67.3 | 0.07 | 0.083 c |
| ρ or Z * | p | |
|---|---|---|
| Age | −0.02 | 0.55 |
| Sex, M vs. F | −1.00 | 0.32 |
| BMI | 0.10 | <0.001 |
| SBP | 0.00 | 0.99 |
| DBP | −0.03 | 0.38 |
| HDL-C | −0.15 | <0.001 |
| LDL-C | 0.05 | 0.10 |
| log TG | 0.11 | <0.001 |
| Smoking, Y vs. N | −0.50 | 0.62 |
| Drinking, Y vs. N | −1.40 | 0.16 |
| High physical activity, Y vs. N | −0.68 | 0.50 |
| Driving, Y vs. N | −0.19 | 0.85 |
| Altitude | 0.16 | <0.001 |
| (A) A model including altitude | |||||
| B | SE | Standardized | t | p | |
| β | |||||
| Age, per 10 years | 0.0001 | 0.002 | 0.002 | 0.07 | 0.94 |
| Sex, M vs. F | 0.002 | 0.002 | 0.03 | 0.81 | 0.42 |
| BMI | 0.001 | 0.0004 | 0.11 | 3.38 | 0.001 |
| HDL-C | −0.0001 | 0.0001 | −0.07 | −1.80 | 0.07 |
| log TG | 0.014 | 0.007 | 0.07 | 1.98 | 0.05 |
| Altitude, quartile | 0.004 | 0.001 | 0.13 | 4.23 | <0.001 |
| (B) A model including distance to primary medical facilities | |||||
| B | SE | Standardized | t | p | |
| β | |||||
| Age, per 10 years | 0.0001 | 0.002 | 0.003 | 0.10 | 0.92 |
| Sex, M vs. F | 0.002 | 0.002 | 0.03 | 0.79 | 0.43 |
| BMI | 0.001 | 0.0004 | 0.12 | 3.49 | 0.001 |
| HDL-C | −0.0002 | 0.0001 | −0.07 | −1.99 | 0.05 |
| log TG | 0.012 | 0.007 | 0.06 | 1.68 | 0.09 |
| Distance to the nearest primary medical facility | 0.0003 | 0.001 | 0.02 | 0.49 | 0.63 |
| (C) A model including distance to secondary medical facilities | |||||
| B | SE | Standardized | t | p | |
| β | |||||
| Age, per 10 years | −0.0002 | 0.002 | −0.004 | −0.14 | 0.89 |
| Sex, M vs. F | 0.002 | 0.002 | 0.02 | 0.79 | 0.43 |
| BMI | 0.001 | 0.0004 | 0.11 | 3.17 | 0.002 |
| HDL-C | −0.0002 | 0.0001 | −0.07 | −1.94 | 0.05 |
| log TG | 0.014 | 0.007 | 0.07 | 1.99 | 0.05 |
| Distance to the nearest secondary medical facility | 0.001 | 0.0002 | 0.17 | 5.70 | <0.001 |
| (D) A model including distance to grocery stores | |||||
| B | SE | Standardized | t | p | |
| β | |||||
| Age, per 10 years | −0.0004 | 0.002 | −0.01 | −0.22 | 0.83 |
| Sex, M vs. F | 0.003 | 0.003 | 0.04 | 0.97 | 0.33 |
| BMI | 0.001 | 0.0005 | 0.08 | 1.97 | 0.05 |
| HDL-C | −0.0002 | 0.0001 | −0.11 | −2.45 | 0.01 |
| log TG | 0.009 | 0.008 | 0.05 | 1.06 | 0.29 |
| Distance to the nearest grocery store | −0.0002 | 0.0004 | −0.02 | −0.61 | 0.54 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fukuoka, R.; Takeda, M.; Abe, T.; Yamasaki, M.; Kimura, S.; Okuyama, K.; Isomura, M.; Nabika, T. Inconvenience of Living Place Affects Individual HbA1c Level in a Rural Area in Japan: Shimane CoHRE Study. Int. J. Environ. Res. Public Health 2021, 18, 1147. https://doi.org/10.3390/ijerph18031147
Fukuoka R, Takeda M, Abe T, Yamasaki M, Kimura S, Okuyama K, Isomura M, Nabika T. Inconvenience of Living Place Affects Individual HbA1c Level in a Rural Area in Japan: Shimane CoHRE Study. International Journal of Environmental Research and Public Health. 2021; 18(3):1147. https://doi.org/10.3390/ijerph18031147
Chicago/Turabian StyleFukuoka, Rie, Miwako Takeda, Takafumi Abe, Masayuki Yamasaki, Shinji Kimura, Kenta Okuyama, Minoru Isomura, and Toru Nabika. 2021. "Inconvenience of Living Place Affects Individual HbA1c Level in a Rural Area in Japan: Shimane CoHRE Study" International Journal of Environmental Research and Public Health 18, no. 3: 1147. https://doi.org/10.3390/ijerph18031147