Abstract
Background: The United Nations predicts that the global population aged 65 years or above will double from 703 million in 2019 to 1.5 billion by 2050. In Malaysia, the older population has reached 2.4 million, accounting for nearly 8% of the population. This study aimed to evaluate the perceptions of the elderly on the importance and availability of the age-friendly features in eight domains specified by the Global Network of Age-Friendly City and Communities. Methods: This was a cross-sectional study conducted by structured face-to-face and or telephone interviews. Gap score analysis was performed for 32 items of the 8 age-friendly domains. The gap scores were categorized as follows: 0 = not important OR important and element available; 1 = important but unsure whether the element is available; 2 = important but element not available. The gap scores were then dichotomized into “yes” and “no”, and multivariate logistic regression analysis was subsequently performed. Results: From the 1061 respondents, the housing (55.4%) and transportation (50.7%) domains reported the highest mean perceived gap scores. Out of the 32 elements, the highest mean gap percent scores were observed in elderly priority parking bays (83.8%), home visits by healthcare professionals (78.9%), financial assistance for home modification and purchase (66.3%), and affordable housing options (63.6%). Respondents in the city center reported higher gap scores for modified restrooms, parks, volunteer activities, and the internet; respondents in the non-city center reported higher gap scores for nursing homes, healthcare professionals, and cultural celebrations. Age, location, marital status, income, duration of stay, physical exercise, internet access, and intention to continue working were found to be associated with a higher perceived gap in specific domains. Conclusion: The most significant unmet needs were detected in the housing, transportation, and employment opportunities domains. Considerable disparities in the perceived gap were detected between the older population in the city center and non-city center. To address shortcomings in the local age-friendly setting, coordinated municipal policies, political commitment, and benchmarking of existing age-friendly cities are warranted.
1. Introduction
The United Nations predicts that the global population aged 65 years or more will double from 703 million (9%) in 2019 to 1.5 billion (16%) by 2050 [1]. Malaysia is not exempted from the ageing population issue. The population aged 65 years and above reached 2.41 million in March 2021, accounting for approximately 8% of the Malaysian population [2]. The rate is on an increasing trend, and it is estimated to reach 20% of the population by 2056 [3].
In view of the rapid growth of aging population globally, the World Health Organization (WHO) took an initiative to improve the living environment for the elderly by launching the “Age-friendly Cities” program in 2005. According to the WHO initiative, an “age-friendly” city is one that encourages active aging; it maximizes possibilities for health, involvement, and security in order to improve people’s quality of life as they age [4]. In this program, a guide describes 8 main features of age-friendly living, namely housing, outdoor spaces, and buildings; transportation; job opportunities and civic participation; social participation; respect and social inclusion; communication and information; and community support and health services. It is published as an assessment tool for cities that have joined the WHO Global Network of Age-Friendly Cities and Communities (GNAFCC). Membership in the network does not imply age-friendliness. Rather, it represents cities’ dedication to listening to the needs of ageing populations, assessing and monitoring age-friendliness features, and collaborating across sectors and with older people to develop age-friendly physical and social settings, and the commitment to share one’s experience, accomplishments, and lessons learned with other cities and communities [5]. The establishment of an age-friendly city benefits not only the elderly but also all generations, whereby it enables citizens to be active and connected, which in turn generates growth in the economic, social, and cultural sector of a community [6].
Given the benefits of forming age-friendly cities and the fact that the population of Malaysia is aging, it is important for the Malaysian government to work toward formulating age-friendly cities. By far, in Malaysia, only Ipoh and Taiping city are members of GNAFCC. In particular, 16.7% out of 739,700 people in Ipoh city are more than 60 years of age [6]. While there are no preliminary data on Ipoh city that fulfils criteria for an age-friendly city, this study aims to evaluate the baseline characteristics of these 8 domains, namely housing, outdoor spaces and buildings, transportation, job opportunities and civic participation, social participation, respect and social inclusion, communication and information, and community support and health services in Ipoh city by exploring the perceptions of the elderly residing in Ipoh city on the importance, availability, and the perceived gap of the features specified under each domain to determine if Ipoh is an age-friendly city.
2. Materials and Methods
2.1. Study Design
This cross-sectional study was conducted from April to August 2021 by structured face-to-face or telephone interviews in the Ipoh City of Perak State, Malaysia. Cross-sectional study design was employed, as it is typical for population-based surveys, allowing estimation of prevalence and establishing association, which is appropriate for prompt public health planning, assessment and informing policies [7,8].
2.2. Study Population
We included older adults who are aged 60 and above, had lived in Ipoh for at least 6 months either continuously or intermittently, and could converse in Malay, English, Chinese, or Tamil. We excluded those who did not consent or were physically or mentally unfit to participate in the survey.
Participants were conveniently sampled at public hospitals, health clinics, recreational parks, and other public locations. The sample size was determined using a sample size calculator for estimation based on the formula to estimate a proportion with finite population correction and using a value of 0.5 (50%) as the desired proportion to be estimated [9]. Using an estimated total population aged ≥60 of 113,729 and a precision of 0.03, a total of 1068 samples were required for the survey.
2.3. Study Instrument
We adapted the English version of the AARP Livable Communities—Great Places for All Ages Survey Questionnaire. It contained eight domains of a WHO age-friendly city: (D1) housing, (D2) outdoor spaces and buildings, (D3) transportation, (D4) health and wellness, (D5) social participation, (D6) volunteering and civic engagement, (D7) job opportunities, and (D8) communication and information.
Content validity and face validity were established through meetings with the state geriatrician, the Ipoh City Council and Perak State Health Department representatives. Content modifications were made to some of the items, such as types of homes, medical emergency response systems, and snow removal, in order to suit the local context. Questions on spoken languages, political views of participants, and season-related questions in the original questionnaire were removed.
Then, pre-tests were conducted to test the Malay, Chinese, and Tamil versions of the questionnaire involving representatives of both health and non-health staff. Minor amendments were made based on the suggestions and the English version of the questionnaire was finalized by the research team. The modified questionnaire underwent a translation process from English into Malay, Chinese, and Tamil following an internationally accepted translation standard [10,11,12]. The forward translation was carried out individually by one subject matter expert and one layperson, and the work was reconciled and finalized after a discussion session. It was then back-translated into English by two independent laypersons with a proficient command of English. Subsequently, we pre-tested the three sets of the questionnaire for each language among community elderly members. The questionnaire was further modified and finalized based on the findings.
The finalized questionnaires contained two main sections (i) demographic characteristics (22 items) and (ii) availability and importance of the age-friendly components in the 8 domains (30 items). Participants rated the availability of the age-friendly elements on a 3-point scale: yes, no, not sure; the importance of each element on a 3-point scale: important, not important, not sure (Supplementary Material).
2.4. Data Collection
Three pairs of data collectors were trained by the investigators in a one-day training session supplemented by a printed manual. Written or verbal consent was obtained from the subject before the interview began, for face-to-face and telephone interviews, respectively. Responses were recorded into the printed questionnaire by the data collectors and subsequently transcribed into the RedCap electronic data collection form.
2.5. Data Analysis
The data, initially entered in RedCap, were exported and analyzed using the Statistical Package for Social Sciences (SPSS) version 20.0. The data were analyzed descriptively with frequencies and percentages (Table S1), while gap score analysis was performed for 32 items of the 8 age-friendly domains. The gap scores were generated by comparing the importance and availability scores (10). The gap scores were categorized as follow: 0 = not important OR important and element available; 1 = important but unsure whether the element is available; 2 = important but element not available in Ipoh (Figure 1 and Table S2). Responses with unsure importance or missing data were not included into the gap score analysis. The gap score was then dichotomized into “yes” and “no”. Subsequently, univariate binary logistic regression analysis was performed (Table S3). Variables with p-values < 0.25 were included into the multivariate binary logistic regression model. Adjusted odds ratio (AOR) with 95% confidence interval were presented.
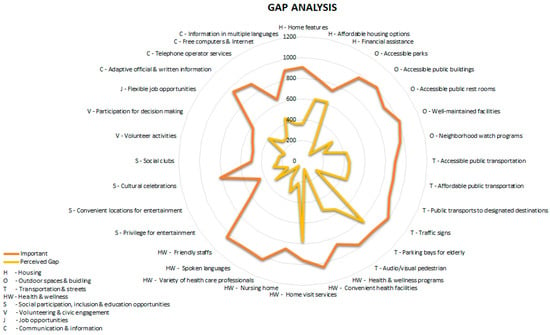
Figure 1.
Distribution of the perceived gap in the elements of eight age-friendly domains.
The respondents were grouped into two sub-areas (city center and non-city center). Based on the Ipoh City Council mapping, Ipoh city was divided into five administrative zones. The only zone with a population of more than 10,000 was categorized as the city center, while the four remaining zones with a population of less than 10,000 were categorized as non-city center [13]. Demographic characteristics and gap scores of older people living in the city center and non-city center were further presented in sub-group analyses.
The individual item mean gap score was generated by dividing the total number of subjects with the perceived gap scores by the total number of valid responses for that item and multiplying them by 100. The domain gap scores were generated by summing the item mean gap scores and dividing by the total number of items in the particular domain.
3. Results
3.1. Demographic Characteristics
A total of 1061 usable responses were included in the final analysis after excluding 7 incomplete questionnaires. Overall, the majority of respondents were comprised of those aged between 60 and 70 (677, 63.8%), females (556, 52.4%), with secondary education (517, 48.7%), living with at least one companion (990, 93.3%), declaring a monthly income of less than RM 2000 (931, 87.7%), staying in Ipoh for more than 60 years (503, 47.4%), and not working (865, 81.5%). About half of the respondents stayed in the city center (533, 50.2%), while the other half stayed in the non-city center (49.8%). The socio-demographic characteristics did not differ between the city center and non-city center respondents, except their age (p = 0.006) and health conditions (p = 0.001) (Table 1).

Table 1.
Socio-demographic characteristics of the respondents in city center and non-city center of Ipoh (n = 1061).
3.2. Perceived Gap Scores
Of the 8 domains, housing (55.4%, D1) and transportation (50.7%, D3) reported the highest mean perceived gap scores. Out of the 32 elements, the highest mean gap percent scores were observed in elderly priority parking bays (83.8%), home visits by healthcare professionals (78.9%), financial assistance for home modification and purchase (66.3%), and affordable housing options (63.6%) (Table 2).
Table 2.
Mean gap percent scores of the WHO AFC items and domains in city center and non-city center.
The mean percent gap scores were compared between the city center and non-city center respondents. Significantly higher gap scores were observed among the city center respondents in 4 elements, including modified rest-rooms for people with disabilities (40.3% in the city center vs. 30.0% in non-city center, D2, p = 0.001); well-maintained parks and facilities (26.8% vs. 16.5%, D2, p < 0.001), a range of volunteer activities (29.9% vs. 22.2%, D6, p = 0.009) and free access to computers and the internet (56.0% vs. 49.0%, D8, p = 0.039). In contrast, respondents in the non-city center reported a significantly higher mean gap percent score in nursing homes for older people (28.3% in the non-city center vs. 16.4% in the city center, D5, p < 0.001), a variety of healthcare professionals (34.7% vs. 27.2%, D5, p = 0.009) and the variety of cultural celebrations (35.9% vs. 24.0%, D5, p < 0.001) (Table 2).
3.3. Multivariate Binary Logistic Regressions
For the housing domain (D1), those who were aged 81 and above had significantly lower odds of a perceived gap (OR: 0.54; CI: 0.31–0.93), while those who actively exercised (5–7 times weekly) (OR: 1.53, CI: 1.01–2.33) and had internet access (OR: 1.50, CI: 1.10–2.04) tended to have a higher perceived gap. In terms of outdoor spaces/buildings (D2) and transportation (D3), those who have lived in Ipoh for more than 60 years have a higher perceived gap. Participants who lived in Ipoh between 11 and 30 years (OR: 2.89, CI: 1.30–6.40) and more than 60 years (OR: 2.34, CI: 1.15–4.77) reported a higher perceived gap in health and wellness (D4).
In the aspect of social participation (D5), those living outside of the city center (OR: 1.38, CI: 1.07–1.79), earning more than RM 4800 per month (OR: 2.98, CI: 1.11–8.01) and having access to the internet (OR: 1.36, CI: 1.04–1.77) were associated with higher odds of perceived gaps. As for the volunteering and civic engagement domain (D6), those in the non-city center who have lived in Ipoh for more than 60 years (OR: 0.71, CI: 0.53–0.94) and with no intention of continuing working (OR: 0.69, CI: 0.49–0.95) reported a lower gap score, while those with access to the internet reported a higher gap score (OR: 1.64, CI: 1.23–2.19). Those with moderate (OR: 1.68, CI: 1.06–2.67) and higher incomes(OR: 3.20, CI: 1.30–7.84), as well as those who have access to the internet (OR: 1.50, CI: 1.14–1.98), have a larger perceived gap in the domain of job opportunities (D7), while those who exercise regularly (OR: 0.67, CI: 0.46–0.99) have lower expectations in this respect. In terms of community information (D8), a higher gap score was seen in those unmarried (OR: 1.66, CI: 1.13–2.45) and those with access to the internet (OR: 1.39, CI: 1.04–1.85) (Figure 2).
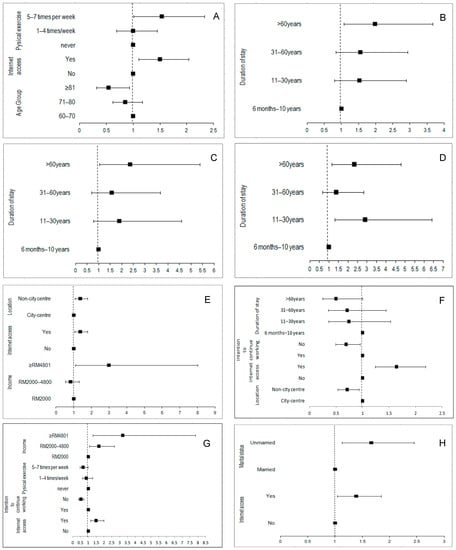
Figure 2.
Multivariate binary logistic regressions assessing significant factors associated with presence of perceived gap on the eight age-friendly domains. (A) Housing, (B) outdoor spaces and buildings, (C) transportation, (D) health and wellness, (E) social participation, (F) volunteering and civic engagement, (G) job opportunities, (H) community and information.
4. Discussion
Out of eight domains, housing recorded the highest perceived gap, with a substantial gap existing in affordable housing options and financial assistance for either house renovation or purchase. According to the WHO, housing contributes to a range of positive health outcomes, particularly in the older population [14]. Housing affordability is a major concern for older people, especially vulnerable individuals with low incomes [15,16]. In European countries, the provision of housing subsidies was proposed to relieve the impact of housing costs on aging in place, which restricts one’s capacity to pay for other essentials [17]. Meanwhile, simple housing modifications such as installing lighting and grab bars in the bathrooms have been found to improve daily activity performance and mental health [18]. Locally, there are limited policies to protect the rights of senior citizens in housing options. Moreover, both public and private housing developers rarely provide affordable housing options for the aged [19]. Additionally, the concepts for older individuals such as co-housing, group living, or reconstruction of deserted vacant houses that may be instrumental for the aging population are yet to be popularised in this country [20]. The current housing financial support program by the government, such as the My First Home Scheme, could be expanded to cover housing modifications and house purchases for older adults [21].
We observed a notable need in transportation in terms of accessibility, cost, and availability of public transport to key destinations for older individuals, which is incongruent with developed European nations where it is evident that older adults are particularly vulnerable to transportation barriers [22]. Although the Malaysian government offered senior citizens a public transportation discount [23], the gap in the basic features of transportation remained significant. This may be related to the issues associated with health and mobility limitations [24]. In addition, public transportation in Ipoh city relies on a fixed route system, where passengers must travel along designated routes with predetermined schedules and designated pickup and drop-off stations [25]. Ergonomic improvement of public transport, addressing the physical challenges associated with boarding and alighting buses or terminals, covering the distance between stops and houses, may encourage older individuals to use public transportation [26]. Flexible transport services are gradually integrated into the UK, European, and American public transport systems to complement the traditional routes covered by small buses, minibuses, or maxi-taxis [27]. Flexible transport services employed interactive booking and reservation systems which could dynamically assign passengers to vacant vehicles and optimizes the routes [28].
Parking difficulties among the elderly are similar to those faced in other countries irrespective of socio-economic development. That is, the need for priority parking bays for senior citizens in close proximity to destinations, drop-off, and pick-up bays, with adequate space for them to get in and out of a car without obstruction, has been raised. Dedicated cycling and walking lanes distanced from car lanes [20], supplemented with audio or visual pedestrian crossings, should be considered to enhance the walkability and age-friendliness of the neighbourhood in future town-planning.
It is unsurprising that our respondents reported a relatively lower overall perceived gap in the healthcare domain, as there is a large network of government-funded primary care clinics and hospitals [29]. However, in congruence to previous findings, older individuals in non-city centers faced greater difficulties in accessing healthcare compared to their city center counterparts, and both reported remarkable perceived gaps in terms of home visit service [30]. The growing number of disabled older people with comorbidities necessitates the expansion of home health care services, which have been shown to reduce mortality and hospitalisation [30,31]. For instance, the Japanese government has promoted physician-led home-visit care for frail and disabled people [31] and such services, yet to be expanded to geriatric patients in this country, can be first considered for implementation in an ageing city like Ipoh.
The gap score was reported to be significantly higher in specialized care and nursing homes for the aged who reside in non-city center areas than those in the city center. The majority of specialist facilities needed by the elderly are placed in the city center [32,33]. Increased funding for geriatric specialist training may be necessary to meet the needs of older adults, particularly those who live outside of city centers. Despite the Malaysian Department of Social Welfare offering long-term care residences for dependent people who have no family support [29], nursing homes in Malaysia are still in short supply [34]. This disparity in nursing home availability and distribution, as suggested by this study, warrants the urgent attention of the welfare department to tackle this problem by providing incentives to nursing homes set up in non-city centers in Ipoh.
Senior citizens living in Ipoh city centers perceive greater barriers to accessing public restrooms and well-maintained parks as compared to their non-city center counterparts. Outdoor space has a significant effect on older adults’ mobility, independence, and emotional and psychological well-being, all of which are factors that influence the quality of life [35,36]. The use of outdoor spaces was strongly influenced by aesthetic features, practical components such as restrooms, and park maintenance [35]. Clean, safe, and accessible public toilets are important for older adults, particularly those with incontinence. Improving the accessibility and safety of parks, for instance, using wide and flat-surfaced pavements separated from cyclists, may promote physical activity among older adults [20]. To preserve outdoor spaces, a multifaceted approach should be taken, including increased budget allocation, integration of age-friendly outdoor features into local city council town-planning policy, collaboration among public and private stakeholders, and public awareness campaigns [37].
Two-fifths of our respondents reported perceived gaps in job opportunities, and this was more likely among seniors with moderate to higher incomes after controlling for demographic characteristics. Employment is crucial for the elderly’s financial well-being since it offers both a source of income and, in certain cases, benefits such as pensions and health insurance [38]. A Dutch study revealed that managers were unlikely to re-employ older employees after mandatory retirement, and re-employment of those who were willing to accept a lower salary was favoured [39]. Measures should be taken to reduce discrimination against older people, re-training and upgrading their skill sets, providing special working arrangements and revising the legal framework to increase older workers’ employment opportunities [40,41].
The lack of employment prospects may result in financial and economic volatility. While the state has the largest resources, a paradigm shift is difficult, as administrators are geared towards bureaucracy rather than implementing new policies. Hence, the government should take precautionary actions in the realm of social protection through revision of the tax system and tapping into existing private capacity to complement current public resources [42]. Meanwhile, individuals’ demands for social safety, self-protection skills and resilience should be understood and addressed through social inclusion policies. Better protection of the most vulnerable allows society to maximize existing capacities without duplicating efforts, resulting in a better alleviation of social anxiety. Recognising vulnerabilities produces synergies between state social protection and social policies, leading to innovative interventions and reorienting social protection [43].
Gap scores were relatively lower in social participation as compared to other domains. Yet, it is an important domain in developing community vitality, promoting physical and mental health, avoiding disabilities [44], and reducing the risk of death and dementia [45]. The importance of social participation should be promoted to older adults. The lack of variety in cultural celebrations and social clubs for hobbies was significantly raised by the non-city center respondents as compared to those in the city center. Social activities that are primarily organized in the city center pose considerable challenges for the participation of elderly who live in areas outside of the city center. A study shows that the main factors driving participation in social activity in older adults are easy access and being informed about transportation options [44]. Most social events could be fixed at the city center due to the consideration of available facilities. The organizers could always make an effort by arranging public transport service for cultural events, and providing priority parking and drop-off bays for senior citizens, and ensure that the information is clearly stated in the promotion advertisement. A senior center that organizes health programs and volunteering activities such as clubs for hobbies, educational courses, and exercise classes is suggested as a measure to increase social interaction among senior citizens [45]. The currently available senior center concept in Ipoh is limited and mainly located at the city center [46,47]. Nevertheless, prior to implementing any interventions prioritizing the needs of senior citizens in non-city center areas, in-depth studies are needed to determine the proximity of the elderly to the facilities, caregivers’ support, transportation, neighborhood security, and user-friendliness of the walking environment [48].
Respondents who have been staying for more than 60 years in non-city centers with no intention of continuing working, perceive a lesser need for civic engagement. In spite of the lesser interest in this domain, engagement in civic activities is proven to reduce mortality rates and encourage the elderly to stay healthy as it is associated with making oneself feel useful and responsible to others, continuing working on personal growth and development instead of receiving instrumental help [49,50]. The benefits of taking part in volunteering activities should be actively promoted to older adults while at the same time adequately addressing the aspects of accessibility, expectations, information, incentives, and facilitation, that in turn would foster the participation of the aged population in civic activities [51].
A perceived gap in communication and information was identified among those who were unmarried and had internet access. The use of the internet for communication could help to reduce social isolation, loneliness, and depression, and enhance social support in the elderly [52]. Even though respondents have access to the internet, which can be used for communication and information, their needs for this domain remained unfulfilled, suggesting that other aspects such as technology infrastructure, internet speed and coverage, digital divide, or a preference for face-to-face communication could be further researched. Another possible reason for this observation could be attributed to the greater need of single people for internet assessment to achieve a higher level of social capital [53]. Evidence shows that being single or a frequent internet user in older populations is associated with higher levels of social capital, and this is important to maintain good health and wellbeing [54].
Roughly half of the respondents, disregarding their geographical location, expressed a significant need for free device and internet access. Unaffordability of devices and internet access among the elderly is not uncommon, and this problem happens even in developed countries, such as the UK. Inequality in the digital divide, and the distribution of technological infrastructure reduce internet access for residents living in different locations, affecting all age groups and resulting in digital poverty [20,55]. A slightly lower gap score rated in the need for free devices and internet access by respondents in the non-city center could be explained by the continuous effort of the Malaysian government to increase internet access for residents in the non-city center area. This has been reflected in allocating funds in the eighth and ninth Malaysia plans and in setting up telecenters in the rural community by establishing facilities for the internet and computer training rooms for use by the rural community [56].
Strength and Limitations
To the best of our knowledge, this is the first study in the Malaysian context that evaluates a city’s age friendliness. This study surveyed the population of older adults that were distributed equally in the city and outside the city area in Ipoh. The findings served as a baseline input for local city councils to make improvements to Ipoh city not only to meet the benchmark of GNAFCC but also to plan for short- and long-term intervention in creating an age-friendly environment. In the global context, the information from this study adds knowledge to existing aging research that allows researchers to make comparisons among the age-friendly cities. Studies with comparable methodology may be replicated in other countries to validate the findings in future.
Convenient and snowball sampling methods may not encompass all social-economic groups of older populations in Ipoh. Sampling was not stratified based on city center and non-city center, thus sample size may not be adequately powered for the subgroup analyses. Nonetheless, the study analysis shows that the distributions of demographic characteristics were not significantly different between those who stayed in the city center and those who did not. The differences in the need for an age-friendly between the two groups can thus be compared, and this allows policymakers to identify and address the inequalities experienced by the aged population, including those residing in the city center or non-city center of Ipoh.
5. Conclusions
Out of the eight domains, the most notable unmet needs were observed in the housing, transportation, and job opportunities domains. Distinct differences in perceived gap were also observed between older populations in the city center and non-city center in six out of the eight domains. A multifaceted approach is recommended to specifically address the unmet needs among older adults in the local context. Public-private housing partnership model could be introduced to revolutionize housing policy and financing assistance scheme to improve house purchase and modifications affordability. Expansion of home visit services is essential to maintain continuity of care for patients who have been discharged, support family members and reduce readmission. Continuation of public transport fare subsidy policy may encourage its usage among older adults. Provision of flexible working arrangements and revision of legislative framework may reduce discrimination and increase job opportunities for older people. On a broader scale, concerted municipal strategies, political commitment, and benchmarking of established age-friendly cities are warranted to address specific gaps in the age-friendly city context.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ijerph19127171/s1, Supplementary material: Study questionnaire. Table S1: Availability and importance of the elements in eight domains of an aged-friendly city in Ipoh city’s perspectives; Table S2: Gap score analysis of the elements in eight domains of an aged-friendly city in Ipoh city’s perspectives; Table S3: Univariate binary logistic regressions assessing demographic characteristics associated with presence of perceived gap on the eight age-friendly domains.
Author Contributions
C.-T.C. and X.-J.L., conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, supervision, writing-original draft, writing-review and editing; P.S., conceptualization, data curation, formal analysis, investigation, methodology, project administration, software, validation, visualization, writing—review and editing; C.-C.C., conceptualization, investigation, methodology, project administration, writing-original draft, writing-review and editing; L.-M.D., conceptualization, funding acquisition, project administration, writing—review and editing; P.R., conceptualization, data curation, funding acquisition, investigation, methodology, project administration, resources, supervision, writing—review and editing. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriate investigated and resolved. All authors have read and agreed to the published version of the manuscript.
Funding
This research is funded by Ministry of Health Malaysia (Warrant Number: 91000782). The authors have full control of the data collected.
Institutional Review Board Statement
This study was registered in the Malaysia National Medical Research Registry (NMRR-19-3191-51748) and obtained the approval of Malaysian Medical Research and Ethics Committee (MREC). We obtained informed consent from all participants prior to collecting their data. All methods were carried out in accordance with relevant guidelines and regulations.
Informed Consent Statement
Patient consent was obtained before conduct of study.
Data Availability Statement
The dataset used in this study can be obtained from the authors upon reasonable requests.
Acknowledgments
We appreciate the administrative support given by the Ipoh City Mayor. We would like to thank the Director General of Health Malaysia for his permission to publish this article. We would like to thank Ms Lina Hashim, Clinical Research Centre, Hospital Raja Permaisuri Bainun for her administrative support in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- United Nations: Department of Economic and Social Affairs: Population Division. World Population Ageing 2019; United Nations: New York, NY, USA, 2020; ISBN 978-92-1-148326-0. [Google Scholar]
- Department of Statistics Malaysia Official Portal. Available online: https://www.dosm.gov.my/v1/index.php?r=column/cthemeByCat&cat=430&bul_id=eGtwdjd4amZJb1JmcFFkYXBKNHg3dz09&menu_id=L0pheU43NWJwRWVSZklWdzQ4TlhUUT09 (accessed on 6 May 2022).
- World Bank Group. A Silver Lining: Productive and Inclusive Aging for Malaysia. Available online: https://www.worldbank.org/en/country/malaysia/publication/a-silver-lining-productive-and-inclusive-aging-for-malaysia (accessed on 6 May 2022).
- World Health Organization. Global Age-Friendly Cities: A Guide; World Health Organization: Paris, France, 2007; ISBN 978-92-4-154730-7. [Google Scholar]
- Flores, R.; Caballer, A.; Alarcón, A. Evaluation of an Age-Friendly City and Its Effect on Life Satisfaction: A Two-Stage Study. IJERPH 2019, 16, 5073. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Age-Friendly World-WHO Global Network. Available online: https://extranet.who.int/agefriendlyworld/?sfid=10015&_sf_s=Malaysia (accessed on 6 May 2022).
- Setia, M. Methodology Series Module 3: Cross-Sectional Studies. Indian J. Derm. 2016, 61, 261. [Google Scholar] [CrossRef] [PubMed]
- Tiraphat, S.; Buntup, D.; Munisamy, M.; Nguyen, T.H.; Yuasa, M.; Nyein Aung, M.; Hpone Myint, A. Age-Friendly Environments in ASEAN Plus Three: Case Studies from Japan, Malaysia, Myanmar, Vietnam, and Thailand. IJERPH 2020, 17, 4523. [Google Scholar] [CrossRef] [PubMed]
- Naing, L.; Winn, T.; Nordin, R. Pratical Issues in Calculating the Sample Size for Prevalence Studies. Arch. Orofac. Sci. 2006, 1, 9–14. [Google Scholar]
- Tsang, S.; Royse, C.; Terkawi, A. Guidelines for Developing, Translating, and Validating a Questionnaire in Perioperative and Pain Medicine. Saudi J. Anaesth 2017, 11, 80. [Google Scholar] [CrossRef]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef]
- World Health Organization Translation_Methodology. Available online: https://www.who.int/nepal/activities/supporting-elimination-of-kala-azar-as-a-public-health-problem/docs/default-source/publishing-policies/whoqol-100-guidelines/translation-methodology (accessed on 6 May 2022).
- Department of Statistics Malaysia. Population Distribution and Basic Demographic Characteristics 2010; Department of Statistics: Putrajaya, Malaysia, 2011; ISBN 978-983-9044-81-2. [Google Scholar]
- World Health Organization. WHO Housing and Health Guidelines; World Health Organization: Geneva, Switzerland, 2018; ISBN 978-92-4-155037-6. [Google Scholar]
- Vega, W.A.; Wallace, S.P. Affordable Housing: A Key Lever to Community Health for Older Americans. Am. J. Public Health 2016, 106, 635–636. [Google Scholar] [CrossRef]
- Fox, S.; Kenny, L.; Day, M.R.; O’Connell, C.; Finnerty, J.; Timmons, S. Exploring the Housing Needs of Older People in Standard and Sheltered Social Housing. Gerontol. Geriatr. Med. 2017, 3, 2333721417702349. [Google Scholar] [CrossRef]
- Lux, M.; Sunega, P. The Impact of Housing Tenure in Supporting Ageing in Place: Exploring the Links between Housing Systems and Housing Options for the Elderly. Eur. J. Hous. Policy 2014, 14, 30–55. [Google Scholar] [CrossRef]
- Szanton, S.L.; Leff, B.; Wolff, J.L.; Roberts, L.; Gitlin, L.N. Home-Based Care Program Reduces Disability and Promotes Aging In Place. Health Aff. 2016, 35, 1558–1563. [Google Scholar] [CrossRef]
- Sulaiman, N.; Baldry, D.; Ruddock, L. Issues Concerning Housing for the Elderly in Malaysia; Research Institute for the Built & Human Environment, University of Salford: Manchester, UK, 2014. [Google Scholar]
- Van Hoof, J.; Marston, H.R.; Kazak, J.K.; Buffel, T. Ten Questions Concerning Age-Friendly Cities and Communities and the Built Environment. Build. Environ. 2021, 199, 107922. [Google Scholar] [CrossRef]
- MyGovernment Public Service Delivery and Local Government: Affordable Home Scheme. Available online: https://www.malaysia.gov.my/portal/content/30704 (accessed on 6 May 2022).
- Shrestha, B.P.; Millonig, A.; Hounsell, N.B.; McDonald, M. Review of Public Transport Needs of Older People in European Context. Popul. Ageing 2017, 10, 343–361. [Google Scholar] [CrossRef] [PubMed]
- MyGovernment Obtaining Facilities, Welfare & Health Care: Senior Citizen Transportation Discount. Available online: https://www.malaysia.gov.my/portal/content/30404 (accessed on 6 May 2022).
- Remillard, E.T.; Campbell, M.L.; Koon, L.M.; Rogers, W.A. Transportation Challenges for Persons Aging with Mobility Disability: Qualitative Insights and Policy Implications. Disabil. Health J. 2021, 15, 101209. [Google Scholar] [CrossRef] [PubMed]
- Bachok, S.; Osman, M.; Ibrahim, M.; Ponrahono, Z. Regenerating Ipoh City Mobility through High Level of Service (LOS) of Public Bus Service. Procedia-Soc. Behav. Sci. 2015, 170, 680–689. [Google Scholar] [CrossRef][Green Version]
- Aceves-González, C.; Cook, S.; May, A. Improving Bus Travel through Inclusive Design Service. In Ergonomics in Design: Methods and Techniques; CRC Press: Boca Raton, FL, USA, 2016; p. 16. ISBN 978-1-4987-6070-6. [Google Scholar]
- Daniels, R.; Mulley, C. Flexible Transport Services: Overcoming Barriers to Implementation in Low-Density Urban Areas. Urban. Policy Res. 2012, 30, 59–76. [Google Scholar] [CrossRef]
- Mulley, C.; Nelson, J.D. Flexible Transport Services: A New Market Opportunity for Public Transport. Res. Transp. Econ. 2009, 25, 39–45. [Google Scholar] [CrossRef]
- Jaafar, S.; Noh, K.M.; Muttalib, K.A.; Othman, N.H.; Healy, J. Malaysia Health System Review; Healy, J., Ed.; WHO: Geneva, Switzerland, 2012; Volume 2, ISBN 978-92-9061-584-2. [Google Scholar]
- Foreman, K.J.; Marquez, N.; Dolgert, A.; Fukutaki, K.; Fullman, N.; McGaughey, M.; Pletcher, M.A.; Smith, A.E.; Tang, K.; Yuan, C.-W.; et al. Forecasting Life Expectancy, Years of Life Lost, and All-Cause and Cause-Specific Mortality for 250 Causes of Death: Reference and Alternative Scenarios for 2016–40 for 195 Countries and Territories. Lancet 2018, 392, 2052–2090. [Google Scholar] [CrossRef]
- Stuck, A.E.; Siu, A.L.; Wieland, G.D.; Rubenstein, L.Z.; Adams, J. Comprehensive Geriatric Assessment: A Meta-Analysis of Controlled Trials. Lancet 1993, 342, 1032–1036. [Google Scholar] [CrossRef]
- Heng Leng, C.; Simon, B. Health Care in Malaysia The Dynamics of Provision, Financing and Access; Routledge: London, UK, 2009; ISBN 978-0-415-54420-7. [Google Scholar]
- Tan, M.P.; Kamaruzzaman, S.B.; Poi, P.J.H. An Analysis of Geriatric Medicine in Malaysia-Riding the Wave of Political Change. Geriatrics 2018, 3, 80. [Google Scholar] [CrossRef]
- Price, R.; Stoneham, J. Making Connections: A Guide to Accessible Greenspace; Sensory Trust: Bath, UK, 2001; ISBN 978-0-9526745-3-5. [Google Scholar]
- Zhang, W.; Yang, J.; Ma, L.; Huang, C. Factors Affecting the Use of Urban Green Spaces for Physical Activities: Views of Young Urban Residents in Beijing. Urban For. Urban Green. 2015, 14, 851–857. [Google Scholar] [CrossRef]
- Kaplan, S.; Talbot, J.F. Psychological Benefits of a Wilderness Experience. In Behavior and the Natural Environment; Altman, I., Wohlwill, J.F., Eds.; Springer: Boston, MA, USA, 1983; pp. 163–203. ISBN 978-1-4613-3541-2. [Google Scholar]
- Hailegiorgis, Y.G. Recreational Parks: Practices and Challenges in Hawassa City. J. Tour. Hosp. 2017, 6. [Google Scholar] [CrossRef]
- Radović-Marković, M. An aging workforce: Employment Opportunities and Obstacles. Cadmus 2013, 1, 142–155. [Google Scholar]
- Oude Mulders, J.; van Dalen, H.P.; Henkens, K.; Schippers, J. How Likely Are Employers to Rehire Older Workers After Mandatory Retirement? A Vignette Study Among Managers. De Econ. 2014, 162, 415–431. [Google Scholar] [CrossRef]
- Naegele, G.; Walker, A. A Guide to Good Practice in Age Management; Office for Official Publication of the European Communities: Luxembourg, 2006; ISBN 978-92-897-0934-7. [Google Scholar]
- Samorodov, A.; Bureau International du Travail, Employment and Training Department. Ageing and Labour Markets for Older Workers; Employment and Training Department, International Labour Office: Genèva, Switzerland, 1999; ISBN 978-92-2-111418-5. [Google Scholar]
- Shaikh, B.; Mazhar, A.; Khan, S.; Hafeez, A. Social Protection Strategies and Health Financing to Safeguard Reproductive Health for the Poor: Making a Case for Pakistan. J. Ayub Med. Coll. Abbottabad. 2013, 23, 126–130. [Google Scholar]
- Adato, M.; Bassett, L. Social Protection to Support Vulnerable Children and Families: The Potential of Cash Transfers to Protect Education, Health and Nutrition. AIDS Care 2009, 21, 60–75. [Google Scholar] [CrossRef]
- Levasseur, M.; Routhier, S.; Clapperton, I.; Doré, C.; Gallagher, F. Social Participation Needs of Older Adults Living in a Rural Regional County Municipality: Toward Reducing Situations of Isolation and Vulnerability. BMC Geriatr. 2020, 20, 456. [Google Scholar] [CrossRef]
- Novek, S.; Menec, V.; Tran, T.; Bell, S. Social Participation and Its Benefits; Centre on Aging, University of Manitoba: Winnipeg, MA, Canada, 2013; p. 84. [Google Scholar]
- MK, T. Ipoh Echo|Senior Citizens Club Perak. Available online: http://www.ipohecho.com.my/v4/article/2016/12/01/senior-citizens-club-perak (accessed on 6 May 2022).
- Loh, I. A Place to Socialise. Available online: https://www.thestar.com.my/metro/community/2015/11/04/a-place-to-socialise-ministry-hopes-to-have-activity-centres-for-senior-citizens-in-each-parliamenta (accessed on 6 May 2022).
- Levasseur, M.; Généreux, M.; Bruneau, J.-F.; Vanasse, A.; Chabot, É.; Beaulac, C.; Bédard, M.-M. Importance of Proximity to Resources, Social Support, Transportation and Neighborhood Security for Mobility and Social Participation in Older Adults: Results from a Scoping Study. BMC Public Health 2015, 15, 503. [Google Scholar] [CrossRef]
- Gottlieb, B.H.; Gillespie, A.A. Volunteerism, Health, and Civic Engagement among Older Adults. Can. J. Aging 2008, 27, 399–406. [Google Scholar] [CrossRef]
- Batista, L.; Cruz-Ledón, A. The Relationship between Civic Engagement and Health among Older Adults. In Proceedings of the South Florida Education Research Conference 2013, Portland, FL, USA, 17–18 July 2013. [Google Scholar]
- McBride, A. Civic Engagement, Older Adults, and Inclusion. Generations 2006, 30, 66–71. [Google Scholar]
- Cotten, S.R.; Ford, G.; Ford, S.; Hale, T.M. Internet Use and Depression among Older Adults. Comput. Hum. Behav. 2012, 28, 496–499. [Google Scholar] [CrossRef]
- Keeley, B. Human Capital: How What You Know Shapes Your Life; OECD Insights; OECD: Paris, France, 2007; ISBN 978-92-64-02908-8. [Google Scholar]
- Neves, B.B.; Fonseca, J.R.S.; Amaro, F.; Pasqualotti, A. Social Capital and Internet Use in an Age-Comparative Perspective with a Focus on Later Life. PLoS ONE 2018, 13, e0192119. [Google Scholar] [CrossRef]
- Organisation for Economic and Co-operation and Development (OECD). Understanding the Digital Divide; OECD Digital Economy Papers; OECD: Paris, France, 2001; Volume 49. [Google Scholar]
- Kamarudin, S.; Omar, S.; Bolong, J.; Osman, M.N.; Mahamed, M. ICT Development of Community in Rural Areas. Acad. Res. Int. 2019, 9, 118–126. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).