
Community Mobility and COVID-19 Dynamics in Jakarta, Indonesia

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data on Cases of COVID-19
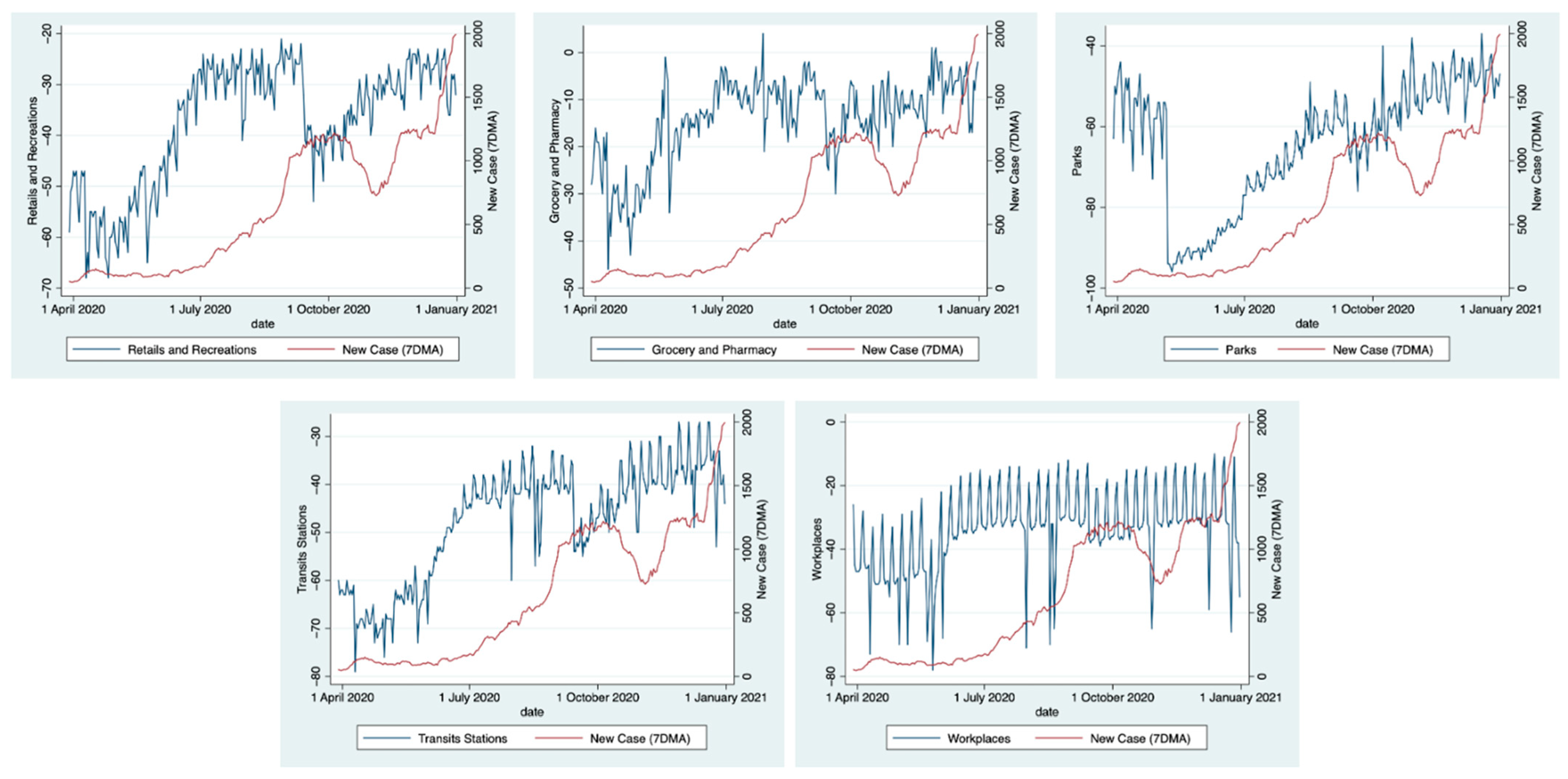
2.2. Data on Community Mobility
- -
- Retail and Recreational: mobility towards places such as restaurants, cafes, shopping centers, museums, libraries, and picture theatres;
- -
- Grocery and Pharmacy: mobility trends for places such as grocery shops, food warehouses, markets, local hats, farmer’s markets, specialty food shops, different drug or medicine stores, and pharmacies;
- -
- Parks: places of attraction including local parks, national parks, public beaches, marinas, dog parks, plazas, and public gardens;
- -
- Transit stations: a process by which a person moves from one place to places like public transport hubs such as subway, bus, and train stations;
- -
- Workplaces: the process of going to places of work from a home;
- -
- Residential mobility: mobility in the direction of places of residence where a person lived.
2.3. Variable Selection
3. Results
COVID-19 Cases and Containment in Jakarta
4. Discussion
4.1. Effect of Mobility by Categories on COVID-19 Dynamics
4.2. Mobility Relaxation, Seasonal Events, and COVID-19 Dynamics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- John Hopkins University. CSSE Coronavirus COVID-19 Global Cases (Dashboard). Available online: https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6 (accessed on 15 January 2022).
- Zhang, S.; Wang, Z.; Chang, R.; Wang, H.; Xu, C.; Yu, X.; Tsamlag, L.; Dong, Y.; Wang, H.; Cai, Y. COVID-19 containment: China provides important lessons for global response. Front. Med. 2020, 14, 215–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varghese, C.; Xu, W. Quantifying what could have been—The impact of the Australian and New Zealand governments’ response to COVID-19. Infect. Dis. Health 2020, 25, 242–244. [Google Scholar] [CrossRef] [PubMed]
- Bajardi, P.; Poletto, C.; Ramasco, J.J.; Tizzoni, M.; Colizza, V.; Vespignani, A. Human Mobility Networks, Travel Restrictions, and the Global Spread of 2009 H1N1 Pandemic. PLoS ONE 2011, 6, e16591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, F.; Ge, X.; Huang, D. Government Intervention, Human Mobility, and COVID-19: A Causal Pathway Analysis from 121 Countries. Sustainability 2022, 14, 3694. [Google Scholar] [CrossRef]
- Oliver, N.; Letouzé, E.; Sterly, H.; Delataille, S.; De Nadai, M.; Lepri, B.; Lambiotte, R.; Benjamins, R.; Cattuto, C.; Colizza, V. Mobile phone data and COVID-19: Missing an opportunity? arXiv 2020, arXiv:200312347. [Google Scholar]
- Badr, H.S.; Du, H.; Marshall, M.; Dong, E.; Squire, M.M.; Gardner, L.M. Association between mobility patterns and COVID-19 transmission in the USA: A mathematical modelling study. Lancet Infect. Dis. 2020, 20, 1247–1254. [Google Scholar] [CrossRef]
- Asweto, C.O.; Onyango, P.O.; Alzain, M.A.; Wang, W. Effects of Increased Residential Mobility and Reduced Public Spaces Mobility in Containing COVID-19 in Africa. J. Glob. Health Rep. 2020, 4, e2020075. [Google Scholar] [CrossRef]
- Sulyok, M.; Walker, M. Community movement and COVID-19: A global study using Google’s Community Mobility Reports. Epidemiol. Infect. 2020, 148, e284. [Google Scholar] [CrossRef]
- Wang, H.Y.; Yamamoto, N. Using a partial differential equation with Google Mobility data to predict COVID-19 in Arizona. Math. Biosci. Eng. 2020, 17, 4891–4904. [Google Scholar] [CrossRef]
- Pérez-Arnal, R.; Conesa, D.; Alvarez-Napagao, S.; Suzumura, T.; Català, M.; Alvarez-Lacalle, E.; Garcia-Gasulla, D. Comparative Analysis of Geolocation Information through Mobile-Devices under Different COVID-19 Mobility Restriction Patterns in Spain. ISPRS Int. J. Geo-Inf. 2021, 10, 73. [Google Scholar] [CrossRef]
- Czech, K.; Davy, A.; Wielechowski, M. Does the COVID-19 Pandemic Change Human Mobility Equally Worldwide? Cross-Country Cluster Analysis. Economies 2021, 9, 182. [Google Scholar] [CrossRef]
- Hanggara, A.G. Jakarta Response to COVID-19 Outbreak: A Timeline. 2020. Available online: https://corona.jakarta.go.id/en/artikel/linimasa-kebijakan-penanganan-pandemi-covid-19-di-jakarta (accessed on 27 January 2021).
- KawalCOVID19: Grafik Interaktif untuk Data per Provinsi. 2020. Available online: https://kawalcovid19.id/ (accessed on 15 January 2021).
- Google LLC. Google COVID-19 Community Mobility Report. 2020. Available online: https://www.google.com/covid19/mobility/ (accessed on 15 January 2021).
- Cot, C.; Cacciapaglia, G.; Sannino, F. Mining Google and Apple mobility data: Temporal anatomy for COVID-19 social distancing. Sci. Rep. 2021, 11, 4150. [Google Scholar] [CrossRef] [PubMed]
- Mahendradhata, Y.; Marthias, T.; Andayani, N.L. COVID-19 Health System Response Monitor. Center for Health Policy and Management, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada. 2021. Available online: https://apps.who.int/iris/rest/bitstreams/1369903/retrieve (accessed on 14 May 2022).
- Suni, N.S. Indonesia’s Preparedness in Dealing with The Potential Spread of Corona Virus Disease. Social Welfare Division 2020, XII(3). Available online: http://berkas.dpr.go.id/puslit/files/info_singkat/Info%20Singkat-XII-3-I-P3DI-Februari-2020-1957-EN.pdf (accessed on 14 May 2022).
- Kim, H.Y. Statistical notes for clinical researchers: Assessing normal distribution (2) using skewness and kurtosis. Restor. Dent. Endod. 2013, 38, 52–54. [Google Scholar] [CrossRef] [PubMed]
- Hammouri, H.M.; Sabo, R.T.; Alsaadawi, R.; Kheirallah, K.A. Handling Skewed Data: A Comparison of Two Popular Methods. Appl. Sci. 2020, 10, 6247. [Google Scholar] [CrossRef]
- Curran-Everett, D. Explorations in statistics: The log transformation. Adv. Physiol. Educ. 2018, 42, 343–347. [Google Scholar] [CrossRef]
- Praharaj, S.; Han, H. A longitudinal study of the impact of human mobility on the incidence of COVID-19 in India. medRxiv 2020. [Google Scholar] [CrossRef]
- Goolsbee, A.; Syverson, C. Fear, lockdown, and diversion: Comparing drivers of pandemic economic decline 2020. J. Public Econ. 2021, 193, 104311. [Google Scholar] [CrossRef]
- Detikcom. Ada 107 Klaster Pasar Jakarta, 555 Orang Positif Corona. detikNews. 2020. Available online: https://news.detik.com/berita/d-5112322/ada-107-klaster-pasar-jakarta-555-orang-positif-corona/ (accessed on 12 April 2021).
- Manurung, H. COVID-19 in Indonesia: Problems and Challenges Facing New Transmission in Traditional Markets. 2020. Available online: https://www.researchgate.net/publication/342210867_COVID-19_in_Indonesia_Problems_and_Challenges_Facing_New_Transmission_in_Traditional_Markets (accessed on 17 April 2021).
- Nugraheny, D.E. Bukan Klaster Perkantoran, Ini Penyumbang Tingginya Kasus COVID-19 di DKI Versi Satgas. 2020. Available online: https://nasional.kompas.com/read/2020/07/29/11455941/bukan-klaster-perkantoran-ini-penyumbang-tingginya-kasus-covid-19-di-dki (accessed on 27 April 2021).
- Simanjuntak, D.R.; Napitupulu, T.M.; Wele, A.M.; Yanie, R. Gambaran Kepatuhan Masyarakat Menerapkan Protokol Kesehatan COVID-19 di Tempat Umum Periode September 2020 di DKI Jakarta. 2020. Available online: http://repository.uki.ac.id/id/eprint/3191 (accessed on 10 May 2021).
- Nishiura, H.; Oshitani, H.; Kobayashi, T.; Saito, T.; Sunagawa, T.; Matsui, T.; Wakita, T.; MHLW COVID Response Team; Suzuki, M. Closed environments facilitate secondary transmission of coronavirus disease 2019 (COVID-19). medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Noorimotlagh, Z.; Jaafarzadeh, N.; Martínez, S.S.; Mirzaee, S.A. A systematic review of possible airborne transmission of the COVID-19 virus (SARS-CoV-2) in the indoor air environment. Environ. Res. 2021, 193, 110612. [Google Scholar] [CrossRef]
- Musselwhite, C.; Avineri, E.; Susilo, Y. Editorial JTH 16—The Coronavirus Disease COVID-19 and implications for transport and health. J. Transp. Health 2020, 16, 100853. [Google Scholar] [CrossRef]
- BPS: Perilaku Masyarakat Di Masa Pandemi COVID-19. Badan Pusat Statistik. 2020. Available online: https://www.bps.go.id/publication/2020/09/28/f376dc33cfcdeec4a514f09c/perilaku-masyarakat-di-masa-pandemi-covid-19.html (accessed on 10 May 2021).
- National COVID-19 Task Force. Kepatuhan Masyarakat Terhadap Protokol Kesehatan Harus Ditingkatkan. 2020. Available online: https://covid19.go.id/p/berita/kepatuhan-masyarakat-terhadap-protokol-kesehatan-harus-ditingkatkan (accessed on 17 April 2021).
- Xiong, C.; Hu, S.; Yang, M.; Luo, W.; Zhang, L. Mobile device data reveal the dynamics in a positive relationship between human mobility and COVID-19 infections. Proc. Natl. Acad. Sci. USA 2020, 117, 27087–27089. [Google Scholar] [CrossRef] [PubMed]
- Peltzman, S. The Effects of Automobile Safety Regulation. J. Political Econ. 1975, 83, 677–725. [Google Scholar] [CrossRef]
- Mantzari, E.; Rubin, G.J.; Marteau, T.M. Is risk compensation threatening public health in the COVID-19 pandemic? BMJ 2020, 370, m2913. [Google Scholar] [CrossRef] [PubMed]
- Gatalo, O.; Tseng, K.; Hamilton, A.; Lin, G.; Klein, E. Associations between phone mobility data and COVID-19 cases. Lancet Infect. Dis. 2021, 21, e111. [Google Scholar] [CrossRef]
- Chinazzi, M.; Davis, J.T.; Ajelli, M.; Gioannini, C.; Litvinova, M.; Merler, S.; Pastore, Y.P.A.; Mu, K.; Rossi, L.; Sun, K.; et al. The effect of travel restrictions on the spread of the 2019 novel coronavirus (COVID-19) outbreak. Science 2020, 368, 395–400. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.; Kim, Y.J.; Peck, K.R.; Ko, Y.; Lee, J.; Jung, E. Keeping Low Reproductive Number Despite the Rebound Population Mobility in Korea, a Country Never under Lockdown during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 9551. [Google Scholar] [CrossRef]
- Nouvellet, P.; Bhatia, S.; Cori, A.; Ainslie, K.E.C.; Baguelin, M.; Bhatt, S.; Boonyasiri, A.; Brazeau, N.F.; Cattarino, L.; Cooper, L.V.; et al. Reduction in mobility and COVID-19 transmission. Nat. Commun. 2021, 12, 1090. [Google Scholar] [CrossRef]
- Drake, J.M.; Chew, S.K.; Ma, S. Societal learning in epidemics: Intervention effectiveness during the 2003 SARS outbreak in Singapore. PLoS ONE 2006, 1, e20. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Lags | AIC | RMSE | R2 |
|---|---|---|---|
| 7 days | 757.02 | 0.92 | 0.28 |
| 14 days | 793.28 | 0.98 | 0.18 |
| Variables | Coefficient | Std. Error | p > |t| | [95% CI] |
|---|---|---|---|---|
| Cons. | 10.25 | 0.21 | 0.00 | (9.84, 10.67) |
| Retail and recreation | −0.01 | 0.01 | 0.08 | (−0.03, 0.00) |
| Grocery and Pharmacies | −0.04 | 0.01 | 0.00 | (−0.06, −0.01) |
| Parks | 0.00 | 0.00 | 0.15 | (−0.00, 0.01) |
| Transits Stations | 0.14 | 0.01 | 0.00 | (0.11, 0.16) |
| Workplaces | −0.04 | 0.01 | 0.00 | (−0.05, −0.33) |
| Model | AIC | RMSE | ||||
|---|---|---|---|---|---|---|
| Pois | NB | MLR | Pois | NB | MLR | |
| 1. Parks_Retails | 3.75 | 5.73 | 2.33 | 0.78 | 0.78 | 0.77 |
| 2. Parks_Retails _Grocery | 3.76 | 5.74 | 2.34 | 0.78 | 0.78 | 0.77 |
| 3. Parks_Retails_Transits | 3.74 | 5.74 | 2.15 | 0.71 | 0.71 | 0.70 |
| 4. Parks_Retails_Workplaces | 3.76 | 5.74 | 2.31 | 0.77 | 0.77 | 0.76 |
| 5. Parks_Retails_Z-Score Grocery_Transits_Workplaces | 3.76 | 5.74 | 2.29 | 0.76 | 0.76 | 0.76 |
| Variables | Coef. | Std. Err. | p > |t| | 95% CI |
|---|---|---|---|---|
| Cons. | 8.44 | 0.28 | 0.00 | (7.88, 9.00) |
| Z_Score_Grocery_Transits_Workplaces (Lagged 7 days) | 0.41 | 0.12 | 0.00 | (0.18, 0.65) |
| Parks (Lagged 7 days) | 0.02 | 0.00 | 0.00 | (0.01, 0.02) |
| Retail and recreation (Lagged 7 days) | 0.03 | 0.00 | 0.00 | (0.01, 0.45) |
| Variable | Coef. (Exp) | Coef. (%) | Mean | Std. Dev | 95% Confidence Interval (Exp) |
|---|---|---|---|---|---|
| Grocery and pharmacy | 1.04 | 4.12 | −12.30 | 10.34 | (1.01, 1.06) |
| Transits stations | 1.02 | 2.26 | −42.98 | 18.64 | (1.00, 1.03) |
| Workplaces | 1.02 | 2.56 | 30.01 | 16.54 | (1.01, 1.04) |
| Parks | 1.01 | 1.93 | −57.22 | 24.02 | (1.01, 1.02) |
| Retails and recreation | 1.03 | 3.11 | −34.03 | 16.03 | (1.01, 1.04) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nanda, R.O.; Nursetyo, A.A.; Ramadona, A.L.; Imron, M.A.; Fuad, A.; Setyawan, A.; Ahmad, R.A. Community Mobility and COVID-19 Dynamics in Jakarta, Indonesia. Int. J. Environ. Res. Public Health 2022, 19, 6671. https://doi.org/10.3390/ijerph19116671
Nanda RO, Nursetyo AA, Ramadona AL, Imron MA, Fuad A, Setyawan A, Ahmad RA. Community Mobility and COVID-19 Dynamics in Jakarta, Indonesia. International Journal of Environmental Research and Public Health. 2022; 19(11):6671. https://doi.org/10.3390/ijerph19116671
Chicago/Turabian StyleNanda, Ratih Oktri, Aldilas Achmad Nursetyo, Aditya Lia Ramadona, Muhammad Ali Imron, Anis Fuad, Althaf Setyawan, and Riris Andono Ahmad. 2022. "Community Mobility and COVID-19 Dynamics in Jakarta, Indonesia" International Journal of Environmental Research and Public Health 19, no. 11: 6671. https://doi.org/10.3390/ijerph19116671
APA StyleNanda, R. O., Nursetyo, A. A., Ramadona, A. L., Imron, M. A., Fuad, A., Setyawan, A., & Ahmad, R. A. (2022). Community Mobility and COVID-19 Dynamics in Jakarta, Indonesia. International Journal of Environmental Research and Public Health, 19(11), 6671. https://doi.org/10.3390/ijerph19116671