
Higher Prevalence of Dementia but No Change in Total Comfort While Dying among Nursing Home Residents with Dementia between 2010 and 2015: Results from Two Retrospective Epidemiological Studies

 , ,
, ,
Abstract
1. Introduction
- -
- Are there differences in the prevalence of dementia in nursing homes between 2010 and 2015?
- -
- Are there differences in the socio-demographic and clinical characteristics of nursing home residents with dementia between 2010 and 2015?
- -
- Are there differences in palliative care service use and comfort in the last week of the life of nursing home residents with dementia between 2010 and 2015?
2. Materials and Methods
2.1. Design
2.2. Participating Nursing Homes
2.3. Data Collection and Study Population
2.4. Measurements and Outcome Measures
2.4.1. Residents’ Characteristics
2.4.2. Palliative Care Services Used
2.4.3. Comfort in the Last Week of Life
2.5. Data Analyses
3. Results
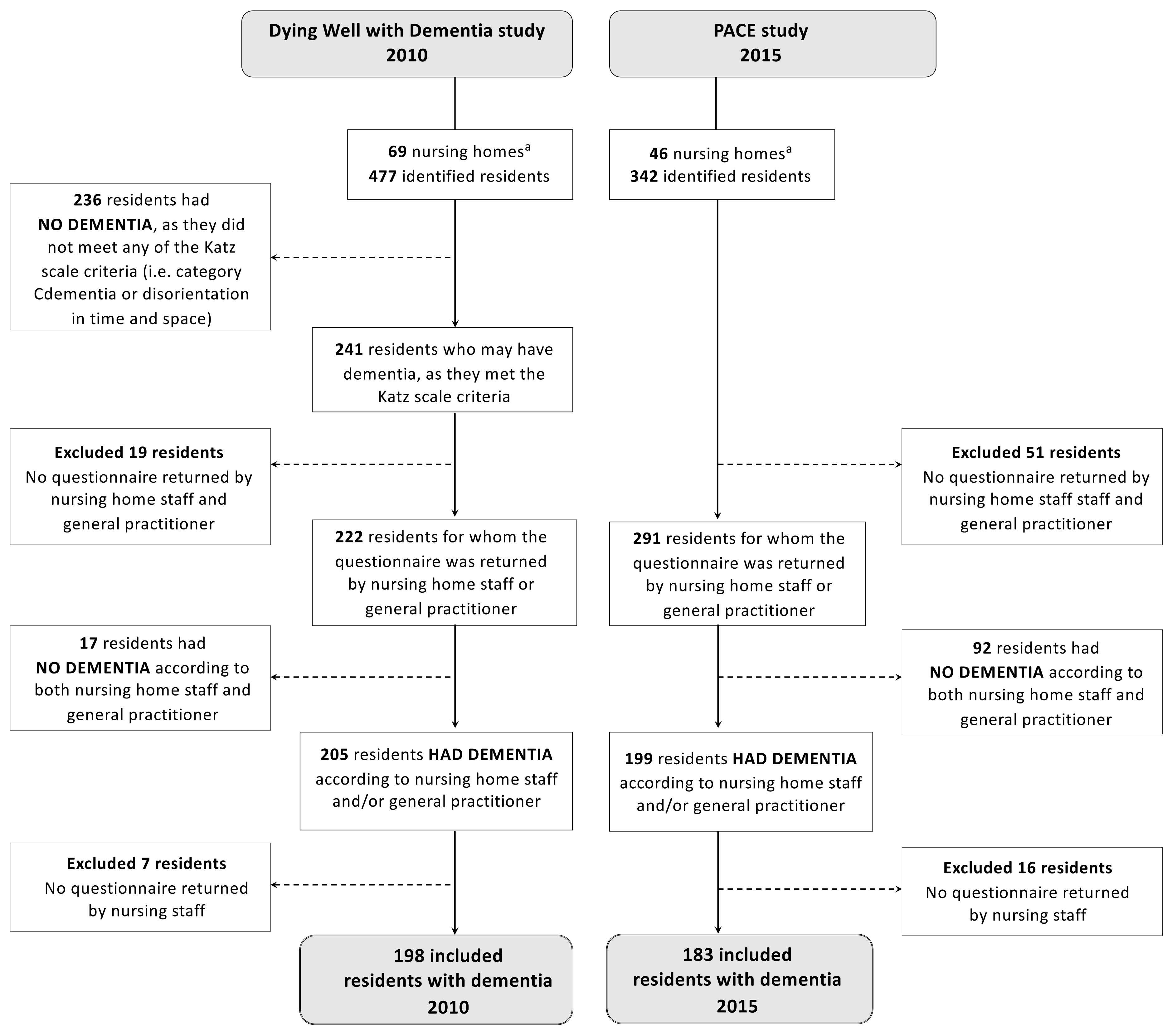
3.1. Prevalence of Dementia
3.2. Characteristics of Residents with Dementia
3.3. Palliative Care Service Use among Residents with Dementia
3.4. Comfort in the Last Week of Life
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van Der Steen, J.T.; Radbruch, L.; Hertogh, C.M.P.M.; E De Boer, M.; Hughes, J.C.; Larkin, P.; Francke, A.L.; Jünger, S.; Gove, D.; Firth, P.; et al. White paper defining optimal palliative care in older people with dementia: A Delphi study and recommendations from the European Association for Palliative Care. Palliat. Med. 2014, 28, 197–209. [Google Scholar] [CrossRef]
- Mitchell, S.L.; Teno, J.M.; Kiely, D.K.; Shaffer, M.L.; Jones, R.N.; Prigerson, H.G.; Volicer, L.; Givens, J.L.; Hamel, M.B. The Clinical Course of Advanced Dementia. N. Engl. J. Med. 2009, 361, 1529–1538. [Google Scholar] [CrossRef]
- Van der Steen, J.T. Dying with dementia: What we know after more than a decade of research. J. Alzheimer’s Dis. 2010, 22, 37–55. [Google Scholar] [CrossRef]
- Alzheimer Europe. Dementia in Europe Yearbook 2019 Estimating the Prevalence of Dementia in Europe; Alzheimer Europe: Luxembourg, 2020. [Google Scholar]
- Reyniers, T.; Deliens, L.; Pasman, H.R.; Morin, L.; Addington-Hall, J.; Frova, L.; Cardenas-Turanzas, M.; Onwuteaka-Philipsen, B.; Naylor, W.; Ruiz-Ramos, M.; et al. International variation in place of death of older people who died from dementia in 14 European and non-European countries. J. Am. Med. Dir. Assoc. 2015, 16, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Houttekier, D.; Cohen, J.; Bilsen, J.; Addington-Hall, J.; Onwuteaka-Philipsen, B.D.; Deliens, L. Place of death of older persons with dementia. A study in five European countries. J. Am. Geriatr. Soc. 2010, 58, 751–756. [Google Scholar] [CrossRef]
- Pivodic, L.; Smets, T.; Noortgate, N.V.D.; Onwuteaka-Philipsen, B.D.; Engels, Y.; Szczerbińska, K.; Finne-Soveri, H.; Froggatt, K.; Gambassi, G.; Deliens, L.; et al. Quality of dying and quality of end-of-life care of nursing home residents in six countries: An epidemiological study. Palliat. Med. 2018, 32, 1584–1595. [Google Scholar] [CrossRef]
- Ariascasais, N.; Garralda, E.; Rhee, J.Y.; Lima, L.; De Pons, J.J.; Clark, D.; Centeno, C. EAPC Atlas of Palliative Care in Europe 2019; EAPC Vzw Press: Vilvoorde, Begium, 2019. [Google Scholar]
- Miranda, R.; Penders, Y.W.H.; Smets, T.; Deliens, L.; Miccinesi, G.; Alonso, T.V.; Moreels, S.; Block, L.V.D. Quality of primary palliative care for older people with mild and severe dementia: An international mortality follow-back study using quality indicators. Age Ageing 2018, 47, 824–833. [Google Scholar] [CrossRef] [PubMed]
- Honinx, E.; Pace, O.B.O.; Van Dop, N.; Smets, T.; Deliens, L.; Noortgate, N.V.D.; Froggatt, K.; Gambassi, G.; Kylänen, M.; Onwuteaka-Philipsen, B.; et al. Dying in long-term care facilities in Europe: The PACE epidemiological study of deceased residents in six countries. BMC Public Health 2019, 19, 1199. [Google Scholar] [CrossRef]
- Mitchell, S.L. Advanced dementia. N. Engl. J. Med. 2015, 372, 2533–2540. [Google Scholar] [CrossRef] [PubMed]
- Sampson, E.L.; Candy, B.; Davis, S.; Gola, A.B.; Harrington, J.; King, M.; Kupeli, N.; Leavey, G.; Moore, K.; Nazareth, I.; et al. Living and dying with advanced dementia: A prospective cohort study of symptoms, service use and care at the end of life. Palliat. Med. 2018, 32, 668–681. [Google Scholar] [CrossRef]
- Alzheimer Europe. Dementia in Europe Yearbook 2018: Comparison of National Dementia Strategies in Europe; Alzheimer Europe: Luxembourg, 2018. [Google Scholar]
- STATBEL: Belgium in Figures. Structure of the Population: Belgium. 2020. Available online: https://statbel.fgov.be/en/themes/population/structure-population (accessed on 20 October 2020).
- Flemish Parliament. Flemish Policy for Older People 2010–2014 [Vlaams Ouderenbeleidsplan 2010–2014]; Flemish Parliament: Brussels, Belgium, 2011; pp. 1–16. [Google Scholar]
- Flemish Government. To a Dementia-Friendly Flanders: Dementiaplan Flanders 2010–2014 [Naar een Dementievriendelijk Vlaanderen: Dementieplan Vlaanderen 2010–2014]; Flemish Government: Brussels, Belgium, 2010.
- Flemish Parliament. Dementia-Evolution-Strategic Policies [Dementie-Evolutie-Beleidsmaatregelen]; Flemish Parliament: Brussels, Belgium, 2015; pp. 1–4. [Google Scholar]
- Flemish Government. Decree Aiming to Stimulate an Inclusive Flemish Policy for Older People and Policy Participation of Older People [Decreet Houdende de Stimulering van een Inclusief Vlaams Ouderenbeleid en de Beleidsparticipatie van Ouderen]; Flemish Government: Brussels, Belgium, 2012.
- Flemish Government. Transition Plan “Dementia Expertise in Basic Care in the Natural Home Setting” [Transitieplan ’Dementiekundige Basiszorg in het Natuurlijk Thuismilieu’]; Flemish Government: Brussels, Belgium, 2014.
- Expertise Center Dementia Vlaanderen. Expertisecentrum Dementie Vlaanderen Annual Reports: Antwerp, Belgium. 2020. Available online: http://www.dementie.be/expertisecentrum-dementie-vlaanderen-vzw/organisatie/jaarverslag/ (accessed on 5 May 2020).
- King Boudewijn Foundation. I Will Remain Who I Was: Ten Years of Working Together for a Dementia-Friendly Society [Ik Blijf Wie Ik Was: Tien Jaar Samen Werken aan een Dementievriendelijke Samenleving]; King Boudewijn Foundation: Brussels, Belgium, 2018. [Google Scholar]
- Flemish Parliament. Dementievriendelijke Gemeente—Stand van Zaken; Brussels, Belgium. 2018. Available online: http://docs.vlaamsparlement.be/pfile?id=1416395 (accessed on 5 May 2020).
- Flemish Parliament. Dementia—Training Psycho-Education [Dementie—Opleiding Psycho-Educatie]; Brussels, Belgium. 2017. Available online: http://docs.vlaamsparlement.be/pfile?id=1416395 (accessed on 5 June 2020).
- Luppa, M.; Luck, T.; Brahler, E.; Konig, H.H.; RiedelHeller, S.G. Prediction of institutionalisation in dementia: A systematic review. Dement. Geriatr. Cogn. Disord. 2008, 26, 65–78. [Google Scholar] [CrossRef]
- Eska, K.; Graessel, E.; Donath, C.; Schwarzkopf, L.; Lauterberg, J.; Holle, R. Predictors of institutionalization of dementia patients in mild and moderate stages: A 4-year prospective analysis. Dement. Geriatr. Cogn. Dis. Extra. 2013, 3, 426–445. [Google Scholar] [CrossRef] [PubMed]
- Belgian Federal Government. Amendments of the 14 June 2002 Law Concerning Palliative Care Belgium, to Expand the Definition of Palliative Care [Wet tot Wijziging van de Wet 14 Juni 2002 Betreffende de Palliatieve zorg, tot Verruiming van de Definitie van Palliatieve Zorg]; Belgian Federal Government: Brussels, Belgium, 2016.
- Flemish Parliament. Decree for Residential Care [Decreet Woonzorgdecreet]; Brussels, Belgium. 2009. Available online: https://codex.vlaanderen.be/Portals/Codex/documenten/1017896.html (accessed on 6 June 2020).
- Federation for Palliative Care Flanders. Pallialine.be: Guideline for Palliative Care; Vilvoorde, Belgium. 2010. Available online: http://www.pallialine.be/template.asp?f=welkom.htm (accessed on 22 July 2020).
- Stabel, K.; Verstraete, A.; Mullie, S.; Vanden Berghe, P. Guideline for Implementation of Palliative Care in Nursing Homes [Leidraad voor Implementatie Van Palliatieve Zorg in Woonzorgcentra]; Federation of Palliative Care Flanders: Vilvoorde, Belgium, 2010. [Google Scholar]
- Sevenants, A.; Spruytte, N.; Van Audenhove, C. Flemish Indicator Project Nursing Homes: Guideline 1.6 [Vlaams Indicatorenproject Woonzorgcentra: Handleiding 1.6]; Agency for Healthcare and Health: Brussels, Belgium, 2015. [Google Scholar]
- Vandervoort, A.; Block, L.V.D.; Van Der Steen, J.T.; Volicer, L.; Stichele, R.V.; Houttekier, D.; Deliens, L. Nursing home residents dying with dementia in Flanders, Belgium: A nationwide postmortem study on clinical characteristics and quality of dying. J. Am. Med. Dir. Assoc. 2013, 14, 485–492. [Google Scholar] [CrossRef]
- Block, L.V.D.; Smets, T.; Van Dop, N.; Adang, E.; Andreasen, P.; Moore, D.C.; Engels, Y.; Finne-Soveri, H.; Froggatt, K.; Gambassi, G.; et al. Comparing Palliative Care in Care Homes Across Europe (PACE): Protocol of a Cross-sectional Study of Deceased Residents in 6 EU Countries. J. Am. Med. Dir. Assoc. 2016, 17, 1–7. [Google Scholar]
- Hillmer, M.P.; Wodchis, W.P.; Gill, S.S.; Anderson, G.M.; Rochon, P.A. Nursing home profit status and quality of care: Is there any evidence of an association? Med. Care Res. Rev. 2005, 62, 139e166. [Google Scholar] [CrossRef] [PubMed]
- McGregor, M.J.; Tate, R.B.; Ronald, L.A.; McGrail, K.M. Variation in site of death among nursing home residents in British Columbia, Canada. J. Palliat. Med. 2007, 10, 1128e1136. [Google Scholar] [CrossRef] [PubMed]
- Alzheimer’s Association. Katz Independence in Activities of Daily Living. Available online: https://www.alz.org/careplanning/downloads/katz-adl.pdf (accessed on 3 February 2021).
- Morris, J.N.; Fries, B.E.; Mehr, D.R.; Hawes, C.; Phillips, C.; Mor, V.; Lipsitz, L.A. MDS cognitive performance scale. J. Gerontol. 1994, 49, M174–M182. [Google Scholar] [CrossRef] [PubMed]
- Reisberg, B.; Ferris, S.H.; de Leon, M.J.; Crook, T. The Global Deterioration Scale for assessment of primary degenerative dementia. Am. J. Psychiatry 1982, 139, 1136–1139. [Google Scholar]
- Bellelli, G.; Frisoni, G.B.; Bianchetti, A.; Trabucchi, M. The Bedford Alzheimer Nursing Severity scale for the severely demented: Validation study. Alzheimer Dis. Assoc. Disord. 1997, 11, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Erel, M.; Marcus, E.-L.; Dekeyser-Ganz, F. Barriers to palliative care for advanced dementia: A scoping review. Ann. Palliat. Med. 2017, 6, 365–379. [Google Scholar] [CrossRef]
- Midtbust, M.H.; Alnes, R.E.; Gjengedal, E.; Lykkeslet, E. Perceived barriers and facilitators in providing palliative care for people with severe dementia: The healthcare professionals’ experiences. BMC Health Serv. Res. 2018, 18, 1–10. [Google Scholar] [CrossRef]
- Ryan, T.; Gardiner, C.; Bellamy, G.; Gott, M.; Ingleton, C. Barriers and facilitators to the receipt of palliative care for people with dementia: The views of medical and nursing staff. Palliat. Med. 2012, 26, 879–886. [Google Scholar] [CrossRef]
- Miranda, R.; Van Der Steen, J.T.; Smets, T.; Noortgate, N.V.D.; Deliens, L.; Payne, S.; Kylänen, M.; Szczerbińska, K.; Gambassi, G.; Block, L.V.D.; et al. Comfort and clinical events at the end of life of nursing home residents with and without dementia: The six-country epidemiological PACE study. Int. J. Geriatr. Psychiatry 2020, 35, 719–727. [Google Scholar] [CrossRef]
- Federation Palliative Care Flanders. Policy Note: Palliative Care in the Nursing Homes—A Path to Quality Improvement [Beleidsnota: Palliatieve Zorg in de Woonzorgcentraeen Pad Naar Kwaliteitsverbetering]; Federation Palliative Care Flanders: Vilvoorde, Belgium, 2017. [Google Scholar]
- Kiely, D.K.; Volicer, L.; Teno, J.; Jones, R.N. The validity and reliability of scales for the evaluation of end-of-life care in advanced dementia. Alzheimer Dis. Assoc. Disord. 2006, 20, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Volicer, L.; Hurley, A.C.; Blasi, Z.V. Scales for Evaluation of End-of-Life Care in Dementia. Alzheimer Dis. Assoc. Disord. 2001, 15, 194–200. [Google Scholar] [CrossRef]
- Parmar, J.; Dobbs, B.; McKay, R.; Kirwan, C.; Cooper, T.; Marin, A.; Gupta, N. Diagnosis and management of dementia in primary care: Exploratory study. Can. Fam. Physician 2014, 60, 457–465. [Google Scholar] [PubMed]
- Elliott, A.F.; Horgas, A.L.; Marsiske, M. Nurses’ Role in Identifying Mild Cognitive Impairment in Older Adults. Geriatr. Nurs. (Minneap) 2008, 29, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Steyaert, J. Expertise Centre Dementia Flanders. Prevalence: How Many People Die with Dementia in Flanders [Prevalentie: Hoeveel Personen in Vlaanderen Hebben Dementie?]. Handboek Dementie. 2016. Available online: http://www.dementie.be/wp-content/uploads/2016/05/2016-steyaert-prevalentie-dementie.pdf (accessed on 20 October 2020).
- Bunn, F.; Burn, A.-M.; Goodman, C.; Robinson, L.; Rait, G.; Norton, S.; Bennett, H.; Poole, M.; Schoeman, J.; Brayne, C. Comorbidity and dementia: A mixed-method study on improving health care for people with dementia (CoDem). Health Serv. Deliv. Res. 2016, 4, 1–156. [Google Scholar] [CrossRef]
- Hendriks, S.A.; Smalbrugge, M.; Galindo-Garre, F.; Hertogh, C.M.; van der Steen, J.T. From Admission to death: Prevalence and course of pain, agitation, and shortness of breath, and treatment of these symptoms in nursing home residents with dementia. J. Am. Med. Dir. Assoc. 2015, 16, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Alonzo, T. Hope for persons with Dementia: Why comfort matters. Gener. J. Am. Soc. Aging 2017, 4, 81–85. [Google Scholar]
- Parker, D.; Lewis, J.; Gourlay, K. Dementia Australia’s Dementia Advisory Committee. Palliative Care and Dementia. Dement. Aust. 2017. Available online: https://palliativecare.org.au/wp-content/uploads/dlm_uploads/2018/05/Dementia-Aus-Palliative-Care-Discussion-Paper-36pp-R5.pdf (accessed on 23 February 2021).
- NHS: North West Coast Strategic Clinical Network. Palliative Care Guidelines in Dementia, 2nd ed.; North West Coast Strategic Clinical Network: Warrington, UK, 2018. [Google Scholar]
- Alzheimer Europe. Dementia in Europe Yearbook 2017 Standards for Residential Care Facilities in Europe; Alzheimer Europe: Luxembourg, 2020. [Google Scholar]
- Prince, M.; Comas-Herrera, A.; Knapp, M.; Guerchet, M.; Karagiannidou, M. World Alzheimer Report 2016 Improving Healthcare for People Living with Dementia. Coverage, Quality and Costs Now and in the Future; Alzheimer’s Disease International: London, UK, 2016; pp. 1–140. [Google Scholar]
- World Health Organization. Global Action Plan on the Public Health Response to Dementia 2017–2025; World Health Organization: Geneva, Switzerland, 2017; pp. 1–52. [Google Scholar]
- Smets, T.; Pivodic, L.; Piers, R.; Pasman, H.R.W.; Engels, Y.; Szczerbińska, K.; Kylänen, M.; Gambassi, G.; Payne, S.; Deliens, L.; et al. The palliative care knowledge of nursing home staff: The EU FP7 PACE cross-sectional survey in 322 nursing homes in six European countries. Palliat. Med. 2018, 32, 1487–1497. [Google Scholar] [CrossRef] [PubMed]
- Van den Block, L.; Honinx, E.; Pivodic, L.; Miranda, R.; Onwuteaka-Philipsen, B.D.; van Hout, H.; Pasman, H.R.W.; Oosterveld-Vlug, M.; Koppel, M.T.; Piers, R.; et al. Evaluation of a Palliative Care Program for Nursing Homes in 7 Countries the PACE Cluster-Randomized Clinical Trial. JAMA Intern. Med. 2020, 180, 233–242. [Google Scholar] [CrossRef]
- Moore, D.C.; Payne, S.; Block, L.V.D.; Ling, J.; Froggatt, K.; Gatsolaeva, Y.; Honinx, E.; Pivodic, L.; Miranda, R.; Onwuteaka-Philipsen, B.D.; et al. Strategies for the implementation of palliative care education and organizational interventions in long-term care facilities: A scoping review. Palliat. Med. 2020, 34, 558–570. [Google Scholar] [CrossRef] [PubMed]
- Froggatt, K.A.; Moore, D.C.; Van den Block, L.; Ling, J.; Payne, S.A. PACE Consortium Collaborative Authors on Behalf of the European Association for Palliative Care. Palliative Care Implementation in Long-Term Care Facilities: European Association for Palliative Care White Paper. J. Am. Med. Dir. Assoc. 2020, 21, 1051–1057. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.C.; Payne, S.A.; Van Den Block, L.; Ten Koppel, M.; Szczerbińska, K.; Froggatt, K. Research, recruitment and observational data collection in care homes: Lessons from the PACE study. BMC Res. Notes 2019, 12, 1–6. [Google Scholar]


{kind=link}
| Residents’ Characteristics | 2010 (N = 198) | 2015 (N = 183) | Change | Difference between the Years p-Values † |
|---|---|---|---|---|
| Socio-demographic characteristics | ||||
| Age at time of death, average in years (SD) | 86.7 (7) | 86.9 (7.3) | +0.2 | 0.73 |
| Gender, female n (%) | 115 (61) | 114 (65) | +4 | 0.43 |
| Clinical characteristics | ||||
| Cognitive performance scale (CPS), n (%) | 0.04 | |||
| - Intact, borderline intact, mild impairment (score 0-1-2) | 8 (4) | 21 (13) | +9 | |
| - Moderate impairment (score 3) | 27 (14) | 20 (12) | −2 | |
| - Moderately severe impairment (score 4) | 9 (5) | 15 (9) | +4 | |
| - Severe impairment (score 5) | 61 (33) | 52 (31) | −2 | |
| - Very severe impairment (score 6) | 82 (44) | 58 (35) | −9 | |
| Global deterioration scale (GDS) stage 7, n (%) | 105 (58) | 123 (72) | +14 | 0.04 |
| Bedford Alzheimer Nursing Severity scale (BANS-S) 1 month before death, mean (SD) | 20.9 (3.9) | 20.3 (4.3) | −0.6 | 0.19 |
| Severity of dementia, n (%) | 0.55 | |||
| - Non-advanced dementia | 95 (51) | 75 (48) | −3 | |
| - Advanced dementia | 92 (49) | 82 (52) | +3 | |
| Occurrence of clinical complications in last month of life, n (%) | 179 (95) | 168 (92) | −3 | 0.31 |
| Co-existing conditions | ||||
| - Cancer | 12 (11) | 19 (14) | +3 | 0.43 |
| - Cardiovascular | 32 (29) | 37 (28) | −1 | 0.89 |
| - Respiratory | 15 (14) | 14 (11) | −3 | 0.51 |
| - Neurological (not dementia) | 17 (15) | 10 (8) | −7 | 0.08 |
| - Urogenital | 9 (8) | 12 (9) | +1 | 0.82 |
| - Other | 18 (16) | 22 (17) | +1 | 0.99 |
| Length of stay in nursing home in days, median days (IQR) | 893 (448–1694) | 688 (283–1678) | −205 | 0.28 |
| Place of death, n (%) | 0.20 | |||
| - Nursing homes | 171 (90) | 152 (86) | −4 | |
| - Hospital | 17 (9) | 24 (14) | +5 | |
| - Other ‡ | 2 (1) | 0 (0) | −1 | |
| Type of unit at time of death, n (%) | 0.71 | |||
| - Open unit | 91 (48) | 88 (50) | +2 | |
| - Secured unit | 98 (51) | 88 (50) | −1 | |
| Dementia care unit, yes, n (%) | 99 (53) | 93 (53) | 0 | 0.95 |
| Palliative Care Service Use | 2010 (N = 198) | 2015 (N = 183) | %-Point | Difference between Years (p-Values ‡) | |
|---|---|---|---|---|---|
| n (%) | n (%) | Change † | Crude | Adjusted | |
| Residents who had a palliative care record | 121 (62) | 97 (72) | +10 | 0.10 | 0.17 |
| Time before death when the palliative care record initiated | |||||
| - <14 days | 51 (51) | 38 (60) | +9 | 0.10 | 0.63 |
| - 15 to 90 days | 32 (32) | 22 (35) | +3 | ||
| - >90 days | 18 (18) | 3 (5) | −13 | ||
| Residents who received palliative care at any time according to nursing home staff | 162 (83) | 145 (82) | −1 | 0.69 | 0.21 |
| Palliative care was provided by GP | 136 (84) | 123 (86) | +2 | 0.84 | 0.89 |
| Other person/initiatives involved in providing the palliative care | |||||
| - Coordinating and advisory physician | 44 (27) | 35 (23) | −4 | 0.44 | 0.11 |
| - Palliative care reference nurse | 110 (66) | 94 (62) | −4 | 0.64 | 0.35 |
| - Palliative care task group within the nursing home | 81 (49) | 64 (42) | −7 | 0.35 | 0.34 |
| - Palliative home care teams (external) | 16 (10) | 8 (5) | −5 | 0.24 | 0.30 |
| - No one from this list was involved | 28 (17) | 30 (20) | +3 | 0.55 | 0.83 |
| Residents who received medical or nursing treatments/procedures during the last week of life | |||||
| Mouthcare | 159 (80) | 152 (88) | +8 | 0.055 | 0.54 |
| Pain assessment | 124 (63) | 143 (83) | +20 | 0.001 | 0.03 |
| Prevention of pressure ulcers | 162 (82) | 151 (87) | +5 | 0.15 | 0.72 |
| Wound care | 45 (23) | 48 (28) | +5 | 0.27 | 0.97 |
| Assistance with eating/drinking | 142 (72) | 141 (82) | +10 | 0.04 | 0.37 |
| Residents who received psychosocial interventions in the last month of life | |||||
| Adjustments of environmental factors ¶ | 19 (10) | 28 (16) | +6 | 0.10 | 0.18 |
| Activity programmes | 25 (13) | 16 (9) | −4 | 0.33 | 0.85 |
| Music therapy | 48 (24) | 28 (16) | −8 | 0.17 | 0.24 |
| Behavioural therapy | 0 (0) | 1 (1) | +1 | 0.87 | 0.78 |
| Experiential approaches # | 52 (26) | 47 (28) | +2 | 0.90 | 0.32 |
| No psychosocial interventions received | 74 (37) | 81 (47) | +10 | 0.15 | 0.78 |
| Residents who received spiritual and/or pastoral care shortly before death | |||||
| Spiritual care provider/Pastoral worker | 98 (48) | 72 (57) | +9 | 0.10 | 0.11 |
| COMFORT IN THE LAST WEEK OF LIFE | 2010 (N = 198) | 2015 (N = 183) | Score-Point | Difference between Years (p-Values ‡) | |
|---|---|---|---|---|---|
| CAD-EOLD individual items | CAD-EOLD scores 0 (worst) to 3 (best) | CAD-EOLD scores 0 (worst) to 3 (best) | Change † | Crude | Adjusted |
| - Discomfort | 2.1 (2.0–2.2) | 2.1 (2.0–2.2) | – | 0.46 | 0.88 |
| - Pain | 2.0 (1.9–2.1) | 2.2 (2.1–2.3) | +0.2 | 0.03 | 0.62 |
| - Restlessness | 2.1 (2.0–2.2) | 2.1 (2.0–2.2) | – | 0.72 | 0.39 |
| - Shortness of breath | 2.2 (2.1–2.3) | 2.4 (2.3–2.5) | +0.2 | 0.03 | 0.14 |
| - Choking | 2.1 (2.0–2.2) | 2.1 (2.0–2.2) | – | 0.77 | 0.75 |
| - Gurgling | 2.3 (2.2–2.4) | 2.5 (2.3–2.6) | +0.2 | 0.13 | 0.83 |
| - Difficulty swallowing | 1.9 (1.8–2.0) | 1.9 (1.8–2.0) | – | 0.61 | 0.84 |
| - Fear | 2.0 (1.9–2.2) | 2.2 (2.1–2.3) | +0.2 | 0.04 | 0.45 |
| - Anxiety | 2.1 (2.1–2.3) | 2.2 (2.1–2.3) | +0.1 | 0.32 | 0.88 |
| - Crying | 2.7 (2.6–2.8) | 2.7 (2.6–2.8) | – | 0.49 | 0.89 |
| - Moaning | 2.3 (2.3–2.4) | 2.5 (2.4–2.6) | +0.2 | 0.02 | 0.03 |
| - Serenity | 2.0 (1.9–2.2) | 2.1 (2.0–2.2) | +0.1 | 0.69 | 0.07 |
| - Peace | 2.0 (1.9–2.1) | 2.0 (1.9–2.2) | – | 0.63 | 0.24 |
| - Calm | 2.0 (1.9–2.1) | 2.0 (1.9–2.1) | – | 0.33 | 0.31 |
| Total score ¶, estimated marginal means (95% CI) | 30.0 (29.2–30.8) | 30.8 (29.2–30.9) | +0.8 | 0.22 | 0.87 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miranda, R.; Smets, T.; Van Den Noortgate, N.; Deliens, L.; Van den Block, L. Higher Prevalence of Dementia but No Change in Total Comfort While Dying among Nursing Home Residents with Dementia between 2010 and 2015: Results from Two Retrospective Epidemiological Studies. Int. J. Environ. Res. Public Health 2021, 18, 2160. https://doi.org/10.3390/ijerph18042160
Miranda R, Smets T, Van Den Noortgate N, Deliens L, Van den Block L. Higher Prevalence of Dementia but No Change in Total Comfort While Dying among Nursing Home Residents with Dementia between 2010 and 2015: Results from Two Retrospective Epidemiological Studies. International Journal of Environmental Research and Public Health. 2021; 18(4):2160. https://doi.org/10.3390/ijerph18042160
Chicago/Turabian StyleMiranda, Rose, Tinne Smets, Nele Van Den Noortgate, Luc Deliens, and Lieve Van den Block. 2021. "Higher Prevalence of Dementia but No Change in Total Comfort While Dying among Nursing Home Residents with Dementia between 2010 and 2015: Results from Two Retrospective Epidemiological Studies" International Journal of Environmental Research and Public Health 18, no. 4: 2160. https://doi.org/10.3390/ijerph18042160
APA StyleMiranda, R., Smets, T., Van Den Noortgate, N., Deliens, L., & Van den Block, L. (2021). Higher Prevalence of Dementia but No Change in Total Comfort While Dying among Nursing Home Residents with Dementia between 2010 and 2015: Results from Two Retrospective Epidemiological Studies. International Journal of Environmental Research and Public Health, 18(4), 2160. https://doi.org/10.3390/ijerph18042160