
Trends in Complementary Feeding Indicators and Intake from Specific Food Groups among Children Aged 6–23 Months in Bangladesh

 ,
,  , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Outcome Measures
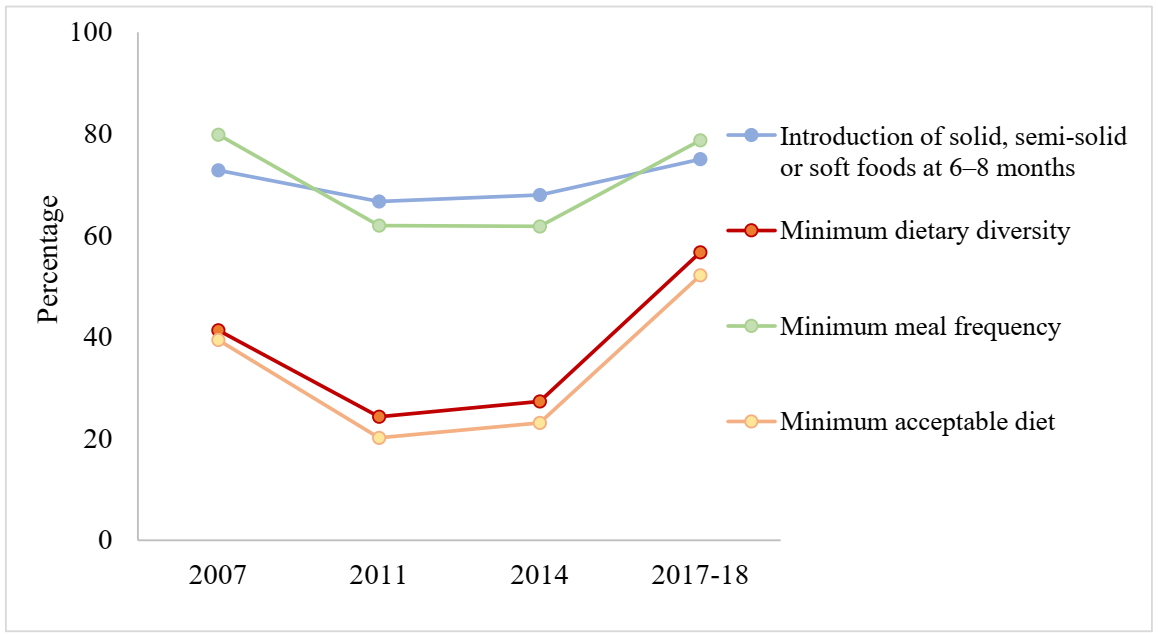
- Timely introduction of solid, semi-solid and soft foods (INTRO): the proportion of children between 6 and 8 months of age who received solid, semi-solid or soft foods.
- Minimum dietary diversity (MDD): the proportion of children who received at least four or more food groups out of six food groups. Instead of seven food groups recommended by the WHO guidelines, the complementary food items provided in the last 24 h were classified into six food groups in the BDHS data as flesh foods, and eggs were combined as one group. These six groups include (1) grains, roots, and tubers; (2) legumes and nuts; (3) dairy products; (4) meat/fish/egg; (5) vitamin-A-rich fruits and vegetables; and (6) other fruits and vegetables. It is notable to mention that egg intake was captured separately from the 2011 BDHS. Therefore, trend analysis for egg intake during 2011 to 2017–2018 are also presented in this study.
- Minimum meal frequency (MMF): the proportion of children aged 6–23 months (breastfed and non-breastfed children) who received solid, semi-solid or soft foods the minimum number of times or more in the previous day of the survey. Minimum meal frequency was defined as having at least 2 meals/day for 6–8 months, 3 or more meals/day for 9–23 months old, breastfed children and 4 or more meals/day for non-breastfed children.
- Minimum acceptable diet (MAD): the proportion of children aged 6–23 months who received and satisfied both the conditions of minimum dietary diversity and minimum meal frequency.
2.3. Explanatory Variables
2.4. Statistical Analysis
3. Results
3.1. Trends in Complementary Feeding Practice
3.2. Trends in Consumption from Different Food Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Children: Improving Survival and Well-Being. Available online: https://www.who.int/news-room/fact-sheets/detail/children-reducing-mortality#:~:text=Malnourished%20children%2C%20particularly%20those%20with,under%2D5%20years%20of%20age (accessed on 3 January 2021).
- Martorell, R. Improved nutrition in the first 1000 days and adult human capital and health. Am. J. Hum. Biol. 2017, 29, e22952. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Infant and Young Child Feeding: Key Facts. Available online: https://www.who.int/news-room/fact-sheets/detail/infant-and-young-child-feeding (accessed on 10 June 2020).
- World Health Organization. World Health Organization Complementary Feeding: Report of the Global Consultation, and Summary of Guiding Principles for Complementary Feeding of the Breastfed Child; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Dagne, A.H.; Anteneh, K.T.; Badi, M.B.; Adhanu, H.H.; Ahunie, M.A.; Aynalem, G.L. Appropriate complementary feeding practice and associated factors among mothers having children aged 6–24 months in Debre Tabor Hospital, North West Ethiopia, 2016. BMC Res. Notes 2019, 12, 215. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Indicators for Assessing Infant and Young Child Feeding Practices: Part 1: Definitions: Conclusions of a Consensus Meeting; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Bhutta, Z.A.; Ahmed, T.; Black, R.E.; Cousens, S.; Dewey, K.G.; Giugliani, E.R.J.; Haider, B.A.; Kirkwood, B.R.; Morris, S.S.; Sachdev, H.P.S.; et al. What works? Interventions for maternal and child undernutrition and survival. Lancet 2008, 371, 417–440. [Google Scholar] [CrossRef]
- Black, R.E.; Allen, L.H.; Bhutta, Z.A.; Caulfield, L.E.; De Onis, M.; Ezzati, M.; Mathers, C.; Rivera, J. Maternal and Child Undernutrition Study Group. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet 2008, 371, 243–260. [Google Scholar] [CrossRef]
- Ogbo, F.A.; Page, A.; Idoko, J.; Claudio, F.; Agho, K.E. Trends in complementary feeding indicators in Nigeria, 2003–2013. BMJ Open 2015, 5, e008467. [Google Scholar] [CrossRef] [Green Version]
- Issaka, A.I.; Agho, K.E.; Burns, P.; Page, A.; Dibley, M.J. Determinants of inadequate complementary feeding practices among children aged 6–23 months in Ghana. Public Health Nutr. 2015, 18, 669–678. [Google Scholar] [CrossRef] [Green Version]
- Walson, J.L.; Berkley, J.A. The impact of malnutrition on childhood infections. Curr. Opin. Infect. Dis. 2018, 31, 231–236. [Google Scholar] [CrossRef]
- Schaible, U.E.; Stefan, H.E. Malnutrition and infection: Complex mechanisms and global impacts. PLoS Med. 2007, 4, e115. [Google Scholar] [CrossRef] [Green Version]
- Black, R.e.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Horton, S.; Steckel, R.H. Malnutrition: Global Economic Losses Attributable to Malnutrition 1900–2000 and Projections to 2050. In How Much Have Global Problems Cost the Earth? A Scorecard from 1900 to 2050; Cambridge University Press: Cambridge, UK, 2014; pp. 247–272. [Google Scholar] [CrossRef] [Green Version]
- National Institute of Population Research and Training (NIPORT); Mitra and Associates. ICF International Bangladesh Demographic and Health Survey 2014; NIPORT, Mitra and Associates, and ICF International: Dhaka, Bangladesh; Rockville, MD, USA, 2016. [Google Scholar]
- Kabir, I.; Khanam, M.; Agho, K.E.; Mihrshahi, S.; Dibley, M.J.; Roy, S.K. Determinants of inappropriate complementary feeding practices in infant and young children in Bangladesh: Secondary data analysis of Demographic Health Survey 2007. Matern. Child Nutr. 2012, 8, 11–27. [Google Scholar] [CrossRef]
- Kabir, A.; Maitrot, M. Factors influencing feeding practices of extreme poor infants and young children in families of working mothers in Dhaka slums: A qualitative study. PLoS ONE 2017, 12, e0172119. [Google Scholar] [CrossRef] [Green Version]
- Senarath, U.; Agho, K.E.; Akram, D.-E.; Godakandage, S.S.; Hazir, T.; Jayawickrama, H.; Joshi, N.; Kabir, I.; Khanam, M.; Patel, A.; et al. Comparisons of complementary feeding indicators and associated factors in children aged 6–23 months across five South Asian countries. Matern. Child Nutr. 2012, 8, 89–106. [Google Scholar] [CrossRef]
- Blackstone, S.; Sanghvi, T. A comparison of minimum dietary diversity in Bangladesh in 2011 and 2014. Matern. Child Nutr. 2018, 14, e12609. [Google Scholar] [CrossRef]
- Ministry of Health and Family Welfare. Ministry of Health and Family Welfare Health Population & Nutrition Sector Development Plan (HPNSDP); Planning Wing, Ministry of Health and Family Welfare; Government of the People’s Republic of Bangladesh: Dhaka, Bangladesh, 2011. [Google Scholar]
- Ministry of Health and Family Welfare. Ministry of Health and Family Welfare Second National Plan of Action for Nutrition (2016–2025); Ministry of Health and Family Welfare, Government of the People’s Republic of Bangladesh: Dhaka, Bangladesh, 2017. [Google Scholar]
- Institute of Public Health Nutrition (IPHN). Institute of Public Health Nutrition (IPHN) National Strategy for Infant and Young Child Feeding in Bangladesh; Institute of Public Health Nutrition (IPHN). Directorate General of Health Services, Ministry of Health and Family Welfare, Government of the People’s Republic of Bangladesh: Dhaka, Bangladesh, 2007. [Google Scholar]
- Ministry of Labour and Employment. Ministry of Labour and Employment National Labour Policy 2012; Ministry of Labour and Employment, Goverment of the Peoples’ Republic of Bangladesh: Dhaka, Bangladesh, 2012. [Google Scholar]
- Ministry of Law. Ministry of Law, J. a. P. A. The Breast-milk Substitutes, Infant Foods, Commercially Manufactured Complementary Foods and the Accessories Thereof (Regulation of Marketing) Act; Ministry of Law, Justice and Parliamentary Affairs, Government of the Peoples’ Republic of Bangladesh: Dhaka, Bangladesh, 2013. [Google Scholar]
- Na, M.; Aguayo, V.M.; Arimond, M.; Narayan, A.; Stewart, C.P. Stagnating trends in complementary feeding practices in Bangladesh: An analysis of national surveys from 2004–2014. Matern. Child Nutr. 2018, 14, e12624. [Google Scholar] [CrossRef]
- National Institute of Population Research and Training (NIPORT); Mitra and Associates; ICF International. Bangladesh Demographic and Health Survey 2011; NIPORT, Mitra and Associates, and ICF International: Dhaka, Bangladesh; Calverton, MD, USA, 2013. [Google Scholar]
- National Institute of Population Research and Training (NIPORT); Mitra and Associates; Macro International. Bangladesh Demographic and Health Survey 2007; National Institute of Population Research and Training, Mitra and Associates, and Macro International: Dhaka, Bangladesh; Calverton, MD, USA, 2009. [Google Scholar]
- World Health Organization. Global Strategy for Infant and Young Child Feeding; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157. [Google Scholar] [CrossRef]
- Corcoran, C. Trend Tests for Binary Data; Wiley: Hoboken, NJ, USA, 2014. [Google Scholar]
- STATA. A Comparison of Different Tests for Trend. Available online: https://www.stata.com/support/faqs/statistics/test-for-trend/ (accessed on 10 June 2020).
- Na, M.; Aguayo, V.M.; Arimond, M.; Dahal, P.; Lamichhane, B.; Pokharel, R.; Chitekwe, S.; Stewart, C.P. Trends and predictors of appropriate complementary feeding practices in Nepal: An analysis of national household survey data collected between 2001 and 2014. Matern. Child Nutr. 2017, 14, e12564. [Google Scholar] [CrossRef] [Green Version]
- Stewart, C.P.; Iannotti, L.; Dewey, K.G.; Michaelsen, K.F.; Onyango, A.W. Contextualising complementary feeding in a broader framework for stunting prevention. Matern. Child Nutr. 2013, 9, 27–45. [Google Scholar] [CrossRef]
- Aemro, M.; Mesele, M.; Birhanu, Z.; Atenafu, A. Dietary Diversity and Meal Frequency Practices among Infant and Young Children Aged 6–23 Months in Ethiopia: A Secondary Analysis of Ethiopian Demographic and Health Survey 2011. J. Nutr. Metab. 2013, 2013, 782931. [Google Scholar] [CrossRef] [Green Version]
- Dhami, M.V.; Ogbo, F.A.; Osuagwu, U.L.; Agho, K.E. Prevalence and factors associated with complementary feeding practices among children aged 6–23 months in India: A regional analysis. BMC Public Health 2019, 19, 1034. [Google Scholar] [CrossRef] [Green Version]
- Senarath, U.; Godakandage, S.S.P.; Jayawickrama, H.; Siriwardena, I.; Dibley, M.J. Determinants of inappropriate complementary feeding practices in young children in Sri Lanka: Secondary data analysis of Demographic and Health Survey 2006–2007. Matern. Child Nutr. 2011, 8, 60–77. [Google Scholar] [CrossRef]
- Patel, A.; Pusdekar, Y.; Badhoniya, N.; Borkar, J.; Agho, K.E.; Dibley, M.J. Determinants of inappropriate complementary feeding practices in young children in India: Secondary analysis of National Family Health Survey 2005–2006. Matern. Child Nutr. 2012, 8, 28–44. [Google Scholar] [CrossRef]
- Ogbo, F.A.; Ogeleka, P.; Awosemo, A.O. Trends and determinants of complementary feeding practices in Tanzania, 2004–2016. Trop. Med. Health 2018, 46, 40. [Google Scholar] [CrossRef] [Green Version]
- Fein, S.B.; Labiner-Wolfe, J.; Scanlon, K.S.; Grummer-Strawn, L.M. Selected complementary feeding practices and their association with maternal education. Pediatrics 2008, 122 (Suppl. S2), S91–S97. [Google Scholar] [CrossRef] [Green Version]
- Alderman, H.; Headey, D.D. How important is parental education for child nutrition? World Dev. 2017, 94, 448–464. [Google Scholar] [CrossRef]
- Oddo, V.M.; Surkan, P.J.; Hurley, K.M.; Lowery, C.; De Ponce, S.; Jones-Smith, J. Pathways of the association between maternal employment and weight status among women and children: Qualitative findings from Guatemala. Matern. Child Nutr. 2018, 14, e12455. [Google Scholar] [CrossRef]
- Komatsu, H.; Malapit, H.J.L.; Theis, S. Does women’s time in domestic work and agriculture affect women’s and children’s dietary diversity? Evidence from Bangladesh, Nepal, Cambodia, Ghana, and Mozambique. Food Policy 2018, 79, 256–270. [Google Scholar] [CrossRef]
- Khanal, V.; Sauer, K.; Zhao, Y. Determinants of complementary feeding practices among Nepalese children aged 6–23 months: Findings from demographic and health survey 2011. BMC Pediatr. 2013, 13, 131. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | Introduction of Solid, Semi-Solid or Soft Foods (%) | Minimum Dietary Diversity (%) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2007 | 2011 | 2014 | 2017–2018 | % Change 3 | p 4 | 2007 | 2011 | 2014 | 2017–2018 | % Change 3 | p 4 | |
| Overall | 72.8 | 66.7 | 68.0 | 75.0 | 3.0 | 0.505 | 41.4 | 24.3 | 27.3 | 56.7 | 37.1 | <0.001 |
| Household characteristics | ||||||||||||
| Administrative division | ||||||||||||
| Barisal | 69.9 | 60.5 | 77.8 | 66.0 | −5.6 | 0.868 | 35.9 | 23.1 | 29.6 | 54.7 | 52.6 | 0.002 |
| Chittagong | 52.1 | 55.4 | 56.6 | 69.8 | 33.9 | 0.056 | 35.4 | 20.8 | 22.4 | 57.2 | 61.7 | <0.001 |
| Dhaka | 79.8 | 68.4 | 76.3 | 87.2 | 9.4 | 0.156 | 42.3 | 25.4 | 28.4 | 54.3 | 28.4 | <0.001 |
| Khulna | 79.1 | 90.1 | 76.6 | 80.1 | 1.3 | 0.673 | 45.7 | 31.1 | 36.2 | 59.1 | 29.3 | 0.003 |
| Rajshahi | 81.9 | 77.7 | 81.6 | 69.0 | −15.8 | 0.180 | 51.9 | 30.9 | 27.3 | 57.0 | 9.8 | 0.834 |
| Rangpur 1 | - | 74.8 | 59.7 | 69.3 | −7.3 | 0.493 | - | 23.4 | 28.7 | 66.2 | 183.3 | <0.001 |
| Sylhet | 66.4 | 50.6 | 47.3 | 59.4 | −10.5 | 0.467 | 24.7 | 14.2 | 24.2 | 52.8 | 114.2 | <0.001 |
| Mymensingh 2 | - | - | - | 77.2 | - | - | - | - | - | 52.5 | - | - |
| Place of residence | ||||||||||||
| Urban | 81.8 | 76.0 | 68.6 | 80.5 | −1.6 | 0.809 | 45.4 | 34.9 | 32.6 | 60.1 | 32.4 | <0.001 |
| Rural | 70.6 | 64.6 | 67.7 | 72.8 | 3.0 | 0.544 | 40.2 | 21.1 | 25.5 | 55.4 | 38.1 | <0.001 |
| Household wealth status | ||||||||||||
| Poorest | 71.0 | 52.8 | 60.1 | 63.6 | −10.5 | 0.581 | 32.2 | 12.4 | 18.0 | 48.4 | 50.4 | <0.001 |
| Poorer | 60.9 | 64.3 | 75.3 | 69.4 | 13.9 | 0.129 | 32.0 | 16.8 | 22.3 | 54.8 | 71.6 | <0.001 |
| Middle | 77.1 | 71.5 | 63.0 | 80.8 | 4.7 | 0.988 | 45.2 | 25.5 | 28.4 | 56.4 | 24.7 | 0.001 |
| Richer | 80.5 | 70.1 | 77.4 | 70.8 | −12.1 | 0.408 | 45.4 | 33.2 | 31.8 | 54.6 | 20.4 | 0.006 |
| Richest | 83.6 | 81.9 | 65.6 | 91.2 | 9.1 | 0.783 | 54.2 | 37.0 | 37.3 | 70.1 | 29.5 | <0.001 |
| Child characteristics | ||||||||||||
| Age (month) | ||||||||||||
| 6–8 | 72.8 | 66.7 | 68.0 | 75.0 | 3.0 | 0.505 | 9.0 | 6.4 | 5.8 | 19.8 | 118.7 | <0.001 |
| 9–11 | - | - | - | - | - | - | 31.8 | 19.6 | 19.6 | 43.8 | 37.9 | 0.015 |
| 12–17 | - | - | - | - | - | - | 49.1 | 27.8 | 27.9 | 66.5 | 35.4 | <0.001 |
| 18–23 | - | - | - | - | - | - | 56.1 | 33.7 | 42.1 | 70.2 | 25.0 | <0.001 |
| Gender | ||||||||||||
| Male | 76.7 | 66.2 | 69.5 | 76.7 | 0.0 | 0.774 | 42.4 | 24.6 | 26.0 | 57.5 | 35.7 | <0.001 |
| Female | 69.5 | 67.3 | 66.3 | 72.8 | 4.8 | 0.658 | 40.4 | 24.1 | 28.8 | 55.8 | 38.2 | <0.001 |
| Birth order | ||||||||||||
| 1 | 82.3 | 74.4 | 66.9 | 76.4 | −7.2 | 0.205 | 48.3 | 30.1 | 33.1 | 62.2 | 28.6 | <0.001 |
| 2 | 73.5 | 67.1 | 71.3 | 78.1 | 6.2 | 0.290 | 41.6 | 25.1 | 24.8 | 54.0 | 29.7 | <0.001 |
| ≥3 | 65.1 | 60.8 | 65.8 | 68.9 | 5.9 | 0.467 | 35.1 | 18.7 | 22.8 | 53.5 | 52.4 | <0.001 |
| Maternal characteristics | ||||||||||||
| Age at child’s birth (years) | ||||||||||||
| <20 | 73.6 | 63.6 | 62.7 | 71.5 | −2.9 | 0.659 | 40.4 | 27.5 | 28.0 | 55.2 | 36.8 | <0.001 |
| 20–29 | 74.0 | 69.1 | 69.6 | 73.1 | −1.2 | 0.909 | 43.0 | 23.4 | 27.2 | 57.5 | 33.7 | <0.001 |
| ≥30 | 68.5 | 61.7 | 69.7 | 86.1 | 25.7 | 0.027 | 37.3 | 24.0 | 26.9 | 55.8 | 49.8 | <0.001 |
| Level of education | ||||||||||||
| 0–4 | 63.0 | 54.9 | 62.5 | 63.1 | 0.2 | 0.822 | 31.5 | 15.7 | 15.8 | 47.1 | 49.7 | <0.001 |
| 5–9 | 77.6 | 72.1 | 71.6 | 75.8 | −2.4 | 0.760 | 47.5 | 25.5 | 28.1 | 56.7 | 19.5 | <0.001 |
| 10+ | 95.2 | 83.0 | 71.1 | 85.3 | −10.4 | 0.303 | 55.9 | 43.9 | 45.1 | 67.4 | 20.6 | <0.001 |
| Occupation | ||||||||||||
| Housewife | 70.2 | 65.5 | 68.8 | 76.0 | 8.2 | 0.163 | 40.8 | 23.8 | 27.4 | 55.6 | 36.5 | <0.001 |
| Working outside | 81.2 | 87.3 | 64.7 | 73.4 | −9.5 | 0.127 | 43.4 | 31.7 | 27.2 | 58.3 | 34.5 | <0.001 |
| Body mass index (kg/m2) | ||||||||||||
| <18.5 | 78.9 | 56.8 | 63.2 | 73.5 | −6.8 | 0.207 | 37.6 | 20.0 | 22.0 | 57.5 | 53.1 | <0.001 |
| 18.5–22.9 | 70.2 | 71.2 | 67.0 | 69.9 | −0.4 | 0.688 | 40.2 | 24.6 | 27.1 | 54.4 | 35.3 | <0.001 |
| 23.0–24.0 | 66.5 | 58.4 | 71.5 | 81.9 | 23.2 | 0.047 | 48.2 | 28.9 | 32.5 | 60.6 | 25.9 | <0.001 |
| ≥25.0 | 69.8 | 80.7 | 77.3 | 82.0 | 17.4 | 0.483 | 63.8 | 34.0 | 34.5 | 58.4 | −8.5 | 0.053 |
| Paternal characteristics | ||||||||||||
| Level of education | ||||||||||||
| 0–4 | 69.2 | 61.0 | 62.2 | 69.0 | −0.2 | 0.798 | 34.1 | 17.7 | 20.0 | 50.5 | 47.9 | <0.001 |
| 5–9 | 78.4 | 67.1 | 69.8 | 75.2 | −4.0 | 0.715 | 43.4 | 25.5 | 28.4 | 55.2 | 27.2 | <0.001 |
| 10+ | 72.3 | 85.2 | 77.5 | 83.1 | 14.9 | 0.410 | 60.3 | 38.9 | 40.1 | 69.1 | 14.6 | <0.001 |
| Occupation | ||||||||||||
| Service holder/businessman | 73.8 | 77.9 | 70.5 | 72.2 | −2.2 | 0.513 | 47.8 | 29.3 | 33.5 | 60.6 | 26.6 | <0.001 |
| Agriculture-based worker | 78.6 | 62.7 | 73.6 | 68.5 | −12.8 | 0.327 | 40.1 | 20.6 | 22.2 | 52.4 | 30.7 | <0.001 |
| Non-agriculture-based worker | 73.6 | 63.3 | 70.1 | 80.8 | 9.8 | 0.037 | 46.2 | 26.1 | 28.8 | 56.0 | 21.4 | 0.009 |
| Others 5 | 63.5 | 59.4 | 48.2 | 68.4 | 7.8 | 0.709 | 29.5 | 15.1 | 20.1 | 56.1 | 90.0 | <0.001 |
| Characteristics | Minimum Meal Frequency (%) | Minimum Acceptable Diet (%) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2007 | 2011 | 2014 | 2017–2018 | % Change 3 | p 4 | 2007 | 2011 | 2014 | 2017–2018 | % Change 3 | p 5 | |
| Overall | 79.9 | 62.0 | 61.8 | 78.7 | 1.4 | 0.935 | 39.4 | 20.2 | 23.1 | 52.1 | 32.2 | <0.001 |
| Household characteristics | ||||||||||||
| Administrative division | ||||||||||||
| Barisal | 72.3 | 61.2 | 60.0 | 74.7 | −3.3 | 0.688 | 32.7 | 17.3 | 24.4 | 49.2 | 50.2 | 0.004 |
| Chittagong | 65.7 | 52.2 | 54.6 | 75.4 | −14.8 | 0.005 | 32.5 | 16.2 | 17.3 | 49.9 | 53.8 | <0.001 |
| Dhaka | 83.0 | 62.9 | 60.3 | 79.1 | 4.7 | 0.025 | 39.7 | 22.2 | 25.0 | 51.3 | 29.2 | <0.001 |
| Khulna | 88.4 | 80.2 | 79.2 | 82.6 | 6.6 | 0.211 | 44.7 | 28.0 | 31.6 | 54.5 | 21.9 | 0.022 |
| Rajshahi | 91.3 | 62.5 | 70.8 | 73.4 | 19.6 | <0.001 | 51.6 | 24.8 | 25.8 | 52.0 | 0.7 | 0.235 |
| Rangpur 1 | - | 70.6 | 65.4 | 85.6 | −21.3 | <0.001 | - | 19.2 | 23.5 | 63.6 | 230.7 | <0.001 |
| Sylhet | 72.3 | 55.8 | 57.4 | 76.2 | −5.4 | 0.407 | 23.8 | 11.3 | 17.9 | 47.1 | 98.1 | <0.001 |
| Mymensingh 2 | - | - | - | 84.7 | - | - | - | - | - | 49.1 | - | - |
| Place of residence | ||||||||||||
| Urban | 83.2 | 65.4 | 65.9 | 80.7 | 3.0 | 0.931 | 43.5 | 28.4 | 27.4 | 55.4 | 27.3 | <0.001 |
| Rural | 78.9 | 60.9 | 60.3 | 78.0 | 1.1 | 0.840 | 38.2 | 17.7 | 21.6 | 51.0 | 33.3 | <0.001 |
| Household wealth status | ||||||||||||
| Poorest | 83.6 | 52.9 | 53.7 | 75.6 | 9.6 | 0.098 | 31.8 | 10.2 | 14.7 | 44.6 | 40.3 | <0.001 |
| Poorer | 76.2 | 61.8 | 61.1 | 79.4 | −4.3 | 0.293 | 31.7 | 13.8 | 17.5 | 50.5 | 59.3 | <0.001 |
| Middle | 78.8 | 66.8 | 63.0 | 77.1 | 2.2 | 0.518 | 43.2 | 22.4 | 23.2 | 50.0 | 15.7 | 0.030 |
| Richer | 82.0 | 61.5 | 65.9 | 78.6 | 4.2 | 0.935 | 42.9 | 27.3 | 28.1 | 50.9 | 18.4 | 0.006 |
| Richest | 78.9 | 69.4 | 66.4 | 83.1 | −5.3 | 0.305 | 49.3 | 30.1 | 33.1 | 65.5 | 32.9 | <0.001 |
| Child characteristics | ||||||||||||
| Age (month) | ||||||||||||
| 6–8 | 59.9 | 51.3 | 48.8 | 62.2 | −3.8 | 0.804 | 9.0 | 6.3 | 5.8 | 19.3 | 115.0 | <0.001 |
| 9–11 | 73.8 | 57.2 | 52.3 | 70.3 | 4.7 | 0.286 | 28.7 | 14.9 | 16.1 | 38.9 | 35.8 | 0.002 |
| 12–17 | 83.8 | 62.7 | 67.2 | 84.1 | −0.4 | 0.063 | 46.8 | 23.3 | 24.4 | 62.0 | 32.5 | <0.001 |
| 18–23 | 89.7 | 70.2 | 68.0 | 85.0 | 5.2 | 0.036 | 54.1 | 27.9 | 34.6 | 63.8 | 17.9 | <0.001 |
| Gender | ||||||||||||
| Male | 80.6 | 62.9 | 62.9 | 78.1 | 3.1 | 0.634 | 39.9 | 20.4 | 22.7 | 51.8 | 29.9 | <0.001 |
| Female | 79.1 | 61.0 | 60.6 | 79.4 | −0.4 | 0.722 | 39.0 | 20.0 | 23.6 | 52.5 | 34.6 | <0.001 |
| Birth order | ||||||||||||
| 1 | 82.5 | 64.6 | 64.2 | 82.6 | 0.0 | 0.764 | 45.4 | 26.0 | 27.8 | 57.7 | 27.2 | <0.001 |
| 2 | 80.0 | 62.8 | 61.7 | 75.9 | 5.1 | 0.621 | 40.0 | 19.0 | 20.6 | 49.1 | 22.7 | <0.001 |
| ≥3 | 77.5 | 59.0 | 58.9 | 77.5 | −0.1 | 0.839 | 33.9 | 16.0 | 19.9 | 49.1 | 45.1 | <0.001 |
| Maternal characteristics | ||||||||||||
| Age at child’s birth (years) | ||||||||||||
| <20 | 82.4 | 62.7 | 61.5 | 77.9 | 5.4 | 0.072 | 39.3 | 23.4 | 22.9 | 50.8 | 29.3 | 0.008 |
| 20–29 | 79.4 | 62.2 | 62.5 | 78.3 | 1.3 | 0.917 | 40.6 | 19.5 | 23.1 | 52.5 | 29.3 | <0.001 |
| ≥30 | 78.0 | 60.5 | 60.0 | 80.4 | −3.1 | 0.116 | 35.8 | 18.9 | 23.5 | 52.3 | 46.2 | <0.001 |
| Level of education | ||||||||||||
| 0–4 | 77.5 | 54.6 | 55.2 | 75.1 | 3.1 | 0.010 | 30.6 | 13.3 | 12.7 | 42.5 | 38.9 | <0.001 |
| 5–9 | 82.0 | 63.7 | 63.1 | 77.6 | 5.4 | 0.574 | 44.6 | 20.8 | 23.7 | 52.0 | 16.5 | 0.015 |
| 10+ | 81.0 | 75.5 | 69.4 | 85.6 | −5.6 | 0.107 | 53.0 | 37.2 | 39.7 | 63.3 | 19.3 | <0.001 |
| Occupation | ||||||||||||
| Housewife | 78.9 | 61.4 | 60.8 | 76.3 | 3.3 | 0.076 | 38.7 | 19.7 | 22.6 | 49.7 | 28.5 | <0.001 |
| Working outside | 83.2 | 68.8 | 65.1 | 82.5 | 0.8 | 0.754 | 42.1 | 26.7 | 24.8 | 55.9 | 33.0 | <0.001 |
| Body mass index (kg/m2) | ||||||||||||
| <18.5 | 83.8 | 61.2 | 61.6 | 78.8 | 6.0 | 0.001 | 36.6 | 17.0 | 18.1 | 51.5 | 40.8 | <0.001 |
| 18.5–22.9 | 78.1 | 62.3 | 59.6 | 76.9 | 1.6 | 0.356 | 38.3 | 20.2 | 22.8 | 49.9 | 30.0 | 0.008 |
| 23.0–24.0 | 73.4 | 60.1 | 65.0 | 82.5 | −12.4 | <0.001 | 44.8 | 22.8 | 27.1 | 58.2 | 30.1 | <0.001 |
| ≥25.0 | 79.1 | 65.1 | 67.3 | 80.2 | −1.3 | 0.048 | 58.0 | 28.7 | 30.7 | 53.3 | −8.0 | 0.036 |
| Paternal characteristics | ||||||||||||
| Level of education | ||||||||||||
| 0–4 | 79.8 | 56.7 | 55.3 | 78.5 | 1.6 | 0.074 | 33.6 | 15.1 | 16.1 | 47.1 | 40.1 | <0.001 |
| 5–9 | 80.1 | 64.8 | 64.2 | 75.9 | 5.2 | 0.453 | 41.4 | 21.5 | 24.3 | 49.2 | 18.9 | <0.001 |
| 10+ | 79.7 | 69.7 | 70.0 | 84.1 | −5.5 | 0.035 | 54.1 | 30.7 | 35.0 | 65.2 | 20.7 | <0.001 |
| Occupation | ||||||||||||
| Service holder/businessman | 78.9 | 66.4 | 63.1 | 79.3 | −0.6 | 0.848 | 44.4 | 24.5 | 27.9 | 56.2 | 26.6 | <0.001 |
| Agriculture-based worker | 83.1 | 62.3 | 57.2 | 78.3 | 5.8 | 0.005 | 39.9 | 17.9 | 18.8 | 47.7 | 19.5 | 0.200 |
| Non-agriculture-based worker | 78.2 | 60.8 | 66.9 | 79.5 | −1.7 | 0.002 | 43.0 | 21.1 | 25.5 | 51.9 | 20.6 | <0.001 |
| Others 5 | 79.2 | 54.3 | 54.6 | 75.0 | 5.4 | 0.007 | 28.8 | 11.9 | 15.3 | 50.3 | 74.3 | <0.001 |
| Characteristics | Grains, Roots or Tubers (%) | Legumes or Nuts (%) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2007 | 2011 | 2014 | 2017–2018 | % Change 3 | p 4 | 2007 | 2011 | 2014 | 2017–2018 | % Change 3 | p 5 | |
| Overall | 84.6 | 78.8 | 78.2 | 87.4 | 3.2 | 0.027 | 29.7 | 5.8 | 7.0 | 21.5 | 27.5 | <0.001 |
| Household characteristics | ||||||||||||
| Administrative division | ||||||||||||
| Barisal | 82.1 | 77.8 | 79.9 | 84.2 | 2.6 | 0.524 | 34.9 | 9.3 | 9.9 | 22.9 | 34.3 | 0.045 |
| Chittagong | 76.0 | 73.4 | 75.4 | 88.6 | 16.7 | <0.001 | 26.7 | 3.6 | 6.3 | 24.6 | 7.9 | 0.568 |
| Dhaka | 86.1 | 76.4 | 75.0 | 84.7 | −1.6 | 0.289 | 33.7 | 5.9 | 9.5 | 21.5 | 36.1 | <0.001 |
| Khulna | 90.7 | 89.4 | 86.0 | 89.6 | −1.3 | 0.613 | 23.8 | 10.2 | 6.6 | 17.1 | 28.2 | 0.116 |
| Rajshahi | 92.5 | 83.8 | 85.4 | 86.1 | −7.0 | 0.012 | 30.5 | 5.7 | 3.2 | 15.2 | 50.2 | <0.001 |
| Rangpur 1 | - | 87.5 | 85.4 | 90.2 | 3.0 | 0.384 | - | 6.1 | 2.6 | 17.3 | −181.4 | <0.001 |
| Sylhet | 77.0 | 72.7 | 74.7 | 88.8 | 15.3 | 0.010 | 22.1 | 4.8 | 5.8 | 30.8 | −39.7 | 0.031 |
| Mymensingh 2 | - | - | - | 89.5 | - | - | - | - | - | 24.4 | - | - |
| Place of residence | ||||||||||||
| Urban | 85.6 | 80.8 | 80.3 | 90.4 | 5.6 | 0.032 | 39.1 | 7.6 | 10.0 | 24.6 | 37.1 | <0.001 |
| Rural | 84.4 | 78.2 | 77.5 | 86.2 | 2.2 | 0.212 | 26.9 | 5.3 | 6.0 | 20.4 | 24.1 | <0.001 |
| Household wealth status | ||||||||||||
| Poorest | 86.3 | 76.0 | 79.6 | 88.1 | 2.1 | 0.188 | 24.6 | 3.5 | 4.3 | 19.6 | 20.6 | 0.144 |
| Poorer | 80.2 | 78.9 | 75.5 | 88.5 | 10.3 | 0.011 | 25.2 | 6.1 | 5.4 | 18.5 | 26.7 | 0.014 |
| Middle | 86.2 | 80.0 | 76.5 | 83.9 | −2.6 | 0.325 | 28.4 | 5.5 | 5.5 | 18.5 | 34.7 | 0.001 |
| Richer | 85.2 | 78.7 | 80.1 | 84.3 | −1.1 | 0.986 | 29.3 | 6.8 | 9.3 | 21.5 | 26.8 | 0.094 |
| Richest | 85.8 | 81.1 | 79.0 | 92.0 | 7.3 | 0.045 | 41.9 | 7.6 | 10.8 | 30.1 | 28.1 | 0.003 |
| Child characteristics | ||||||||||||
| Age (month) | ||||||||||||
| 6–8 | 56.0 | 47.9 | 39.7 | 56.0 | 0.0 | 0.465 | 9.1 | 4.2 | 2.6 | 8.3 | 9.4 | 0.475 |
| 9–11 | 86.6 | 79.4 | 76.7 | 89.8 | 3.7 | 0.397 | 24.2 | 4.4 | 7.1 | 19.9 | 17.8 | 0.434 |
| 12–17 | 91.4 | 84.2 | 87.2 | 93.3 | 2.0 | 0.035 | 32.8 | 6.7 | 5.7 | 23.6 | 27.9 | 0.006 |
| 18–23 | 93.0 | 90.5 | 88.8 | 94.7 | 1.8 | 0.458 | 40.3 | 6.6 | 10.7 | 26.4 | 34.6 | <0.001 |
| Gender | ||||||||||||
| Male | 85.2 | 78.5 | 78.5 | 87.4 | 2.5 | 0.129 | 28.5 | 5.4 | 6.8 | 21.0 | 26.1 | 0.002 |
| Female | 84.0 | 79.1 | 77.9 | 87.3 | 3.9 | 0.112 | 30.9 | 6.3 | 7.3 | 22.1 | 28.5 | <0.001 |
| Birth order | ||||||||||||
| 1 | 85.1 | 79.6 | 81.0 | 87.2 | 2.4 | 0.228 | 34.0 | 6.7 | 7.4 | 23.3 | 31.3 | <0.001 |
| 2 | 85.2 | 81.0 | 77.8 | 88.0 | 3.3 | 0.318 | 30.7 | 6.4 | 6.8 | 20.4 | 33.6 | 0.003 |
| ≥3 | 83.8 | 76.3 | 75.0 | 86.9 | 3.7 | 0.764 | 25.3 | 4.5 | 6.8 | 20.7 | 18.1 | 0.031 |
| Maternal characteristics | ||||||||||||
| Age at child’s birth (years) | ||||||||||||
| <20 | 84.0 | 77.7 | 79.9 | 84.6 | 0.7 | 0.764 | 29.3 | 4.9 | 7.7 | 19.7 | 32.9 | <0.001 |
| 20–29 | 84.5 | 79.1 | 78.5 | 87.4 | 3.5 | 0.063 | 29.9 | 6.3 | 6.7 | 23.1 | 22.7 | 0.001 |
| ≥30 | 86.0 | 79.0 | 75.3 | 89.4 | 3.9 | 0.174 | 29.4 | 5.1 | 7.4 | 18.8 | 36.1 | 0.015 |
| Level of education | ||||||||||||
| 0–4 | 82.7 | 74.4 | 71.6 | 85.1 | 2.9 | 0.670 | 27.1 | 3.7 | 5.8 | 18.5 | 31.6 | <0.001 |
| 5–9 | 86.5 | 80.0 | 80.4 | 87.6 | 1.3 | 0.171 | 29.6 | 6.8 | 7.6 | 21.8 | 26.5 | 0.037 |
| 10+ | 85.4 | 86.1 | 82.7 | 89.3 | 4.5 | 0.213 | 38.4 | 7.9 | 7.4 | 24.2 | 36.9 | 0.009 |
| Occupation | ||||||||||||
| Housewife | 83.2 | 78.5 | 77.5 | 86.2 | 3.5 | 0.190 | 31.1 | 5.6 | 7.4 | 23.1 | 25.8 | <0.001 |
| Working outside | 89.4 | 82.2 | 80.4 | 89.2 | −0.2 | 0.796 | 25.0 | 7.9 | 5.9 | 19.1 | 23.4 | 0.070 |
| Body mass index (kg/m2) | ||||||||||||
| <18.5 | 87.1 | 78.4 | 76.4 | 86.9 | −0.2 | 0.175 | 28.7 | 5.9 | 7.0 | 23.7 | 17.4 | <0.001 |
| 18.5–22.9 | 83.7 | 79.3 | 78.2 | 86.5 | 3.4 | 0.188 | 28.9 | 5.4 | 6.2 | 20.4 | 29.6 | <0.001 |
| 23.0–24.0 | 76.8 | 76.5 | 78.9 | 88.1 | 14.7 | 0.001 | 31.9 | 6.9 | 7.8 | 20.5 | 35.9 | 0.622 |
| ≥25.0 | 87.5 | 79.9 | 81.0 | 89.2 | 1.9 | 0.071 | 38.7 | 6.6 | 9.3 | 23.1 | 40.3 | 0.608 |
| Paternal characteristics | ||||||||||||
| Level of education | ||||||||||||
| 0–4 | 85.1 | 77.3 | 76.2 | 86.3 | 1.4 | 0.944 | 26.7 | 5.4 | 6.7 | 18.3 | 31.6 | <0.001 |
| 5–9 | 83.9 | 78.1 | 78.2 | 87.1 | 3.8 | 0.047 | 30.7 | 4.9 | 6.9 | 22.3 | 27.4 | 0.057 |
| 10+ | 84.6 | 83.8 | 82.3 | 89.5 | 5.9 | 0.051 | 37.0 | 8.5 | 8.0 | 25.2 | 32.0 | 0.029 |
| Occupation | ||||||||||||
| Service holder/businessman | 84.2 | 81.3 | 77.8 | 85.6 | 1.7 | 0.808 | 29.6 | 6.2 | 7.4 | 21.9 | 26.2 | 0.023 |
| Agriculture-based worker | 85.1 | 79.8 | 79.5 | 86.5 | 1.7 | 0.907 | 28.2 | 5.1 | 3.7 | 20.9 | 25.9 | <0.001 |
| Non-agriculture-based worker | 86.9 | 77.4 | 79.9 | 88.8 | 2.2 | 0.009 | 36.3 | 6.8 | 8.9 | 22.5 | 38.1 | 0.005 |
| Others 5 | 81.8 | 74.9 | 72.9 | 87.1 | 6.5 | 0.652 | 23.2 | 3.1 | 7.4 | 18.2 | 21.4 | 0.005 |
| Characteristics | Dairy Products (%) | Meat/Fish/EGG (%) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2007 | 2011 | 2014 | 2017–2018 | % Change 3 | p 4 | 2007 | 2011 | 2014 | 2017–2018 | % Change 3 | p 4 | |
| Overall | 39.7 | 32.7 | 37.6 | 32.2 | 18.7 | 0.001 | 46.9 | 53.0 | 55.0 | 67.2 | 43.2 | <0.001 |
| Household characteristics | ||||||||||||
| Administrative division | ||||||||||||
| Barisal | 40.4 | 25.5 | 35.7 | 25.1 | 38.0 | 0.090 | 43.0 | 51.4 | 57.6 | 65.9 | 53.3 | 0.001 |
| Chittagong | 34.3 | 32.3 | 28.2 | 24.9 | 27.4 | 0.002 | 42.9 | 49.5 | 52.9 | 67.6 | 57.7 | <0.001 |
| Dhaka | 45.4 | 35.2 | 46.1 | 44.9 | 1.1 | 0.270 | 45.3 | 49.9 | 53.1 | 63.6 | 40.3 | <0.001 |
| Khulna | 43.8 | 32.2 | 35.1 | 25.5 | 41.8 | 0.002 | 59.0 | 67.7 | 62.9 | 72.9 | 23.4 | 0.036 |
| Rajshahi | 39.6 | 39.4 | 42.8 | 35.3 | 10.9 | 0.506 | 53.7 | 60.6 | 54.5 | 68.6 | 27.8 | 0.002 |
| Rangpur 1 | - | 31.8 | 35.5 | 27.7 | 13.1 | 0.317 | - | 59.4 | 65.8 | 77.3 | 30.1 | <0.001 |
| Sylhet | 27.2 | 19.5 | 25.0 | 19.8 | 27.2 | 0.300 | 36.5 | 38.7 | 49.1 | 62.3 | 71.0 | <0.001 |
| Mymensingh 2 | - | - | - | 33.9 | - | - | - | - | - | 61.2 | - | - |
| Place of residence | ||||||||||||
| Urban | 47.3 | 44.9 | 44.3 | 35.1 | 25.9 | <0.001 | 51.8 | 60.0 | 59.9 | 70.6 | 36.3 | <0.001 |
| Rural | 37.4 | 29.0 | 35.3 | 31.2 | 16.6 | 0.041 | 45.5 | 50.9 | 53.3 | 65.9 | 45.0 | <0.001 |
| Household wealth status | ||||||||||||
| Poorest | 23.1 | 14.7 | 20.9 | 19.7 | 14.8 | 0.842 | 43.4 | 40.3 | 46.8 | 63.2 | 45.9 | <0.001 |
| Poorer | 29.8 | 22.3 | 30.0 | 28.5 | 4.4 | 0.702 | 36.0 | 50.5 | 49.2 | 65.1 | 81.1 | <0.001 |
| Middle | 38.2 | 37.6 | 42.5 | 32.6 | 14.7 | 0.275 | 45.9 | 55.7 | 57.4 | 68.4 | 49.0 | <0.001 |
| Richer | 47.4 | 43.6 | 47.2 | 35.3 | 25.6 | 0.005 | 54.1 | 61.0 | 60.0 | 67.2 | 24.2 | 0.001 |
| Richest | 62.7 | 50.5 | 49.8 | 46.3 | 26.2 | <0.001 | 57.2 | 60.4 | 62.5 | 72.3 | 26.3 | <0.001 |
| Child characteristics | ||||||||||||
| Age (month) | ||||||||||||
| 6–8 | 39.8 | 29.8 | 36.4 | 31.9 | 19.9 | 0.163 | 12.9 | 20.0 | 19.3 | 30.6 | 136.8 | <0.001 |
| 9–11 | 43.7 | 32.7 | 34.6 | 32.2 | 26.2 | 0.012 | 31.2 | 48.4 | 43.0 | 55.7 | 78.5 | <0.001 |
| 12–17 | 41.7 | 32.5 | 38.0 | 33.2 | 20.6 | 0.040 | 54.3 | 58.7 | 61.5 | 75.2 | 38.5 | <0.001 |
| 18–23 | 36.0 | 34.7 | 39.6 | 31.5 | 12.7 | 0.291 | 65.6 | 68.6 | 72.9 | 81.6 | 24.3 | <0.001 |
| Gender | ||||||||||||
| Male | 42.3 | 34.6 | 39.4 | 34.4 | 18.6 | 0.010 | 48.9 | 54.1 | 53.6 | 66.9 | 36.9 | <0.001 |
| Female | 37.1 | 30.8 | 35.7 | 29.8 | 19.6 | 0.019 | 45.0 | 51.9 | 56.6 | 67.5 | 50.0 | <0.001 |
| Birth order | ||||||||||||
| 1 | 43.4 | 37.9 | 43.7 | 35.6 | 18.0 | 0.049 | 53.1 | 60.8 | 59.1 | 69.4 | 30.7 | <0.001 |
| 2 | 39.3 | 35.4 | 39.7 | 32.8 | 16.5 | 0.089 | 44.5 | 54.1 | 54.6 | 67.8 | 52.3 | <0.001 |
| ≥3 | 36.7 | 26.1 | 27.6 | 27.8 | 24.1 | 0.001 | 43.2 | 45.3 | 50.2 | 64.0 | 48.2 | <0.001 |
| Maternal characteristics | ||||||||||||
| Age at child’s birth (years) | ||||||||||||
| <20 | 36.9 | 32.8 | 42.0 | 29.9 | 18.9 | 0.374 | 46.8 | 58.0 | 53.5 | 65.5 | 40.1 | <0.001 |
| 20–29 | 40.4 | 32.1 | 38.1 | 32.5 | 19.5 | 0.011 | 48.2 | 53.0 | 55.3 | 68.1 | 41.3 | <0.001 |
| ≥30 | 40.9 | 34.6 | 31.1 | 33.5 | 18.2 | 0.037 | 42.9 | 47.6 | 55.6 | 66.0 | 53.9 | <0.001 |
| Level of education | ||||||||||||
| 0–4 | 27.5 | 18.6 | 25.2 | 23.5 | 14.6 | 0.285 | 38.5 | 43.1 | 44.4 | 59.2 | 53.6 | <0.001 |
| 5–9 | 46.9 | 36.9 | 40.0 | 31.2 | 33.3 | <0.001 | 51.9 | 56.2 | 57.3 | 69.5 | 34.1 | <0.001 |
| 10+ | 58.3 | 55.9 | 52.2 | 44.5 | 23.7 | <0.001 | 59.8 | 68.3 | 66.2 | 70.3 | 17.6 | 0.018 |
| Occupation | ||||||||||||
| Housewife | 40.1 | 32.2 | 37.6 | 33.4 | 16.7 | 0.030 | 47.3 | 52.4 | 53.7 | 66.4 | 40.4 | <0.001 |
| Working outside | 38.3 | 39.7 | 37.9 | 30.5 | 20.4 | 0.004 | 45.5 | 60.8 | 59.1 | 68.3 | 50.0 | <0.001 |
| Body mass index (kg/m2) | ||||||||||||
| <18.5 | 31.3 | 26.7 | 31.4 | 29.1 | 6.9 | 0.863 | 46.1 | 48.9 | 51.6 | 67.9 | 47.2 | <0.001 |
| 18.5–22.9 | 39.6 | 32.5 | 36.3 | 28.6 | 27.8 | <0.001 | 45.9 | 55.1 | 54.2 | 65.9 | 43.8 | <0.001 |
| 23.0–24.0 | 58.6 | 39.2 | 39.3 | 34.8 | 40.6 | <0.001 | 47.3 | 52.3 | 60.2 | 68.7 | 45.4 | <0.001 |
| ≥25.0 | 64.7 | 48.9 | 52.6 | 41.9 | 35.2 | <0.001 | 59.1 | 57.2 | 60.2 | 68.2 | 15.3 | 0.011 |
| Paternal characteristics | ||||||||||||
| Level of education | ||||||||||||
| 0–4 | 28.1 | 21.0 | 29.0 | 23.7 | 15.8 | 0.439 | 41.1 | 48.1 | 48.0 | 65.4 | 59.0 | <0.001 |
| 5–9 | 45.1 | 37.9 | 38.9 | 31.3 | 30.7 | <0.001 | 47.9 | 54.0 | 56.3 | 65.2 | 36.1 | <0.001 |
| 10+ | 65.6 | 52.7 | 52.7 | 47.4 | 27.7 | <0.001 | 63.3 | 63.5 | 66.4 | 73.4 | 16.1 | 0.001 |
| Occupation | ||||||||||||
| Service holder/businessman | 50.8 | 40.8 | 44.6 | 40.8 | 19.8 | 0.015 | 55.5 | 57.8 | 60.7 | 68.0 | 22.5 | <0.001 |
| Agriculture-based worker | 31.8 | 27.2 | 32.9 | 23.0 | 27.7 | 0.081 | 44.1 | 49.1 | 47.8 | 64.5 | 46.3 | <0.001 |
| Non-agriculture-based worker | 42.7 | 33.7 | 38.9 | 32.4 | 24.0 | 0.006 | 51.2 | 52.5 | 56.9 | 67.2 | 31.2 | <0.001 |
| Others 5 | 32.6 | 23.1 | 29.0 | 27.7 | 15.0 | 0.268 | 35.2 | 52.7 | 51.0 | 68.9 | 95.7 | <0.001 |
| Characteristics | Vitamin-A Rich Fruits or Vegetables (%) | Other Fruits or Vegetables (%) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2007 | 2011 | 2014 | 2017–2018 | % Change 3 | p 4 | 2007 | 2011 | 2014 | 2017–2018 | % Change 3 | p 4 | |
| Overall | 53.8 | 36.6 | 40.4 | 37.7 | 29.9 | <0.001 | 46.4 | 17.6 | 19.7 | 26.6 | 42.7 | <0.001 |
| Household characteristics | ||||||||||||
| Administrative division | ||||||||||||
| Barisal | 42.5 | 40.6 | 45.0 | 35.7 | 16.2 | 0.465 | 39.6 | 10.6 | 15.5 | 23.5 | 40.6 | 0.026 |
| Chittagong | 45.1 | 35.7 | 36.1 | 40.4 | 10.5 | 0.197 | 42.2 | 11.5 | 17.8 | 30.9 | 26.8 | 0.005 |
| Dhaka | 55.1 | 36.2 | 39.1 | 38.5 | 30.1 | <0.001 | 43.1 | 17.9 | 19.1 | 24.3 | 43.5 | <0.001 |
| Khulna | 56.8 | 35.8 | 53.4 | 24.5 | 56.9 | <0.001 | 47.7 | 26.4 | 32.8 | 27.2 | 43.0 | 0.002 |
| Rajshahi | 66.5 | 39.5 | 38.9 | 37.3 | 43.9 | <0.001 | 61.2 | 24.3 | 15.0 | 23.3 | 61.9 | <0.001 |
| Rangpur 1 | - | 38.9 | 39.6 | 47.0 | −21.1 | 0.067 | - | 19.1 | 20.8 | 31.7 | −65.6 | 0.001 |
| Sylhet | 42.6 | 31.1 | 44.9 | 36.8 | 13.6 | 0.875 | 33.7 | 17.3 | 22.5 | 22.4 | 33.7 | 0.067 |
| Mymensingh 2 | - | - | - | 33.4 | - | - | - | - | - | 27.6 | - | - |
| Place of residence | ||||||||||||
| Urban | 50.9 | 40.2 | 38.2 | 39.6 | 22.3 | 0.001 | 50.7 | 20.7 | 23.6 | 26.3 | 48.2 | <0.001 |
| Rural | 54.6 | 35.6 | 41.2 | 37.0 | 32.2 | <0.001 | 45.1 | 16.7 | 18.3 | 26.7 | 40.8 | <0.001 |
| Household wealth status | ||||||||||||
| Poorest | 50.9 | 29.2 | 37.9 | 35.5 | 30.2 | 0.002 | 45.2 | 14.5 | 20.0 | 20.4 | 54.8 | <0.001 |
| Poorer | 50.3 | 33.2 | 41.4 | 35.8 | 28.9 | 0.001 | 38.6 | 17.4 | 17.0 | 24.7 | 36.1 | <0.001 |
| Middle | 57.2 | 41.2 | 42.6 | 37.0 | 35.4 | <0.001 | 50.3 | 14.3 | 17.0 | 30.0 | 40.4 | <0.001 |
| Richer | 57.0 | 39.3 | 39.6 | 33.2 | 41.8 | <0.001 | 47.4 | 20.8 | 21.7 | 26.4 | 44.3 | <0.001 |
| Richest | 54.4 | 42.4 | 41.2 | 47.7 | 12.4 | 0.090 | 51.8 | 21.7 | 22.6 | 32.2 | 37.8 | <0.001 |
| Child characteristics | ||||||||||||
| Age (month) | ||||||||||||
| 6–8 | 27.0 | 13.9 | 18.6 | 14.6 | 46.0 | 0.001 | 21.8 | 5.0 | 5.6 | 12.2 | 44.1 | <0.001 |
| 9–11 | 48.3 | 31.8 | 30.6 | 31.0 | 35.9 | <0.001 | 39.8 | 15.2 | 20.3 | 19.5 | 51.0 | <0.001 |
| 12–17 | 59.0 | 40.6 | 46.1 | 43.2 | 26.8 | <0.001 | 52.1 | 18.5 | 17.7 | 31.4 | 39.7 | <0.001 |
| 18–23 | 65.9 | 48.3 | 51.0 | 46.2 | 30.0 | <0.001 | 57.6 | 25.5 | 28.7 | 31.9 | 44.6 | <0.001 |
| Gender | ||||||||||||
| Male | 53.0 | 36.9 | 38.7 | 40.1 | 24.3 | <0.001 | 49.1 | 16.5 | 19.1 | 26.9 | 45.3 | <0.001 |
| Female | 54.5 | 36.4 | 42.4 | 35.0 | 35.8 | <0.001 | 43.8 | 18.8 | 20.4 | 26.3 | 39.9 | <0.001 |
| Birth order | ||||||||||||
| 1 | 57.3 | 40.7 | 41.0 | 40.5 | 29.4 | <0.001 | 48.7 | 19.2 | 20.0 | 30.6 | 37.2 | <0.001 |
| 2 | 51.2 | 35.3 | 39.7 | 35.0 | 31.6 | <0.001 | 46.1 | 17.6 | 18.0 | 24.9 | 46.0 | <0.001 |
| ≥3 | 52.5 | 34.1 | 40.6 | 37.6 | 28.4 | <0.001 | 44.7 | 16.3 | 21.3 | 24.0 | 46.3 | <0.001 |
| Maternal characteristics | ||||||||||||
| Age at child’s birth (years) | ||||||||||||
| <20 | 54.9 | 40.7 | 40.3 | 36.1 | 34.2 | <0.001 | 44.0 | 17.9 | 16.6 | 27.3 | 38.0 | <0.001 |
| 20–29 | 54.4 | 34.7 | 40.7 | 37.6 | 30.9 | <0.001 | 48.8 | 16.7 | 19.6 | 25.7 | 47.2 | <0.001 |
| ≥30 | 50.4 | 38.7 | 39.8 | 39.3 | 22.0 | 0.012 | 41.9 | 20.4 | 23.9 | 28.4 | 32.2 | 0.004 |
| Level of education | ||||||||||||
| 0–4 | 49.9 | 30.9 | 36.1 | 34.7 | 30.4 | <0.001 | 39.8 | 15.3 | 16.0 | 21.7 | 45.5 | <0.001 |
| 5–9 | 56.7 | 36.8 | 40.2 | 34.7 | 38.7 | <0.001 | 51.1 | 17.3 | 20.2 | 25.6 | 49.9 | <0.001 |
| 10+ | 58.3 | 52.4 | 48.8 | 48.3 | 17.0 | 0.014 | 54.3 | 25.5 | 24.7 | 34.6 | 36.3 | <0.001 |
| Occupation | ||||||||||||
| Housewife | 53.2 | 36.2 | 41.2 | 36.9 | 30.7 | <0.001 | 43.4 | 17.4 | 19.2 | 25.9 | 40.3 | <0.001 |
| Working outside | 55.7 | 42.0 | 37.9 | 39.0 | 30.0 | <0.001 | 56.7 | 20.0 | 21.5 | 27.7 | 51.2 | <0.001 |
| Body mass index (kg/m2) | ||||||||||||
| <18.5 | 54.9 | 35.2 | 36.8 | 34.8 | 36.6 | <0.001 | 47.8 | 15.0 | 14.3 | 20.9 | 56.3 | <0.001 |
| 18.5–22.9 | 51.7 | 35.7 | 40.5 | 38.0 | 26.6 | <0.001 | 44.0 | 18.7 | 20.2 | 25.7 | 41.6 | <0.001 |
| 23.0–24.0 | 56.9 | 42.3 | 45.8 | 38.1 | 33.1 | 0.003 | 43.2 | 18.8 | 26.8 | 29.3 | 32.2 | 0.334 |
| ≥25.0 | 61.0 | 41.0 | 43.0 | 39.5 | 35.2 | 0.002 | 61.9 | 19.9 | 23.0 | 32.2 | 48.0 | 0.003 |
| Paternal characteristics | ||||||||||||
| Level of education | ||||||||||||
| 0–4 | 51.8 | 32.6 | 36.0 | 35.3 | 31.7 | <0.001 | 43.8 | 17.1 | 18.4 | 23.5 | 46.4 | <0.001 |
| 5–9 | 52.2 | 35.3 | 42.7 | 35.1 | 32.7 | <0.001 | 46.6 | 15.1 | 18.7 | 25.9 | 44.5 | <0.001 |
| 10+ | 63.4 | 49.5 | 44.9 | 46.0 | 27.4 | <0.001 | 54.3 | 23.8 | 24.5 | 32.9 | 39.5 | <0.001 |
| Occupation | ||||||||||||
| Service holder/businessman | 58.8 | 41.0 | 46.1 | 42.8 | 27.2 | <0.001 | 46.6 | 17.6 | 21.6 | 28.5 | 38.9 | <0.001 |
| Agriculture-based worker | 53.1 | 37.2 | 33.9 | 34.7 | 34.7 | <0.001 | 48.5 | 18.0 | 16.5 | 25.0 | 48.4 | <0.001 |
| Non-agriculture-based worker | 52.3 | 33.8 | 40.8 | 37.1 | 29.1 | <0.001 | 48.9 | 17.6 | 21.1 | 26.4 | 46.0 | <0.001 |
| Others 5 | 50.8 | 34.0 | 39.0 | 33.4 | 34.3 | <0.001 | 40.7 | 17.0 | 17.9 | 24.1 | 40.9 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mistry, S.K.; Hossain, M.B.; Irfan, N.M.; Saha, M.; Saberin, S.; Shamim, A.A.; Arora, A. Trends in Complementary Feeding Indicators and Intake from Specific Food Groups among Children Aged 6–23 Months in Bangladesh. Int. J. Environ. Res. Public Health 2022, 19, 550. https://doi.org/10.3390/ijerph19010550
Mistry SK, Hossain MB, Irfan NM, Saha M, Saberin S, Shamim AA, Arora A. Trends in Complementary Feeding Indicators and Intake from Specific Food Groups among Children Aged 6–23 Months in Bangladesh. International Journal of Environmental Research and Public Health. 2022; 19(1):550. https://doi.org/10.3390/ijerph19010550
Chicago/Turabian StyleMistry, Sabuj Kanti, Md Belal Hossain, Nafis Md Irfan, Manika Saha, Silvia Saberin, Abu Ahmed Shamim, and Amit Arora. 2022. "Trends in Complementary Feeding Indicators and Intake from Specific Food Groups among Children Aged 6–23 Months in Bangladesh" International Journal of Environmental Research and Public Health 19, no. 1: 550. https://doi.org/10.3390/ijerph19010550
APA StyleMistry, S. K., Hossain, M. B., Irfan, N. M., Saha, M., Saberin, S., Shamim, A. A., & Arora, A. (2022). Trends in Complementary Feeding Indicators and Intake from Specific Food Groups among Children Aged 6–23 Months in Bangladesh. International Journal of Environmental Research and Public Health, 19(1), 550. https://doi.org/10.3390/ijerph19010550