
Interventions on Food Security and Water Uses for Improving Nutritional Status of Pregnant Women and Children Younger Than Five Years in Low-Middle Income Countries: A Systematic Review




Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Research Question
2.3. Literature Search and Selection Criteria
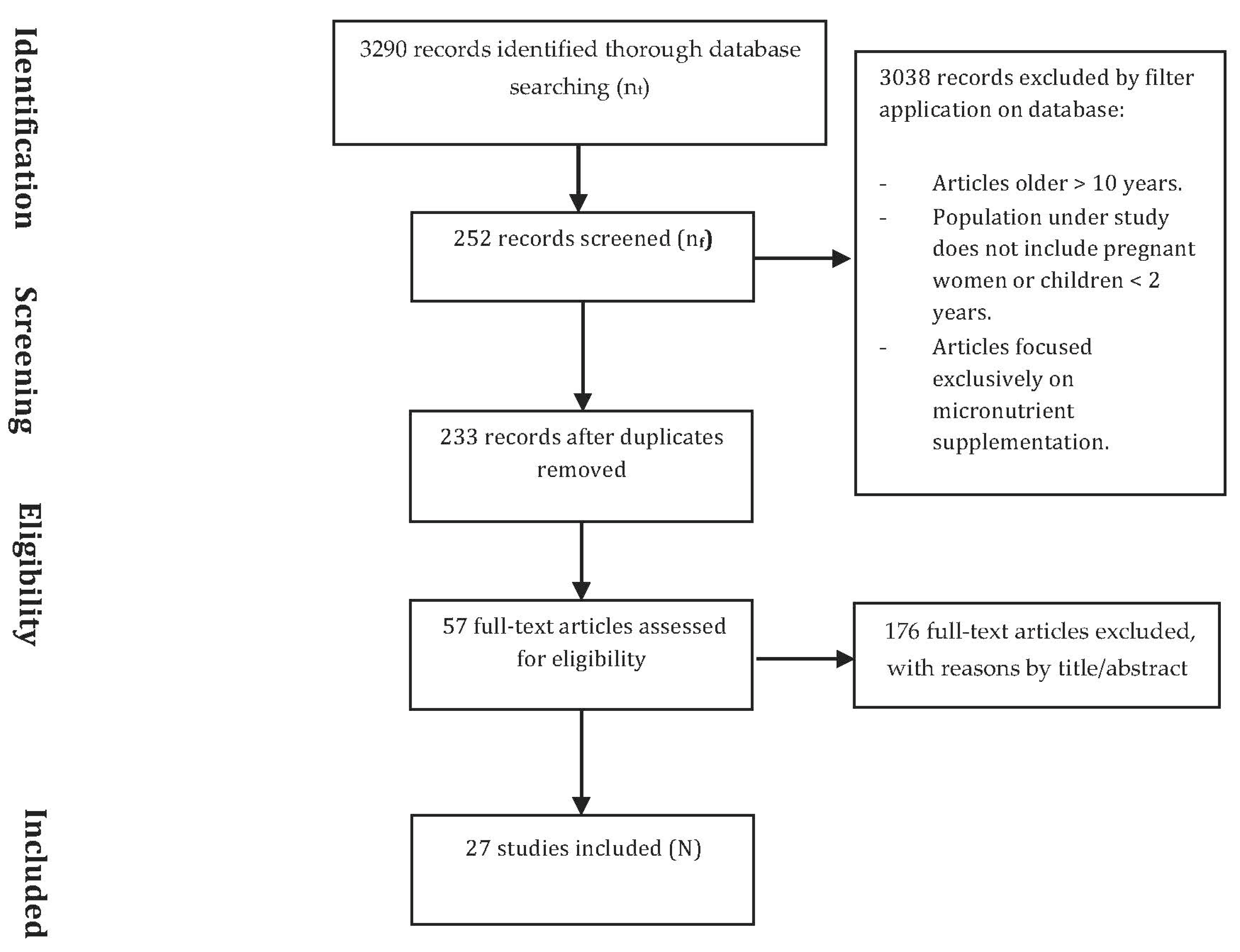
2.4. Search Outcomes
2.5. Quality Appraisal
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.3. Food-Based and Nutritional Interventions
3.4. WASH Interventions
3.5. Food-Based Interventions Combined with WASH Interventions
4. Discussion
4.1. Socioeconomic Variables and Nutritional Status
4.2. Diet Diversity and Seasonality: Factors for Zero Hunger, Considering the Climate Change Context
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- FAO; IFAD; UNICEF; WFP; WHO. The State of Food Security in the World 2019. In Safeguarding against Economic Slowdowns and Downturns; FAO: Rome, Italy, 2019; p. 212. [Google Scholar]
- Boliko, M.C. FAO and the Situation of Food Security and Nutrition in the World. J. Nutr. Sci. Vitaminol. 2019, 65, S4–S8. [Google Scholar] [CrossRef] [PubMed]
- FAO; IFAD; UNICEF; WFP; WHO. The State of Food Security and Nutrition in the World 2020: Transforming Food Systems for Affordable Healthy Diets; FAO: Rome, Italy, 2020. [Google Scholar]
- Ghosh-Jerath, S.; Downs, S.; Singh, A.; Paramanik, S.; Goldberg, G.; Fanzo, J. Innovative matrix for applying a food systems ap-proach for developing interventions to address nutrient deficiencies in indigenous communities in India: A study protocol. BMC Public Health 2019, 19, 1–2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prüss-Üstün, A.; Bos, R.; Gore, F.; Bartram, J. Safer Water, Better Health: Costs, Benefits and Sustainability of Interventions to Pro-Tect and Promote Health; World Health Organization: Geneva, Switzerland, 2008; p. 53. [Google Scholar]
- Myers, S.S.; Smith, M.R.; Guth, S.; Golden, C.D.; Vaitla, B.; Mueller, N.D.; Dangour, A.D.; Huybers, P. Climate Change and Global Food Systems: Potential Impacts on Food Security and Undernutrition. Annu. Rev. Public Health 2017, 38, 259–277. [Google Scholar] [CrossRef] [PubMed]
- Bartram, J.; Cairncross, S. Hygiene, Sanitation, and Water: Forgotten Foundations of Health. PLoS Med. 2010, 7, e1000367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piper, J.; Chandna, J.; Allen, E.; Linkman, K.; Cumming, O.; Prendergast, A.; Gladstone, M.J. Water, sanitation and hygiene (WASH) interven-tions: Effects on child developement in low- and middle-income coutries. Cochrane Database Syst. Rev. 2017, 3, 1–39. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Kimani-Murage, E.W.; Griffiths, P.L.; Wekesah, F.M.; Wanjohi, M.; Muhia, N.; Muriuki, P.; Egondi, T.; Kyobutungi, C.; Ezeh, A.C.; McGarvey, S.T.; et al. Effectiveness of home-based nutri-tional counselling and support on exclusive breastfeeding in urban poor settings in Nairobi: A cluster randomized controlled trial. Glob. Health 2017, 13, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Mutisya, M.; Kandala, N.B.; Ngware, M.W.; Kabiru, C.W. Household food (in)security and nutritional status of urban poor chil-dren aged 6 to 23 months in Kenya Global health. BMC Public Health 2015, 15, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Hasan, T.; Magalhaes, R.J.S.; Williams, G.M.; Mamun, A.A. The role of maternal education in the 15-year trajectory of malnutrition in children under 5 years of age in Bangladesh. Matern. Child. Nutr. 2015, 12, 929–939. [Google Scholar] [CrossRef]
- Campbell, R.K.; Hurley, K.M.; Shamim, A.A.; Shaikh, S.; Chowdhury, Z.T.; Mehra, S.; De Pee, S.; Ahmed, T.; West, K.P., Jr.; Christian, P. Effect of complementary food supplemen-tation on breastfeeding and home diet in rural Bangladeshi children. Am. J. Clin. Nutr. 2016, 104, 1450–1458. [Google Scholar] [CrossRef]
- Stevens, B.; Watt, K.; Brimbecombe, J.; Clough, A.; Judd, J.; Lindsay, D. The role of seasonality on the diet and household food secu-rity of pregnant women living in rural Bangladesh: A cross-sectional study. Public Health Nutr. 2017, 20, 121–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lander, R.L.; Hambidge, K.M.; Westcott, J.E.; Tejeda, G.; Diba, T.S.; Mastiholi, S.C.; Khan, U.S.; Garcés, A.; Figueroa, L.; Tshefu, A.; et al. Pregnant Women in Four Low-Middle Income Countries Have a High Prevalence of Inadequate Dietary Intakes That Are Improved by Dietary Diversity. Nutrients 2019, 11, 1560. [Google Scholar] [CrossRef] [Green Version]
- Shaheen, R.; Streatfield, P.K.; Naved, R.T.; Lindholm, L.; Persson, L.A. Equity in adherence to and effect of prenatal food and mi-cronutrient supplementation on child mortality: Results from the MINIMat randomized trial, Bangladesh. BMC Public Health 2014, 14, 5. [Google Scholar] [CrossRef] [PubMed]
- Shafique, S.; Sellen, D.W.; Lou, W.; Jalal, C.S.; Jolly, S.P.; Zlotkin, S.H. Mineral- and vitamin-enhanced micronutrient powder reduces stunting in full-term low-birth-weight infants receiving nutrition, health, and hygiene education: A 2 × 2 factorial, cluster-randomized trial in Bangladesh. Am. J. Clin. Nutr. 2016, 103, 1357–1369. [Google Scholar] [CrossRef] [PubMed]
- Le Port, A.; Bernard, T.; Hidrobo, M.; Birba, O.; Rawat, R.; Ruel, M.T. Delivery of iron-fortified yoghurt, through a dairy value chain program, increases hemoglobin concentration among children 24 to 59 months old in Northern Senegal: A clus-ter-randomized control trial. PLoS ONE 2017, 12, e0172198. [Google Scholar] [CrossRef] [PubMed]
- Borg, B.; Mihrshahi, S.; Griffin, M.; Sok, D.; Chhoun, C.; Laillou, A.; Berger, J.; Wieringa, F.T. Reandomised controlled trial to test the effectiveness of a locally-produced ready-to-use supplemetrary food and improving micronutrient status for children under two years in Cam-bodia: A study protocol. Nutr. J. 2018, 17, 1–11. [Google Scholar] [CrossRef]
- Sigh, S.; Roos, N.; Chamnan, C.; Laillou, A.; Prak, S.; Wieringa, F.T. Effectiveness of a Locally Produced, Fish-Based Food Product on Weight Gain among Cambodian Children i the Treatmen of Acute Malnutrition: A Randomized Controlled Trial. Nutrients 2018, 10, 909. [Google Scholar] [CrossRef] [Green Version]
- Fenn, B.; Sangrasi, G.M.; Puett, C.; Trenouth, L.; Pietzsch, S. The REFANI Pakistan stuady-a cluster randomised controlled trial of the effectiveness and cost-effectiveness of cash-based transfer programmes on child nutrition status: Study protocol. BMC Public Health 2015, 15, 1044. [Google Scholar] [CrossRef] [Green Version]
- Stewart, C.P.; Dewey, K.G.; Lin, A.; Pickering, A.J.; Byrd, K.A.; Jannat, K.; Ali, S.; Rao, G.; Dentz, H.N.; Kiprotich, M.; et al. Effects of lipid-based nutrient supplements and infant and young child feeding counseling with or without improved water, sanitation, and hygiene (WASH) on anemia and micronutrient status: Results from 2 cluster-randomized trials in Kenya and Bangladesh. Am. J. Clin. Nutr. 2019, 109, 148–164. [Google Scholar] [CrossRef] [Green Version]
- Huda, T.M.N.; Unicomb, L.; Johnston, R.B.; Halder, A.K.; Sharker, A.Y.; Luby, S.P. Interim evaluation of a large scale sanitation, hygiene and water improvement programme on childhood diarrhea and respiratory disease in rural Bangladesh. Soc. Sci. Med. 2012, 75, 604–611. [Google Scholar] [CrossRef]
- Otsuka, Y.; Agestika, L.; Widyarani; Sintawardani, N.; Yamauchi, T. Risk Factors for Undernutrition and Diarrhea Prevalence in an Urban Slum in Indonesia: Focus on Water, Sanitation, and Hygiene. Am. J. Trop. Med. Hyg. 2019, 100, 727–732. [Google Scholar] [CrossRef] [Green Version]
- Mostafa, I.; Naila, N.N.; Mahfuz, M.; Roy, M.; Faruque, A.S.G.; Ahmed, T. Children living in the slums of Bangladesh face risks from unsafe food and water and stunted growth is common. Acta Paediatr. 2018, 107, 1230–1239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aw, J.Y.H.; Clarke, N.E.; McCarthy, J.S.; Traub, R.J.; Amaral, S.; Huque, H.; Andrews, R.M.; Gray, D.J.; Clements, A.C.A.; Nery, S.V. Giardia duodenalis infection in the context of a community-based deworming and water, sanitation and hygiene trial in Timor-Leste. Parasites Vectors 2019, 12, 491. [Google Scholar] [CrossRef]
- Dangour, A.D.; Watson, L.; Cumming, O.; Boisson, S.; Che, Y.; Velleman, Y.; Cavill, S.; Allen, E.; Uauy, R. Interventions to improve water quality and sup-ply, sanitation and hygiene practices, and their effects on the nutritional status of children. Cochrane Database Syst. Rev. 2013, 8, 84. [Google Scholar]
- Kimani-Murage, E.W.; Kyobutungi, C.; Ezeh, A.C.; Wekesah, F.; Wanjohi, M.; Muriuki, P.; Musoke, R.N.; A Norris, S.; Griffiths, P.; Madise, N.J. Effectiveness of personalised, home-based nutritional counselling on infant feeding practices, morbidity and nutritional outcomes among infants in Nairobi slums: Study protocol for a cluster randomised controlled trial. Trials 2013, 14, 445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Na, M.; Mehra, S.; Christian, P.; Ali, H.; Shaikh, S.; Shamim, A.A.; Labrique, A.B.; Klemm, R.D.; Wu, L.S.; West, K.P. Maternal Dietary Diversity Decreases with Household Food Insecurity in Rural Bangladesh: A Longitudinal Analysis. J. Nutr. 2016, 146, 2109–2116. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, P.H.; Strizich, G.; Lowe, A.; Nguyen, H.; Pham, H.; Truong, T.V.; Nguyen, S.; Martorell, R.; Ramakrishnan, U. Food consumption patterns and associated factors among Vietnamese women of reproductive age. Nutr. J. 2013, 12, 126. [Google Scholar] [CrossRef] [Green Version]
- Ryckman, T.; Robinson, M.; Pedersen, C.; Bhattacharya, J.; Bendavid, E. Impact of Feed the Future initiative on nutrition in chil-dren aged less than 5 years in sub-Saharan Africa: Difference-in-differences analysis. BMJ 2019, 367, l6540. [Google Scholar] [CrossRef] [Green Version]
- Argaw, A.; Hanley-Cook, G.; De Cock, N.; Kolsteren, P.; Huybregts, L.; Lachat, C. Drivers of Under-Five Stunting Trend in 14 Low- and Middle-Income Countries since the Turn of the Millennium: A Multilevel Pooled Analysis of 50 Demographic and Health Surveys. Nutrients 2019, 11, 2485. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Keywords Searched by Boolean Operators | nt | nf |
|---|---|---|
| (food security) AND (nutritional status) AND (low and middle income countries) | 41 | 2 |
| ((water OR sanitation OR hygiene) OR (WASH)) AND (nutritional status) AND (low and middle income countries) | 58 | 1 |
| (food security) AND (malnutrition) AND (low and middle income countries) | 38 | 1 |
| (pregnancy OR pregnant) AND ((water AND sanitation) OR WASH) AND (nutritional status OR malnutrition) | 58 | 3 |
| ((water AND hygiene AND sanitation) OR WASH) AND (disease) AND (malnutrition OR undernutrition) AND ((pregnant or pregnancy) OR (children)) | 55 | 1 |
| ((water AND sanitation AND hygiene) OR WASH) AND (nutritional status) | 155 | 12 |
| (food security) AND (nutritional status) | 2466 | 137 |
| ((water AND sanitation AND hygiene) OR (WASH)) AND (food security) | 222 | 10 |
| (water contaminants) AND (low and middle income countries) | 8 | 1 |
| (WASH) AND (intervention) AND (low and middle income countries) | 38 | 2 |
| (food security) AND (nutritional status) AND (low and middle income countries) | 32 | 20 |
| (water AND sanitation AND hygiene) AND (malnutrition OR undernutrition) AND (low and middle income countries) | 8 | 6 |
| (water AND sanitation AND hygiene) AND (food security) AND (low and middle income countries) | 2 | 1 |
| (pregnant OR pregnancy) AND (malnutrition OR undernutrition) AND (low and middle income countries) | 109 | 55 |
| 3290 | 252 |
| Type of Intervention | Author | Study Design | Study Location | Sample Size | Participant | Dimension of Intervention | Main Findings | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| EduNC | RUTF | MiS | MaS | VO | |||||||
| Food-based and nutritional | Kureishy S | cRCTC | Pakistan | 7360 | PLW | * | * | Effectiveness of food-based interventions in managing stunting | |||
| Kimani-Murage EW | cRCTC | Kenya | 1110 mother-child pairs | PLW | * | Basic nutritional training and/or provision of information may be adequate in improving exclusive breastfeeding rates in communities significantly | |||||
| Ara G | Study protocol | Bangladesh | 205 mother-child pairs | WM and CH 6–18 | * | The results provide robust evidence to improve the linear growth of children in developing countries by integrated intervention | |||||
| Frongillo EA | cRCTC | Bangladesh | 300 pregnant women and 1000 recently delivered women | PLW | * | Household food insecurity was reduced in areas where nutrition-focused antenatal care was implemented. The integration of nutrition interventions into the maternal, newborn, child program was feasible and well implemented | |||||
| Menasria L | cRCTC | Cambodia | 360 | CHL5 | * | * | Adding supplementary foods to education and counselling (CEN) activities did not improve young child nutritional status, as compared to CEN alone. Nutrition education and couselling alone was as effective as combining it with food supplements with regard to the impact on child anthropometry. | ||||
| Sigh S | Prospective RCT | Cambodia | 121 | CHL5 | * | A locally produced ready-to-use therapeutic food (RUTF) might be as effective in terms of weight gain as an imported milk-based RUTF. | |||||
| Borg B | ProspectivecRCTC | Cambodia | 540 | CH 6–18 | * | * | * | There is a need to develop locally produced and culturally acceptable RUSF, and to compare these with existing options for preventing malnutrition. This trial contributed to compare the effectiveness of supplementary foods with animal-source food and milk | |||
| Le port A | cRCTC | Senegal | 321 | CH 18 | * | * | Anaemia prevalence was very high at baseline (80%) and dropped to close to 60% at endline. Haemoglobin increased by 0.55 g/dL, 95%OI more in the intervention compared to the control group after one year, in models that controlled for potentially confounding factors. The impact was greater for boys compared to girls. | ||||
| Campbell RK | cRCTC | Bangladesh | 5499 | CH 6–18 | * | * | Child dietary diversity is low. The meeting of the minimum dietary diversity (MDD) was equal or greater in the supplemented group with home foods than the control group at all ages. High socioeconomic status and maternal education were associated with increased odds of MDD, whereas household security was not associated with MDD. | ||||
| Na M | cRCTC | Bangladesh | 14,600 | WRA | * | * | Poverty and poor maternal education were recognized as important determinants that influence quality of diet. Economic and social strategies may be required to overcome food insecurity beyond maternal education itself. | ||||
| Fenn B | cRCT | Pakistan | CHL5 | * | Different modalities of cash-based transfer work best to reduce the risk of wasting during a season where food insecurity is at its highest. | ||||||
| Shaheen R | RCT | Bangladesh | 4436 | PLW | * | The combination of an early intervention to prenatal food supplementation and multiple micronutrient supplementation lowered mortality in children younger than five years and reduced the gap in child survival chances between social groups. | |||||
| Nguyen PH | RCT | Vietnam | 4983 | WRA and PLW | * | * | Poor dietary intakes and diet quality among underprivileged women (lower education, farers, and those living in households with lower socio-economic status) suggests that nutrition programs and policies should be linked with social development programs. | ||||
| Ryckman T | Difference-in- quasi-experimental approach | 33 Countries in Sub-Saharan Africa | 883,309 | CHL5 | * | Feed the Future’s activities were linked to notable improvements in stunting and underweight levels and moderate improvements in wasting in children <5 years. | |||||
| Ghosh-Jerath S | Cross-sectional study design | India | 280 households per tribal group (3) | All | * | This study provides the first comprehensive examination of the food system of tribal communities. Interventions help to support the sustainable production and consumption of indigenous foods. Also, interventions address the burden of malnutrition in the tribal communities. | |||||
| Stevens B | Cross-sectional study | Bangladesh | 288 | PLW | * | Dietary diversity and household food security were sensitive to seasonal variations. Women had higher dietary diversity in autumn and winter. Household food insecurity peaked during autumn and was lesser in spring. | |||||
| Mutisya M | Prospective longitudinal trial | Kenya | 6858 | CHL5 | * | Stunting was highest among poorest households and lowest among the least poor households. The proportion of children who were stunted was higher among mothers with lower levels of education. | |||||
| Lander RL | RCT | Guatemala, India, Pakistan and DR of Congo | 988 | PLW | * | * | Dietary patterns varied widely among sites. Significantly higher intakes of most key nutrients were observed in participants with adequate dietary diversity. There is a likely need for micronutrient supplementation in pregnancy as well as supporting the value of increasing dietary diversity. | ||||
| Hasan MT | Series of cross-sectional nationally representative DHS data | Bangladesh | 28,941 | CHL5 | * | Children of mothers with secondary or higher education had a lower risk of childhood stunting, underweight and wasting. Promoting women’s education at least up to secondary level has great importance as a means to tackle the malnutrition in Bangladesh. | |||||
| Food-based & WASH | Shafique S | Cluster randomized trial | Bangladesh | 467 | CH 6 | * | * | The use of mineral- and vitamin-enhanced micronutrient powders reduced stunting significantly. On the contrary, the use of a water-based hygiene and sanitation did not have an additive effect. | |||
| Mostafa I | Cross-sectional study | Bangladesh | 370 | WM | * | A total of 83% of the selected households experienced food insecurity. Mothers or caregivers in slums are less likely to have higher levels of education on hygienic practices. The poor personal hygiene practices of mothers, especially hand washing practices before food preparation, may be a contributing factor to the high contamination rate. All water samples were contaminated with faeces. | |||||
| Stewart CP | 2 cRCTC | Kenya and Bangladesh | 699 Kenya and 1470 Bangladesh | PLW, CHL5 | * | * | The distribution of lipid-based nutrition supplements resulted in a lower prevalence of anaemia and iron deficiency in both countries. There were also reductions in the prevalence of low vitamin B12 status. | ||||
| WASH | Schlegelmilch MP | Cluster randomized comparison study | Kenya | 250 | All | Improvements from baseline were observed, yet overall levels of latrine coverage are still low. The findings challenge the assumption that providing WASH infrastructure and education will result in behaviour change. | |||||
| Tsuka Y | Cross-sectional study | Indonesia | 228 pairs of children and their caretakers | CHL5 | * | Not using a towel for hand washing practices was significantly associated with an increased risk of stunting. Children from households using tap water as drinking water were associated with an increased risk of stunting and thinness compared with households using tank water. Children from households using open containers for water storage were associated with an increased risk of diarrhoea. | |||||
| Nurul TM | Cross sectional survey | Bangladesh | 1000 households for observation, 1700 for cross sectional and 1000 for diarrhoea | CHW and CHL5 | * | After 18 months of promoting key behaviours related to sanitation, hygiene and safe water, the improvements were modest. No reduction in the prevalence of diarrhoea or respiratory disease in children <5 years was observed. Eighteen months of the program were not sufficient to produce the targeted behaviour. | |||||
| Aw JYH | cRCTC | Timor-Leste | 24 communities | PLW, WM, WRA, CHL5 | * | No impact was found from community-based WASH intervention in terms of reducing G. duodenalis prevalence. Risk factors for G. duodenalis included living in a household with a child <5 years, living in a household with more than six people, and sampling during the rainy season. | |||||
| Lin A | cRCTC | Bangladesh | 4102 available women, 6694 children | PLW | * | Individual hand washing and hygienic sanitation interventions reduced childhood Giardia infections. There were no effects from chlorinated drinking water and nutrition improvements. Combined WASH interventions provided no additional benefit in this context. | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urgell-Lahuerta, C.; Carrillo-Álvarez, E.; Salinas-Roca, B. Interventions on Food Security and Water Uses for Improving Nutritional Status of Pregnant Women and Children Younger Than Five Years in Low-Middle Income Countries: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 4799. https://doi.org/10.3390/ijerph18094799
Urgell-Lahuerta C, Carrillo-Álvarez E, Salinas-Roca B. Interventions on Food Security and Water Uses for Improving Nutritional Status of Pregnant Women and Children Younger Than Five Years in Low-Middle Income Countries: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(9):4799. https://doi.org/10.3390/ijerph18094799
Chicago/Turabian StyleUrgell-Lahuerta, Cristina, Elena Carrillo-Álvarez, and Blanca Salinas-Roca. 2021. "Interventions on Food Security and Water Uses for Improving Nutritional Status of Pregnant Women and Children Younger Than Five Years in Low-Middle Income Countries: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 9: 4799. https://doi.org/10.3390/ijerph18094799
APA StyleUrgell-Lahuerta, C., Carrillo-Álvarez, E., & Salinas-Roca, B. (2021). Interventions on Food Security and Water Uses for Improving Nutritional Status of Pregnant Women and Children Younger Than Five Years in Low-Middle Income Countries: A Systematic Review. International Journal of Environmental Research and Public Health, 18(9), 4799. https://doi.org/10.3390/ijerph18094799