
Strengthening the Health System as a Strategy to Achieving a Universal Health Coverage in Underprivileged Communities in Africa: A Scoping Review


 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Defining the Research Question
2.2. Inclusion Criteria
2.3. Search Strategy
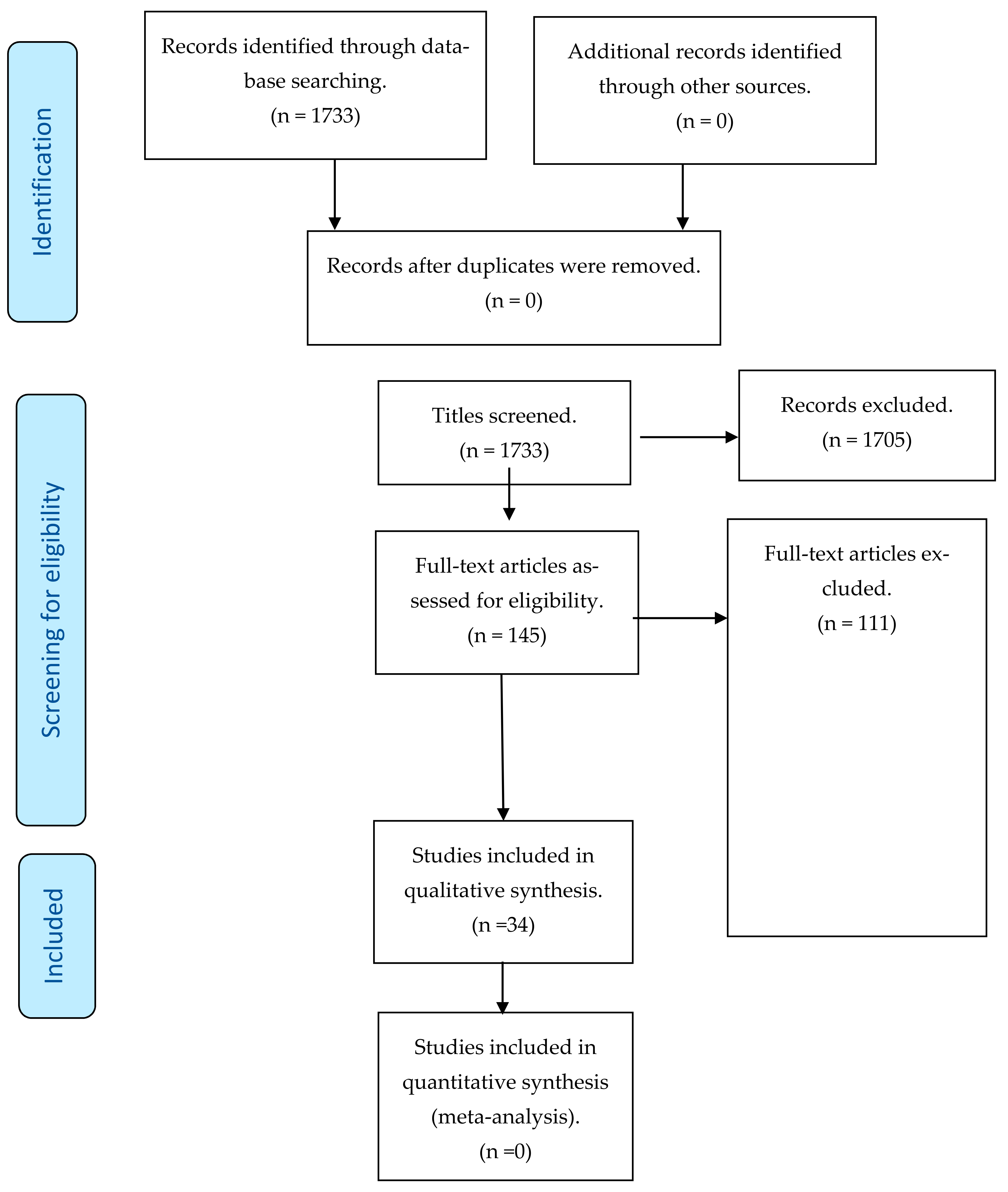
2.4. Selection of Studies Relevant to the Research Question
2.5. Extraction and Charting the Results
2.6. Patient and Public Involvement
3. Results
3.1. Characteristics of Included Studies
3.1.1. Setting and Publication Dates
3.1.2. Study Designs
3.1.3. Participants
Health Providers
Policy Makers
Patients/Consumers
3.2. Interventions to Increase Universal Health Coverage
3.2.1. Health Workforce: Developing and Improving Health Infrastructure
3.2.2. Health Information Systems: Health Technology
3.2.3. Access to Essential Medicines
3.2.4. Health Financing
4. Discussion
4.1. Country Reports on Achieving UHC in Africa
4.2. Progress and Challenges of UHC in Africa
Government Spending on Health Has Increased
4.3. Growth in Development Assistance for Health
4.4. Service Delivery Capacity Has Expanded
4.5. Non-State vs. State Healthcare Workers in Achieving UHC
4.6. Essential Medicines and Technologies
4.7. Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sanogo, A.N.; Fantaye, W.A.; Yaya, S. Universal Health Coverage and facilitation of equitable access to care in Africa: A systematic review. Front. Public Heal. 2019, 7, 102. [Google Scholar] [CrossRef] [Green Version]
- Fadlallah, R.; El-Jardali, F.; Hemadi, N.; Morsi, R.Z.; Abou Samra, C.A.; Ahmad, A.; Arif, K.; Hishi, L.; Honein-Abouhaidar, G.; Akl, E.A. Barriers and facilitators to implementation, uptake and sustainability of community-based health insurance schemes in low- and middle-income countries: A systematic review. Int. J. Equity Health 2018, 17. [Google Scholar] [CrossRef] [Green Version]
- Friebel, R.; Molloy, A.; Leatherman, S.; Dixon, J.; Bauhoff, S.; Chalkidou, K. Achieving high-quality universal health coverage: A perspective from the National Health Service in England. BMJ Glob. Heal. 2018, 3, 1–6. [Google Scholar] [CrossRef]
- Fusheini, A.; Eyles, J. Achieving universal health coverage in South Africa through a district health system approach: Conflicting ideologies of health care provision. BMC Health Serv. Res. 2016, 16, 558. [Google Scholar] [CrossRef] [Green Version]
- Hodes, R.; Price, I.; Bungane, N.; Hons, B.; Toska, E.; Cluver, L. How front-line healthcare workers respond to stock-outs of essential medicines in the Eastern Cape Province of South Africa. S. Afr. Med. J. 2017, 107, 2016–2018. [Google Scholar] [CrossRef] [Green Version]
- Tarricone, R. Setting the Scene: The Challenges of Universal Health Coverage and the Contribution of Management Education. Value Heal. 2013, 16, S4–S6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kutzin, J.; Sparkes, S.P. Health systems strengthening, universal health coverage, health security and resilience. Bull World Heal. Organ. 2016, 94, 2. [Google Scholar] [CrossRef]
- Kruk, M.E.; Gage, A.D.; Arsenault, C.; Jordan, K.; Leslie, H.H.; Roder-DeWan, S.; Adeyi, O.; Barker, P.; Daelmans, B.; Doubova, S.V.; et al. High-quality health systems in the Sustainable Development Goals era: Time for a revolution. Lancet Glob. Heal. 2018, 6, e1196–e1252. [Google Scholar] [CrossRef] [Green Version]
- Kieny, M.P.; Bekedam, H.; Dovlo, D.; Fitzgerald, J.; Habicht, J.; Harrison, G.; Kluge, H.; Lin, V.; Menabde, N.; Mirza, Z.; et al. Strengthening Health Systems For Universal Health Coverage and Sustainable Development. Available online: http://www.who.int/entity/bulletin/volumes/95/7/16-187476.pdf (accessed on 6 September 2019).
- Gilson, L.; Kalyalya, D.; Kuchler, F.; Lake, S.; Oranga, H.; Ouendo, M. The equity impacts of community financing activities in three African countries. Int. J. Health Plann. Manag. 2000, 15, 291–317. [Google Scholar] [CrossRef]
- McLaren, Z.; Ardington, C.; Leibbrandt, M. Distance as a Barrier to Health Care Access in South Africa; University of Cape Town: Cape Town, South Africa, 2013. [Google Scholar]
- Bredenkamp, C.; Evans, T.; Lagrada, L.; Langenbrunner, J.; Nachuk, S.; Palu, T. Emerging challenges in implementing universal health coverage in Asia. Soc. Sci. Med. 2014, 145, 243–248. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Universal Health Coverage. Available online: https://www.who.int/news-room/fact-sheets/detail/universal-health-coverage-(uhc) (accessed on 20 December 2021).
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horton, S.; Camacho Rodriguez, R.; Anderson, B.O.; Aung, S.; Awuah, B.; Delgado Pebé, L.; Duggan, C.; Dvaladze, A.; Kumar, S.; Murillo, R.; et al. Health system strengthening: Integration of breast cancer care for improved outcomes. Cancer 2020, 126, 2353–2364. [Google Scholar] [CrossRef] [PubMed]
- Cotlear, D.; Nagpal, S.; Smith, O.; Tandon, A.; Cortez, R. How 24 Developing Countries are Implementing Universal Health Coverage Reforms from the Bottom Up. World Bank Publications: Herndon, VA, USA, 2015; ISBN 9781464806100. [Google Scholar]
- Abdulmalik, J.; Olayiwola, S.; Docrat, S.; Lund, C.; Chisholm, D.; Gureje, O. Sustainable financing mechanisms for strengthening mental health systems in Nigeria. Int. J. Ment. Health Syst. 2019, 13, 38. [Google Scholar] [CrossRef] [PubMed]
- Ebunoha, G.N.; Ughasoro, M.D.; Nwakoby, I.C.; Onwujekwe, O.E. Achieving financial risk protection through a national Social Health Insurance Programme in Nigeria: Perspectives of enrollees and healthcare providers. Int. J. Health Plann. Manage. 2019, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kapologwe, N.A.; Meara, J.G.; Kengia, J.T.; Sonda, Y.; Gwajima, D.; Alidina, S.; Kalolo, A. Development and upgrading of public primary healthcare facilities with essential surgical services infrastructure: A strategy towards achieving universal health coverage in Tanzania. BMC Health Serv. Res. 2020, 20, 218. [Google Scholar] [CrossRef]
- Laokri, S.; Soelaeman, R.; Hotchkiss, D.R. Assessing out-of-pocket expenditures for primary health care: How responsive is the Democratic Republic of Congo health system to providing financial risk protection? BMC Health Serv. Res. 2018, 18, 451. [Google Scholar] [CrossRef]
- Lavers, T. Towards Universal Health Coverage in Ethiopia’s “developmental state”? The political drivers of health insurance. Soc. Sci. Med. 2019, 228, 60–67. [Google Scholar] [CrossRef]
- Maluka, S.; Chitama, D.; Dungumaro, E.; Masawe, C.; Rao, K.; Shroff, Z. Contracting-out primary health care services in Tanzania towards UHC: How policy processes and context influence policy design and implementation. Int. J. Equity Health 2018, 17, 118. [Google Scholar] [CrossRef] [Green Version]
- Kasilo, O.M.J.; Wambebe, C.; Nikiema, J.-B.; Nabyonga-Orem, J. Towards universal health coverage: Advancing the development and use of traditional medicines in Africa. BMJ Glob. Heal. 2019, 4. [Google Scholar] [CrossRef] [PubMed]
- Nagai, M.; Fujita, N.; Diouf, I.S.; Salla, M. Retention of qualified healthcare workers in rural Senegal: Lessons learned from a qualitative study. Rural Remote Health 2017, 17, 4149. [Google Scholar] [CrossRef] [Green Version]
- Nakovics, M.I.; Brenner, S.; Bongololo, G.; Chinkhumba, J.; Kalmus, O.; Leppert, G.; De Allegri, M. Determinants of healthcare seeking and out-of-pocket expenditures in a “free” healthcare system: Evidence from rural Malawi. Health Econ. Rev. 2020, 10, 14. [Google Scholar] [CrossRef] [PubMed]
- Perehudoff, S.K.; Alexandrov, N.V.; Hogerzeil, H.V. Legislating for universal access to medicines: A rights-based cross-national comparison of UHC laws in 16 countries. Health Policy Plan. 2019, 34, iii48–iii57. [Google Scholar] [CrossRef] [PubMed]
- Renggli, S.; Mayumana, I.; Mboya, D.; Charles, C.; Mshana, C.; Kessy, F.; Glass, T.R.; Lengeler, C.; Schulze, A.; Aerts, A.; et al. Towards improved health service quality in Tanzania: Contribution of a supportive supervision approach to increased quality of primary healthcare. BMC Health Serv. Res. 2019, 19, 848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shamu, S.; January, J.; Rusakaniko, S. Who benefits from public health financing in Zimbabwe? Towards universal health coverage. Glob. Public Health 2017, 12, 1169–1182. [Google Scholar] [CrossRef] [PubMed]
- Uzochukwu, B.S.C.; Okeke, C.; O’Brien, N.; Ruiz, F.; Sombie, I.; Hollingworth, S. Health technology assessment and priority setting for universal health coverage: A qualitative study of stakeholders’ capacity, needs, policy areas of demand and perspectives in Nigeria. Global. Health 2020, 16, 58. [Google Scholar] [CrossRef]
- Workie, N.W.; Shroff, E.; Yazbeck, A.S.; Nguyen, S.N.; Karamagi, H. Who Needs Big Health Sector Reforms Anyway? Seychelles’ Road to UHC Provides Lessons for Sub-Saharan Africa and Island Nations. Heal. Syst. Reform 2018, 4, 362–371. [Google Scholar] [CrossRef] [Green Version]
- Yip, W.; Berman, P. Targeted health insurance in a low income country and its impact on access and equity in access: Egypt’s school health insurance. Health Econ. 2001, 10, 207–220. [Google Scholar] [CrossRef]
- Koon, A.D.; Conrad, A.; Naimoli, J.F.; Saxena, S.; Connor, C.; Rodriguez, D.C. Implementing health system strengthening projects at USAID: Findings from five cases using an integrated framework. Glob. Public Health 2019, 14, 1829–1846. [Google Scholar] [CrossRef]
- Demissie, B.; Negeri, K.G. Effect of community-based health insurance on utilization of outpatient health care services in southern ethiopia: A comparative cross-sectional study. Risk Manag. Healthc. Policy 2020, 13, 141–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelissen, H.E.; Brals, D.; Ameen, H.A.; van der List, M.; Kramer, B.; Akande, T.M.; Janssens, W.; Van’t Hoog, A.H. The prominent role of informal medicine vendors despite health insurance: A weekly diaries study in rural Nigeria. Health Policy Plan. 2020, 35, 354–363. [Google Scholar] [CrossRef] [Green Version]
- Woldemichael, A.; Takian, A.; Akbari Sari, A.; Olyaeemanesh, A. Availability and inequality in accessibility of health centre-based primary healthcare in Ethiopia. PLoS ONE 2019, 14, e0213896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Were, L.P.O.; Were, E.; Wamai, R.; Hogan, J.; Galarraga, O. Effects of social health insurance on access and utilization of obstetric health services: Results from HIV+ pregnant women in Kenya. BMC Public Health 2020, 20, 87. [Google Scholar] [CrossRef] [Green Version]
- Sanogo, N.A.; Yaya, S. Wealth Status, Health Insurance, and Maternal Health Care Utilization in Africa: Evidence from Gabon. Biomed Res. Int. 2020, 2020, 4036830. [Google Scholar] [CrossRef] [PubMed]
- Mwase, T.; Brenner, S.; Mazalale, J.; Lohmann, J.; Hamadou, S.; Somda, S.M.A.; Ridde, V.; De Allegri, M. Inequities and their determinants in coverage of maternal health services in Burkina Faso. Int. J. Equity Health 2018, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abiiro, G.A.; Mbera, G.B.; De Allegri, M. Gaps in universal health coverage in Malawi: A qualitative study in rural communities. BMC Health Serv. Res. 2014, 14, 234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suchman, L.; Hashim, C.V.; Adu, J.; Mwachandi, R. Seeking care in the context of social health insurance in Kenya and Ghana. BMC Public Health 2020, 20. [Google Scholar] [CrossRef]
- Knoblauch, A.M.; de la Rosa, S.; Sherman, J.; Blauvelt, C.; Matemba, C.; Maxim, L.; Defawe, O.D.; Gueye, A.; Robertson, J.; McKinney, J.; et al. Bi-directional drones to strengthen healthcare provision: Experiences and lessons from Madagascar, Malawi and Senegal. BMJ Glob. Heal. 2019, 4, e001541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathews, C.; Goga, A.; Loveday, M.; Zembe, W.; Daviaud, E.; Siegfried, N.; Lewin, S. Moving towards universal health coverage: Strengthening the evidence ecosystem for the South African health system. South Afr. Med. J. 2019, 109, 8–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miot, J.; Thiede, M. Adapting Pharmacoeconomics to Shape Efficient Health Systems en Route to UHC—Lessons from Two Continents. Front. Pharmacol. 2017, 8, 715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Den Heever, A.M. The role of insurance in the achievement of universal coverage within a developing country context: South Africa as a case study. BMC Public Health 2012, 12, S5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mbogo, B.A.; McGill, D. perspectives on financing population-based health care towards Universal Health Coverage among employed individuals in Ghanzi district, Botswana: A qualitative study. BMC Health Serv. Res. 2016, 16. [Google Scholar] [CrossRef] [Green Version]
- Husøy, O.K.; Molla, S.M.; Muluken, G.; Marie, M.K.; Frithof, N.O.; Ingrid, M. Selling my sheep to pay for medicines—Household priorities and coping strategies in a setting without universal health coverage. BMC Health Serv. Res. 2018, 18, 153. [Google Scholar] [CrossRef] [Green Version]
- Lu, C.; Chin, B.; Lewandowski, J.L.; Basinga, P.; Hirschhorn, L.R.; Hill, K.; Murray, M.; Binagwaho, A. Towards universal health coverage: An evaluation of Rwanda Mutuelles in its first eight years. PLoS ONE 2012, 7, e39282. [Google Scholar] [CrossRef] [Green Version]
- Mills, A.; Ally, M.; Goudge, J.; Gyapong, J.; Mtei, G. Progress towards universal coverage: The health systems of Ghana, South Africa and Tanzania. Health Policy Plan. 2012, 27 (Suppl. 1), i4–i12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foster, A.A.; Makukula, M.K.; Moore, C.; Chizuni, N.L.; Goma, F.; Myles, A.; Nelson, D. Strengthening and Institutionalizing the Leadership and Management Role of Frontline Nurses to Advance Universal Health Coverage in Zambia. Glob. Heal. Sci. Pract. 2018, 6, 736–746. [Google Scholar] [CrossRef] [PubMed]
- Onwujekwe, O.; Onoka, C.; Nwakoby, I.; Ichoku, H.; Uzochukwu, B.; Wang, H. Examining the Financial Feasibility of Using a New Special Health Fund to Provide Universal Coverage for a Basic Maternal and Child Health Benefit Package in Nigeria. Front. Public Heal. 2018, 6, 200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abodey, E.; Vanderpuye, I.; Mensah, I.; Badu, E. In search of universal health coverage-highlighting the accessibility of health care to students with disabilities in Ghana: A qualitative study. BMC Health Serv. Res. 2020, 20, 270. [Google Scholar] [CrossRef]
- Asante, A.; Price, J.; Hayen, A.; Jan, S.; Wiseman, V. Equity In Health care financing in low-and middle-income countries: A systematic review of evidence from studies using benefit and financing incidence analyses. PLoS ONE 2016, 11, e0152866. [Google Scholar] [CrossRef] [Green Version]
- Ranabhat, C.L.; Acharya, D. Methodological issues on “challenges and opportunities towards the road of universal health coverage (UHC) in Nepal: A systematic review”. Arch. Public Heal. 2020, 78, 1–10. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization World Health Organization. Universal Health Coverage. 2020. Available online: https://www.who.int/health-topics/universal-health-coverage#tab=tab_1 (accessed on 20 September 2021).
- Bonilla-chacin, M.E.; Rathe, M. UNICO: Demand Side Strategies for Universal Health Coverage (UHC). World Hospitals and Health Services-Universal Health Coverage (UHC): Making Progress Towards the 2016. 54, pp. 26–30. Available online: https://fundacionplenitud.org/wp-content/uploads/2020/04/Bonilla-Rathe-Demand-side-financing-for-UHC.pdf (accessed on 20 September 2021).
- World Bank. UHC in Africa: A Framework for Action Executive Summary. 2016. Available online: http://hdl.handle.net/10986/26072 (accessed on 20 September 2021).


{kind=link}
| Population | Concept | Context |
|---|---|---|
| Health policy makers, healthcare providers, health facilities, government and non-government organizations (e.g., health insurance companies) | Access to healthcare services or UHC | Africa |
| Search # | Search String |
|---|---|
| #1 | “Comprehensive Health Insurance” OR “Universal Coverage” OR “Insurance Coverage” OR “Insurance, Hospitalization” OR “Single-Payer System” OR “Prepaid Health Plans” OR “Not-For Profit Insurance Plans” OR “Insurance, Health”) OR “Universal Health Coverage” |
| #2 | implement* OR facilitat* OR enabl* OR resist* OR promot* OR applica* OR integrat* OR utiliz* OR utilis* OR success* OR access* OR accept* OR lesson* OR experienc* OR scale-up OR roll-out OR sustainab* |
| #3 | “Health systems” OR “Health facility” OR “Health care services” OR “Health services” OR “Healthcare services” OR “Healthcare workers” OR “Health care workers” OR “Healthcare providers” OR “Health care providers” |
| #4 | Algeria OR Angola OR Benin OR Botswana OR Burkina Faso OR Burundi OR Cameroon OR “Cape Verde” OR “Central African Republic” OR Chad OR “Democratic Republic” of Congo OR “Republic of Congo” OR “Cote d’Ivoire” OR Djibouti OR Egypt OR “Equatorial Guinea” OR Eritrea OR Ethiopia OR Gabon OR Gambia OR Ghana OR Guinea OR Guinea Bissau OR Kenya OR Lesotho OR Liberia OR Libya OR Madagascar OR Malawi OR Mali OR Mauritania OR Mauritius OR Morocco OR Mozambique OR Namibia OR Niger OR Nigeria OR Reunion OR Rwanda OR “Sao Tome and Principe” OR Senegal OR Seychelles OR “Sierra Leone” OR Somalia OR “South Africa” OR “South Sudan” OR Sudan OR Swaziland OR Tanzania OR Togo OR Tunisia OR Uganda OR Zambia OR Zimbabwe |
| #5 | #1 AND #2 AND #3 AND #4 |
| Author, Year | Population | Intervention to UHC | Aim of the Study | Outcome | Study Design | Setting |
|---|---|---|---|---|---|---|
| Abdulmalik, 2019 [17] | Health and financial sectors stakeholders. | Financing support and increasing HCW force. | To review the health and socioeconomic contexts of Nigeria as well as to generate strategies for sustainable mental health financing that will be feasible, within the specific context of the country. | Financing strategies: governance and leadership, financing generation, and financing pooling. | Cross-sectional study | Nigeria |
| Ebunoha, 2019 [18] | Consumers and providers of the Formal Sector Social Health Insurance Programme and healthcare workers. | Financing support and increasing HCW force. | To understand peoples’ perceptions of the Formal Sector Social Health Insurance Programme. To understand the prevalence of out-of-pocket among enrollees of the FSSHIP, which will provide an evidence base on the financial risk protection that the scheme currently provides. | Nigeria needs to show a strong commitment to achieving UHC by involving the informal sector in the social health insurance scheme through awareness campaign about the benefits of NHIS. | Cross-sectional study | Nigeria |
| Kapologwe, 2020 [19] | Primary health facilities. | Developing and upgrading infrastructure of primary healthcare facilities. | To understand the public sector’s efforts to improve the infrastructure of primary health facilities between 2005 and 2019. | In this study only 17.4% of 115 health centers had facilities for offering blood transfusion services and 33% (1673) of health facilities had piped water and 5.1% had landline telecommunication system. | Cross-sectional study | Tanzania |
| Laokri, 2018 [20] | Household and health facility representatives. | Health financing through household out-of-pocket payments. | To gain a deeper understanding of the poverty impact of using essential care services in selected provinces in the DRC. We sought to inform the evidence base regarding the policy and technical challenges inherent to developing financial risk protection strategies. | Those who did not seek care when needed reported financial constraints as the major reason for postponing or foregoing care. Wealth-related inequities were found in service and population coverage and in out-of-pocket payment for outpatient care. | Cross-sectional study | Democratic Republic of Congo |
| Lavers, 2019 [21] | Politicians, policy makers, and donor officials. | Health financing through social health insurance. | To examine the political drivers of the adoption and evolution of state health insurance based on 28 key informant interviews conducted between 2015 and 2018 with politicians, policy makers, and donor officials. | The government noted insurance as a possible source of finance in the 1993 Health Policy and 1998 Healthcare Financing Strategy (HCFS). Nonetheless, health insurance was merely one of many future policy options, without a clear implementation strategy. | Cross-sectional study | Ethiopia |
| Maluka, 2018 [22] | Actors, policy processes, and content. | Contract out the delivery of primary health care services. | To report on the design and implementation of service agreements (SAs) between local governments and NSPs for the provision of primary healthcare services in Tanzania. It examines the actors, policy process, context, and policy content that influenced how the SAs were designed and implemented. | Delays in reimbursements, limited financial and technical capacity of local government authorities, and lack of trust between the government and private partners affected the implementation of the contractual arrangements. | Cross-sectional study | Tanzania |
| Kasilo, 2019 [23] | Traditional and conventional health practitioners. | African traditional medicine (ATM) and traditional health practitioners (THPs). | To report the regional status of African traditional medicine and traditional health practitioners (THPs) using information from the survey conducted in 47 countries in sub-Saharan Africa. The survey focused on the nature and level of collaboration between THPs and community-based health plans concerning research, training, treatment, and care. | The significant progress made by some African countries in the development and integration of ATM and THPs into the national health systems provides lessons that can be harnessed to improve access to quality health services and subsequently contribute to the attainment of UHC. The research infrastructure and mechanisms in place provide a platform for further development of efficacious and affordable ATM. | Cross-sectional study | 47 countries in the WHO African region |
| Nagai, 2017 [24] | Doctors, nurses, midwives, and superior technicians in anesthesiology. | Retention of qualified healthcare workers in rural areas. | To identify the determining factors for the retention of qualified human resources for health in rural areas, and to explore an effective and feasible policy that the Ministry of Health could implement in the member countries. | Improved human resources for health (HRH) management, e.g., the transparency of human resource management by the MoH, was identified as a pre-condition of any policy implementation related to HRH. This factor can be considered in other countries struggling to retain healthcare workers in rural areas. | Cross-sectional study | Senegal |
| Nakovics, 2020 [25] | Households. | Financial support (out-of-pocket expenditure). | To investigate out-of-pocket expenditure (OOPE) on curative healthcare services and their determinants in rural Malawi, a country that has consistently aimed at providing free healthcare services. | Our findings indicate that a formal policy commitment to providing free healthcare services is not enough to guarantee widespread financial protection and that additional measures are needed to protect particularly vulnerable population groups. | Cross-sectional study | Malawi |
| Perehudof, 2019 [26] | National UHC legislation that promote universal access to medicines. | Access to medicines. | To identify and compares legal texts from national UHC legislation that promote universal access to medicines in the legislation of 16 mostly LMICs. | National policies, particularly for pharmaceuticals, health, and intellectual property, can instruct the development of health law or substitute it entirely by directing state policies and programming. Future research should investigate the content, implementation, and impact of national policies in relation to access to medicines as part of the right to health. | Cross-sectional study | Algeria, Ghana, Nigeria, Rwanda, South Africa, Tanzania |
| Renggli, 2019 [27] | Healthcare providers from the public and private sector. | Improving quality of primary healthcare through enhanced routine supportive supervision. | To improve quality of primary healthcare through enhanced routine supportive supervision. | The results showed that the new approach managed to address quality issues that could be solved either solely by the healthcare provider, or in collaboration with the council. The new approach was able to improve and maintain crucial primary healthcare quality standards across different health facility level and owner categories in various contexts. | Cross-sectional study | Tanzania |
| Shamu, 2016 [28] | Households. | Health financing. | To assess the utilization of healthcare services and benefits at different levels of care by different socioeconomic groups. | Our results showed that richer people disproportionately benefited from public health subsidies overall, particularly at secondary and tertiary levels, which receive more funding and provide a higher level of care. | Cross-sectional study | Zimbabwe |
| Uzochukwu, 2020 [29] | Decision makers, policy makers, academic researchers, civil society organizations, community-based organizations, development partners, and health professional organizations. | Health technology assessment (HTA) is an effective tool to support priority setting and generate evidence for decision making especially en route to achieving UHC. | To assess the capacity needs, policy areas of demand, and perspectives of key stakeholders for evidence-informed decision making in Nigeria, where health technology assessment is still new. | Public health programs, medicines, and vaccines were the three main technology types that would especially benefit from the application of HTA. The perceived availability and accessibility of suitable local data to support HTA varied widely but was mostly considered inadequate and limited. | Cross-sectional study | Nigeria |
| Workie, 2018 [30] | Ministry of Finance. | Health insurance, provider–funder separation. | To trace the factors that facilitated UHC success in the Seychelles, including high political commitment, strong voice and a downward accountability culture, strong public health functions, and an impressive investment in primary healthcare. | Two decades later, in 2000, the number of health centers more than doubled to 17; the number of doctors and dentists increased more than fivefold to 119; coverage of essential child, maternal, and reproductive health pushed to the upper 90%; the infant mortality rate dropped by over three quarters from 43.2 per 1000 live births in 1977 to 9.9 per 1000 live births in the year 2000; and average life expectancy for both sexes increased from 69.5 in 1980 to 72.7 years in 2000. | Cross-sectional study | Seychelles |
| Yip, 2001 [31] | Households. | Health insurance system that targets school children, School Health Insurance Programme (SHIP). | To assesses the extent to which the School Health Insurance Programme achieves its stated goals, that is, improving access and equity in access to healthcare for children. | Our findings show that the SHIP significantly improved access by increasing visit rates and reducing financial burden of use (out-of-pocket expenditures). Regarding the success of targeting the poor, conditional upon being covered, the SHIP reduced the differentials in visit rates between the highest- and lowest-income children. However, only the middle-income children benefited from reduced financial burden. | Cross-sectional study | Egypt |
| Koon, 2019 [32] | Different political contexts. | Evidence on the implementation of health systems strengthening (HSS) interventions is scarce. Donors need this information to prioritize investments and lobby for continued financial support. | To identify and reflect upon the factors that facilitate or impede health system strengthening interventions within and between contexts, and especially in donor-funded projects. | As donors’ transition to new forms of technical assistance, this article explores how attenuated contributions may continue to facilitate health system strengthening. This includes a strong commitment to participatory processes of engagement in the design and implementation of well-defined activities at multiple levels of the health system, by harnessing the power of an array of actors. We introduce a number of key considerations for donors, including the way in which HSS projects are structured, supported, and financed. The research presented here not only contributes to the global pool of knowledge on HSS, but also helps further implementation science, and thereby carries the potential to ultimately enhance health service delivery for the poor and vulnerable. | Cross sectional study | Ethiopia, Rwanda, and Zambia |
| Demissie, 2020 [33] | Household heads. | Community-based health insurance. | To analyze the effects of a community-based health insurance scheme on the utilization of healthcare services in Yirgalem town, southern Ethiopia. | The study reveals that community-based health insurance member households were about three times more likely to utilize outpatient care than their non-member counterparts. | Cross-sectional study | Ethiopia |
| Nelissen, 2020 [34] | Individuals with access to a private subsidized health insurance program. | Healthcare insurance program. | To explore the utilization of different types of healthcare providers and the factors associated with provider choice by insurance status in rural Nigeria. | The study shows that higher utilization of formal healthcare for insured compared to uninsured health episodes was driven by higher utilization of upgraded facilities. Upgraded facilities in the Kwara State Health Insurance Programme were visited during 20% of insured episodes compared with only 3% of uninsured episodes. Contrary to program implementers’ expectations, individuals with an uninsured episode did not access the upgraded facilities to benefit from the improved quality care. | Cross-sectional study | Nigeria |
| Woldemichael, 2019 [35] | Population-based analysis of district-level. | Trend of inequalities in accessibility of health center-based primary healthcare (PHC). | To assess availability and measure magnitude and trend of inequalities in accessibility of health center-based primary health care resources in Ethiopia from 2015 to 2017. | This analysis provided a clear picture of availability and inequalities in PHC resources across three regions in Ethiopia. Identifying contributing factors to low densities and high inequalities of SHWs may help improve PHC services nationwide, along with pathway toward UHC. | Cross-sectional study | Ethiopia |
| Were, 2020 [36] | Pregnant women living with HIV. | Effect of health insurance on obstetric healthcare. | To analyze the effect of health insurance on obstetric healthcare access including institutional delivery and skilled birth attendants for HIV+ pregnant women in Kenya. | This study confirms conceptual and practical considerations around health insurance and healthcare access for HIV+ persons. Further, it helps to inform relevant policy development for health insurance and HIV financing and delivery in Kenya and in similar countries in sub-Saharan Africa in the universal health coverage (UHC) era. | Cross-sectional study | Kenya |
| Sanogo, 2020 [37] | Antenatal care (ANC) visits during pregnancy, place of birth delivery, and postnatal health care. | Association of compulsory health insurance on maternal healthcare utilization. | To explore the wealth-related association of compulsory health insurance on maternal healthcare utilization in Gabon. | The findings proved that getting women to enroll in health insurance is a major strategy to improve the utilization of some important maternal health services, which include adequate ANC visits, delivery at health facilities, as well as attending postnatal care clinic. Generally, the findings of this study point to the fact that there is a significant increment in the use of standards recommended for adequate maternal healthcare which can be attributable to coverage of health insurance. | Cross-sectional study | Gabon |
| Mwase, 2018 [38] | Poor women who had completed a pregnancy in the 24 months prior to the survey date. | Inequities in access to and utilization of maternal care. | To assess the magnitude of the inequities and their determinants in coverage of maternal health services in Burkina Faso. | The study shows that existing inequities in maternal health services in Burkina Faso are likely going to jeopardize the achievement of Universal Health Coverage. It is important that policy makers continue to strengthen and monitor the implementation of strategies that promote proportionate universalism and forge multi-sectoral approach in dealing with social determinants of inequities in maternal health services coverage. | Cross-sectional study | Burkina Faso |
| Abiiro, 2014 [39] | Community residents. | Free access to an essential health package (EHP). | To explore how rural communities experience and define gaps in universal health coverage in Malawi, a country which endorses free access to an essential health package (EHP) as a means toward universal health coverage. | The study findings show that moving toward UHC in Malawi implies the introduction of appropriate interventions to fill the financial protection gaps in the private sector and the access-related gaps in the public sector and/or an effective public-private partnership that completely integrates both sectors. | Cross-sectional study | Malawi |
| Suchman, 2020 [40] | Exiting patients at health facilities. | Social health insurance. | To examine how social health insurance affects patient decision making regarding when and where to seek care in Kenya and Ghana. | The study shows that clients and providers would benefit from education on what is included in the SHI package. Providers should be monitored and held accountable for charging clients inappropriately; in Ghana, this should be accompanied by reforms to make government financing for SHI sustainable. Since clients value provider proximity and both Kenya and Ghana have a dearth of providers in rural areas, both countries should incentivize providers to work in these areas and prioritize accrediting rural facilities into SHI schemes to increase accessibility and reach. | Cross-sectional study | Kenya and Ghana |
| Knoblauch, 2019 [41] | Governments, implementers, drone providers, and funders of healthcare. | The use of bi-directional transport drones for health systems. | To perform a SWOT analysis (strengths, weaknesses, opportunities, and threats) use of bi-directional transport drones for health systems in sub-Saharan Africa. | Governments should also employ a system-strengthening approach to identify health system bottlenecks and explore new areas for supply chain optimization and cost-effectiveness using drones. After approximately 3 years of implementation of several proof-of-concept drone projects, the technology is still in its feasibility phase for many use cases. To this date, projects have yet to produce enough data to demonstrate a direct or indirect impact on health outcomes. | Case study | Madagascar, Malawi, and Senegal |
| Matthews, 2019 [42] | Health system governance and community health worker programs. | Strengthening the evidence ecosystem (using evidence to strengthen health system governance and support for community health worker programs; managing the growing epidemic of drug-resistant tuberculosis; social protection; the child support grant and its impact on health). | To apply an evidence ecosystem lens to the SA health system, and discuss its current functioning in support of the achievement of a high-quality health system that is able to achieve universal health coverage. | The evidence ecosystem model for health systems illustrates how evidence needs to be transferred between different key stages to strengthen health systems and inform care. It shows the importance of “closing the loop” between evidence producers, synthesizers, and disseminators and users. | Case study | South Africa |
| Miot, 2017 [43] | Public and private sector. | Optimization of pharmacoeconomics as a steering tool under the universal health coverage. | To explore factors that determine the introduction of pharmacoeconomics into health systems’ regulatory frameworks. Simultaneously, it seeks to provide guidance on processes for the design, implementation, and optimization of pharmacoeconomics as a steering tool within a health system under the UHC paradigm. | In the public sector, the process for selection of medicines onto the Essential Medicines List (EML) allows for the use of pharmacoeconomics to assess the cost-effectiveness of proposed additions to the list. This has developed over time, however, with earlier editions of the EML only considering clinical evidence and some costing. Even in the current environment, full pharmacoeconomic analysis is lacking in areas. | Case study | South Africa |
| Van Der Heever, 2012 [44] | Private health systems. | Health insurance. | To examine whether private health systems are susceptible to regulation and therefore able to support an extension and deepening of coverage when complementing a pre-existing publicly funded and delivered health system. | The private health system in South Africa has played an important supplementary role in achieving universal coverage throughout its history, but more especially in the post-Apartheid period. However, the quality of this role has been erratic, influenced predominantly by policy vacillation.The private system expanded rapidly during the 1980s mainly due to the pre-existence of a mature health insurance system and a weakening public hospital system that could accommodate and facilitate an increased demand for private hospital services. | Case study | South Africa |
| Mbogo, 2016 [45] | Males and females aged 23 to 59 years. | Financing population-based healthcare interventions. | To explore perspectives on employed individuals regarding financing population-based healthcare interventions toward UHC to make recommendations to the Ministry of Health on health financing options to cover population-based health services. | The study highlights that increasing enrolment in health coverage schemes requires targeted campaign for information dissemination through use of myriads mass media including: social networks, TV, radio and others. Moreover, re-designing health insurance schemes is critical in order to include population-based interventions and expand uptake of unemployed and informal sector employees; flexibility in monthly premiums payment plan; and use of technology to increase access to payment points. | Qualitative study | Botswana |
| Onarheim, 2018 [46] | Household members, health workers, and community members. | Intra-household resource allocation, focusing on how families prioritize newborn health and household needs in Ethiopia. | To explore intra-household resource allocation, focusing on how families prioritize new born health versus other household needs and their coping strategies for managing these priorities. | The study highlights that while improving neonatal health is prioritized at policy level in Ethiopia, poor households with sick neonates may prioritize differently. With limited money at hand and high direct health care costs, families balanced conflicting concerns to newborn health and family welfare. We argue that families should not be left in situations where they have to choose between survival of the newborn and economic ruin. Protection against out-of-pocket spending is key as Ethiopia moves toward universal health coverage. A necessary step is to provide prioritized newborn health care services free of charge. | Qualitative study | Ethiopia |
| Lu, 2012 [47] | Enrollees’ medical care utilization. | Health financing through Mutuelles community-based health insurance program. | To evaluate the impact of Mutuelles on achieving universal coverage of medical services and financial risk protection in its first eight years of implementation. | The findings show that Mutuelles improved medical care utilization and protected households from catastrophic health spending. | Quantitative | Rwanda |
| Mills, 2012 [48] | Households. | Healthcare financing. | To present a body of research whose overall aim was to critically evaluate existing inequities in health care financing and provision in Ghana, South Africa and Tanzania, and the extent to which health insurance mechanisms (broadly defined) could address financial protection and equity of access challenges. | Direct taxes were progressive in all three countries. Indirect taxes were regressive in South Africa but progressive in Ghana and Tanzania. Out-of-pocket payments were regressive and overall healthcare financing was progressive in all three countries. All forms of indirect tax (value-added tax (VAT), fuel levies, and excise duties) were regressive in South Africa. By contrast, VAT and excise and import duties were all progressive in Tanzania. | Qualitative study | Ghana, South Africa, and Tanzania |
| Foster, 2018 [49] | Nurse facility heads and district nurse supervisors. | Improving leadership capacity and management skills of facility heads. | To design and test a 12-month blended learning program for a certificate in leadership and management practice to build leadership and management competencies of rural facility heads, including increasing their ability to lead frontline teams and strengthening their skills and confidence in technology use. | Findings suggested that the facility heads had successfully strengthened their leadership and management competencies, increased their ability to lead frontline teams, and strengthened their skills and confidence in use of technology, including using a WhatsApp community of practice for support and consultation with other colleagues, with demonstrated improvements in the quality and accessibility of services. | Qualitative and quantitative study | Zambia |
| Country | Number of UHC Studies | References |
|---|---|---|
| Nigeria | 6 studies | [17,18,26,29,34,50] |
| Ethiopia | 5 studies | [21,32,33,35,46] |
| South Africa | 5 studies | [26,42,43,44,48] |
| Tanzania | 5 studies | [19,22,26,27,48] |
| Ghana | 4 studies | [26,40,48,51] |
| Malawi | 3 studies | [25,39,41] |
| Rwanda | 3 studies | [26,32,47] |
| Kenya | 2 studies | [36,40] |
| Senegal | 2 studies | [24,41] |
| Zambia | 2 studies | [32,49] |
| Algeria | 1 study | [26] |
| Botswana | 1 study | [45] |
| Burkina Faso | 1 study | [38] |
| Egypt | 1 study | [31] |
| Democratic Republic of Congo | 1 study | [20] |
| Gabon | 1 study | [37] |
| Madagascar | 1 study | [41] |
| Seychelles | 1 study | [30] |
| Zimbabwe | 1 study | [28] |
| 47 countries in the WHO African region | 1 study | [23] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jaca, A.; Malinga, T.; Iwu-Jaja, C.J.; Nnaji, C.A.; Okeibunor, J.C.; Kamuya, D.; Wiysonge, C.S. Strengthening the Health System as a Strategy to Achieving a Universal Health Coverage in Underprivileged Communities in Africa: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 587. https://doi.org/10.3390/ijerph19010587
Jaca A, Malinga T, Iwu-Jaja CJ, Nnaji CA, Okeibunor JC, Kamuya D, Wiysonge CS. Strengthening the Health System as a Strategy to Achieving a Universal Health Coverage in Underprivileged Communities in Africa: A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(1):587. https://doi.org/10.3390/ijerph19010587
Chicago/Turabian StyleJaca, Anelisa, Thobile Malinga, Chinwe Juliana Iwu-Jaja, Chukwudi Arnest Nnaji, Joseph Chukwudi Okeibunor, Dorcas Kamuya, and Charles Shey Wiysonge. 2022. "Strengthening the Health System as a Strategy to Achieving a Universal Health Coverage in Underprivileged Communities in Africa: A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 1: 587. https://doi.org/10.3390/ijerph19010587
APA StyleJaca, A., Malinga, T., Iwu-Jaja, C. J., Nnaji, C. A., Okeibunor, J. C., Kamuya, D., & Wiysonge, C. S. (2022). Strengthening the Health System as a Strategy to Achieving a Universal Health Coverage in Underprivileged Communities in Africa: A Scoping Review. International Journal of Environmental Research and Public Health, 19(1), 587. https://doi.org/10.3390/ijerph19010587