
Home and Neighborhood Physical Activity Location Availability among African American Adolescent Girls Living in Low-Income, Urban Communities: Associations with Objectively Measured Physical Activity

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Objective 1 (Methodological): To Generate a Replicable Neighborhood-Level PALAS and Apply This Score to Baltimore City Neighborhoods
2.1.1. PALAS Development
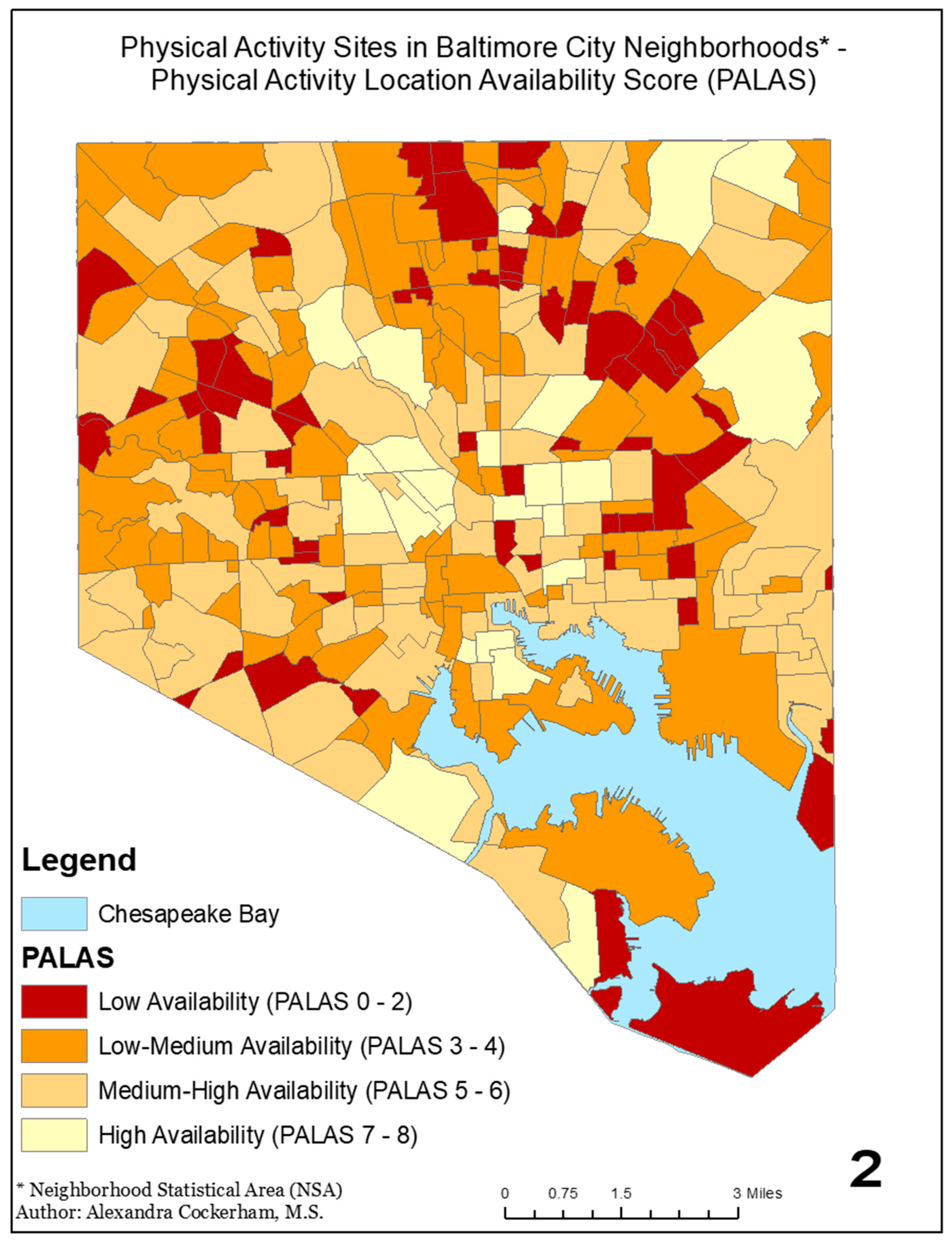
2.1.2. PALAS Map
2.2. Objective 2 (Applied): To Examine the Relationship between Objectively Measured PA among Predominantly African American Adolescent Girls and the PALAS Ratings of Both Their Neighborhood and the Area within 0.25 Miles of Their Homes
2.2.1. Sample
2.2.2. Demographics
2.2.3. Anthropometrics
2.2.4. Accelerometry
2.2.5. Neighborhood PALAS
2.2.6. PA Locations Near the Home
2.2.7. Data Analysis
3. Results
3.1. Sample Description
3.2. Neighborhood PALAS and Objectively Measured PA
3.3. PA Locations near the Home and Objectively Measured PA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- USDHHS. Physical Activity Guidelines for Americans, 2nd ed.; U.S. Department of Health and Human Services: Washington, DC, USA, 2018.
- Väistö, J.; Haapala, E.A.; Viitasalo, A.; Schnurr, T.M.; Kilpeläinen, T.O.; Karjalainen, P.; Westgate, K.; Lakka, H.-M.; Laaksonen, D.E.; Ekelund, U.; et al. Longitudinal associations of physical activity and sedentary time with cardiometabolic risk factors in children. Scand. J. Med. Sci. Sports 2019, 29, 113–123. [Google Scholar] [CrossRef]
- Keane, E.; Li, X.; Harrington, J.M.; Fitzgerald, A.P.; Perry, I.J.; Kearney, P.M. Physical Activity, Sedentary Behavior and the Risk of Overweight and Obesity in School-Aged Children. Pediatr. Exerc. Sci. 2017, 29, 408. [Google Scholar] [CrossRef]
- Dale, L.P.; Vanderloo, L.; Moore, S.; Faulkner, G. Physical activity and depression, anxiety, and self-esteem in children and youth: An umbrella systematic review. Ment. Health Phys. Act. 2019, 16, 66–79. [Google Scholar] [CrossRef]
- Schwarzfischer, P.; Gruszfeld, D.; Stolarczyk, A.; Ferre, N.; Escribano, J.; Rousseaux, D.; Moretti, M.; Mariani, B.; Verduci, E.; Koletzko, B.; et al. Physical Activity and Sedentary Behavior From 6 to 11 Years. Pediatrics 2019, 143, e20180994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- CAHMI. National Survey of Childrens Health Health; CAHMI: Washington, DC, USA, 2016. [Google Scholar]
- Tate, N.H.; Dillaway, H.E.; Yarandi, H.N.; Jones, L.M.; Wilson, F.L. An Examination of Eating Behaviors, Physical Activity, and Obesity in African American Adolescents: Gender, Socioeconomic Status, and Residential Status Differences. J. Pediatric Health Care 2015, 29, 243–254. [Google Scholar] [CrossRef] [PubMed]
- Parise, I. The built environment and obesity. Aust. J. Gen. Pract. 2020, 49, 226–230. [Google Scholar] [CrossRef]
- Bird, E.L.; Ige, J.O.; Pilkington, P.; Pinto, A.; Petrokofsky, C.; Burgess-Allen, J. Built and natural environment planning principles for promoting health: An umbrella review. BMC Public Health 2018, 18, 930. [Google Scholar] [CrossRef] [PubMed]
- Özbil, A.; Yeşiltepe, D.; Argın, G. Home and school environmental correlates of childhood BMI. J. Transp. Health 2020, 16, 100823. [Google Scholar] [CrossRef]
- Jia, P.; Zou, Y.; Wu, Z.; Zhang, D.; Wu, T.; Smith, M.; Xiao, Q. Street connectivity, physical activity, and childhood obesity: A systematic review and meta-analysis. Obes. Rev. 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Day, K. Built environmental correlates of physical activity in China: A review. Prev. Med. Rep. 2016, 3, 303–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, X.; Zhao, L.; Luo, J.; Li, Y.; Zhang, L.; Wu, T.; Smith, M.; Dai, S.; Jia, P. Access to bike lanes and childhood obesity: A systematic review and meta-analysis. Obes. Rev. 2021, 22, e13042. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, X.; Zhou, S.; Wu, W. The association between spatial access to physical activity facilities within home and workplace neighborhoods and time spent on physical activities: Evidence from Guangzhou, China. Int. J. Health Geogr. 2020, 19, 22. [Google Scholar] [CrossRef] [PubMed]
- Blanck, H.M.; Allen, D.; Bashir, Z.; Gordon, N.; Goodman, A.; Merriam, D.; Rutt, C. Let’s Go to the Park Today: The Role of Parks in Obesity Prevention and Improving the Public’s Health. Child. Obes. 2012, 8, 423–428. [Google Scholar] [CrossRef] [Green Version]
- Grow, H.M.; Saelens, B.E.; Kerr, J.; Durant, N.H.; Norman, G.J.; Sallis, J.F. Where are youth active? Roles of proximity, active transport, and built environment. Med. Sci. Sports Exerc. 2008, 40, 2071–2079. [Google Scholar] [CrossRef] [Green Version]
- Oreskovic, N.M.; Blossom, J.; Field, A.E.; Chiang, S.R.; Winickoff, J.P.; Kleinman, R.E. Combining global positioning system and accelerometer data to determine the locations of physical activity in children. Geospat Health 2012, 6, 263–272. [Google Scholar] [CrossRef]
- Ward, J.S.; Duncan, J.S.; Jarden, A.; Stewart, T. The impact of children’s exposure to greenspace on physical activity, cognitive development, emotional wellbeing, and ability to appraise risk. Health Place 2016, 40, 44–50. [Google Scholar] [CrossRef]
- An, R.; Shen, J.; Yang, Q.; Yang, Y. Impact of built environment on physical activity and obesity among children and adolescents in China: A narrative systematic review. J. Sport Health Sci. 2019, 8, 153–169. [Google Scholar] [CrossRef]
- Casey, R.; Chaix, B.; Weber, C.; Schweitzer, B.; Charreire, H.; Salze, P.; Badariotti, D.; Banos, A.; Oppert, J.M.; Simon, C. Spatial accessibility to physical activity facilities and to food outlets and overweight in French youth. Int. J. Obes. 2012, 36, 914–919. [Google Scholar] [CrossRef] [Green Version]
- TIGER/Line Shapefiles: Metropolitan Statistical Areas; United States Census Bureau: Washington DC, USA, 2014.
- Jia, P.; Cao, X.; Yang, H.; Dai, S.; He, P.; Huang, G.; Wu, T.; Wang, Y. Green space access in the neighbourhood and childhood obesity. Obes. Rev. 2020, 22, e13100. [Google Scholar] [CrossRef]
- Benjamin-Neelon, S.E.; Platt, A.; Bacardi-Gascon, M.; Armstrong, S.; Neelon, B.; Jimenez-Cruz, A. Greenspace, physical activity, and BMI in children from two cities in northern Mexico. Prev. Med. Rep. 2019, 14, 100870. [Google Scholar] [CrossRef] [PubMed]
- McCrorie, P.R.W.; Fenton, C.; Ellaway, A. Combining GPS, GIS, and accelerometry to explore the physical activity and environment relationship in children and young people—A review. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 93. [Google Scholar] [CrossRef] [Green Version]
- Wolch, J.; Jerrett, M.; Reynolds, K.; McConnell, R.; Chang, R.; Dahmann, N.; Brady, K.; Gilliland, F.; Su, J.G.; Berhane, K. Childhood obesity and proximity to urban parks and recreational resources: A longitudinal cohort study. Health Place 2011, 17, 207–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, P.; Cheng, X.; Xue, H.; Wang, Y. Applications of geographic information systems (GIS) data and methods in obesity-related research. Obes. Rev. 2017, 18, 400–411. [Google Scholar] [CrossRef] [PubMed]
- Aguayo, L.; Khan, M.; De Leon, R., Jr.; Schwingel, A. Use of Geographic Information Systems in Physical Activity Interventions: A Systematic Review. Prog. Prev. Med. (N. Y.) 2019, 4, e0022. [Google Scholar] [CrossRef]
- Smith, M.; Hosking, J.; Woodward, A.; Witten, K.; MacMillan, A.; Field, A.; Baas, P.; Mackie, H. Systematic literature review of built environment effects on physical activity and active transport—An update and new findings on health equity. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 158. [Google Scholar] [CrossRef]
- Ravensbergen, L.; Buliung, R.N.; Wilson, K.; Faulkner, G. Socioeconomic Discrepancies in Children’s Access to Physical Activity Facilities: Activity Space Analysis. Transp. Res. Rec. 2016, 2598, 11–18. [Google Scholar] [CrossRef]
- Van Dyke, M.E.; Cheung, P.C.; Franks, P.; Gazmararian, J.A. Socioeconomic and Racial/Ethnic Disparities in Physical Activity Environments in Georgia Elementary Schools. Am. J. Health Promot. 2017, 32, 453–463. [Google Scholar] [CrossRef]
- Goodway, J.D.; Smith, D.W. Keeping All Children Healthy: Challenges to Leading an Active Lifestyle for Preschool Children Qualifying for At-Risk Programs. Fam. Community Health J. Health Promot. Maint. 2005, 28, 142–155. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.H.; Kim, K. A review of factors limiting physical activity among young children from low-income families. J. Exerc. Rehabil. 2017, 13, 375–377. [Google Scholar] [CrossRef]
- Sallis, J.F.; Cervero, R.B.; Ascher, W.; Henderson, K.A.; Kraft, M.K.; Kerr, J. An ecological approach to creating active living communities. Annu. Rev. Public Health 2006, 27, 297–322. [Google Scholar] [CrossRef] [Green Version]
- Bureau, U.C. (Ed.) 2010 Census Data—City of Baltimore—City Neighorbood Statistical Areas; Summary File 1 ed.; Department of Planning: Baltimore, MD, USA.
- Baltimore’s Neighborhood Statistical Areas—2010; Baltimore City Department of Planning: Baltimore, MD, USA, 2020. Available online: planning.baltimorecity.gov/sites/default/files/NeighborhoodStatisticalAreas1220.pdf (accessed on 4 May 2021).
- Google Maps. Available online: https://www.google.com/maps (accessed on 5 May 2021).
- Redesigning Suburbia for Walking and Transit: Emerging Concepts. J. Urban Plan. Dev. 1994, 120, 48–57. [CrossRef]
- Pushkarev, B.; Zupan, J. Urban Space for Pedestrians: A Report of the Regional Plan Association; MIT Press: Cambridge, MA, USA, 1975. [Google Scholar]
- Yeh, C.-T.; Cheng, Y.-Y.; Liu, T.-Y. Spatial Characteristics of Urban Green Spaces and Human Health: An Exploratory Analysis of Canonical Correlation. Int. J. Environ. Res. Public Health 2020, 17, 3227. [Google Scholar] [CrossRef] [PubMed]
- Akpinar, A.; Cankurt, M. How are characteristics of urban green space related to levels of physical activity: Examining the links. Indoor Built Environ. 2016, 26, 1091–1101. [Google Scholar] [CrossRef]
- Braubach, M.; Egorov, A.; Mudu, P.; Wolf, T.; Thompson, C.W.; Martuzzi, M. Effects of urban green space on environmental health, equity and resilience. In Nature-Based Solutions to Climate Change Adaptation in Urban Areas; Springer: Cham, Switzerland, 2017; pp. 187–205. [Google Scholar]
- Flowers, E.P.; Freeman, P.; Gladwell, V.F. A cross-sectional study examining predictors of visit frequency to local green space and the impact this has on physical activity levels. BMC Public Health 2016, 16, 420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Zhou, S.; Kwan, M.-P.; Chen, F.; Lin, R. Impacts of Individual Daily Greenspace Exposure on Health Based on Individual Activity Space and Structural Equation Modeling. Int. J. Environ. Res. Public Health 2018, 15, 2323. [Google Scholar] [CrossRef] [Green Version]
- Kärmeniemi, M.; Lankila, T.; Ikäheimo, T.; Koivumaa-Honkanen, H.; Korpelainen, R. The Built Environment as a Determinant of Physical Activity: A Systematic Review of Longitudinal Studies and Natural Experiments. Ann. Behav. Med. 2018, 52, 239–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reuben, A.; Rutherford, G.W.; James, J.; Razani, N. Association of neighborhood parks with child health in the United States. Prev. Med. 2020, 141, 106265. [Google Scholar] [CrossRef]
- Ribeiro, A.I.; Pires, A.; Carvalho, M.S.; Pina, M.F. Distance to parks and non-residential destinations influences physical activity of older people, but crime doesn’t: A cross-sectional study in a southern European city. BMC Public Health 2015, 15, 593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tewahade, S.; Li, K.; Goldstein, R.B.; Haynie, D.; Iannotti, R.J.; Simons-Morton, B. Association between the built environment and active transportation among U.S. adolescents. J. Transp. Health 2019, 15, 100629. [Google Scholar] [CrossRef]
- Kaufman, T.K.; Rundle, A.; Neckerman, K.M.; Sheehan, D.M.; Lovasi, G.S.; Hirsch, J.A. Neighborhood Recreation Facilities and Facility Membership Are Jointly Associated with Objectively Measured Physical Activity. J. Urban Health 2019, 96, 570–582. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, L. Associations between spatial access to physical activity facilities and frequency of physical activity; how do home and workplace neighbourhoods in West Central Scotland compare? Int. J. Health Geogr. 2019, 18, 2. [Google Scholar] [CrossRef] [Green Version]
- Hager, E.R.; Treuth, M.S.; Gormely, C.; Epps, L.; Snitker, S.; Black, M.M. Ankle Accelerometry for Assessing Physical Activity Among Adolescent Girls: Threshold Determination, Validity, Reliability, and Feasibility. Res. Q. Exerc. Sport 2015, 86, 397–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cromley, E.; McLafferty, S. GIS and Public Health, 2nd ed.; The Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Kann, L.; Kinchen, S.A.; Williams, B.I.; Ross, J.G.; Lowry, R.; Hill, C.V.; Grunbaum, J.A.; Blumson, P.S.; Collins, J.L.; Kolbe, L.J. Youth risk behavior surveillance—United States, 1997. Mmwr. Cdc Surveill. Summ. Morb. Mortal. Wkly. Rep. Cdc Surveill. Summ./Cent. Dis. Control 1998, 47, 1–89. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Simons-Morton, B.G.; Stone, E.J.; Corbin, C.B.; Epstein, L.H.; Faucette, N.; Iannotti, R.J.; Killen, J.D.; Klesges, R.C.; Petray, C.K.; et al. Determinants of physical activity and interventions in youth. Med. Sci. Sports Exerc. 1992, 24 (Suppl. 6), S248–S257. [Google Scholar] [CrossRef]
- Heath, G.W.; Pratt, M.; Warren, C.W.; Kann, L. Physical activity patterns in American high school students. Results from the 1990 Youth Risk Behavior Survey. Arch. Pediatrics Adolesc. Med. 1994, 148, 1131–1136. [Google Scholar] [CrossRef]
- Aaron, D.J.; Kriska, A.M.; Dearwater, S.R.; Anderson, R.L.; Olsen, T.L.; Cauley, J.A.; Laporte, R.E. The epidemiology of leisure physical activity in an adolescent population. Med. Sci. Sports Exerc. 1993, 25, 847–853. [Google Scholar] [CrossRef] [PubMed]
- Corder, K.; Sharp, S.J.; Atkin, A.J.; Andersen, L.B.; Cardon, G.; Page, A.; Davey, R.; Grøntved, A.; Hallal, P.C.; Janz, K.F.; et al. Age-related patterns of vigorous-intensity physical activity in youth: The International Children’s Accelerometry Database. Prev. Med. Rep. 2016, 4, 17–22. [Google Scholar] [CrossRef] [Green Version]
- Corder, K.; Sharp, S.J.; Atkin, A.J.; Griffin, S.J.; Jones, A.P.; Ekelund, U.; van Sluijs, E.M.F. Change in objectively measured physical activiy during the transition to adolescence. Br. J. Sports Med. 2015, 49, 730–736. [Google Scholar] [CrossRef] [Green Version]
- Chiaki, T.; Xanne, J.; Mark, P.; Kathryn, P.; Laura, B.; Ashley, A.; John, J.R. Bidirectional Associations Between Adiposity, Sedentary Behavior, and Physical Activity: A Longitudinal Study in Children. J. Phys. Act. Health 2018, 15, 918–926. [Google Scholar]
- Janssen, X.; Basterfield, L.; Parkinson, K.N.; Pearce, M.S.; Reilly, J.K.; Adamson, A.J.; Reilly, J.J. Non-linear longitudinal associations between moderate-to-vigorous physical activity and adiposity across the adiposity distribution during childhood and adolescence: Gateshead Millennium Study. Int. J. Obes. 2019, 43, 744–750. [Google Scholar] [CrossRef] [Green Version]
- Yan, A.F.; Voorhees, C.C.; Beck, K.H.; Wang, M.Q. A social ecological assessment of physical activity among urban adolescents. Am. J. Health Behav. 2014, 38, 379–391. [Google Scholar] [CrossRef] [PubMed]
- Johnson, K.A.; Showell, N.N.; Flessa, S.; Janssen, M.; Reid, N.; Cheskin, L.J.; Thornton, R.L.J. Do Neighborhoods Matter? A Systematic Review of Modifiable Risk Factors for Obesity among Low Socio-Economic Status Black and Hispanic Children. Child. Obes. 2018, 15, 71–86. [Google Scholar] [CrossRef]
- Telford, R.M.; Telford, R.D.; Olive, L.S.; Cochrane, T.; Davey, R. Why Are Girls Less Physically Active than Boys? Findings from the LOOK Longitudinal Study. PLoS ONE 2016, 11, e0150041. [Google Scholar] [CrossRef] [PubMed]
- Kavita, A.G.; Kelli, L.C.; Terry, L.C.; Brian, E.S.; Lawrence, D.F.; Jacqueline, K.; Karen, G.; James, F.S. Associations Between Neighborhood Recreation Environments and Adolescent Physical Activity. J. Phys. Act. Health 2019, 16, 880–885. [Google Scholar]
- Loh, V.H.Y.; Veitch, J.; Salmon, J.; Cerin, E.; Thornton, L.; Mavoa, S.; Villanueva, K.; Timperio, A. Built environment and physical activity among adolescents: The moderating effects of neighborhood safety and social support. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 132. [Google Scholar] [CrossRef] [Green Version]
- Carlson, S.A.; Brooks, J.D.; Brown, D.R.; Buchner, D.M. Racial/Ethnic differences in perceived access, environmental barriers to use, and use of community parks. Prev. Chronic. Dis. 2010, 7, A49–A59. [Google Scholar]
- Sandra, E.E.; Amiee Luan, K.; Carmen, R.I.; Janice, J.-D.; Dula, P. A Community Survey on Neighborhood Violence, Park Use, and Physical Activity Among Urban Youth. J. Phys. Act. Health 2014, 11, 186–194. [Google Scholar]
- Larson, N.I.; Story, M.T.; Nelson, M.C. Neighborhood environments: Disparities in access to healthy foods in the U.S. Am. J. Prev. Med. 2009, 36, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Galvez, M.P.; Pearl, M.; Yen, I.H. Childhood obesity and the built environment. Curr. Opin. Pediatr. 2010, 22, 202–207. [Google Scholar] [CrossRef] [Green Version]
- Hager, E.R.; Witherspoon, D.O.; Gormley, C.; Latta, L.W.; Pepper, M.R.; Black, M.M. The perceived and built environment surrounding urban schools and physical activity among adolescent girls. Ann. Behav. Med. 2013, 45 (Suppl. 1), S68–S75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poitras, V.J.; Gray, C.E.; Borghese, M.M.; Carson, V.; Chaput, J.-P.; Janssen, I.; Katzmarzyk, P.T.; Pate, R.R.; Connor Gorber, S.; Kho, M.E.; et al. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 2016, 41 (Suppl. 3), S197–S239. [Google Scholar] [CrossRef] [PubMed]
- Boone-Heinonen, J.; Gordon-Larsen, P.; Guilkey, D.K.; Jacobs, D.R.; Popkin, B.M. Environment and physical activity dynamics: The role of residential self-selection. Psychol. Sport Exerc. 2011, 12, 54–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamidi, S.; Ewing, R. Compact Development and BMI for Young Adults. J. Am. Plan. Assoc. 2020, 86, 349–363. [Google Scholar] [CrossRef]
- Bustad, J.; Andrews, D. Remaking recreation: Neoliberal urbanism and public recreation in Baltimore. Cities 2020, 103, 102757. [Google Scholar] [CrossRef]

{kind=link}
| Variable | Threshold Definition | Description | References: Support for Inclusion | ||
|---|---|---|---|---|---|
| NSA | HNA | ||||
| 1 | Green Space | Y(1)/N(0) | Y(1)/N(0) | Green space that could possibly be used for PA (includes institutional land, open urban land, deciduous forest, evergreen forest, and mixed forest) | [40,41,42,43,44] |
| 2 | Parks | Y(1)/N(0) | Y(1)/N(0) | Parks at least one acre in area and that have at least one feature (ballfield, basketball court, playground, tennis court, multiuse field, volleyball court, fitness stations, multiuse trails, and paths) | [20,45,46,47] |
| 3 | Recreation Center | Y(1)/N(0) | Y(1)/N(0) | All city-owned recreation centers | [20,45,48] |
| 4 | Other Government/City-Owned PA Location | Y(1)/N(0) | Y(1)/N(0) | All city-owned (school and non-school) PA locations (ice rinks, soccer pavilions, tennis courts, pools, school playground, park playground, multiuse fields/courts, basketball courts, ballfields, golf courses, volleyball courts, bocce ball courts, horseshoe pits, outdoor fitness stations, skate parks, kayak/canoe launch points, dog parks, specialty boxing center, and specialty recreation facility) (see 4a–4b for more detailed lists) | [20,45,48] |
| 4a School-Owned PALocation | -- | Y(1)/N(0) | All school-owned PA locations (playgrounds, ice rinks, multiuse fields, basketball court, etc.) | [20,45,48] | |
| 4b Non-School Other Government/City-Owned PA Location | -- | Y(1)/N(0) | All non-school-owned PA locations (ice rinks, soccer pavilions, etc.) | [20,45,48] | |
| 5 | Private PA Location | Y(1)/N(0) | Y(1)/N(0) | All for-profit, non-profit, and residential PA locations (see 5a–5c for detailed lists) | [48,49,50] |
| 5a For-Profit PA Location | - | Y(1)/N(0) | All for-profit PA locations (gyms, health clubs, studios (gymnastics, yoga, pilates, boot camp, cross-fit, mixed martial arts, dance, karate, rock climbing, and roller blading), tennis courts, pools, fitness centers, ice rinks, golf courses [indoor and outdoor], skate parks, bowling alleys, and disc golf courses) | [20,49,50] | |
| 5b Non-Profit PA Location | -- | Y(1)/N(0) | All non-profit PA locations (Y of Central Maryland, community center) | [20,49,50] | |
| 5c Residential PA Location | -- | Y(1)/N(0) | All residential PA locations (gyms, fitness centers, health clubs, and pools) | [20,49,50] | |
| 6 | Park Proximity Buffer * | Y(1)/N(0) | -- | Parks at least one acre in area and that have at least one feature (ballfield, basketball court, playground, tennis court, multiuse field, volleyball court, fitness stations, multiuse trails, and paths) | [20,45,47] |
| 7 | Recreation Center Proximity Buffer * | Y(1)/N(0) | -- | All city-owned recreation centers | [20,45,48] |
| 8 | Other Government/City-Owned PA Facility Proximity Buffer * | Y(1)/N(0) | -- | All city-owned (school and non-school) PA locations (ice rinks, soccer pavilions, tennis courts, pools, school playground, park playground, multiuse fields, basketball courts, ballfields, golf courses, volleyball courts, bocce ball courts, horseshoe pits, outdoor fitness stations, skate parks, kayak/canoe launch points, dog parks, specialty boxing center, and specialty recreation facility) | [20,45,48] |
| 9 | Private PA Facility Proximity Buffer * | Y(1)/N(0) | -- | All for-profit, non-profit, and residential PA locations | [49,50] |
| Mean (Range) or % | |
|---|---|
| Age | |
| Years | 11.67 (10–14) |
| Race/Ethnicity | |
| % African American | 89.9% |
| Weight Status | |
| % overweight or obese | 49.7% |
| BMI-for-age z-score | 0.99 (−3.56–2.91) |
| Physical Activity | |
| Walks to and/or from school | 41.1% |
| Minutes Per Day Spent in MVPA | 41.95 (0–255.33) |
| Square Root (MVPA) | 6.16 (0–15.01) |
| Percent of NSAs with (x = #) Value (%) | Cumulative Percent (%) | |
|---|---|---|
| PALAS (x = 0) | 0.7% | 0.7% |
| PALAS (x = 1) | 2.0% | 2.7% |
| PALAS (x = 2) | 4.1% | 6.8% |
| PALAS (x = 3) | 8.1% | 15.0% |
| PALAS (x = 4) | 23.1% | 38.0% |
| PALAS (x = 5) | 18.6% | 56.6% |
| PALAS (x = 6) | 18.6% | 75.1% |
| PALAS (x = 7) | 20.0% | 95.1% |
| PALAS (x = 8) | 4.9% | 100.0% |
| Mean% | |
|---|---|
| Private | 13.7% |
| Residential (subset of private) | 4.3% |
| Non-Profit (subset of private) | 4.3% |
| For-Profit (subset of private) | 7.9% |
| Parks | 58.0% |
| Recreation Centers | 32.1% |
| All government | 74.2% |
| School government (subset of all government) | 52.3% |
| Other government (not-school) (subset of all government) | 59.8% |
| β (p) | 95% CI | |
|---|---|---|
| Intercept | 1.921 (0.181) | −0.893, 4.736 |
| PALAS | 0.102 (0.041) | 0.004, 0.200 |
| Age | 0.322 (0.006) | 0.094, 0.549 |
| BMI z-score | −0.191 (0.018) | −0.650, −0.033 |
| Mean | t (p) | β (p) | 95% CI | ||
|---|---|---|---|---|---|
| Private | Present | 6.34 | 0.86 (0.39) | 0.252 (0.305) | −0.229, 0.733 |
| Not Present | 6.13 | ||||
| Residential (subset of private) | Present | 6.29 | 0.334 (0.74) | 0.275 (0.509) | −0.543, 1.092 |
| Not Present | 6.15 | ||||
| Non-Profit (subset of private) | Present | 6.87 | 1.788 (0.07) | 0.663 (0.109) | −0.149, 1.476 |
| Not Present | 6.13 | ||||
| For-Profit (subset of private) | Present | 6.23 | 0.243 (0.81) | 1.199 (0.228) | −0.755, 3.153 |
| Not Present | 6.15 | ||||
| Parks | Present | 6.22 | 0.85 (0.34) | 0.412 (0.082) | −0.052, 0.875 |
| Not Present | 6.07 | ||||
| Recreation Centers | Present | 6.51 | 2.846 (0.01) ** | 0.461(0.011) ** | 0.108, 0.815 |
| Not Present | 5.99 | ||||
| All government | Present | 6.28 | 2.376 (0.02) ** | 0.438 (0.068) | −0.032, 0.908 |
| Not Present | 5.82 | ||||
| School location (subset of all government) | Present | 6.34 | 2.27 (0.02) ** | 0.487 (0.140) | −0.161, 1.135 |
| Not Present | 5.96 | ||||
| Other government (not-school) (subset of all government) | Present | 6.27 | 1.652 (0.10) | 0.432 (0.062) | −0.022, 0.886 |
| Not Present | 5.99 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pulling Kuhn, A.; Cockerham, A.; O’Reilly, N.; Bustad, J.; Miranda, V.; Loboda, T.V.; Black, M.M.; Hager, E.R. Home and Neighborhood Physical Activity Location Availability among African American Adolescent Girls Living in Low-Income, Urban Communities: Associations with Objectively Measured Physical Activity. Int. J. Environ. Res. Public Health 2021, 18, 5003. https://doi.org/10.3390/ijerph18095003
Pulling Kuhn A, Cockerham A, O’Reilly N, Bustad J, Miranda V, Loboda TV, Black MM, Hager ER. Home and Neighborhood Physical Activity Location Availability among African American Adolescent Girls Living in Low-Income, Urban Communities: Associations with Objectively Measured Physical Activity. International Journal of Environmental Research and Public Health. 2021; 18(9):5003. https://doi.org/10.3390/ijerph18095003
Chicago/Turabian StylePulling Kuhn, Ann, Alexandra Cockerham, Nicole O’Reilly, Jacob Bustad, Victor Miranda, Tatiana V. Loboda, Maureen M. Black, and Erin R. Hager. 2021. "Home and Neighborhood Physical Activity Location Availability among African American Adolescent Girls Living in Low-Income, Urban Communities: Associations with Objectively Measured Physical Activity" International Journal of Environmental Research and Public Health 18, no. 9: 5003. https://doi.org/10.3390/ijerph18095003
APA StylePulling Kuhn, A., Cockerham, A., O’Reilly, N., Bustad, J., Miranda, V., Loboda, T. V., Black, M. M., & Hager, E. R. (2021). Home and Neighborhood Physical Activity Location Availability among African American Adolescent Girls Living in Low-Income, Urban Communities: Associations with Objectively Measured Physical Activity. International Journal of Environmental Research and Public Health, 18(9), 5003. https://doi.org/10.3390/ijerph18095003