
The Interlink among Age, Functional Fitness, and Perception of Health and Quality of Life: A Mediation Analysis

 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Procedures
2.3. Health and Quality of Life Perception
2.4. Anthropometric Measurements
2.5. Functional Fitness
2.6. Statistical Analysis
- (1)
- Age, Back Scratch, Arm Curl, Inphase, 3 min walking, PCS/MCS;
- (2)
- Age, Back Scratch, Arm Curl, Antiphase, 3 min walking, PCS/MCS;
- (3)
- Age, Chair Sit-and-Reach, Chair stand, Inphase, 3 min walking, PCS/MCS;
- (4)
- Age, Chair Sit-and-Reach, Chair stand, Antiphase, 3 min walking, PCS/MCS.
3. Results
3.1. Preliminary Analysis
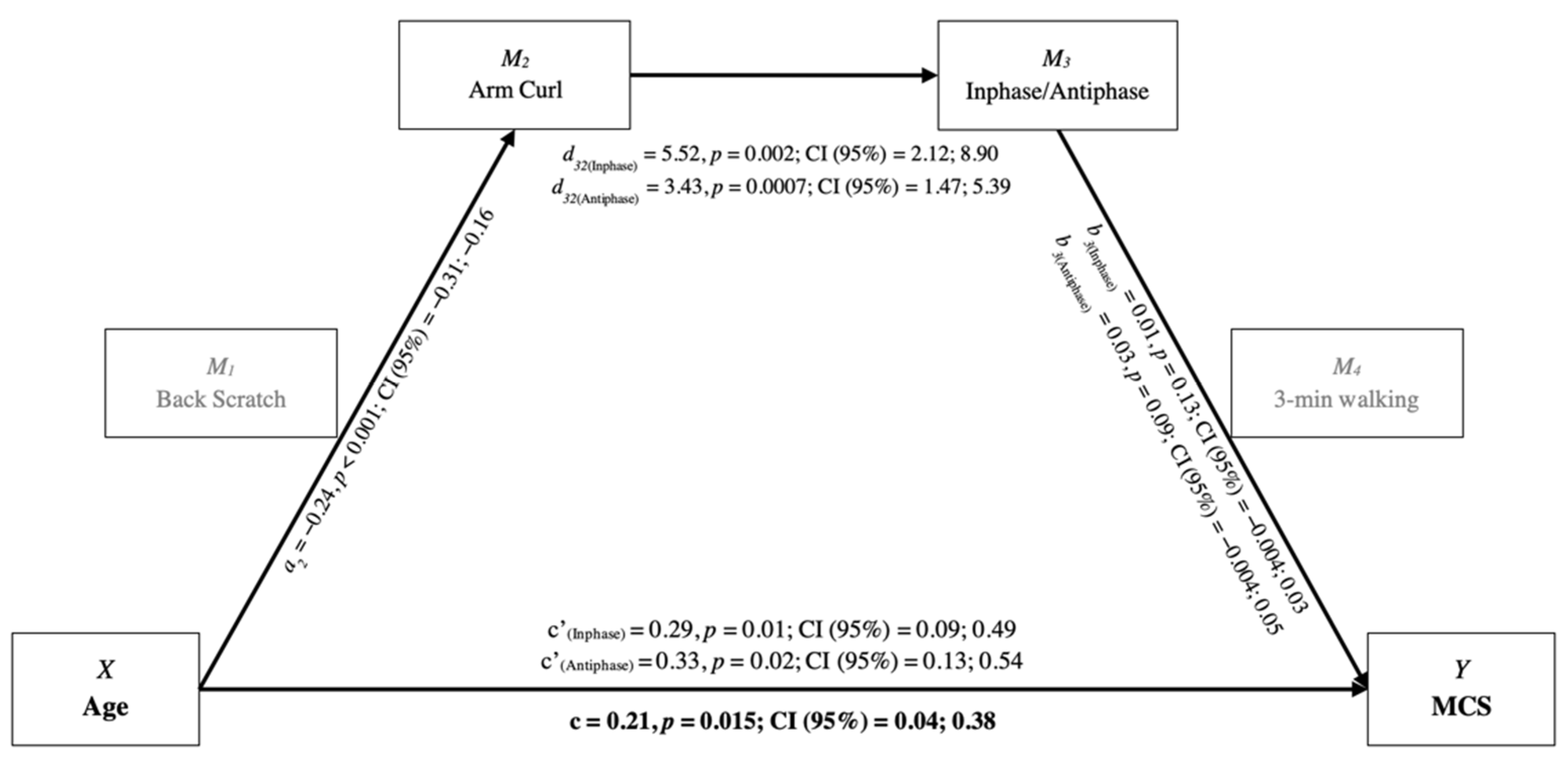
3.2. Mediation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Spirduso, W.; Francis, K.; MacRae, P. Physical Dimensions of Aging; Human Kinetics: Champain, IL, USA, 2005. [Google Scholar]
- World Health Organization. World Report on Ageing and Health. 2015. Available online: https://apps.who.int/iris/handle/10665/186463 (accessed on 25 January 2021).
- Condello, G.; Ling, F.C.M.; Bianco, A.; Chastin, S.; Cardon, G.; Ciarapica, D.; Conte, D.; Cortis, C.; De Craemer, M.; Di Blasio, A. Using concept mapping in the development of the EU-PAD framework (EUropean-Physical Activity Determinants across the life course): A DEDIPAC-study. BMC Public Health 2016, 16, 1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biddle, S.J.; Mutrie, N.; Gorely, T.; Faulkner, G. Psychology of Physical Activity: Determinants, Well-being and Interventions; Routledge: Oxfordshire, UK, 2021. [Google Scholar] [CrossRef]
- World Health Organization. Integrated Care for Older People: Guidelines on Community-Level Interventions to Manage Declines in Intrinsic Capacity. 2017. Available online: https://www.who.int/publications/i/item/9789241550109 (accessed on 25 January 2021).
- Burbank, P.M.; Padula, C.A.; Nigg, C.R. Changing health behaviors of older adults. J. Gerontol. Nurs. 2000, 26, 26–33; quiz 52–23. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Ciaccioni, S.; Capranica, L.; Forte, R.; Chaabene, H.; Pesce, C.; Condello, G. Effects of a judo training on functional fitness, anthropometric, and psychological variables in old novice practitioners. J. Aging. Phys. Act. 2019, 27, 831–842. [Google Scholar] [CrossRef] [PubMed]
- Eurobarometer. Sport and Physical Activity. European Commission. 2018. Available online: https://europa.eu/eurobarometer/surveys/detail/2164 (accessed on 25 January 2021).
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World. 2018. Available online: https://apps.who.int/iris/handle/10665/272722 (accessed on 25 January 2021).
- Rosenbloom, C.; Bahns, M. What can we learn about diet and physical activity from master athletes? Holist. Nurs. Pract. 2006, 20, 161–166; quiz 167–168. [Google Scholar] [CrossRef]
- Sallinen, J.; Ojanen, T.; Karavirta, L.; Ahtiainen, J.P.; Hakkinen, K. Muscle mass and strength, body composition and dietary intake in master strength athletes vs untrained men of different ages. J. Sports Med. Phys. Fit. 2008, 48, 190–196. [Google Scholar]
- Condello, G.; Capranica, L.; Stager, J.; Forte, R.; Falbo, S.; Di Baldassarre, A.; Segura-Garcia, C.; Pesce, C. Physical activity and health perception in aging: Do body mass and satisfaction matter? A three-path mediated link. PLoS ONE 2016, 11, e0160805. [Google Scholar] [CrossRef] [Green Version]
- Dionigi, R. Leisure and identity management in later life: Understanding competitive sport participation among older adults. World Leis. J. 2002, 44, 4–15. [Google Scholar] [CrossRef]
- Holland, G.J.; Tanaka, K.; Shigematsu, R.; Nakagaichi, M. Flexibility and physical functions of older adults: A review. J. Aging Phys. Activ. 2002, 10, 169–206. [Google Scholar] [CrossRef] [Green Version]
- Cadore, E.L.; Rodriguez-Manas, L.; Sinclair, A.; Izquierdo, M. Effects of different exercise interventions on risk of falls, gait ability, and balance in physically frail older adults: A systematic review. Rejuv. Res. 2013, 16, 105–114. [Google Scholar] [CrossRef] [Green Version]
- Abu-Omar, K.; Gelius, P.; Messing, S. The evolution of physical activity promotion. Are we entering a liquid age? Glob. Health Promot. 2020, 27, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Brug, J.; van der Ploeg, H.P.; Loyen, A.; Ahrens, W.; Allais, O.; Andersen, L.F.; Cardon, G.; Capranica, L.; Chastin, S.; De Bourdeaudhuij, I.; et al. Determinants of diet and physical activity (DEDIPAC): A summary of findings. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 150. [Google Scholar] [CrossRef] [Green Version]
- Layte, R.; Sexton, E.; Savva, G. Quality of life in older age: Evidence from an Irish cohort study. J. Am. Geriatr. Soc. 2013, 61, S299–S305. [Google Scholar] [CrossRef] [PubMed]
- Borg, C.; Fagerström, C.; Balducci, C.; Burholt, V.; Ferring, D.; Weber, G.; Wenger, C.; Holst, G.; Hallberg, I.R. Life satisfaction in 6 European countries: The relationship to health, self-esteem, and social and financial resources among people (aged 65–89) with reduced functional capacity. Geriatr. Nurs. 2008, 29, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Domingos, C.; Pêgo, J.M.; Santos, N.C. Effects of physical activity on brain function and structure in older adults: A systematic review. Behav. Brain Res. 2021, 402, 113061. [Google Scholar] [CrossRef]
- Maynou, L.; Hernández-Pizarro, H.M.; Errea Rodríguez, M. The association of physical (in) activity with mental health. Differences between elder and younger populations: A systematic literature review. Int. J. Environ. Res. Public Health 2021, 18, 4771. [Google Scholar] [CrossRef]
- Chung, P.K.; Zhao, Y.; Liu, J.D.; Quach, B. A canonical correlation analysis on the relationship between functional fitness and health-related quality of life in older adults. Arch. Gerontol. Geriatr. 2017, 68, 44–48. [Google Scholar] [CrossRef]
- Wanderley, F.A.; Silva, G.; Marques, E.; Oliveira, J.; Mota, J.; Carvalho, J. Associations between objectively assessed physical activity levels and fitness and self-reported health-related quality of life in community-dwelling older adults. Qual. Life Res. 2011, 20, 1371–1378. [Google Scholar] [CrossRef]
- Halaweh, H. Correlation between health-related quality of life and hand grip strength among older adults. Exp. Aging Res. 2020, 46, 178–191. [Google Scholar] [CrossRef]
- Gómez-Bruton, A.; López-Torres, O.; Gómez-Cabello, A.; Rodríguez-Gomez, I.; Pérez-Gómez, J.; Pedrero-Chamizo, R.; Gusi, N.; Ara, I.; Casajús, J.A.; Gonzalez-Gross, M.; et al. How important is current physical fitness for future quality of life? Results from an 8-year longitudinal study on older adults. Exp. Gerontol. 2021, 149, 111301. [Google Scholar] [CrossRef]
- Jantunen, H.; Wasenius, N.; Salonen, M.K.; Kautiainen, H.; von Bonsdorff, M.B.; Kajantie, E.; Eriksson, J.G. Change in physical activity and health-related quality of life in old age—A 10-year follow-up study. Scand. J. Med. Sci. Sports 2019, 29, 1797–1804. [Google Scholar] [CrossRef] [PubMed]
- Condello, G.; Capranica, L.; Migliaccio, S.; Forte, R.; Di Baldassarre, A.; Pesce, C. Energy balance and active lifestyle: Potential mediators of health and quality of life perception in aging. Nutrients 2019, 11, 2122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osness, W.H.; Adrian, M.; Clark, B.; Hoeger, W.; Diane, R.; Robert, W. Functional Fitness Assessment for Adults Over 60 Years (A Field Based Assessment); The American Alliance for Health, Physical Education, Recreation and Dance, Reston: New York, NY, USA, 1990. [Google Scholar]
- Ware, J.; Kosinski, M.; Keller, S. SF12: How To Score The SF-12 Physical And Mental Health Summary Scales, 2nd ed.; The Health Institute, New England Medical Center: Boston, MA, USA, 1995. [Google Scholar]
- Gandek, B.; Ware, J.E.; Aaronson, N.K.; Apolone, G.; Bjorner, J.B.; Brazier, J.E.; Bullinger, M.; Kaasa, S.; Leplege, A.; Prieto, L.; et al. Cross-validation of item selection and scoring for the SF-12 Health Survey in nine countries: Results from the IQOLA Project. International quality of life assessment. J. Clin. Epidemiol. 1998, 51, 1171–1178. [Google Scholar] [CrossRef]
- Apolone, G.; Mosconi, P.; Quattrociocchi, L.; Gianicolo, E.A.L.; Groth, N.; Ware, J.E.J. Questionario Sullo Stato di Salute SF-12. Versione Italiana [SF-12 Questionnaire. Italian Version]; IRFMN: Milano, Italy, 2005. [Google Scholar]
- Rikli, R.E.; Jones, C.J. Senior Fitness Test Manual; Human Kinetics: Champain, IL, USA, 2013. [Google Scholar]
- Liu, C.J.; Marie, D.; Fredrick, A.; Bertram, J.; Utley, K.; Fess, E.E. Predicting hand function in older adults: Evaluations of grip strength, arm curl strength, and manual dexterity. Aging Clin. Exp. Res. 2017, 29, 753–760. [Google Scholar] [CrossRef] [Green Version]
- Mehmet, H.; Yang, A.W.; Robinson, S.R. What is the optimal chair stand test protocol for older adults? A systematic review. Disabil. Rehabil. 2020, 42, 2828–2835. [Google Scholar] [CrossRef]
- Capranica, L.; Tessitore, A.; Olivieri, B.; Minganti, C.; Pesce, C. Field evaluation of cycled coupled movements of hand and foot in older individuals. Gerontology 2004, 50, 399–406. [Google Scholar] [CrossRef]
- Cortis, C.; Tessitore, A.; Perroni, F.; Lupo, C.; Pesce, C.; Ammendolia, A.; Capranica, L. Interlimb coordination, strength, and power in soccer players across the lifespan. J. Strength Cond. Res. 2009, 23, 2458–2466. [Google Scholar] [CrossRef]
- Cao, Z.B.; Miyatake, N.; Aoyama, T.; Higuchi, M.; Tabata, I. Prediction of maximal oxygen uptake from a 3-minute walk based on gender, age, and body composition. J. Phys. Act. Health 2013, 10, 280–287. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Functional fitness normative scores for community-residing older adults, ages 60–94. J. Aging Phys. Activ. 1999, 7, 162–181. [Google Scholar] [CrossRef]
- Richardson, J.T. Eta squared and partial eta squared as measures of effect size in educational research. Educ. Res. Rev. 2011, 6, 135–147. [Google Scholar] [CrossRef]
- Hopkins, W.G. A scale of magnitudes for effect statistics. New View Stat. 2002, 502, 411. [Google Scholar]
- Hayes, A.F. Introduction To Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2017. [Google Scholar]
- Zhao, Y.; Wang, Z.; Chung, P.K.; Wang, S. Functional fitness norms and trends of community-dwelling older adults in urban China. Sci. Rep. 2021, 11, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, B.M.; Stalling, I.; Bammann, K. Sex-and age-specific normative values for handgrip strength and components of the Senior Fitness Test in community-dwelling older adults aged 65–75 years in Germany: Results from the OUTDOOR ACTIVE study. BMC Geriatr. 2021, 21, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Konig, H.H.; Heider, D.; Lehnert, T.; Riedel-Heller, S.G.; Angermeyer, M.C.; Matschinger, H.; Vilagut, G.; Bruffaerts, R.; Haro, J.M.; de Girolamo, G.; et al. Health status of the advanced elderly in six European countries: Results from a representative survey using EQ-5D and SF-12. Health Qual. Life Outcomes 2010, 8, 143. [Google Scholar] [CrossRef]
- Gayman, A.M.; Fraser-Thomas, J.; Dionigi, R.A.; Horton, S.; Baker, J. Is sport good for older adults? A systematic review of psychosocial outcomes of older adults’ sport participation. Int. Rev. Sport Exerc. Psychol. 2017, 10, 164–185. [Google Scholar] [CrossRef]
- Bouaziz, W.; Lang, P.O.; Schmitt, E.; Kaltenbach, G.; Geny, B.; Vogel, T. Health benefits of multicomponent training programmes in seniors: A systematic review. Int. J. Clin. Pract. 2016, 70, 520–536. [Google Scholar] [CrossRef]
- Raafs, B.M.; Karssemeijer, E.G.; Van der Horst, L.; Aaronson, J.A.; Rikkert, M.G.O.; Kessels, R.P. Physical exercise training improves quality of life in healthy older adults: A meta-analysis. J. Aging Phys. Act. 2020, 28, 81–93. [Google Scholar] [CrossRef]
- Santos, D.A.; Silva, A.M.; Baptista, F.; Santos, R.; Vale, S.; Mota, J.; Sardinha, L.B. Sedentary behavior and physical activity are independently related to functional fitness in older adults. Exp. Gerontol. 2012, 47, 908–912. [Google Scholar] [CrossRef]
- Ciaccioni, S.; Pesce, C.; Capranica, L.; Condello, G. Effects of a judo training program on falling performance, fear of falling and exercise motivation in older novice judoka. Ido. Mov. Cult. 2021, 21, 9–17. [Google Scholar] [CrossRef]
- Kawagoe, T.; Onoda, K.; Yamaguchi, S. Associations among executive function, cardiorespiratory fitness, and brain network properties in older adults. Sci. Rep. 2017, 7, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Geard, D.; Rebar, A.L.; Dionigi, R.A.; Reaburn, P.R.J. Testing a model of successful aging on masters athletes and non-sporting adults. Res. Exerc. Sport 2021, 92, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.S.; Yan, J.H.; Payne, V.G. The impact of obesity and exercise on cognitive aging. Front. Aging Neurosci. 2013, 5, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.; Chan, J.S.; Ren, L.; Yan, J.H. Obesity reduces cognitive and motor functions across the lifespan. Neural. Plast. 2016, 2016, 2473081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacKinnon, D.P.; Fairchild, A.J.; Fritz, M.S. Mediation analysis. Annu. Rev. Psychol. 2007, 58, 593–614. [Google Scholar] [CrossRef] [PubMed]
- Thomas, M.L.; Kaufmann, C.N.; Palmer, B.W.; Depp, C.A.; Martin, A.S.; Glorioso, D.K.; Thompson, W.K.; Jeste, D.V. Paradoxical trend for improvement in mental health with aging: A community-based study of 1,546 adults aged 21-100 years. J. Clin. Psychiatry 2016, 77, e1019–e1025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Lai, D.W.L.; Chappell, N.L. The older, the happier? A cross-sectional study on the “Paradox of Aging” in China. Res. Aging 2022, 44, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Tseng, H.Y.; Löckenhoff, C.; Lee, C.Y.; Yu, S.H.; Wu, I.; Chang, H.Y.; Chiu, Y.-F.; Hsiung, C.A. The paradox of aging and health-related quality of life in Asian Chinese: Results from the Healthy Aging Longitudinal Study in Taiwan. BMC Geriatr. 2020, 20, 1–10. [Google Scholar] [CrossRef]
- Rejeski, W.J.; Mihalko, S.L. Physical activity and quality of life in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, 23–35. [Google Scholar] [CrossRef] [Green Version]
- Spector, P.E. Do not cross me: Optimizing the use of cross-sectional designs. J. Bus. Psychol. 2019, 34, 125–137. [Google Scholar] [CrossRef]
- Di Lorito, C.; Long, A.; Byrne, A.; Harwood, R.H.; Gladman, J.R.; Schneider, S.; Logan, P.; Bosco, A.; van der Wardt, V. Exercise interventions for older adults: A systematic review of meta-analyses. J. Sport Health Sci. 2021, 10, 29–47. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Body Mass (kg) | Height (m) | BMI (kg·m−2) | Medications (n) | Diseases (n) | |
|---|---|---|---|---|---|
| Activity level | |||||
| Senior athletes | 69.5 ± 10.0 | 1.67 ± 0.07 | 24.87 ± 2.72 1,2 | 1.2 ± 1.2 1,2 | 1.8 ± 2.0 |
| Physically active | 73.7 ± 12.0 | 1.65 ± 0.09 | 27.15 ± 3.73 | 3.5 ± 2.9 | 2.9 ± 2.2 |
| Sedentary | 75.7 ± 14.6 | 1.64 ± 0.10 | 27.96 ± 3.80 | 3.6 ± 2.8 | 3.0 ± 2.9 |
| Age class | |||||
| 55–64 | 76.0 ± 14.3 4 | 1.68 ± 0.08 3,4 | 26.81 ± 4.14 | 1.9 ± 1.8 3,4 | 1.5 ± 2.1 3,4 |
| 65–74 | 73.8 ± 12.7 4 | 1.64 ± 0.09 | 27.45 ± 3.61 | 3.3 ± 2.6 | 2.9 ± 2.3 |
| 75–84 | 69.6 ± 9.8 | 1.63 ± 0.09 | 26.19 ± 3.18 | 3.8 ± 3.3 | 3.7 ± 2.6 |
| Gender | |||||
| Female | 65.3 ± 9.8 5 | 1.59 ± 0.06 5 | 26.05 ± 4.01 | 3.3 ± 3.2 | 2.8 ± 2.5 |
| Male | 79.6 ± 11.3 | 1.70 ± 0.07 | 27.48 ± 3.35 | 2.6 ± 2.2 | 2.5 ± 2.5 |
| Back Scratch (cm) | Chair Sit-and-Reach (cm) | Arm Curl (n) | Chair Stand (n) | InPhase (s) | Antiphase (s) | 3 min Walking (m) | PCS (pt) | MCS (pt) | |
|---|---|---|---|---|---|---|---|---|---|
| Activity level | |||||||||
| Senior athletes | −2.2 ± 10.1 1 | 2.4 ± 12.5 1 | 18.9 ± 4.6 1,2 | 16.6 ± 3.4 1,2 | 225.7 ± 96.5 | 53.5 ± 71.5 1,2 | 330.4 ± 28.2 1,2 | 54.7 ± 5.0 1 | 53.7 ± 7.7 1 |
| Physically active | −3.5 ± 9.3 | 0.4 ± 11.6 | 17.0 ± 3.8 | 14.1 ± 3.0 | 232.3 ± 93.1 | 33.2 ± 55.9 | 291.8 ± 42.5 | 51.9 ± 7.2 | 52.0 ± 9.0 |
| Sedentary | −6.2 ± 10.4 | −5.7 ± 11.1 2 | 14.5 ± 3.6 2 | 13.0 ± 2.4 2 | 198.3 ± 69.1 2 | 19.5 ± 34.5 | 276.8 ± 45.3 2 | 49.7 ± 8.3 | 49.4 ± 10.0 |
| Age class | |||||||||
| 55–64 | −0.3 ± 6.8 3,4 | 2.4 ± 12.1 3,4 | 19.1 ± 4.4 3,4 | 15.4 ± 3.6 3,4 | 245.5 ± 80.0 3 | 64.9 ± 71.6 3,4 | 315.5 ± 42.0 3,4 | 52.8 ± 6.7 | 49.1 ± 10.6 4 |
| 65–74 | −5.0 ± 9.9 | −2.2 ± 11.9 | 15.8 ± 3.2 4 | 13.7 ± 2.1 | 190.9 ± 82.4 | 17.7 ± 32.6 | 293.9 ± 40.8 4 | 50.3 ± 8.0 | 51.7 ± 8.2 |
| 75–84 | −7.9 ± 11.8 | −5.1 ± 11.3 | 14.4 ± 3.9 | 13.7 ± 3.5 | 215.3 ± 90.6 | 13.0 ± 32.0 | 275.3 ± 46.1 | 52.3 ± 7.1 | 54.2 ± 7.7 |
| Gender | |||||||||
| Female | −0.4 ± 7.4 5 | 2.9 ± 12.4 5 | 16.6 ± 4.5 | 14.0 ± 3.6 | 211.4 ± 89.4 | 38.3 ± 62.7 | 277.8 ± 48.0 5 | 51.0 ± 7.6 | 49.4 ± 10.7 |
| Male | −7.1 ± 10.8 | −4.8 ± 10.8 | 16.5 ± 4.2 | 14.5 ± 2.9 | 222.5 ± 84.6 | 29.5 ± 48.7 | 310.9 ± 37.8 | 52.4 ± 7.2 | 53.1 ± 7.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciaccioni, S.; Pesce, C.; Forte, R.; Presta, V.; Di Baldassarre, A.; Capranica, L.; Condello, G. The Interlink among Age, Functional Fitness, and Perception of Health and Quality of Life: A Mediation Analysis. Int. J. Environ. Res. Public Health 2022, 19, 6850. https://doi.org/10.3390/ijerph19116850
Ciaccioni S, Pesce C, Forte R, Presta V, Di Baldassarre A, Capranica L, Condello G. The Interlink among Age, Functional Fitness, and Perception of Health and Quality of Life: A Mediation Analysis. International Journal of Environmental Research and Public Health. 2022; 19(11):6850. https://doi.org/10.3390/ijerph19116850
Chicago/Turabian StyleCiaccioni, Simone, Caterina Pesce, Roberta Forte, Valentina Presta, Angela Di Baldassarre, Laura Capranica, and Giancarlo Condello. 2022. "The Interlink among Age, Functional Fitness, and Perception of Health and Quality of Life: A Mediation Analysis" International Journal of Environmental Research and Public Health 19, no. 11: 6850. https://doi.org/10.3390/ijerph19116850