
Is Foundational Movement Skill Competency Important for Keeping Children Physically Active and at a Healthy Weight?

 ,
, 
 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.1.1. Baseline
2.1.2. Follow Up
2.2. Measures
2.2.1. Foundational Movement Skills
2.2.2. Anthropometry
2.2.3. Physical Activity
2.3. Data Analysis
3. Results
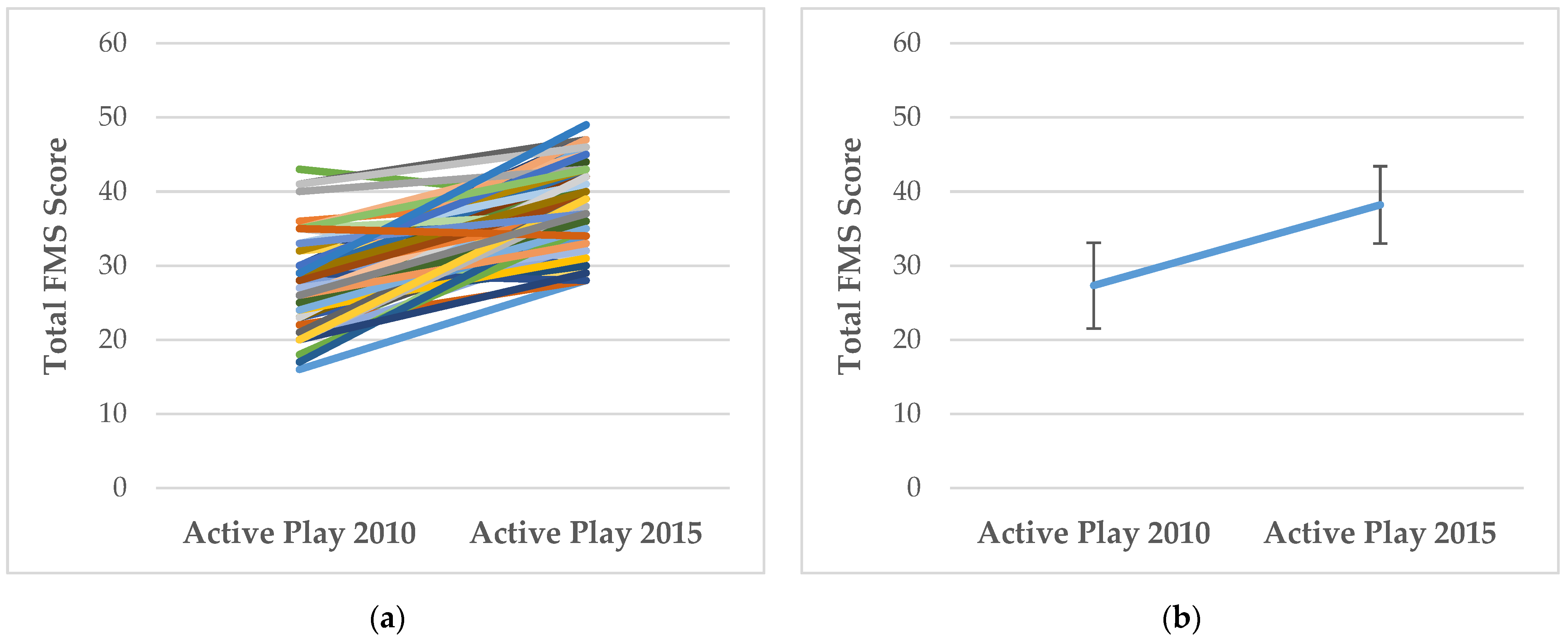
3.1. How Does FMS Competency and MVPA Change with Age?
3.2. Does Baseline FMS Competence Predict MVPA at Follow Up?
3.3. Does Baseline MVPA Predict FMS Competence at Follow-Up?
3.4. How Does the Association between FMS and MVPA Change between Baseline and Follow-Up?
3.5. Does Baseline FMS Competency Predict Follow-Up Weight Classification?
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hulteen, R.M.; Morgan, P.J.; Barnett, L.M.; Stodden, D.F.; Lubans, D.R. Development of Foundational Movement Skills: A Conceptual Model for Physical Activity Across the Lifespan. Sports Med. 2018, 48, 1533–1540. [Google Scholar] [CrossRef] [PubMed]
- Stodden, D.F.; Goodway, J.D.; Langendorfer, S.J.; Roberton, M.A.; Rudisill, M.E.; Garcia, C.; Garcia, L.E. A Developmental Perspective on the Role of Motor Skill Competence in Physical Activity: An Emergent Relationship. Quest 2008, 60, 290–306. [Google Scholar] [CrossRef]
- Gallahue, D.L.; Ozmun, J.C.; Goodway, J.D. Understanding Motor Development: Infants, Children, Adolescents, Adults, 7th ed.; McGraw Hill: New York, NY, USA, 2012. [Google Scholar]
- Clark, J.E.; Metcalfe, J.S. The mountain of motor development: A methaphor. In Motor Development: Research and Reviews; Clarke, J.E., Humphrey, J.H., Eds.; National Association of Sport and Physical Education: Reston, VA, USA, 2002; Volume 2, pp. 163–190. [Google Scholar]
- Lima, R.A.; Pfeiffer, K.; Larsen, L.R.; Bugge, A.; Moller, N.C.; Anderson, L.B.; Stodden, D.F. Physical Activity and Motor Competence Present a Positive Reciprocal Longitudinal Relationship Across Childhood and Early Adolescence. J. Phys. Act. Health 2017, 14, 440–447. [Google Scholar] [CrossRef] [PubMed]
- De Meester, A.; Stodden, D.; Goodway, J.; True, L.; Brian, A.; Ferkel, R.; Haerens, L. Identifying a motor proficiency barrier for meeting physical activity guidelines in children. J. Sci. Med. Sport 2018, 21, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Foulkes, J.D.; Knowles, Z.; Fairclough, S.J.; Stratton, G.; O’Dwyer, M.V.; Ridgers, N.D.; Foweather, L. Fundamental movement skills of preschool children in Northwest England. Percept. Mot. Ski. 2015, 121, 260–283. [Google Scholar] [CrossRef]
- Dobell, A.; Pringle, A.; Faghy, M.A.; Roscoe, C.M.P. Fundamental Movement Skills and Accelerometer-Measured Physical Activity Levels during Early Childhood: A Systematic Review. Children 2020, 7, 224. [Google Scholar] [CrossRef]
- Department for Health and Social Care. UK Chief Medical Officers’ Physical Activity Guidelines 2019. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/832868/uk-chief-medical-officers-physical-activity-guidelines.pdf (accessed on 30 September 2021).
- Tinner, L.; Kipping, R.; White, J.; Jago, R.; Metcalfe, C.; Hollingworth, W. Cross-sectional analysis of physical activity in 2–4-year-olds in England with paediatric quality of life and family expenditure on physical activity. BMC Public Health 2019, 19, 846. [Google Scholar] [CrossRef]
- Carson, V.; Lee, E.Y.; Hewitt, L.; Jennings, C.; Hunter, S.; Kuzik, N.; Stearns, J.A.; Unrau, S.P.; Poitras, V.J.; Gray, C.; et al. Systematic review of the relationships between physical activity and health indicators in the early years (0–4 years). BMC Public Health 2017, 17, 854. [Google Scholar] [CrossRef]
- Robinson, L.E.; Stodden, D.F.; Barnett, L.M.; Lopes, V.P.; Logan, S.W.; Rodrigues, L.P.; D’Hondt, E. Motor Competence and its Effect on Positive Developmental Trajectories of Health. Sports Med. 2015, 45, 1273–1284. [Google Scholar] [CrossRef]
- D’Hondt, E.; Deforche, B.; Vaeyens, R.; Vandorpe, B.; Vandendriessche, J.; Pion, J.; Philippaerts, R.; de Bourdeaudhuij, I.; Lenoir, M. Gross motor coordination in relation to weight status and age in 5- to 12-year-old boys and girls: A cross-sectional study. Int. J. Pediatr. Obes. 2011, 6, e556–e564. [Google Scholar] [CrossRef]
- Barnett, L.M.; Webster, E.K.; Hulteen, R.M.; De Meester, A.; Valentini, N.C.; Lenoir, M.; Pesce, C.; Getchell, N.; Lopes, V.P.; Robinson, L.E.; et al. Through the Looking Glass: A Systematic Review of Longitudinal Evidence, Providing New Insight for Motor Competence and Health. Sports Med. 2021, 1–46. [Google Scholar] [CrossRef]
- Barnett, L.M.; Van Beurden, E.; Morgan, P.J.; Brooks, L.O.; Beard, J.R. Childhood motor skill proficiency as a predictor of adolescent physical activity. J. Adolesc. Health 2009, 44, 252–259. [Google Scholar] [CrossRef]
- Lopes, V.P.; Stodden, D.F.; Bianchi, M.M.; Maia, J.A.R.; Rodrigues, L.P. Correlation between BMI and motor coordination in children. J. Sci. Med. Sport 2012, 15, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Kiphard, E.J.; Schilling, F. Körperkoordinationstest Für Kinder Überarbeitete und Ergänzte Auflage [Body Coordination Test for Children. Revised and Supplemented Edition]; Beltz Test GmbH: Göttingen, Germany, 2007. [Google Scholar]
- Fisher, A.; Reilly, J.J.; Kelly, L.A.; Montgomery, C.; Williamson, A.; Paton, J.Y.; Grant, S. Fundamental movement skills and habitual physical activity in young children. Med. Sci. Sports Exerc. 2005, 37, 684–688. [Google Scholar] [CrossRef]
- Williams, H.G.; Pfeiffer, K.A.; O’Neill, J.R.; Dowda, M.; McIver, K.; Brown, W.H.; Pate, R.R. Motor skill performance and physical activity in preschool children. Obesity 2008, 16, 1421–1426. [Google Scholar] [CrossRef]
- Cliff, D.P.; Okely, A.D.; Smith, L.M.; McKeen, K. Relationships between fundamental movement skills and objectively measured physical activity in preschool children. Pediatr. Exerc. Sci. 2009, 21, 436–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burgi, F.; Meyer, U.; Granacher, U.; Schindler, C.; Marques-Vidal, P.; Kriemler, S.; Puder, J.J. Relationship of physical activity with motor skills, aerobic fitness and body fat in preschool children: A cross-sectional and longitudinal study (Ballabeina). Int. J. Obes. 2011, 35, 937–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iivonen, K.S.; Sääkslahti, A.K.; Mehtälä, A.; Villberg, J.J.; Tammelin, T.H.; Kulmala, J.S.; Poskiparta, M. Relationship Between Fundamental Motor Skills And Physical Activity In 4-year-old Preschool Children. Percept. Mot. Ski. 2013, 117, 627–646. [Google Scholar] [CrossRef] [PubMed]
- Roscoe, C.M.P.; James, R.S.; Duncan, M.J. Accelerometer-based physical activity levels, fundamental movement skills and weight status in British preschool children from a deprived area. Eur. J. Pediatr. 2019, 178, 1043–1052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bryant, E.S.; James, R.S.; Birch, S.L.; Duncan, M. Prediction of habitual physical activity level and weight status from fundamental movement skill level. J. Sports Sci. 2014, 32, 1775–1782. [Google Scholar] [CrossRef]
- Zask, A.; Barnett, L.; Ros, L.; Brooks, L.; Molyneux, M.; Hughes, D.; Adams, J.; Salmon, J. Does a movement skill intervention in preschools result in movement skill and physical activity outcomes three years later? J. Sci. Med. Sport 2012, 15, S61. [Google Scholar] [CrossRef]
- Cohen, K.; Morgan, P.J.; Plotnikoff, R.; Callister, R.; Lubans, D. Fundamental movement skills and physical activity among children living in low-income communities: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rich, C.; Griffiths, L.; Dezateux, C. Seasonal variation in accelerometer-determined sedentary behaviour and physical activity in children: A review. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carson, V.; Spence, J.C. Seasonal Variation in Physical Activity Among Children and Adolescents: A Review. Pediatr. Exerc. Sci. 2010, 22, 81–92. [Google Scholar] [CrossRef] [Green Version]
- Foweather, L.; Knowles, Z.; Ridgers, N.D.; O’Dwyer, M.V.; Foulkes, J.D.; Stratton, G. Fundamental movement skills in relation to weekday and weekend physical activity in preschool children. J. Sci. Med. Sport 2015, 18, 691–696. [Google Scholar] [CrossRef]
- Foweather, L.; Crotti, M.; Foulkes, J.D.; O’Dwyer, M.V.; Utesch, T.; Knowles, Z.R.; Fairclough, S.J.; Ridgers, N.D.; Stratton, G. Foundational Movement Skills and Play Behaviors during Recess among Preschool Children: A Compositional Analysis. Children 2021, 8, 543. [Google Scholar] [CrossRef] [PubMed]
- Foulkes, J.D.; Knowles, Z.; Fairclough, S.J.; Stratton, G.; O’Dwyer, M.; Ridgers, N.D.; Foweather, L. Effect of a 6-Week Active Play Intervention on Fundamental Movement Skill Competence of Preschool Children. Percept. Mot. Ski. 2017, 124, 393–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Dwyer, M.; Fairclough, S.J.; Ridgers, N.D.; Knowles, Z.R.; Foweather, L.; Stratton, G. Patterns of Objectively Measured Moderate-to-Vigorous Physical Activity in Preschool Children. J. Phys. Act. Health 2014, 11, 1233–1238. [Google Scholar] [CrossRef] [Green Version]
- O’Dwyer, M.V.; Fairclough, S.J.; Ridgers, N.D.; Knowles, Z.R.; Foweather, L.; Stratton, G. Effect of a school-based active play intervention on sedentary time and physical activity in preschool children. Health Educ. Res. 2013, 28, 931–942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stratton, G.; Canoy, D.; Boddy, L.M.; Taylor, S.R.; Hackett, A.F.; Buchan, I.E. Cardiorespiratory fitness and body mass index of 9–11-year-old English children: A serial cross-sectional study from 1998 to 2004. Int. J. Obes. 2007, 31, 1172–1178. [Google Scholar] [CrossRef] [Green Version]
- Boddy, L.M.; Fairclough, S.J.; Hackett, A.F.; Stratton, G. Changes in cardiorespiratory fitness in 9-to 10.9 yr-old children: SportsLinx 1998–2010. Med. Sci. Sports Exerc. 2012, 44, 481–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Association of Public Health Observatories. Liverpool Health Profile 2009. Available online: www.apho.org.uk/resource/view.aspx?RID=71192 (accessed on 30 April 2015).
- Children Schools and Families Committee. Sure Start Children’s Centres. Commons; The Stationary Office: London, UK, 2010. [Google Scholar]
- Department of Communities and Local Government. The English Indices of Deprivation: Annual Report; Department of Education: London, UK, 2010. [Google Scholar]
- Ulrich, D.A. Test of Gross Motor Development: Examiner’s Manual, 2nd ed.; PRO-ED: Austin, TX, USA, 2000. [Google Scholar]
- Williams, H.G.; Pfeiffer, K.A.; Dowda, M.; Jeter, C.; Jones, S.; Pate, R.R. A field-based testing protocol for assessing gross motor skills in preschool children: The CHAMPS motor skills protocol (CMSP). Meas. Phys. Educ. Exerc. Sci. 2009, 13, 151–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Mars, H. Observer Reliability: Issues and Procedures. In Analyzing Physical Education and Sport Instruction; Darst, P.W., Zakrajsek, D.B., Mancini, V.H., Eds.; Human Kinetics: Champaign, IL, USA, 1989; pp. 53–80. [Google Scholar]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jimmy, G.; Seiler, R.; Mäder, U. Comparing the Validity and Output of the GT1M and GT3X Accelerometer in 5- to 9-Year-Old Children. Meas. Phys. Educ. Exerc. Sci. 2013, 17, 236–248. [Google Scholar] [CrossRef]
- Janssen, X.; Cliff, D.P.; Reilly, J.J.; Hinkley, T.; Jones, R.A.; Batterham, M.; Ekelund, U.; Brage, S.; Okely, A.D. Predictive Validity and Classification Accuracy of ActiGraph Energy Expenditure Equations and Cut-Points in Young Children. PLoS ONE 2013, 8, e79124. [Google Scholar] [CrossRef]
- Evenson, K.R.; Catellier, D.J.; Gill, K.; Ondrak, K.S.; McMurray, R.G. Calibration of two objective measures of physical activity for children. J. Sports Sci. 2008, 26, 1557–1565. [Google Scholar] [CrossRef]
- Pate, R.R.; Almeida, M.J.; McIver, K.L.; Pfeiffer, K.A.; Dowda, M. Validation and Calibration of an Accelerometer in Preschool Children. Obesity 2006, 14, 2000–2006. [Google Scholar] [CrossRef]
- Trost, S.G.; Loprinzi, P.D.; Moore, R.; Pfeiffer, K.A. Comparison of accelerometer cut points for predicting activity intensity in youth. Med. Sci. Sports Exerc. 2011, 43, 1360–1368. [Google Scholar] [CrossRef]
- Butterfield, S.A.; Angell, R.M.; Mason, C.A. Age and sex differences in object control skills by children ages 5 to 14. Percept. Mot. Ski. 2012, 114, 261–274. [Google Scholar] [CrossRef]
- Navarro-Patón, R.; Mecías-Calvo, M.; Rodríguez Fernández, J.E.; Arufe-Giráldez, V. Relative Age Effect on Motor Competence in Children Aged 4–5 Years. Children 2021, 8, 115. [Google Scholar] [CrossRef]
- Hardy, L.L.; King, L.; Espinel, P.; Cosgrave, C.; Bauman, A. NSW Schools Physical Activity and Nutrition Survey (SPANS) 2010: Full Report; NSW Ministry of Health: Sydney, Australia, 2010. [Google Scholar]
- O’Brien, W.; Issartel, J.; Belton, S. Evidence for the efficacy of the youth-physical activity towards health (Y-PATH) intervention. Adv. Phys. Educ. 2013, 3, 145–153. [Google Scholar] [CrossRef] [Green Version]
- LeGear, M.; Greyling, L.; Sloan, E.; Bell, R.; Williams, B.-L.; Naylor, P.-J.; Temple, V. A window of opportunity? Motor skills and perceptions of competence of children in Kindergarten. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bryant, E.S.; Duncan, M.J.; Birch, S.L. Fundamental movement skills and weight status in British primary school children. Eur. J. Sport Sci. 2014, 14, 730–736. [Google Scholar] [CrossRef] [PubMed]
- Okely, A.D.; Booth, M.L. Mastery of fundamental movement skills among children in New South Wales: Prevalence and sociodemographic distribution. J. Sci. Med. Sport 2004, 7, 358–372. [Google Scholar] [CrossRef]
- Van Beurden, E.; Zask, A.; Barnett, L.M.; Dietrich, U.C. Fundamental movement skills—How do primary school children perform? The “move it groove it” program in rural Australia. J. Sci. Med. Sport 2002, 5, 244–252. [Google Scholar] [CrossRef]
- Goodway, J.D.; Robinson, L.E.; Crowe, H. Gender Differences in Fundamental Motor Skill Development in Disadvantaged Preschoolers From Two Geographical Regions. Res. Q. Exerc. Sport 2010, 81, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Morley, D.; Till, K.; Ogilvie, P.; Turner, G. Influences of gender and socioeconomic status on the motor proficiency of children in the UK. Hum. Mov. Sci. 2015, 44, 150–156. [Google Scholar] [CrossRef]
- Goodway, J.D.; Smith, D.W. Keeping all children healthy: Challenges to leading an active lifestyle for preschool children qualifying for at-risk programs. Fam. Community Health 2005, 28, 142–155. [Google Scholar] [CrossRef]
- Barnett, L.M.; Ridgers, N.D.; Salmon, J. Associations between young children’s perceived and actual ball skill competence and physical activity. J. Sci. Med. Sport 2015, 18, 167–171. [Google Scholar] [CrossRef]
- Hardy, L.L.; King, L.; Farrell, L.; Macniven, R.; Howlett, S. Fundamental movement skills among Australian preschool children. J. Sci. Med. Sport 2010, 13, 503–508. [Google Scholar] [CrossRef]
- Van Cauwenberghe, E.; Jones, R.; Hinkley, T.; Crawford, D.; Okely, A. Patterns of physical activity and sedentary behaviour in preschool children. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hesketh, K.; McMinn, A.; Ekelund, U.; Sharp, S.; Collings, P.; Harvey, N.; Godfrey, K.; Inskip, H.; Cooper, C.; van Sluijs, E. Objectively measured physical activity in four-year-old British children: A cross-sectional analysis of activity patterns segmented across the day. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortega, F.B.; Konstabel, K.; Pasquali, E.; Ruiz, J.R.; Hurtig-Wennlöf, A.; Mäestu, J.; Löf, M.; Harro, J.; Bellocco, R.; Labayen, I.; et al. Objectively Measured Physical Activity and Sedentary Time during Childhood, Adolescence and Young Adulthood: A Cohort Study. PLoS ONE 2013, 8, e60871. [Google Scholar] [CrossRef] [Green Version]
- Cools, W.; De Martelaer, K.; Samaey, C.; Andries, C. Fundamental movement skill performance of preschool children in relation to family context. J. Sports Sci. 2011, 29, 649–660. [Google Scholar] [CrossRef] [PubMed]
- Barnett, L.M.; Hinkley, T.; Okely, A.D.; Salmon, J. Child, family and environmental correlates of children’s motor skill proficiency. J. Sci. Med. Sport 2013, 16, 332–336. [Google Scholar] [CrossRef] [Green Version]
- Sterdt, E.; Liersch, S.; Walter, U. Correlates of physical activity of children and adolescents: A systematic review of reviews. Health Educ. J. 2014, 73, 72–89. [Google Scholar] [CrossRef]
- Lopes, V.P.; Rodrigues, L.P.; Maia, J.; Malina, R. Motor coordination as predictor of physical activity in childhood. Scand. J. Med. Sci. Sports 2011, 21, 663–669. [Google Scholar] [CrossRef]
- Sirard, J.R.; Pate, R.R. Physical Activity Assessment in Children and Adolescents. Sports Med. 2001, 31, 439–454. [Google Scholar] [CrossRef] [PubMed]
- Erwin, H.E.; Castelli, D.M. National Physical Education Standards: A summary of student performance and its correlates. Res. Q. Exerc. Sport 2008, 79, 495–505. [Google Scholar] [CrossRef]
- Graf, C.; Koch, B.; Kretschmann-Kandel, E.; Falkowski, G.; Christ, H.; Coburger, S.; Lehmacher, W.; Bjarnason-Wehrens, B.; Platen, P.; Tokarski, W.; et al. Correlation between BMI, leisure habits and motor abilities in childhood (CHILT-Project). Int. J. Obes. 2004, 28, 22–26. [Google Scholar] [CrossRef] [Green Version]
- Southall, J.E.; Okely, A.; Steele, J.R. Actual and perceived physical competence in overweight and non-overweight children. Pediatr. Exerc. Sci. 2004, 16, 15–24. [Google Scholar] [CrossRef]
- D’Hondt, E.; Deforche, B.; Gentier, I.; De Bourdeaudhuij, I.; Vaeyens, R.; Philippaerts, R.; Lenoir, M. A longitudinal analysis of gross motor coordination in overweight and obese children versus normal-weight peers. Int. J. Obes. 2013, 37, 61–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cliff, D.P.; Okely, A.D.; Morgan, P.J.; Steele, J.R.; Jones, R.A.; Colyvas, K.; Baur, L.A. Movement Skills and Physical Activity in Obese Children: Randomized Controlled Trial. Med. Sci. Sports Exerc. 2011, 43, 90–100. [Google Scholar] [CrossRef] [PubMed]
- D’Hondt, E.; Gentier, I.; Deforche, B.; Tanghe, A.; De Bourdeaudhuij, I.; Lenoir, M. Weight Loss and Improved Gross Motor Coordination in Children as a Result of Multidisciplinary Residential Obesity Treatment. Obesity 2011, 19, 1999–2005. [Google Scholar] [CrossRef]
- Cliff, D.P.; Okely, A.D.; Morgan, P.J.; Jones, R.A.; Steele, J.R.; Baur, L.A. Proficiency Deficiency: Mastery of Fundamental Movement Skills and Skill Components in Overweight and Obese Children. Obesity 2012, 20, 1024–1033. [Google Scholar] [CrossRef] [PubMed]
- Han, A.; Fu, A.; Cobley, S.; Sanders, R.H. Effectiveness of exercise intervention on improving fundamental movement skills and motor coordination in overweight/obese children and adolescents: A systematic review. J. Sci. Med. Sport 2018, 21, 89–102. [Google Scholar] [CrossRef]
- Okely, A.D.; Booth, M.L.; Chey, T. Relationships between Body Composition and Fundamental Movement Skills among Children and Adolescents. Res. Q. Exerc. Sport 2004, 75, 238–247. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Active Play 2010 | Active Play 2015 | |||||
|---|---|---|---|---|---|---|
| Measure | Boys | Girls | Total | Boys | Girls | Total |
| (n = 38) | (n= 37) | (n = 75) | (n = 38) | (n = 37) | (n = 75) | |
| Age (y) | 4.5 ± 0.6 | 4.6 ± 0.4 | 4.6 ±0.5 | 10.0 ± 0.6 * | 10.0 ± 0.4 * | 10.0 ± 0.5 * |
| BMI (kg/m2) | 16.7 ± 1.8 | 16.6 ± 1.9 | 16.7 ± 1.8 | 18.5 ± 3.4 * | 18.7 ± 3.6 * | 18.6 ± 3.5 * |
| BMI-z Score (IOTF) | 0.7 ± 1.1 | 0.7 ± 1.1 | 0.7 ± 1.1 | 0.7 ± 1.1 | 0.7 ± 1.1 | 0.7 ± 1.1 |
| MVPA (min) | 95.6 ± 22.8 | 84.9 ± 25.3 | 90.3 ± 24.5 | 78.6 ± 23.6 * | 59.3 ± 14.3 * | 69.0 ± 21.7 * |
| Wear Time (min) | 780.3 ± 105.7 | 778.6 ± 97.9 | 779.5 ± 101.2 | 698.5 ± 57.3 * | 692.2 ± 57.4 * | 695.4 ± 57.1 * |
| Total FMS ‡ | 28.2 ± 5.9 | 26.41 ± 5.6 | 27.3 ± 5.8 | 40.1 ± 5.0 * | 36.2 ± 4.8 * | 38.2 ± 5.2 * |
| OC Score ‡ | 12.3 ± 3.8 | 9.5 ± 3.0 | 11.0 ± 3.7 | 19.5 ± 4.1 * | 15.0 ± 3.6 * | 17.3 ± 4.4 * |
| LM Score ‡ | 15.9 ± 3.7 | 16.9 ± 3.6 | 16.4 3.6 | 20.7 ± 2.3 * | 21.2 ± 2.9 * | 20.9 ± 2.6 * |
| Temperature (°C) | 9.8 ±1.1 | 10.1 ± 1.0 | 9.9 ± 1.0 | 15.5 ± 1.5 * | 15.4 ± 1.3 * | 15.4 ± 1.4 * |
| Rainfall (mm) | 3.3 ± 2.0 | 3.2 ± 2.1 | 3.3 ± 2.0 | 1.5 ± 0.8 * | 1.5 ± 1.1 * | 1.5 ± 1.0 * |
| Daylength (hours) | 11.7 ± 0.9 | 11.6 ± 1.0 | 11.7 ± 0.9 | 16.4 ± 1.1 * | 16.3 ± 1.3 * | 16.4 ± 1.2 * |
| Median (IQR) | ||||||
| Deprivation † | 4.03 (1.1, 20.7) | 3.4 (0.8, 19.8) | 3.84 (1.0, 20.4) | 47.0 (21.0, 59.5)* | 53.0 (31.8, 59.0) * | 50.5 (24.8, 59.0) * |
| Baseline (2010) | Follow-Up (2015) | Repeated Measures ANCOVA | ||||||
|---|---|---|---|---|---|---|---|---|
| Score | NW | OW/OB | NW | OW/OB | FTime | p | FTime × Weight Class | p |
| (n = 52) | (n= 21) | (n = 52) | (n = 21) | |||||
| FMS Score | ||||||||
| Total | 27.65 ± 5.96 | 25.82 ± 5.10 | 38.73 ± 5.21 | 36.33 ± 6.97 | 21.85 | <0.001 * | 0.000 | 0.99 |
| OC | 11.31 ± 3.65 | 9.62 ± 3.34 | 17.58 ± 4.30 | 15.90 ± 6.08 | 21.33 | <0.001 * | 0.18 | 0.67 |
| LM | 16.35 ± 3.77 | 16.24 ± 3.49 | 21.15 ± 2.52 | 20.43 ± 2.79 | 2.82 | 0.01 * | 0.30 | 0.59 |
| MVPA1 | ||||||||
| MVPA | 88.33 ± 23.72 | 93.19 ± 26.91 | 71.40 ± 22.00 | 62.55 ± 21.11 | 1.31 | 0.26 | 4.95 | 0.03 * |
| Baseline (2010) | Follow-Up (2015) | Repeated Measures ANCOVA | ||||||
|---|---|---|---|---|---|---|---|---|
| Score | Boys | Girls | Boys | Girls | FTime | p | FTime × Weight Class | p |
| (n = 38) | (n= 37) | (n = 38) | (n = 37) | |||||
| FMS Score | ||||||||
| Total | 28.21 ± 5.92 | 26.41 ± 5.57 | 40.11 ± 5.01 | 36.24 ± 4.75 | 37.89 | <0.001 * | 7.53 | 0.007 * |
| OC | 12.34 ± 3.82 | 9.54 ± 2.98 | 19.45 ± 4.05 | 15.03 ± 3.62 | 26.43 | <0.001 * | 5.71 | 0.02 * |
| LM | 15.87 ± 3.66 | 16.86 ± 3.58 | 20.66 ± 2.25 | 21.22 ± 2.89 | 15.46 | <0.001 * | 1.72 | 0.19 |
| MVPA 1 | ||||||||
| MVPA | 95.57 ± 22.83 | 84.87 ± 25.27 | 78.56 ± 23.55 | 59.25 ± 14.30 | 13.86 | <0.001 * | 1.74 | 0.19 |
| Predictor | β | SE | 95% CI | p | r2 | sri2 |
|---|---|---|---|---|---|---|
| Baseline FMS and Baseline MVPA 1 | ||||||
| Total | 1.04 | 0.42 | 0.20 to 1.9 | 0.02 * | 53.8% | 4.53% |
| OC | 0.62 | 0.78 | −0.94 to 2.19 | 0.43 | 54.1% | 0.48% |
| LM | 1.34 | 0.64 | 0.06 to 2.61 | 0.04 * | 3.31% | |
| Baseline FMS and Follow-up MVPA 2 | ||||||
| Total | 0.08 | 0.39 | −0.69 to 0.85 | 0.83 | 47.6% | 0.04% |
| OC | 0.30 | 0.70 | −1.38 to 1.43 | 0.97 | 47.6% | <0.01% |
| LM | 0.13 | 0.65 | −1.16 to 1.43 | 0.84 | 0.04% | |
| Baseline MVPA and Follow-up FMS 3 | ||||||
| Total | 0.04 | 0.03 | −0.20 to 0.11 | 0.19 | 26.6% | 1.96% |
| OC | 0.04 | 0.03 | −0.01 to 0.09 | 0.15 | 39.6% | 2.04% |
| LM | 0.01 | 0.02 | −0.03 to 0.04 | 0.69 | 18.2% | 0.21% |
| Follow-up FMS and Follow-up MVPA 4 | ||||||
| Total | 0.71 | 0.41 | −0.12 to 1.54 | 0.09 | 56.0% | 2.46% |
| OC | 0.75 | 0.55 | −0.35 to 1.86 | 0.08 | 56.0% | 1.56% |
| LM | 0.63 | 0.83 | −1.04 to 2.30 | 0.16 | 0.49% | |
| Predictor | B | SE | 95% CI | Odds Ratio | p |
|---|---|---|---|---|---|
| Total | 0.15 | 0.19 | 0.81 to 1.68 | 1.17 | 0.41 |
| OC | −1.95 | 3.00 | 0.00 to 50.97 | 0.14 | 0.52 |
| LM | 1.42 | 2.04 | 0.08 to 225.57 | 4.12 | 0.49 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Foulkes, J.D.; Knowles, Z.; Fairclough, S.J.; Stratton, G.; O’Dwyer, M.V.; Foweather, L. Is Foundational Movement Skill Competency Important for Keeping Children Physically Active and at a Healthy Weight? Int. J. Environ. Res. Public Health 2022, 19, 105. https://doi.org/10.3390/ijerph19010105
Foulkes JD, Knowles Z, Fairclough SJ, Stratton G, O’Dwyer MV, Foweather L. Is Foundational Movement Skill Competency Important for Keeping Children Physically Active and at a Healthy Weight? International Journal of Environmental Research and Public Health. 2022; 19(1):105. https://doi.org/10.3390/ijerph19010105
Chicago/Turabian StyleFoulkes, Jonathan D., Zoe Knowles, Stuart J. Fairclough, Gareth Stratton, Mareesa V. O’Dwyer, and Lawrence Foweather. 2022. "Is Foundational Movement Skill Competency Important for Keeping Children Physically Active and at a Healthy Weight?" International Journal of Environmental Research and Public Health 19, no. 1: 105. https://doi.org/10.3390/ijerph19010105
APA StyleFoulkes, J. D., Knowles, Z., Fairclough, S. J., Stratton, G., O’Dwyer, M. V., & Foweather, L. (2022). Is Foundational Movement Skill Competency Important for Keeping Children Physically Active and at a Healthy Weight? International Journal of Environmental Research and Public Health, 19(1), 105. https://doi.org/10.3390/ijerph19010105