
A Community-Based Participatory Action Research with Women from Disadvantaged Populations: Strengths and Weaknesses of a Multiple Health Behaviour Change Intervention

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
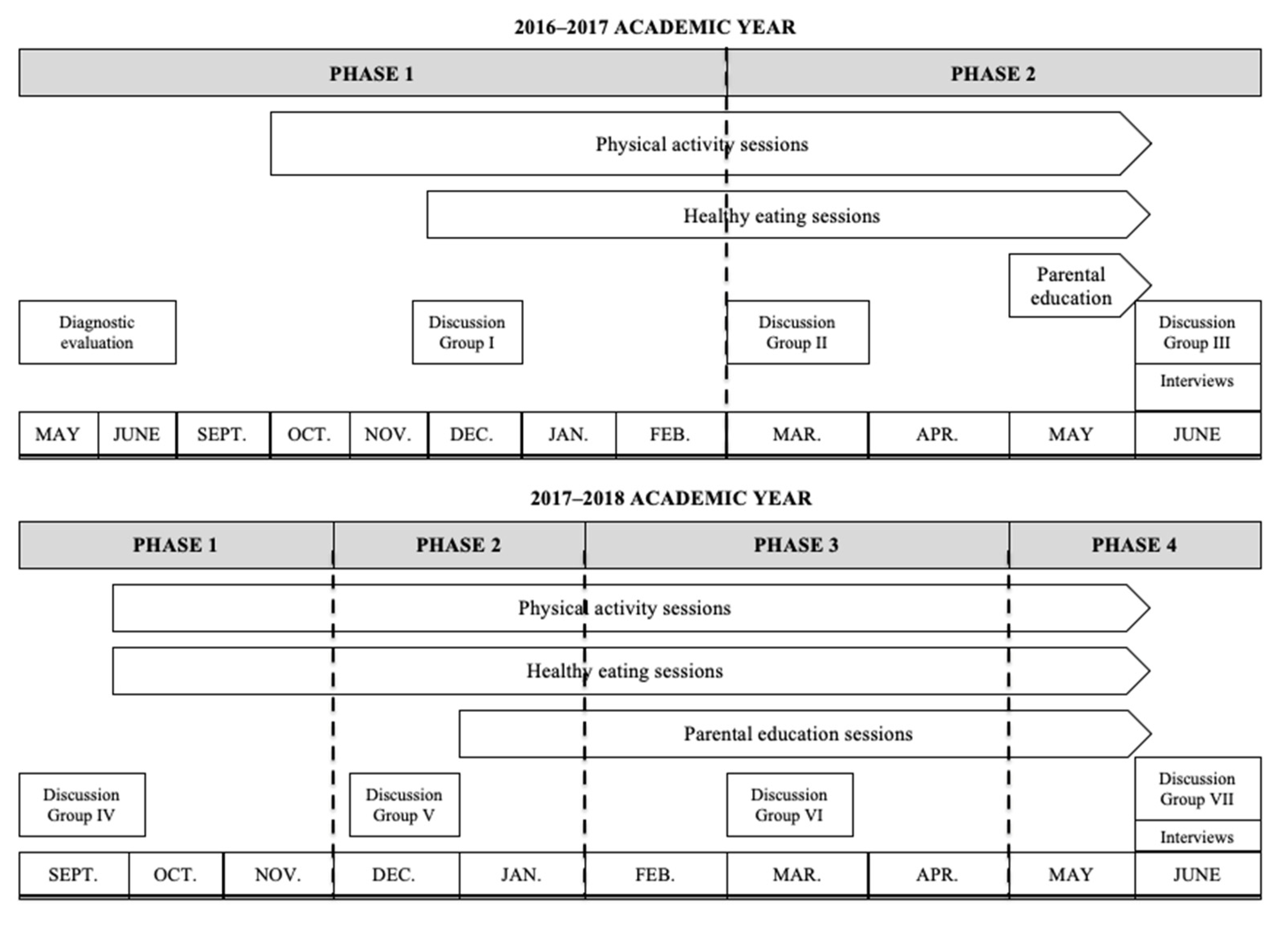
2.1. Study Design and Contextualisation
2.2. Participants and Recruitment
2.3. The ‘Pío Keeps Moving’ Intervention Programme
2.3.1. Physical Activity Sessions
2.3.2. Healthy Eating Sessions
2.4. Data Collection
2.5. Data Analysis
3. Results and Discussion
3.1. Strengths of the Intervention Programme
“Well, you’ve been very patient with us and you’ve been there for us. For example, you’ve not been discouraged when only a few people came; you have carried on and [told us], come on! Don’t worry, come on! You’ve fought”.(Participant 5)
“…You’ve woken up the gymnasts we had inside, because if it were up to us, we restrict ourselves a lot”.(Participant 7)
“For me, PA has been very enjoyable”.(Participant 8)
“It’s given me more confidence in myself, and then, of course, the affection and companionship that we have established”.(Participant 1)
“The variety of activities we’ve done. Because, as I’ve said before, if it’s always the same, it’s boring; the time comes when you get bored. But, this year, there’ve been more activities than last year”.(Participant 1)
“Me, for example, well it’s the group that’s been formed; do you know what I mean? The friendship that’s been formed. That’s been great”.(Participant 2)
3.2. Weaknesses of the Intervention Programme
“The fact that they’ve not attended the last few days, and I didn’t know [they hadn’t come]. Everything else has been fine”.(Participant 7)
“That the group has disappeared”.(Participant 1)
“The schedule, because, for example, when I sorted things out to be able to come at midday, it wasn’t possible, because it was held in the mornings. And then, it couldn’t be changed because of those who came in the mornings; but of course, they’re not going to change just for me, for one person. The rest was OK (…) The schedule”.(Participant 5)
“More negative points… I don’t know… the schedule… I don’t know”.(Participant 7)
4. Practical Implications for Future Interventions in Disadvantaged Populations
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Fundación FOESSA. VI Informe Sobre Exclusión y Desarrollo Social en España; Cáritas Española Editores: Madrid, España, 2008. [Google Scholar]
- La Parra-Casado, D.; Gil González, D.; de la Torre Esteve, M. The social class gradient in health in Spain and the health status of the Spanish Roma. Ethn. Health 2015, 21, 468–479. [Google Scholar] [CrossRef]
- Fernández-Feito, A.; Pesquera-Cabezas, R.; González-Cobo, C.; Prieto-Salceda, M.D. What do we know about the health of Spanish Roma people and what has been done to improve it? A scoping review. Ethn. Health 2017, 24, 224–243. [Google Scholar] [CrossRef]
- Carrasco-Garrido, P.; López De Andrés, A.; Hernández Barrera, V.; Jiménez-Trujillo, I.; Jiménez-García, R. Health status of Roma women in Spain. Eur. J. Public Health 2010, 21, 793–798. [Google Scholar] [CrossRef]
- Laparra Navarro, M. Diagnóstico Social de la Comunidad Gitana en España. Un Análisis Contrastado de la de la Encuesta del CIS a Hogares de Población Gitana 2007; Ministry of Health, Social Policy and Equality: Madrid, Spain, 2011. [Google Scholar]
- Cook, B.; Ferris Wayne, G.; Valentine, A.; Lessios, A.; Yeh, E. Revisiting the evidence on health and health care disparities among the Roma: A systematic review 2003–2012. Int. J. Public Health 2013, 58, 885–911. [Google Scholar] [CrossRef]
- O’Donoghue, G.; Perchoux, C.; Mensah, K.; Lakerveld, J.; Van Der Ploeg, H.; Bernaards, C.; Chastin, S.F.M.; Simon, C.; O’Gorman, D.; Nazare, J.A. A systematic review of correlates of sedentary behaviour in adults aged 18–65 years: A socio-ecological approach. BMC Public Health 2016, 16, 163. [Google Scholar] [CrossRef] [Green Version]
- Galobardes, B.; Shaw, M.; Lawlor, D.A.; Lynch, J.W.; Smith, G.D. Indicators of socioeconomic position (part 1). J. Epidemiol. Community Health 2006, 60, 7–12. [Google Scholar] [CrossRef] [Green Version]
- van Lenthe, F.J.; Kamphuis, C.B.; Beenackers, M.A.; Jansen, T.; Looman, C.W.; Nusselder, W.J.; Mackenbach, J.P. Cohort Profile: Understanding socioeconomic inequalities in health and health behaviours: The GLOBE study. Int. J. Epidemiol. 2014, 43, 721–730. [Google Scholar] [CrossRef] [Green Version]
- Cleland, C.L.; Tully, M.A.; Kee, F.; Cupples, M.E. The effectiveness of physical activity interventions in socio-economically disadvantaged communities: A systematic review. Prev. Med. 2012, 54, 371–380. [Google Scholar] [CrossRef]
- Cleland, V.; Granados, A.; Crawford, D.; Winzenberg, T.; Ball, K. Effectiveness of interventions to promote physical activity among socioeconomically disadvantaged women: A systematic review and meta-analysis. Obes. Rev. 2013, 14, 197–212. [Google Scholar] [CrossRef] [Green Version]
- Darmon, N.; Drewnowski, A. Does social class predict diet quality? Am. J. Clin. Nutr. 2008, 87, 1107–1117. [Google Scholar] [CrossRef] [Green Version]
- Demarest, S.; Van Oyen, H.; Roskam, A.-J.; Cox, B.; Regidor, E.; Mackenbach, J.P.; Kunst, A.E. Educational inequalities in leisure-time physical activity in 15 European countries. Eur. J. Public Health 2013, 24, 119–204. [Google Scholar] [CrossRef] [Green Version]
- Gidlow, C.; Johnston, L.H.; Crone, D.; Ellis, N.; James, D. A systematic review of the relationship between socio-economic position and physical activity. Health Educ. J. 2006, 65, 338–367. [Google Scholar] [CrossRef]
- Ball, K.; Carver, A.; Downing, K.; Jackson, M.; O’Rourke, K. Addressing the social determinants of inequities in physical activity and sedentary behaviours. Health Promot. Int. 2015, 30, ii8–ii19. [Google Scholar] [CrossRef] [Green Version]
- Glover, J.D.; Hetzel, D.M.; Tennant, S.K. The socioeconomic gradient and chronic illness and associated risk factors in Australia. BMC Health Policy 2004, 1, 8. [Google Scholar]
- Sanz-Remacha, M.; García-González, L.; Sevil Serrano, J.; Generelo, G.; Aibar, A. Barriers to physical activity in disadvantaged population: A qualitative comparison between Roma and Non-Roma women. Res. Q. Exerc. Sport 2019, 90, 567–577. [Google Scholar] [CrossRef]
- Baruth, M.; Sharpe, P.A.; Parra-Medina, D.; Wilcox, S. Perceived barriers to exercise and healthy eating among women from disadvantaged neighborhoods: Results from a focus groups assessment. Women Health 2014, 54, 336–353. [Google Scholar] [CrossRef] [Green Version]
- Craike, M.; Bourke, M.; Hilland, T.A.; Wiesner, G.; Pascoe, M.C.; Bengoechea, E.G.; Parker, A.G. Correlates of Physical Activity Among Disadvantaged Groups: A Systematic Review. Am. J. Prev. Med. 2019, 57, 700–715. [Google Scholar] [CrossRef]
- Craike, M.; Wiesner, G.; Hilland, T.; Bengoechea, E. Interventions to improve physical activity among socioeconomically disadvantaged groups: An umbrella review. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 43. [Google Scholar] [CrossRef]
- NHS Health and Social Care Information Centre. Health Survey for England—2004: Health of Ethnic Minorities. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/health-survey-for-england/health-survey-for-england-2004-health-of-ethnic-minorities-headline-results (accessed on 25 March 2021).
- Wilcox, S.; Sharpe, P.A.; Liese, A.D.; Dunn, C.G.; Hutto, B. Socioeconomic factors associated with diet quality and meeting dietary guidelines in disadvantaged neighborhoods in the Southeast United States. Ethn. Health 2020, 25, 1115–1131. [Google Scholar] [CrossRef]
- Moredich, C.A.; Kessler, T.A. Physical activity and nutritional weight loss interventions in obese, low-income women: An integrative review. J. Midwifery Women’s Health 2014, 59, 380–387. [Google Scholar] [CrossRef]
- Bull, E.R.; McCleary, N.; Li, X.; Dombrowski, S.U.; Dusseldorp, E.; Johnston, M. Interventions to promote healthy eating, physical activity and smoking in low-income groups: A systematic review with meta-analysis of behavior change techniques and delivery/context. Int. J. Behav. Med. 2018, 25, 605–616. [Google Scholar] [CrossRef] [PubMed]
- Everson-Hock, E.S.; Johnson, M.; Jones, R.; Woods, H.B.; Goyder, E.; Payne, N.; Chilcott, J. Community-based dietary and physical activity interventions in low socioeconomic groups in the UK: A mixed methods systematic review. Prev. Med. 2013, 56, 265–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jordan, K.C.; Freeland-Graves, J.H.; Klohe-Lehman, D.M.; Cai, G.; Voruganti, V.S.; Proffitt, J.M.; Nuss, H.J.; Milani, T.J.; Bohman, T.M. A nutrition and physical activity intervention promotes weight loss and enhances diet attitudes in low-income mothers of young children. Nutr. Res. 2008, 28, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Wieland, M.L.; Hanza, M.M.; Weis, J.A.; Meiers, S.J.; Patten, C.A.; Clark, M.M.; Sloan, J.A.; Novotny, P.J.; Njeru, J.W.; Abbenyi, A.; et al. Healthy immigrant families: Randomized controlled trial of a family-based nutrition and physical activity intervention. Am. J. Health Promot. 2018, 32, 473–484. [Google Scholar] [CrossRef]
- Nigg, C.R.; Long, C.R. A systematic review of single health behavior change interventions vs. multiple health behavior change interventions among older adults. TBM 2012, 2, 163–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prochaska, J.J.; Nigg, C.R.; Spring, B.; Velicer, W.F.; Prochaska, J.O. The benefits and challenges of multiple health behavior change in research and in practice. Prev. Med. 2010, 50, 26–29. [Google Scholar] [CrossRef] [Green Version]
- Bull, E.R.; Dombrowski, S.U.; McCleary, N.; Johnston, M. Are interventions for low-income groups effective in changing healthy eating, physical activity and smoking behaviours? A systematic review and meta-analysis. BMJ Open 2014, 4, e006046. [Google Scholar] [CrossRef]
- Mummery, W.K.; Brown, W.J. Whole of community physical activity interventions: Easier said than done. Br. J. Sports Med. 2009, 43, 39–43. [Google Scholar] [CrossRef]
- Prochaska, J.; DiClemente, C. Stage of Change in the Modification of Problem Behaviors; SAGE: Newbury Park, CA, USA, 1992. [Google Scholar]
- Selener, D. Participatory Action Research and Social Change; The Cornell Participatory Action Research Network, Cornell University: Ithaca, NY, USA, 1997; ISBN 997895130X. [Google Scholar]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E.; Michie, S.; et al. The Behavior Change Technique Taxonomy (v1) of 93 Hierarchically Clustered Techniques: Building an International Consensus for the Reporting of Behavior Change Interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Weerts, S.E.; Amoran, A. Pass the Fruits and Vegetables! A Community–University–Industry Partnership Promotes Weight Loss in African American Women. Soc. Public Health Educ. 2011, 12, 252–260. [Google Scholar] [CrossRef]
- Samuel-Hodge, C.D.; Johnston, L.F.; Gizlice, Z.; Garcia, B.A.; Lindsley, S.C.; Bramble, K.P.; Hardy, T.E.; Ammerman, A.S.; Poindexter, P.A.; Will, J.C.; et al. Randomized trial of a behavioral weight loss intervention for low-income women: The weight wise program. Obesity 2009, 17, 1891–1899. [Google Scholar] [CrossRef] [PubMed]
- Faucher, M.A.; Mobley, J. A Community Intervention on Portion Control Aimed at Weight Loss in Low-Income Mexican American Women. J. Midwifery Womens Health 2010, 55, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Goldfinger, J.Z.; Arniella, G.; Wylie-Rosett, J.; Horowitz, C.R. Project HEAL: Peer education leads to weight loss in Harlem. J. Health Care Poor Underserved 2008, 19, 180–192. [Google Scholar] [CrossRef] [PubMed]
- Keyserling, T.C.; Samuel Hodge, C.D.; Jilcott, S.B.; Johnston, L.F.; Garcia, B.A.; Gizlice, Z.; Gross, M.D.; Saviñon, C.E.; Bangdiwala, S.I.; Will, J.C.; et al. Randomized trial of a clinic-based, community-supported, lifestyle intervention to improve physical activity and diet: The North Carolina enhanced WISEWOMAN project. Prev. Med. 2008, 46, 499–510. [Google Scholar] [CrossRef]
- Kwasnicka, D.; Dombrowski, S.U.; White, M.; Sniehotta, F. Theoretical explanations for maintenance of behaviour change: A systematic review of behaviour theories. Health Psychol. Rev. 2016, 10, 277–296. [Google Scholar] [CrossRef]
- Sallis, J.F. Needs and Challenges Related to Multilevel Interventions: Physical Activity Examples. Health Educ. Behav. 2018, 45, 661–667. [Google Scholar] [CrossRef]
- Evans, J.M.M.; Connelly, J.; Jepson, R.; Gray, C.; Shepherd, A.; Mackison, D. A physical activity intervention in a Bingo club: Significance of the setting. Health Educ. J. 2018, 77, 377–384. [Google Scholar] [CrossRef]
- Stasi, S.; Spengler, J.; Maddock, J.; McKyer, L.; Clark, H. Increasing Access to Physical Activity within Low Income and Diverse Communities: A Systematic Review. Am. J. Health Promot. 2019, 33, 089011711983225. [Google Scholar] [CrossRef]
- Fortier, M.S.; Duda, J.L.; Guerin, E.; Teixeira, P.J. Promoting physical activity: Development and testing of self-determination theory-based interventions. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 20. [Google Scholar] [CrossRef] [Green Version]
- Ryan, R.M.; Deci, E.L. Self-Determination Theory: Basic Psychological Needs in Motivation, Development, and Wellness; Guilford Publications: New York, NY, USA, 2017; ISBN 9781462538966. [Google Scholar]
- Miller, L.S.; Gramzow, R.H. A self-determination theory and motivational interviewing intervention to decrease racial/ethnic disparities in physical activity: Rationale and design. BMC Public Health 2016, 16, 768. [Google Scholar] [CrossRef] [Green Version]
- Zhang, T.; Solmon, M. Integrating self-determination theory with the social ecological model to understand students’ physical activity behaviours. Int. Rev. Sport Exerc. Psychol. 2013, 6, 37–41. [Google Scholar] [CrossRef]
- Ntoumanis, N.; Ng, J.Y.Y.; Prestwich, A.; Quested, E. A meta-analysis of Self-Determination Theory-informed intervention studies in the health domain: Effects on motivation, health behavior, physical, and psychological health. Health Psychol. Rev. 2021, 15, 214–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodrigues, F.; Bento, T.; Cid, L.; Pereira Neiva, H.; Teixeira, D.; Moutão, J.; Almeida Marinho, D.; Monteiro, D. Can interpersonal behavior influence the persistence and adherence to physical exercise practice in adults? A systematic review. Front. Psychol. 2018, 9, 2141. [Google Scholar] [CrossRef]
- Miranda, D.E.; Garcia-Ramirez, M.; Balcazar, F.E.; Suarez-Balcazar, Y. A community-based participatory action research for Roma health justice in a deprived district in Spain. Int. J. Environ. Res. Public Health 2019, 16, 3722. [Google Scholar] [CrossRef] [Green Version]
- Wallerstein, N.; Duran, B. Community-based participatory research contributions to intervention research: The intersection of science and practice to improve health equity. Am. J. Public Health 2010, 100, 40–46. [Google Scholar] [CrossRef]
- Draper, C.E.; Grobler, L.; Micklesfield, L.K.; Norris, S.A. Impact of social norms and social support on diet, physical activity and sedentary behaviour of adolescents: A scoping review. Child Care Health Dev. 2015, 41, 654–667. [Google Scholar] [CrossRef]
- Teychenne, M.; Ball, K.; Salmon, J. Promoting physical activity and reducing sedentary behavior in disadvantaged neighborhoods: A qualitative study of what women want. PLoS ONE 2012, 7, e49583. [Google Scholar] [CrossRef]
- Griffin, J.B.; Struempler, B.; Funderburk, K.; Parmer, S.M.; Tran, C.; Wadsworth, D.D. My Quest, an Intervention using text messaging to improve dietary and physical activity behaviors and promote weight loss in low-income women. J. Nutr. Educ. Behav. 2018, 50, 11–18. [Google Scholar] [CrossRef] [Green Version]
- St. George, S.M.; Wilson, D.K.; Van Horn, M.L. Project SHINE: Effects of a randomized family-based health promotion program on the physical activity of African American parents. J. Behav. Med. 2018, 41, 537–549. [Google Scholar] [CrossRef]
- Bernal, G.; Sáez-Santiago, E. Culturally centered psychosocial interventions. J. Community Psychol. 2006, 34, 121–132. [Google Scholar] [CrossRef]
- Murillo Pardo, B.; García Bengoechea, E.; Lanaspa, E.G.; Bush, P.L.; Casterad, J.Z.; Clemente, J.A.J.; García González, L. Promising school-based strategies and intervention guidelines to increase physical activity of adolescents. Health Educ. Res. 2013, 28, 523–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baum, F.; MacDougall, C.; Smith, D. Participatory action research. J. Epidemiol. Community Health 2006, 60, 854–857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bazeley, P.; Jackson, K. Qualitative Data Analysis with NVivo, 2nd ed.; Seaman, J., Ed.; SAGE Publications: Southern Oaks, CA, USA, 2013; ISBN 9781446281413. [Google Scholar]
- Shenton, A.K. Strategies for ensuring trustworthiness in qualitative research projects. Educ. Inf. 2004, 22, 63–75. [Google Scholar] [CrossRef] [Green Version]
- Portacio, F.G.; Botero, P.; St. George, S.M.; Stoutenberg, M. Informing the adaptation and implementation of a lifestyle modification program in Hispanics: A qualitative study among low-income hispanic adults. Hisp. Health Care Int. 2018, 16, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, P.J.; Carraça, E.V.; Markland, D.; Silva, M.N.; Ryan, R.M. Exercise, physical activity, and self-determination theory: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prestwich, A.; Sniehotta, F.F.; Whittington, C.; Dombrowski, S.U.; Rogers, L.; Michie, S. Does theory influence the effectiveness of health behavior interventions? Meta-analysis. Health Psychol. 2014, 33, 465–474. [Google Scholar] [CrossRef]
- Bagheri, L.; Milyavskaya, M. Novelty–variety as a candidate basic psychological need: New evidence across three studies. Motiv. Emot. 2020, 44, 32–53. [Google Scholar] [CrossRef]
- Sanz-Remacha, M.; García-González, L.; Sevil Serrano, J.; Aibar Solana, A. A Qualitative Evaluation of a Community-Based Intervention on Health-Related Behaviors in Disadvantaged Women. Res. Q. Exerc. Sport 2022, 1–11. [Google Scholar] [CrossRef]
- Sanz-Remacha, M.; Aibar, A.; Sevil-Serrano, J.; García-González, L. Evaluation of a 20-Month Physical Activity Intervention to Improve Motivational and Affective Outcomes among Disadvantaged Adult Women. Qual. Health Res. 2021, 31, 1392–1403. [Google Scholar] [CrossRef]
- Ransford, C.P. A role tor amines in the antidepressant effect of exercise: A review. Med. Sci. Sports Exerc. 1982, 14, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Teychenne, M.; Ball, K.; Salmon, J. Physical activity and likelihood of depression in adults: A review. Prev. Med. 2008, 46, 397–411. [Google Scholar] [CrossRef] [PubMed]
- Pels, F.; Kleinert, J. Loneliness and physical activity: A systematic review. Int. Rev. Sport Exerc. Psychol. 2016, 9, 231–260. [Google Scholar] [CrossRef]
- De Vries, H.; Schulz, D.; Scheneider, F.; Stanczyk, N.; Smit, E.; van Adrichem, M.; Vandelanotte, C.; Evers, S.; Candel, M.; Kremers, S. Effectiveness and cost-effectiveness of a web-based tailored multiple behavior change intervention. Eur. Health Psychol. 2014, 16, 439. [Google Scholar]
- Renzaho, A.M.; Mellor, D.; Boulton, K.; Swinburn, B. Effectiveness of prevention programmes for obesity and chronic diseases among immigrants to developed countries: A systematic review. Public Health Nutr. 2010, 13, 438–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Congello, N.C.; Koniak-Griffin, D.; Brecht, M.-L.; Hays, R.D.; Heilemann, M.-S.V.; Nyamathi, A.M. Associations of partner support and acculturation with physical activity in Mexican American women. Hisp. Health Care Int. 2020, 18, 98–104. [Google Scholar] [CrossRef]
- Joseph, R.P.; Ainsworth, B.E.; Keller, C.; Dodgson, J.E. Barriers to Physical Activity among African American Women: An Integrative Review of the Literature. Women Health 2015, 55, 679–699. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| ID | Age | Marital Status | Ethnic Group | Employment Contract |
|---|---|---|---|---|
| 1 | 42 | Married | Non-Roma | Short-term contract |
| 2 | 32 | Married | Roma | Unemployment |
| 3 | 36 | Widow | Roma | Short-term contract |
| 4 | 58 | Divorced | Non-Roma | Short-term contract |
| 5 | 44 | Widow | Roma | Unemployment |
| 6 | 38 | Married | Roma | Short-term contract |
| 7 | 39 | Married | Roma | Unemployment |
| 8 | 31 | Married | Non-Roma | Short-term contract |
| 9 | 29 | Married | Non-Roma | Short-term contract |
| 10 | 40 | Married | Roma | Unemployment |
| 11 | 28 | Married | Roma | Unemployment |
| Practical Sessions | Cognitive Sessions | Awareness Actions | |||
|---|---|---|---|---|---|
| Behaviours | Academic Year | Group-Based Sessions | Family Sessions | ||
| PA | 2016–2017 |
|
| The main topics of the sessions were:
| Four personalised notebooks with the following topics:
|
| 2017–2018 |
|
|
| ||
| HEALTHY EATING | 2016–2017 |
|
| Four personalised notebooks with the following topics:
| |
| 2017–2018 |
|
| |||
| FINAL SESSIONS | 2017–2018(4) | Aim of ending sessions: to close the program and remove consciousness to promote sustainability of the behavioural change First session (4): Projection of a video with a set of the interventions’ photos: questions about the video (4)
| |||
| Strategies’ Topic | Relatedness-Supportive Strategies |
|---|---|
| ‘Pío keeps moving’ decisions | Decisions about the organisational-intervention programme were discussed in groups. For example, the types of activities, timetables, and frequency of the sessions. |
| Sizes of groups | Continuous change in the size of groups carried out in the different PA sessions. For example, different couples. |
| Cooperative games | Teamwork and dynamic activities aimed to obtain an agreed solution. |
| Environment | Participants chose a friendly and comfortable environment to perform the activities in. |
| Mood’s PA professional | The PA professional was a trusted person, who was empathetic and patient throughout the intervention. |
| Funny meetings | Having dinner at the end of the first year; healthy snacks or coffee meetings to talk about the programme and share the participants’ experiences. |
| Social networking | Creating a WhatsApp group and Facebook profile for participants to keep in touch, and using it to remind participants about the timetables and meeting to perform PA. The motivational videos and positive feedback were provided by the Facebook profile. |
| Competence-supportive strategies | |
| Initial information | Participants were informed about the activities at the beginning of the sessions by the PA professional. |
| Variety of material and places | Participants tried out different type of new materials (e.g., elastic bands, bosus, TRX, fitballs, medicine balls) and places during the intervention (e.g., fitness centre, indoor sports centre facilities, swimming pool). |
| Variety of activities | A variety of group activities. For example, walking in groups around the city, familiar activities on the weekend, dancing in groups, circuits of muscle-building and toning exercises. |
| Adapted activities | PA professional offered the intensity and frequency levels in each activity depending on the subject. In addition, the trainer/staff designed activities for people who had suffered some type of injury. |
| Number of activities | Whenever possible, two or more different exercises were carried out in each PA session, and a vast body of opportunities were offered to achieve success. |
| Improvement feedback | Several strategies were implemented as follows:
|
| Motivational videos | Recording videos during the sessions (e.g., dances). From them, participants could analyse themselves and show them and compare their improvement. |
| Goals | Several strategies were implemented as follows:
|
| Autonomy-supportive strategies | |
| Making decisions | Several strategies were implemented as follows:
|
| PA events | Participants were encouraged to participate in PA events (e.g., popular walking) carried out in the city of Huesca (Spain) throughout the intervention. |
| Autonomous PA | Participants were encouraged and empowered to participate in autonomous PA. PA professional provided information related to friendly environments in the city to perform PA, material (e.g., PA notebook), City Hall’s activities with reduced prices (e.g., relaxation, gymnastics maintenance). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanz-Remacha, M.; Aibar, A.; Abós, Á.; Generelo-Lanaspa, E.; García-González, L. A Community-Based Participatory Action Research with Women from Disadvantaged Populations: Strengths and Weaknesses of a Multiple Health Behaviour Change Intervention. Int. J. Environ. Res. Public Health 2022, 19, 6830. https://doi.org/10.3390/ijerph19116830
Sanz-Remacha M, Aibar A, Abós Á, Generelo-Lanaspa E, García-González L. A Community-Based Participatory Action Research with Women from Disadvantaged Populations: Strengths and Weaknesses of a Multiple Health Behaviour Change Intervention. International Journal of Environmental Research and Public Health. 2022; 19(11):6830. https://doi.org/10.3390/ijerph19116830
Chicago/Turabian StyleSanz-Remacha, María, Alberto Aibar, Ángel Abós, Eduardo Generelo-Lanaspa, and Luis García-González. 2022. "A Community-Based Participatory Action Research with Women from Disadvantaged Populations: Strengths and Weaknesses of a Multiple Health Behaviour Change Intervention" International Journal of Environmental Research and Public Health 19, no. 11: 6830. https://doi.org/10.3390/ijerph19116830