
Stretching and Multicomponent Training to Functional Capacities of Older Women: A Randomized Study

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
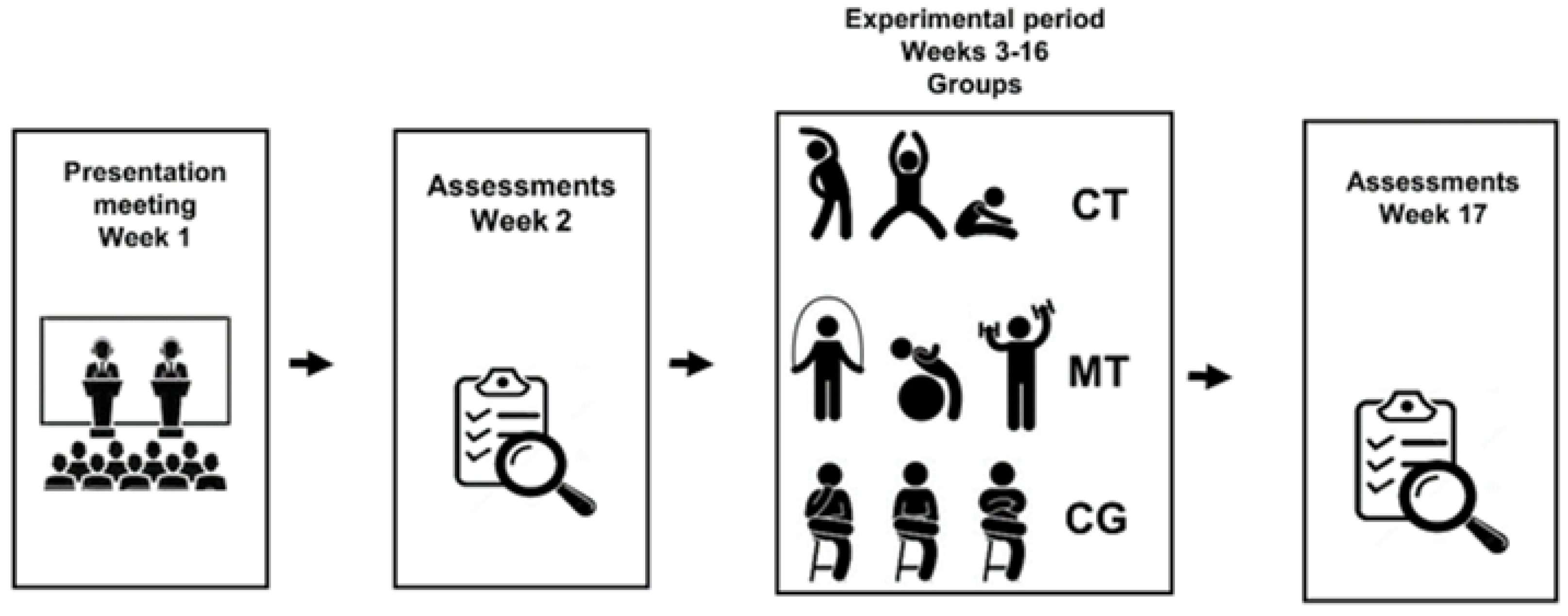
2.1. Study Design
2.2. Participants
2.3. Interventions
2.3.1. Multicomponent Training
2.3.2. Individualized Flexibility Training
2.4. Evaluations
2.4.1. Evaluation of Sample Characterization
2.4.2. Motor Evaluations
2.5. Statistical Analysis
2.6. Data Availability
3. Results
4. Discussion
Limitation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rebelo-Marques, A.; Lages, A.S.; Andrade, R.; Ribeiro, C.F.; Pinto, A.M.; Carrilho, F.; Mendes, J.E. Aging hallmarks: The benefits of physical exercise. Front. Endocrinol. (Lausanne) 2018, 9, 258. [Google Scholar] [CrossRef]
- Labra, C.; Guimaraes, P.C.; Maseda, A.; Lorenzo, T.; Millán, C.J.C. Effects of physical exercise interventions in frail older adults: A systematic review of randomized controlled trials. BMC Geriatr. 2015, 15, 154. [Google Scholar] [CrossRef] [Green Version]
- Huisingh, S.M.; Wroblewski, K.; Kocherginsky, M.; Huang, E.; Dale, W.; Waite, L.; Schumm, L.P. The relationship between physical activity and frailty among U.S. older adults based on hourly accelerometry data. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 622–629. [Google Scholar] [CrossRef]
- Portegijs, E.; Karavirta, L.; Saajanaho, M.; Rantalainen, T.; Rantanen, T. Assessing physical performance and physical activity in large population-based aging studies: Home-based assessments or visits to the research center? BMC Public Health 2019, 19, 1570. [Google Scholar] [CrossRef]
- Thandi, M.K.G.; Phinney, A.; Oliffe, J.L.; Wong, S.; McKay, H.; Sims-Gould, J.; Sahota, S. Engaging older men in physical activity: Implications for health promotion practice. Am. J. Men’s Health 2018, 12, 2064–2075. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010; Available online: https://https://www.who.int/dietphysicalactivity/global-PA-recs-2010.pdf (accessed on 2 June 2021).
- Bangsbo, J.; Blackwell, J.; Boraxbekk, C.J.; Boraxbekk, C.J.; Caserotti, P.; Dela, F.; Vina, J. Copenhagen consensus statement 2019: Physical Activity and Ageing. Br. J. Sports Med. 2019, 53, 856–858. [Google Scholar] [CrossRef] [Green Version]
- Valenti, G.; Bonomi, A.G.; Westerterp, K.R. Multicomponent fitness training improves walking economy in older adults. Med. Sci. Sports Exerc. 2016, 48, 1365–1370. [Google Scholar] [CrossRef]
- Turunen, K.; Salpakoski, A.; Edgren, J.; Törmäkangas, T.; Arkela, M.; Kallinen, M.; Sipilä, S. Physical activity acter a hip fracture: Effect of a multicomponent home-based rehabilitation program-a secondary analysis of a randomized controlled trial. Arch. Phys. Med. Rehabil. 2017, 98, 981–988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machado, O.A.S.; Lima, W.P.; Souza, B.V.; Gianolla, F.; Killian, L.F.; Machado, G.A.C.; Gorjão, R. Comparison of functional capability, flexibility, strength and quality of life in aged women engaged in resistance exercise, weight-bearing training or hydro-gymnastics. J. Sport Sci. 2019, 7, 106–114. [Google Scholar]
- Caldas, L.R.R.; Albuquerque, M.R.; Lopes, E.; Moreira, A.C.; Ribeiro, A.Q.; Carneiro-Júnior, M.A. Multicomponent physical training increases strength, agility and dynamic balance in middle-aged women. Revista Brasileira de Fisiologia do Exercí Cio 2020, 19, 478–488. [Google Scholar] [CrossRef]
- Medeiros, D.M.; Lima, C.S. Influence of chronic stretching on muscle performance: Systematic review. Hum. Mov. Sci. 2017, 54, 220–229. [Google Scholar] [CrossRef]
- Zambon, T.B.; Gonelli, P.R.G.; Gonçalves, R.D.; Borges, B.L.A.; Montebelo, M.D.C. Análise comparativa da flexibilidade de mulheres idosas ativas e não ativas. Acta Fisiatr. 2015, 22, 14–18. [Google Scholar]
- Trapé, A.A.; Lizzi, E.A.D.S.; Gonçalves, T.C.P.; Rodrigues, J.A.L.; Tavares, S.S.; Lacchini, R.; Bueno Junior, C.R. Effect of multicomponent training on blood pressure, nitric oxide, redox status, and physical fitness in older adult women: Influence of endothelial nitric oxide synthase (NOS3) Haplotypes. Oxid. Med. Cell. Longev. 2017, 2017, 2578950. [Google Scholar] [CrossRef] [Green Version]
- Foster, C. Monitoring Training in Athletes with Reference to Overtraining Syndrome. Med. Sci. Sports Exerc. 1998, 30, 1164–1168. [Google Scholar] [CrossRef]
- Borg, G.A.; Noble, B.J. Perceived exertion. Exerc. Sport Sci. Rev. 1974, 2, 131–154. [Google Scholar] [CrossRef]
- Nelson, A.; Kokkonen, J. Stretching Anatomy; Human Kinetics: Champaign, IL, USA, 2007. [Google Scholar]
- Patel, A.V.; Friedenreich, C.M.; Moore, S.C.; Hayes, S.C.; Silver, J.K.; Campbell, K.L.; Matthews, C.E. American college of sports medicine roundtable report on physical activity, sedentary behavior, and cancer prevention and control. Med. Sci. Sports Exerc. 2019, 51, 2391. [Google Scholar] [CrossRef] [Green Version]
- Thong, I.S.K.; Jensen, M.P.; Miró, J.; Tan, G. The validity of pain intensity measures: What do the NRS, VAS, VRS, and FPS-R measure? Scand. J. Pain 2018, 18, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Sobrinho, A.C.S.; Almeida, M.L.; Silva, V.R.R.; Wiggers, E.; Bueno Júnior, C.R. Relationship between cognitive performance, sedentary behavior and physical activity level of brazilian older people women. Alzheimers Dement. 2019, 15, 847. [Google Scholar] [CrossRef]
- Freedson, P.S.; Melanson, E.; Sirard, J. Calibration of the computer science and applications, Inc. accelerometer. Med. Sci. Sports Exerc. 1998, 30, 777–781. [Google Scholar] [CrossRef]
- Riklli, R.E.; Jones, C.J. Development and validation of a functional fitness test for community-residing older adults. J. Aging Phys. Act. 1999, 7, 129–161. [Google Scholar] [CrossRef]
- Osness, W.H.; Adrian, M.; Clark, B.; Hoeger, W.; Raab, D.; Wiswell, R. Functional Fitness Assessment for Adults over 60 Years. 1990. Available online: https://www.scienceopen.com/document?vid=24e042cb-a996-4b68-a239-64b397f9dd53 (accessed on 2 June 2021).
- Lee, D.K. Alternatives to P value: Confidence interval and effect size. Korean J. Anesth. 2016, 69, 555–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leppink, J.; O’Sullivan, P.; Winston, K. Effect size-large, medium, and small. Perspect. Med. Educ. 2016, 5, 347–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bucht, H.; Donath, L. Sauna Yoga Superiorly Improves flexibility, strength, and balance: A two-armed randomized controlled trial in healthy older adults. Int. J. Environ. Res. Public Health 2019, 16, 3721. [Google Scholar] [CrossRef] [Green Version]
- Jung, K.S.; In, T.S.; Cho, H.Y. Effects of sit-to-stand training combined with transcutaneous electrical stimulation on spastiitly, muscle strength and balance ability in patients with stroke: A randomized controlled study. Gait Posture 2017, 54, 183–187. [Google Scholar] [CrossRef]
- Leite, T.B.; Costa, P.B.; Leite, R.D.; Novaes, J.S.; Fleck, S.J.; Simão, R. Effects of different number of sets of resistance training on flexibility. Int. J. Exerc. Sci. 2017, 10, 354–364. [Google Scholar]
- Cadore, E.L.; Sáez de Asteasu, M.L.; Izquierdo, M. Multicomponent exercise and the hallmarks of frailty: Considerations on cognitive impairment and acute hospitalization. Exp. Gerontol. 2019, 122, 10–14. [Google Scholar] [CrossRef]
- Kang, S.; Hwang, S.; Klein, A.B.; Kim, S.H. Multicomponent exercise for physical fitness of community-dwelling older people women. J. Phys. Ther. Sci. 2015, 27, 911–915. [Google Scholar] [CrossRef] [Green Version]
- Lima, C.Z.L. Efeitos da periodização linear versus ondulatório diária no treinamento de força sobre a flexibilidade. Brazilian J. Exerc. Physiol. Prescr. (RBPFEX) 2018, 12, 1037–1044. [Google Scholar]
- Simão, R.; Lemos, A.; Salles, B.; Leite, T.; Oliveira, E.; Rhea, M.; Reis, V.M. The influence of strength, flexibility, and simultaneous training on flexibility and strength gains. J. Strength Cond. Res. 2011, 25, 1333–1338. [Google Scholar] [CrossRef] [PubMed]
- Lyakh, V.; Mikołajec, K.; Bujas, P.; Litkowycz, R. Review of platonov’s “sports training periodization. general theory and its practical application”-kiev: Olympic literature, 2013. J. Hum. Kinet. 2014, 44, 259–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joho, K.; Abe, T.; Seol, J.; Fujii, Y.; Fujii, K.; Okura, T. Examining physical functioning in older adults: A comparison of two stretching practice methods. Innov. Aging 2017, 1, 586. [Google Scholar] [CrossRef] [Green Version]
- Fjerstad, B.M.; Hammer, R.L.; Hammer, A.M.; Connolly, G.; Lomond, K.V.; O’Connor, P. Comparison of two static stretching Procedures on Hip Adductor Flexibility and Strength. Int. J. Exerc. Sci. 2018, 11, 1074–1085. [Google Scholar]
- Kaya, F. Positive Effects of proprioceptive neuromuscular facilitation stretching on sports performance: A review. J. Educ. Train Stud. 2018, 6, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Ball, S.; Gammon, R.; Kelly, P.J.; Cheng, A.L.; Chertoff, K.; Kaume, L.; Abreu, E.L.; Brotto, M. Outcomes of stay strong, stay healthy in community settings. J. Aging Health. 2013, 25, 1388–1397. [Google Scholar] [CrossRef]
- Syed-Abdul, M.M.; Ball, S.D. Muscle activation in older females after a community-based resistance training program: A pilot study. Reports 2021, 4, 38. [Google Scholar] [CrossRef]
- Higgs, F.; Winter, S.L. The effect of a four-week proprioceptive neuromuscular facilitation stretching program on isokinetic torque production. J. Strength Cond. Res. 2009, 23, 1442–1447. [Google Scholar] [CrossRef] [Green Version]
- Brooks, J.H.; Fuller, C.W.; Kemp, S.P.; Reddin, D.B. Incidence, risk, and prevention of hamstring muscle injuries in professional rugby union. Am. J. Sports Med. 2006, 34, 1297–1306. [Google Scholar] [CrossRef]
- Jadczak, A.D.; Makwana, N.; Luscombe-Marsh, N.; Visvanathan, R.; Schultz, T.J. Effectiveness of exercise interventions on physical function in community-dwelling frail older people: An umbrella review of systematic reviews. JBI Database Syst. Rev. Implement Rep. 2018, 16, 752–775. [Google Scholar] [CrossRef] [PubMed]
- Sekendiz, B.; Cuğ, M.; Korkusuz, F. Effects of swiss-ball core strength training on strength, endurance, flexibility, and balance in sedentary. J. Strength Cond. Res. 2010, 24, 3032–3040. [Google Scholar] [CrossRef] [Green Version]
- Richman, E.D.; Tyo, B.M.; Nicks, C.R. Combined effects of self-myofascial release and dynamic stretching on range of motion, jump, sprint, and agility performance. J. Strength Cond. Res. 2019, 33, 1795–1803. [Google Scholar] [CrossRef]
- Donath, L.; van Dieën, J.; Faude, O. Exercise-based fall prevention in the older people: What about agility? Sports Med. 2016, 46, 143–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carneiro, N.H.; Ribeiro, A.S.; Nascimento, M.A.; Gobbo, L.A.; Schoenfeld, B.J.; Júnior, A.A.; Cyrino, E.S. Effects of different resistance training frequencies on flexibility in older women. Clin. Interv. Aging 2015, 10, 531–538. [Google Scholar] [PubMed] [Green Version]

{kind=link}
| MT (n = 52) | CT (n = 4 3) | d-Cohen | |
|---|---|---|---|
| Trimp (au) | 667.0 ± 42.9 | 693.9 ± 58.1 * | 0.533 |
| Borg (au) | 7.3 ± 0.4 | 7.7 ± 0.5 * | 0.889 |
| Monotony (au) | 4.4 ± 1.0 | 5.3 ± 3.1 * | 0.439 |
| MT (n = 52) | CT (n = 43) | CG (n = 47) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Effect Size | Pre | Post | Effect Size | Pre | Post | Effect Size | |
| Sitting and standing (rep) † | 12 ± 4 | 18.1 ± 4.4 * | 1.452 | 13.6 ± 4.4 | 25.1 ± 5.4 *,$ | 2.347 | 12.4 ± 5.1 | 11.3 ± 5.4 #,$ | 0.210 |
| Elbow flexion and extension (rep) † | 14.6 ± 4.4 | 20 ± 4.7 * | 1.187 | 16.7 ± 3.8 | 27.2 ± 4.3 *,$ | 2.593 | 13.7 ± 4.7 | 14.8 ± 3.5 #,$ | 0.268 |
| Six-minute walk (m) † | 522.2 ± 70.7 | 594.7 ± 119.6 | 0.762 | 526.8 ± 56.9 | 716.9 ± 68.2 *,$ | 3.039 | 520.9 ± 66.7 | 558.8 ± 78.6 # | 0.522 |
| Agility (s) † | 26.9 ± 3.2 | 25 ± 3.4 * | 0.576 | 27.4 ± 4 | 19.6 ± 4 *,$ | 1.950 | 25.2 ± 3.4 | 27.6 ± 2.4 #,$ | 0.828 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sobrinho, A.C.d.S.; Almeida, M.L.d.; Rodrigues, G.d.S.; Bertani, R.F.; Lima, J.G.R.; Bueno Junior, C.R. Stretching and Multicomponent Training to Functional Capacities of Older Women: A Randomized Study. Int. J. Environ. Res. Public Health 2022, 19, 27. https://doi.org/10.3390/ijerph19010027
Sobrinho ACdS, Almeida MLd, Rodrigues GdS, Bertani RF, Lima JGR, Bueno Junior CR. Stretching and Multicomponent Training to Functional Capacities of Older Women: A Randomized Study. International Journal of Environmental Research and Public Health. 2022; 19(1):27. https://doi.org/10.3390/ijerph19010027
Chicago/Turabian StyleSobrinho, Andressa Crystine da Silva, Mariana Luciano de Almeida, Guilherme da Silva Rodrigues, Rodrigo Fenner Bertani, Joao Gabriel Ribeiro Lima, and Carlos Roberto Bueno Junior. 2022. "Stretching and Multicomponent Training to Functional Capacities of Older Women: A Randomized Study" International Journal of Environmental Research and Public Health 19, no. 1: 27. https://doi.org/10.3390/ijerph19010027