
Acute Effects of High-Intensity Interval Training on Diabetes Mellitus: A Systematic Review

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.1.1. Population
2.1.2. Intervention
2.1.3. Comparator
2.1.4. Outcomes
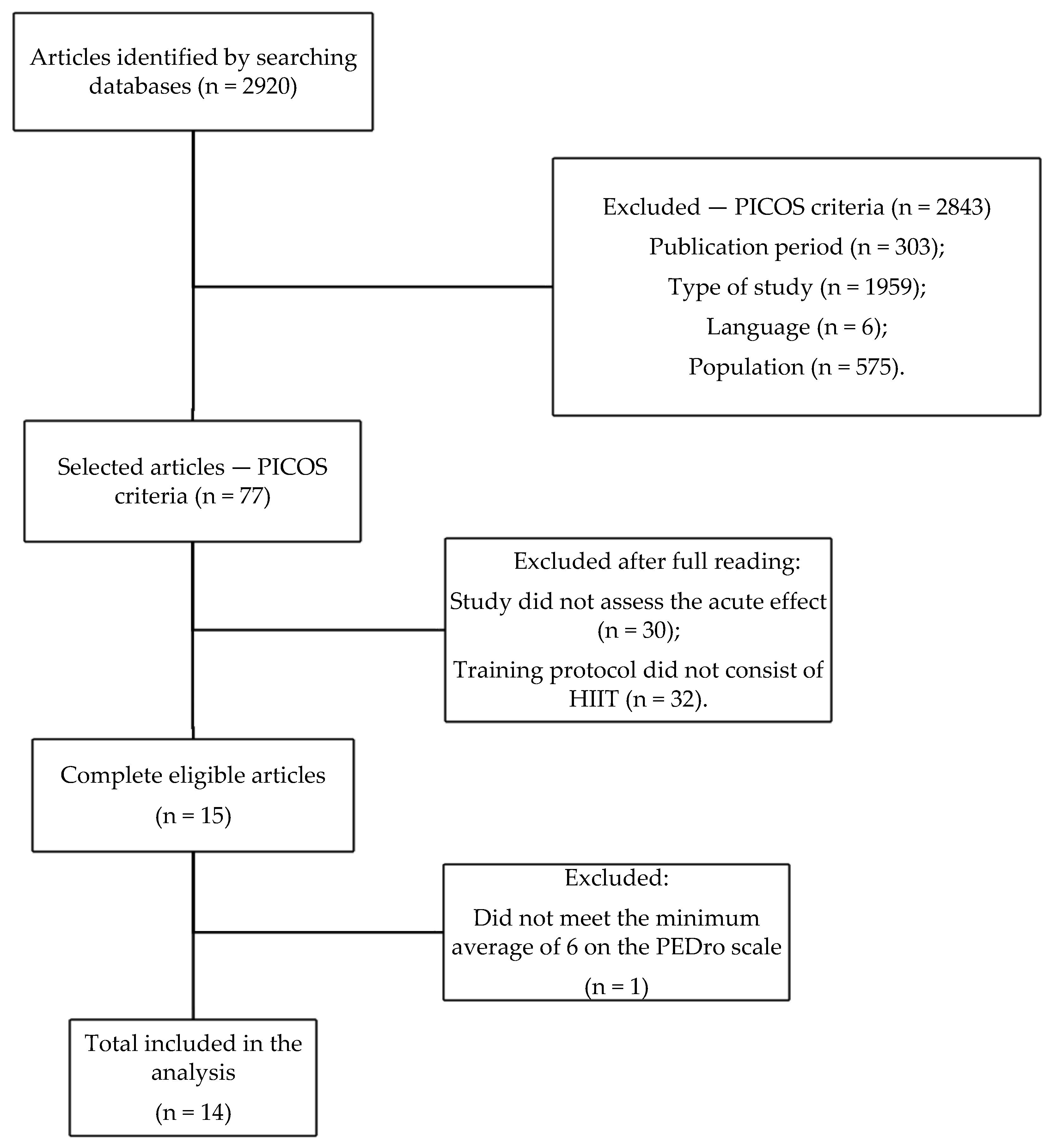
2.2. Study Design
2.3. Data Extraction
2.4. Evaluation of Methodological Quality
3. Results
4. Discussion
4.1. Capillary Blood Glucose Levels
4.2. Postprandial Blood Glucose and Time/Exposure to Hyperglycemia
4.3. 24 h Glycemic Profile and Hypoglycemia
4.4. Blood Pressure and Vascular Function
4.5. Hormones and Indicators of Cellular and Systemic Inflammation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- International Diabetes Federation (IDF). IDF Diabetes Atlas. 2019; p. 1. Available online: https://www.diabetesatlas.org/en/ (accessed on 26 January 2022).
- American Diabetes Association. Standards of Medical Care in Diabetes-2019 Abridged for Primary Care Providers. Clin. Diabetes 2019, 37, 11–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Report on Diabetes. 2016. Available online: http://apps.who.int/iris/bitstream/handle/10665/204871/9789241565257_eng.pdf?sequence=1&isAllowed=y (accessed on 26 January 2022).
- De Nardi, A.T.; Tolves, T.; Lenzi, T.L.; Signori, L.U.; da Silva, A.M.V. High-intensity interval training versus continuous training on physiological and metabolic variables in prediabetes and type 2 diabetes: A meta-analysis. Diabetes Res. Clin. Pract. 2018, 137, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Thiel, D.M.; Al Sayah, F.; Vallance, J.K.; Johnson, S.T.; Johnson, J.A. Association between Physical Activity and Health-Related Quality of Life in Adults with Type 2 Diabetes. Can. J. Diabetes 2017, 41, 58–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sacre, J.W.; Jellis, C.L.; Jenkins, C.; Haluska, B.A.; Baumert, M.; Coombes, J.S.; Marwick, T.H. A six-month exercise intervention in subclinical diabetic heart disease: Effects on exercise capacity, autonomic and myocardial function. Metab. Clin. Exp. 2014, 63, 1104–1114. [Google Scholar] [CrossRef] [Green Version]
- Egan, A.M.; Mahmood, W.A.W.; Fenton, R.; Redziniak, N.; Kyaw Tun, T.; Sreenan, S.; Mcdermott, J.H. Barriers to exercise in obese patients with type 2 diabetes. QJM 2013, 106, 635–638. [Google Scholar] [CrossRef]
- Guiraud, T.; Nigam, A.; Gremeaux, V.; Meyer, P.; Juneau, M.; Bosquet, L. High-Intensity Interval Training in Cardiac Rehabilitation. Sport 2012, 42, 587–605. [Google Scholar] [CrossRef]
- Weston, K.S.; Wisløff, U.; Coombes, J.S. High-intensity interval training in patients with lifestyle-induced cardiometabolic disease: A systematic review and meta-analysis. Br. J. Sports Med. 2014, 48, 1227–1234. [Google Scholar] [CrossRef]
- Kelly, B.M.; Xenophontos, S.; King, J.A.; Nimmo, M.A. An evaluation of low volume high-intensity intermittent training (HIIT) for health risk reduction in overweight and obese men. BMC Obes. 2017, 4, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Meyer, P.; Normandin, E.; Gayda, M.; Billon, G.; Guiraud, T.; Bosquet, L.; Nigam, A. High-intensity interval exercise in chronic heart failure: Protocol optimization. J. Card. Fail. 2012, 18, 126–133. [Google Scholar] [CrossRef]
- Bird, S.R.; Hawley, J.A. Update on the effects of physical activity on insulin sensitivity in humans. BMJ Open Sport Exerc. Med. 2017, 2, 1–26. [Google Scholar] [CrossRef] [Green Version]
- Francois, M.E.; Durrer, C.; Pistawka, K.J.; Halperin, F.A.; Little, J.P. Resistance-based interval exercise acutely improves endothelial function in type 2 diabetes. Am. J. Physiol. Heart Circ. Physiol. 2016, 311, H1258–H1267. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durrer, C.; Francois, M.; Neudorf, H.; Little, J.P. Acute high-intensity interval exercise reduces human monocyte toll-like receptor 2 expression in type 2 diabetes. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2017, 312, R529–R538. [Google Scholar] [CrossRef]
- Jayawardene, D.C.; McAuley, S.A.; Horsburgh, J.C.; La Gerche, A.; Jenkins, A.J.; Ward, G.M.; O’Neal, D.N. Closed-loop insulin delivery for adults with type 1 diabetes undertaking high-intensity interval exercise versus moderate-intensity exercise: A randomized, crossover study. Diabetes Technol. Ther. 2017, 19, 340–348. [Google Scholar] [CrossRef]
- Karstoft, K.; Christensen, C.S.; Pedersen, B.K.; Solomon, T.P.J. The acute effects of interval-Vs continuous-walking exercise on glycemic control in subjects with type 2 diabetes: A crossover, controlled study. J. Clin. Endocrinol. Metab. 2014, 99, 3334–3342. [Google Scholar] [CrossRef] [Green Version]
- Karstoft, K.; Wallis, G.A.; Pedersen, B.K.; Solomon, T.P.J. The effects of interval vs. continuous exercise on excess post-exercise oxygen consumption and substrate oxidation rates in subjects with type 2 diabetes. Metab. Clin. Exp. 2016, 65, 1316–1325. [Google Scholar] [CrossRef] [Green Version]
- Mendes, R.; Sousa, N.; Themudo-Barata, J.L.; Reis, V.M. High-intensity interval training versus moderate-intensity continuous training in middle-aged and older patients with type 2 diabetes: A randomized controlled crossover trial of the acute effects of treadmill walking on glycemic control. Int. J. Environ. Res. Public Health 2019, 16, 4163. [Google Scholar] [CrossRef] [Green Version]
- Mendes, R.; Sousa, N.; Garrido, N.; Rocha, P.; Themudo Barata José, L.; Reis Victor, M. Efficacy of Acute High-Intensity Interval Training in Lowering Glycemia in Patients With Type 2 Diabetes: Diabetes Em Movimento® Pilot Study. Br. J. Sports Med. 2013, 47, e3. [Google Scholar] [CrossRef]
- Metcalfe, R.S.; Fitzpatrick, B.; Fitzpatrick, S.; McDermott, G.; Brick, N.; McClean, C.; Davison, G.W. Extremely short duration interval exercise improves 24-h glycaemia in men with type 2 diabetes. Eur. J. Appl. Physiol. 2018, 118, 2551–2562. [Google Scholar] [CrossRef]
- Rooijackers, H.M.; Wiegers, E.C.; Van Der Graaf, M.; Thijssen, D.H.; Kessels, R.P.C.; Tack, C.J.; De Galan, B.E. A single bout of high-intensity interval training reduces awareness of subsequent hypoglycemia in patients with type 1 diabetes. Diabetes 2017, 66, 1990–1998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santiago, É.; Delevatti, R.S.; Bracht, C.G.; Netto, N.; Lisboa, S.C.; Vieira, A.F.; Kruel, L.F.M. Acute glycemic and pressure responses of continuous and interval aerobic exercise in patients with type 2 diabetes. Clin. Exp. Hypertens. 2017, 40, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Scott, S.N.; Cocks, M.; Andrews, R.C.; Narendran, P.; Purewal, T.S.; Cuthbertson, D.J.; Shepherd, S.O. Fasted high-intensity interval and moderate-intensity exercise do not lead to detrimental 24-hour blood glucose profiles. J. Clin. Endocrinol. Metab. 2019, 104, 111–117. [Google Scholar] [CrossRef]
- Viana, A.A.; Fernandes, B.; Alvarez, C.; Guimarães, G.V.; Ciolac, E.G. Prescribing high-intensity interval exercise by rpe in individuals with type 2 diabetes: Metabolic and hemodynamic responses. Appl. Physiol. Nutr. Metab. 2019, 44, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Gillen, J.B.; Little, J.P.; Punthakee, Z.; Tarnopolsky, M.A.; Riddell, M.C.; Gibala, M.J. Acute high-intensity interval exercise reduces the postprandial glucose response and prevalence of hyperglycaemia in patients with type 2 diabetes. Diabetes Obes. Metab. 2012, 14, 575–577. [Google Scholar] [CrossRef]
- Terada, T.; Wilson, B.J.; Myette-Cóté, E.; Kuzik, N.; Bell, G.J.; McCargar, L.J.; Boulé, N.G. Targeting specific interstitial glycemic parameters with high-intensity interval exercise and fasted-state exercise in type 2 diabetes. Metab. Clin. Exp. 2016, 65, 599–608. [Google Scholar] [CrossRef]
- Kirwan, J.P.; Sacks, J.; Nieuwoudt, S. The essential role of exercise in the management of type 2 diabetes. Clevel. Clin. J. Med. 2017, 84, S15–S21. [Google Scholar] [CrossRef]
- Magkos, F.; Tsekouras, Y.; Kavouras, S.A.; Mittendorfer, B.; Sidossis, L.S. Improved insulin sensitivity after a single bout of exercise is curvilinearly related to exercise energy expenditure. Clin. Sci. 2008, 114, 59–64. [Google Scholar] [CrossRef] [Green Version]
- Turnbull, F. Effects of different blood pressure-lowering regimens on major cardiovascular events in individuals with and without diabetes mellitus: Results of prospectively designed overviews of randomized trials. Arch. Intern. Med. 2005, 165, 1410–1419. [Google Scholar] [CrossRef] [Green Version]
- Michael, S.; Graham, K.S.; Oam, G.M.D. Cardiac autonomic responses during exercise and post-exercise recovery using heart rate variability and systolic time intervals-a review. Front. Physiol. 2017, 8, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Robinson, E.; Durrer, C.; Simtchouk, S.; Jung, M.E.; Bourne, J.E.; Voth, E.; Little, J.P. Short-term high-intensity interval and moderate-intensity continuous training reduce leukocyte TLR4 in inactive adults at elevated risk of type 2 diabetes. J. Appl. Physiol. 2015, 119, 508–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gleeson, M.; Bishop, N.C.; Stensel, D.J.; Lindley, M.R.; Mastana, S.S.; Nimmo, M.A. The anti-inflammatory effects of exercise: Mechanisms and implications for the prevention and treatment of disease. Nat. Rev. Immunol. 2011, 11, 607–610. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reference | Specific Eligibility Criteria | Randomized Allocation | Secret Allocation (Blind) | Groups Similar to Baseline | Blind Participation of Subjects | Blind Intervention and Evaluation | <15% Loss | Intent-to-Treat Analysis | Intergroup Statistics Reported | Measurements and Precision and Variability | Total PEDro Score |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Durrer et al., 2017 [16] | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Francois et al., 2015 [13] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 8 |
| Jayawardene et al., 2017 [17] | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 8 | |
| Karstoft et al., 2014 [18] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 8 |
| Karstoft et al., 2016 [19] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 8 |
| Mendes et al., 2019 [20] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 8 |
| Mendes et al., 2013 [21] | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Metcalfe et al., 2018 [22] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 8 |
| Rooijackers et al., 2017 [23] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 8 |
| Santiago et al., 2017 [24] | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 6 |
| Scott et al., 2019 [25] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 8 |
| Viana et al., 2019 [26] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 8 |
| Gillen et al., 2012 [27] | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Terada et al., 2016 [28] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 8 |
| Author/Year | Participants | Sex | N | Age (Years) | BMI (kg/m²) |
|---|---|---|---|---|---|
| Durrer et al., 2017 [16] | DM2 and NG | 5F 5M 5F 4M | 10 DM2 and 9 NG | 57.9 ± 5.4 and 55.8 ± 9.0 | 34.8 ± 5.9 and 24.8 ± 3.6 |
| Francois et al., 2015 [13] | DM2 NG TN NG SD | 21F 14M | 12 DM2 11 NG TN 12 NG SD | 57.5 ± 5.0 55.3 ± 9.1 55.1 ± 7.0 | 35.0 ± 7.0 26.0 ± 5.0 23.0 ± 3.0 |
| Jayawardene et al., 2017 [17] | DM1 | 9F 3M | 12 DM1 | 40.0 ± 13.0 | 25.3 ± 3.2 |
| Karstoft et al., 2014 [18] | DM2 | 3F 7M | 10 DM2 | 60.3 ± 2.3 | 28.3 ± 1.1 |
| Karstoft et al., 2016 [19] | DM2 | 3F 7M | 10 DM2 | 60.3 ± 2.3 | 28.3 ± 1.1 |
| Mendes et al., 2019 [20] | DM2 | 8F 7M | 15 DM2 | 60.2 ± 3.1 | 29.6 ± 4.61 |
| Mendes et al., 2013 [21] | DM2 | 6F 6M | 12 DM2 | 58.7 ± 5.3 | 30.7 ± 5.6 |
| Metcalfe et al., 2018 [22] | DM2 | 11M | 11 DM2 | 52.0 ± 6.0 | 29.7 ± 3.1 |
| Rooijackers et al., 2017 [23] | DM1–AH DM1–AH NG | 4F 6M 5F 5M 5W 5M | 10 DM1 NAH 10 DM1 IAH 10 NG | 23.9 ± 4.4 25.7 ± 5.8 25.2 ± 5.5 | 23.0 ± 2.3 23.4 ± 1.4 22.5 ± 1.8 |
| Santiago et al., 2017 [24] | DM2 | No Information | 14 DM2 | 63.6 ± 9.8 | 30.3 ± 4.4 |
| Scott et al., 2019 [25] | DM1 | 8F 6M | 14 DM1 | 26.0 ± 3.0 | 27.6 ± 13.0 |
| Viana et al., 2019 [26] | DM2 | 9F 2M | 11 DM2 | 52.3 ± 3.0 | 28.4 ± 1.5 |
| Gillen et al., 2012 [27] | DM2 | No Information | 7 DM2 | 62.0 ± 3.0 | 30.5 ± 1.9 |
| Terada et al., 2016 [28] | DM2 | 2F 8M | 10 DM2 | 60.0 ± 6.0 | 30.8 ± 5.4 |
| Author/Year | Objectives | Methods | Equipment | Type of Training | Duration (min) | Protocol |
|---|---|---|---|---|---|---|
| Durrer et al., 2017 [16] | To determine the impact of a single HIIT session on cellular, molecular, and circulating markers of inflammation in individuals with DM2. | Four familiarization sessions. Evaluation of HR and SPE during, and blood collection before, after, and 1 h after, training 4 h after eating. | Bicycle | HIIT | 19 | 4 min warm-up at 30 W 7 × 1 min at 85% Wmax × 1 min rest at 15%, with 1 min recovery |
| Francois et al., 2015 [13] | To examine the effect of a single resistance interval aerobic exercise session compared to an equivalent control on endothelial function in untrained and normoglycemic trained participants with DM2. | Six familiarization sessions. Standardized diet 4 h before. Collection: pre, 5 min, 1 h, 2 h post. Collection of flow-mediated dilatation (endothelial function) by ultrasound: 1 min pre, 30 s before dilatation, 3 min during. | Bicycle and three resistance exercises for lower limbs | CYCLE ERGOMETER HIIT RESISTED HIIT CONT | 14 14 0 | CYCLE ERGOMETER HIIT: 7 × 1 min at 85% VO2 max. × 1′ recovery 15%. RESISTED HIIT: 7 × 1 min, in a maximum number of repetitions, of six-legged exercises. CONT: 20 min seated. |
| Jayawardene et al., 2017 [17] | Examine the effectiveness of a closed-loop system to prevent hypoglycemia and maintain glucose in the target range for adults with type 1 diabetes performing HIIT vs. CMIT, and secondarily investigate exercise-related metabolic changes in blood glucose, ketones, and lactate during the cycle, and to evaluate the association of changes in these parameters with changes observed in the levels of counterregulatory hormones. | 1 to 4 weeks between workouts, standardized breakfast. | Bicycle | HIIT CMIT | 45 | 5 min warm-up at 25% VO2 max.; HIIT: 6 × 4 min between AT and VO2 max., 2 min rest CMIT: 40 min at 70% of AT |
| Karstoft et al., 2014 [18] | Determine the effect of an interval walking session vs. a continuous walking session equivalent in time and oxygen consumption for glycemic control in subjects with DM2. | 1–2 weeks of familiarization. Pause on anti-diabetes medication, exercise, and alcohol. Online food reminder. Blood for glucose and lactate—using HIIT, before, during and after. Using CMIT: (every 15 min). Borg scale and HR. After: 4 h glucose tolerance test, continuous monitoring 32 h after. | Treadmill | HIIT CMIT CONT | 60 | HIIT: 3 min at 54% and 3 min at 89% VO2 max.; CMIT: 73% of VO2 max.; CONT: seated. |
| Karstoft et al., 2016 [19] | Compare the acute effects of interval exercise vs. continuous equivalents in time and oxygen consumption in EPOC, rate substrate oxidation, and lipid metabolism in the hours following exercise in subjects with DM2. | 1–2 weeks between tests, 24 h food recall. Direct calorimetry 30′ post-training, and indirect calorimetry for 4 h post. Blood collection before, during, and after, urine 2× | Treadmill | HIIT CMIT CONT | 60 | HIIT: 3 min at 54% and 3 min at 89% of VO2 max.; CMIT: 73% of VO2 max.; CONT: seated. |
| Mendes et al., 2019 [20] | Compare the acute effects of HIIT vs. CMIT on glycemic control in middle-aged and elderly patients with DM2. | Standardized breakfast, 1 week between sessions, postprandial. Capillary blood glucose in the ear, pre, every 10′ and post. Capillary glucose before, during (every 10′), and up to 50 min after (50, 60, 70, 80, and 90). | Treadmill | HIIT CMIT CONT | 40 | 5 min of warm-up HIIT: 5 × 3 min at 70% HRR + 3 min at 30%, 5 min cool down; CMIT: 30 min at 50% HRR, 5 min cool-down; CONT: seated. |
| Mendes et al., 2013 [21] | To analyze the acute effects of HIIT on postprandial glucose levels in DM2 patients. | After breakfast. Collection: resting blood glucose, 0 min before, 10, 20, 30 min during, immediately after, and in recovery 50, 60, 70, 80, and 90. total 11×. | Treadmill | HIIT | 40 | 5 min of warm-up 5 × 3-min walk 70% HRR, × 3 min at 30%, 5 min cool-down. |
| Metcalfe et al., 2018 [22] | To examine the effect of a single session of high-intensity, reduced-effort interval training (REHIT) on 24 h blood glucose in men with DM2 compared to a no-exercise control using continuous glucose monitoring. | Standardized diet, continuous 24 h glucose monitoring. | Bicycle | HIIT REHIT CMIT CONT | 25 10 30 0 | HIIT: 25 min, 10 × 1 min at ~90% HRM; REHIT: 10 min − 2 × 20 s all-out sprints in min 2′40 and 6′40. CMIT: 30 min at 50% HRM; CONT: no exercise; |
| Rooijackers et al., 2017 [23] | To investigate the effect of HIIT on hyperglycemic symptoms, counterregulatory hormone response, and cognitive function during subsequent hypoglycemia in patients with DM1 and normal awareness of hypoglycemia (NAH) and impaired awareness of hypoglycemia (IAH), but also in healthy participants. | Cognitive function test 15 min after hypoglycemia (attention and memory; verbal fluency; information processing speed). Symptom score and glycemia; 20.40, and 60 min hypoglycemia. | Bicycle | HIIT | 15 | 4 min warm-up at 50 w; 3 × 30 s sprint (as fast as possible); 4 min recovery at 50 W. |
| Santiago et al., 2017 [24] | To compare acute glycemic and pressure responses of continuous aerobic exercise with interval aerobic exercise in patients with DM2. | Blood glucose and BP collection: pre, immediately post, 5, 10, 15, 20, 25, 30 min. Food control. | Treadmill | HIIT CMIT | 45 35 | HIIT: 45 min, 9 × 5 min (4 min 85–90% AT + 1 min < 85% AI); CMIT: 35 min between 85 and 90% HR of AI. |
| Scott et al., 2019 [25] | Compare the effects of a single session of HIIT with a session of CMIT on glucose concentrations in the subsequent period of 24 h. | Standardized diet with 3 meals, 3-day food recall, continuous monitoring of glucose in the abdomen 24 h. Fasting training. Pre and post glucose. | Bicycle | HIIT CMIT CONT | 17 30 0 | 5 min warm-up at 50 W; HIT: 17 min, 6 × 1 min at 100% VO2 max. × 1 min rest; CMIT: 30 min at 65%. VO2 max.; CONT: no exercise. |
| Viana et al., 2019 [26] | Test the hypothesis that (1) SPE is as efficient a tool as HR relative to cardiopulmonary testing to guide and self-regulate HIIT; (2) metabolic and hemodynamic responses of HIIT are superior to CMIT, regardless of whether suggested and regulated by SPE or HR relative to the cardiopulmonary test. | Blood glucose, HR, BP, femoral pulse velocity. and endothelial reactivity before, after, and 45 min after. | Treadmill | HIIT SPE HIIT HR CMIT CONT | 25 25 30 0 | 4 min warm-up to 9 SPE or 50% HRR; HIIT SPE: 25 min, 21 min being 1 min at 15–17 SPE + 2 min at 9–11 SPE; HIIT HR: 25 min, 21 min being 1 min at 85% HRR + 2 min at 50%; CMIT: 30 min, 26 min at 11–14 SPE; CONT: 30 min seated. |
| Gillen et al., 2012 [27] | Examine the glycemic response 24 h after a HIIT session consisting of cycling efforts of 10 × 60 s at ~90% of HRM, interspersed with 60 s of rest. | Continuous monitoring of glucose 24 h, standardized diet, training 1.5 h after breakfast. Collection: 24 h glucose mean, hyperglycemia time, 3 h post-eating, glucose peak, and postprandial mean 60 min to 120 min. | Bicycle | HIIT | 25 | 3 min warm-up at 50 W; 10 × 1 min at 90% of HRM and 60 s rest; 2 min back to calm at 50 W. |
| Terada et al., 2016 [28] | To compare the acute glycemic response of a HIIT and CMIT session performed under fasting and postprandial conditions. | 24 h continuous monitoring of blood glucose, 48 h between workouts. 24 h average, postprandial, fasting, nocturnal, variability, and time in hypoglycemia and hyperglycemia. | Treadmill | HIIT fasting HIIT with coffee CMIT fasting CMIT with coffee CONT | 60 | HIIT: 3 min at 40% + 1 min at 100% of VO2 max. (15×); CMIT: 55% of VO2 max. CONT: no exercise. |
| Author/Year | Results |
|---|---|
| Durrer et al., 2017 [16] | HIIT reduces TLR2 expression after and 1 h after exercise in DM2 and normoglycemics. |
| Francois et al., 2015 [13] | HIIT resistance exercise is efficient to improve the endothelial function of DM2 in trained and sedentary normoglycemics. |
| Jayawardene et al., 2017 [17] | HIIT resulted in higher glycemic levels and greater hyperglycemic exposure than CMIT during training. There was a greater increase in ketone levels in HIIT than in CMIT. Elevation of counterregulatory hormones (epinephrine, norepinephrine, and cortisol). GH and glucagon did not change. |
| Karstoft et al., 2014 [18] | HIIT improves postprandial glycemic control in DM2 compared to CMIT. |
| Karstoft et al., 2016 [19] | EPOC was higher after HIIT compared to CMIT. Lipid, carbohydrate, and protein oxidation did not differ. HR, SPE, and VO2 were similar. Lactate was higher at HIIT. Lipid oxidation increases during and after exercise in DM2, but with no difference between protocols. |
| Mendes et al., 2019 [20] | Both workouts reduced blood glucose during exercise and within 50 min of recovery. The effect of HIIT was greater than that of CMIT. |
| Mendes et al., 2013 [21] | Capillary blood glucose significantly different at 20, 30, 40 min during, and 50 min after exercise. HIIT appears to be an effective and safe strategy for acute glucose control in DM2 patients. |
| Metcalfe et al., 2018 [22] | Hyperglycemia time was reduced in all protocols, being more expressive in HIIT. CMIT promoted the greatest beneficial effect on the 24 h profile. REHIT reduced the mean 24 h glucose and the prevalence of hyperglycemia compared to the control. REHIT may offer an efficient option to improve the glycemic profile in males with DM2. |
| Rooijackers et al., 2017 [23] | HIIT reduced symptoms of hypoglycemia in normotensive individuals, but not in healthy or hypertensive individuals. HIIT attenuated the cognitive dysfunction induced by hypoglycemia. |
| Santiago et al., 2017 [24] | Blood glucose reduced immediately after and during recovery in both protocols, being more expressive in CMIT. SBP reduced in both, with greater reduction within 30 min of recovery. Both were effective in reducing blood glucose and acute blood pressure in patients with DM2. |
| Scott et al., 2019 [25] | There was no difference between HIIT and CMIT in the 24 h glycemic profile. Fasting training did not increase the incidence of 24 h or nocturnal hypoglycemia. Stable glycemic control during training. |
| Viana et al., 2019 [26] | HIIT was more effective than CMIT in lowering blood glucose regardless of which was used. Only HIIT SPE reduced BP 24 h. |
| Gillen et al., 2012 [27] | There was a reduction in mean glucose 24 h, hyperglycemia time, 3 h after eating, peak glucose, and mean postprandial 60 min to 120 min after HIIT. HIIT promotes improved glycemic control in people with DM2. |
| Terada et al., 2016 [28] | Fasting exercise reduced postprandial blood glucose more than after breakfast. HIIT promoted a greater reduction in nocturnal and fasting blood glucose than CMIT. Compared to control, fasting, HIIT improved glycemic parameters. There was no increased risk of hypoglycemia. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Oliveira Teles, G.; da Silva, C.S.; Rezende, V.R.; Rebelo, A.C.S. Acute Effects of High-Intensity Interval Training on Diabetes Mellitus: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 7049. https://doi.org/10.3390/ijerph19127049
de Oliveira Teles G, da Silva CS, Rezende VR, Rebelo ACS. Acute Effects of High-Intensity Interval Training on Diabetes Mellitus: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(12):7049. https://doi.org/10.3390/ijerph19127049
Chicago/Turabian Stylede Oliveira Teles, Gabriela, Carini Silva da Silva, Vinicius Ramos Rezende, and Ana Cristina Silva Rebelo. 2022. "Acute Effects of High-Intensity Interval Training on Diabetes Mellitus: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 12: 7049. https://doi.org/10.3390/ijerph19127049
APA Stylede Oliveira Teles, G., da Silva, C. S., Rezende, V. R., & Rebelo, A. C. S. (2022). Acute Effects of High-Intensity Interval Training on Diabetes Mellitus: A Systematic Review. International Journal of Environmental Research and Public Health, 19(12), 7049. https://doi.org/10.3390/ijerph19127049