
Perceived Gap of Age-Friendliness among Community-Dwelling Older Adults: Findings from Malaysia, a Middle-Income Country

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Study Instrument
2.4. Data Collection
2.5. Data Analysis
3. Results
3.1. Demographic Characteristics
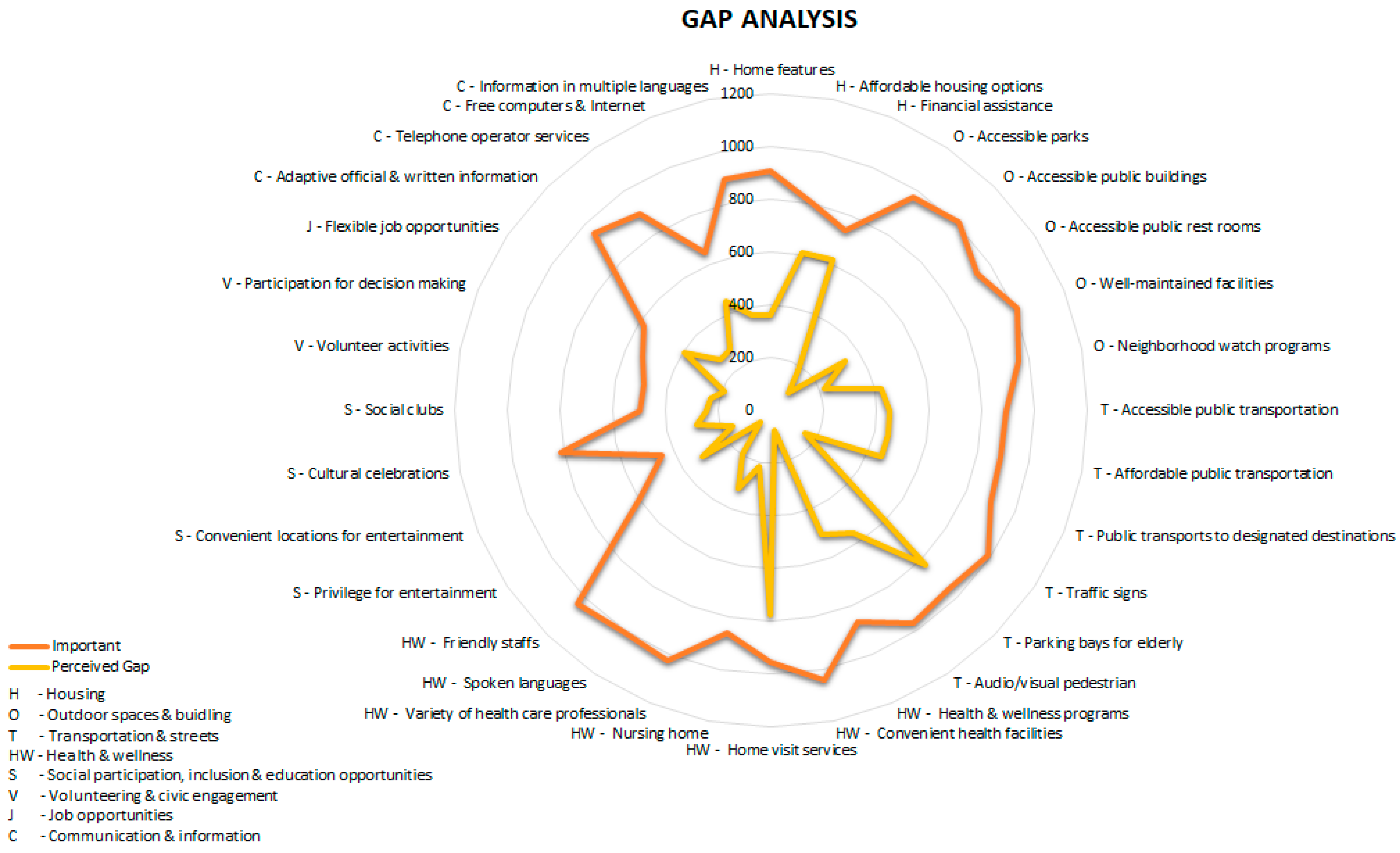
3.2. Perceived Gap Scores
3.3. Multivariate Binary Logistic Regressions
4. Discussion
Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations: Department of Economic and Social Affairs: Population Division. World Population Ageing 2019; United Nations: New York, NY, USA, 2020; ISBN 978-92-1-148326-0. [Google Scholar]
- Department of Statistics Malaysia Official Portal. Available online: https://www.dosm.gov.my/v1/index.php?r=column/cthemeByCat&cat=430&bul_id=eGtwdjd4amZJb1JmcFFkYXBKNHg3dz09&menu_id=L0pheU43NWJwRWVSZklWdzQ4TlhUUT09 (accessed on 6 May 2022).
- World Bank Group. A Silver Lining: Productive and Inclusive Aging for Malaysia. Available online: https://www.worldbank.org/en/country/malaysia/publication/a-silver-lining-productive-and-inclusive-aging-for-malaysia (accessed on 6 May 2022).
- World Health Organization. Global Age-Friendly Cities: A Guide; World Health Organization: Paris, France, 2007; ISBN 978-92-4-154730-7. [Google Scholar]
- Flores, R.; Caballer, A.; Alarcón, A. Evaluation of an Age-Friendly City and Its Effect on Life Satisfaction: A Two-Stage Study. IJERPH 2019, 16, 5073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Age-Friendly World-WHO Global Network. Available online: https://extranet.who.int/agefriendlyworld/?sfid=10015&_sf_s=Malaysia (accessed on 6 May 2022).
- Setia, M. Methodology Series Module 3: Cross-Sectional Studies. Indian J. Derm. 2016, 61, 261. [Google Scholar] [CrossRef] [PubMed]
- Tiraphat, S.; Buntup, D.; Munisamy, M.; Nguyen, T.H.; Yuasa, M.; Nyein Aung, M.; Hpone Myint, A. Age-Friendly Environments in ASEAN Plus Three: Case Studies from Japan, Malaysia, Myanmar, Vietnam, and Thailand. IJERPH 2020, 17, 4523. [Google Scholar] [CrossRef] [PubMed]
- Naing, L.; Winn, T.; Nordin, R. Pratical Issues in Calculating the Sample Size for Prevalence Studies. Arch. Orofac. Sci. 2006, 1, 9–14. [Google Scholar]
- Tsang, S.; Royse, C.; Terkawi, A. Guidelines for Developing, Translating, and Validating a Questionnaire in Perioperative and Pain Medicine. Saudi J. Anaesth 2017, 11, 80. [Google Scholar] [CrossRef]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization Translation_Methodology. Available online: https://www.who.int/nepal/activities/supporting-elimination-of-kala-azar-as-a-public-health-problem/docs/default-source/publishing-policies/whoqol-100-guidelines/translation-methodology (accessed on 6 May 2022).
- Department of Statistics Malaysia. Population Distribution and Basic Demographic Characteristics 2010; Department of Statistics: Putrajaya, Malaysia, 2011; ISBN 978-983-9044-81-2. [Google Scholar]
- World Health Organization. WHO Housing and Health Guidelines; World Health Organization: Geneva, Switzerland, 2018; ISBN 978-92-4-155037-6. [Google Scholar]
- Vega, W.A.; Wallace, S.P. Affordable Housing: A Key Lever to Community Health for Older Americans. Am. J. Public Health 2016, 106, 635–636. [Google Scholar] [CrossRef]
- Fox, S.; Kenny, L.; Day, M.R.; O’Connell, C.; Finnerty, J.; Timmons, S. Exploring the Housing Needs of Older People in Standard and Sheltered Social Housing. Gerontol. Geriatr. Med. 2017, 3, 2333721417702349. [Google Scholar] [CrossRef] [Green Version]
- Lux, M.; Sunega, P. The Impact of Housing Tenure in Supporting Ageing in Place: Exploring the Links between Housing Systems and Housing Options for the Elderly. Eur. J. Hous. Policy 2014, 14, 30–55. [Google Scholar] [CrossRef]
- Szanton, S.L.; Leff, B.; Wolff, J.L.; Roberts, L.; Gitlin, L.N. Home-Based Care Program Reduces Disability and Promotes Aging In Place. Health Aff. 2016, 35, 1558–1563. [Google Scholar] [CrossRef]
- Sulaiman, N.; Baldry, D.; Ruddock, L. Issues Concerning Housing for the Elderly in Malaysia; Research Institute for the Built & Human Environment, University of Salford: Manchester, UK, 2014. [Google Scholar]
- Van Hoof, J.; Marston, H.R.; Kazak, J.K.; Buffel, T. Ten Questions Concerning Age-Friendly Cities and Communities and the Built Environment. Build. Environ. 2021, 199, 107922. [Google Scholar] [CrossRef]
- MyGovernment Public Service Delivery and Local Government: Affordable Home Scheme. Available online: https://www.malaysia.gov.my/portal/content/30704 (accessed on 6 May 2022).
- Shrestha, B.P.; Millonig, A.; Hounsell, N.B.; McDonald, M. Review of Public Transport Needs of Older People in European Context. Popul. Ageing 2017, 10, 343–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MyGovernment Obtaining Facilities, Welfare & Health Care: Senior Citizen Transportation Discount. Available online: https://www.malaysia.gov.my/portal/content/30404 (accessed on 6 May 2022).
- Remillard, E.T.; Campbell, M.L.; Koon, L.M.; Rogers, W.A. Transportation Challenges for Persons Aging with Mobility Disability: Qualitative Insights and Policy Implications. Disabil. Health J. 2021, 15, 101209. [Google Scholar] [CrossRef] [PubMed]
- Bachok, S.; Osman, M.; Ibrahim, M.; Ponrahono, Z. Regenerating Ipoh City Mobility through High Level of Service (LOS) of Public Bus Service. Procedia-Soc. Behav. Sci. 2015, 170, 680–689. [Google Scholar] [CrossRef] [Green Version]
- Aceves-González, C.; Cook, S.; May, A. Improving Bus Travel through Inclusive Design Service. In Ergonomics in Design: Methods and Techniques; CRC Press: Boca Raton, FL, USA, 2016; p. 16. ISBN 978-1-4987-6070-6. [Google Scholar]
- Daniels, R.; Mulley, C. Flexible Transport Services: Overcoming Barriers to Implementation in Low-Density Urban Areas. Urban. Policy Res. 2012, 30, 59–76. [Google Scholar] [CrossRef]
- Mulley, C.; Nelson, J.D. Flexible Transport Services: A New Market Opportunity for Public Transport. Res. Transp. Econ. 2009, 25, 39–45. [Google Scholar] [CrossRef]
- Jaafar, S.; Noh, K.M.; Muttalib, K.A.; Othman, N.H.; Healy, J. Malaysia Health System Review; Healy, J., Ed.; WHO: Geneva, Switzerland, 2012; Volume 2, ISBN 978-92-9061-584-2. [Google Scholar]
- Foreman, K.J.; Marquez, N.; Dolgert, A.; Fukutaki, K.; Fullman, N.; McGaughey, M.; Pletcher, M.A.; Smith, A.E.; Tang, K.; Yuan, C.-W.; et al. Forecasting Life Expectancy, Years of Life Lost, and All-Cause and Cause-Specific Mortality for 250 Causes of Death: Reference and Alternative Scenarios for 2016–40 for 195 Countries and Territories. Lancet 2018, 392, 2052–2090. [Google Scholar] [CrossRef] [Green Version]
- Stuck, A.E.; Siu, A.L.; Wieland, G.D.; Rubenstein, L.Z.; Adams, J. Comprehensive Geriatric Assessment: A Meta-Analysis of Controlled Trials. Lancet 1993, 342, 1032–1036. [Google Scholar] [CrossRef]
- Heng Leng, C.; Simon, B. Health Care in Malaysia The Dynamics of Provision, Financing and Access; Routledge: London, UK, 2009; ISBN 978-0-415-54420-7. [Google Scholar]
- Tan, M.P.; Kamaruzzaman, S.B.; Poi, P.J.H. An Analysis of Geriatric Medicine in Malaysia-Riding the Wave of Political Change. Geriatrics 2018, 3, 80. [Google Scholar] [CrossRef] [Green Version]
- Price, R.; Stoneham, J. Making Connections: A Guide to Accessible Greenspace; Sensory Trust: Bath, UK, 2001; ISBN 978-0-9526745-3-5. [Google Scholar]
- Zhang, W.; Yang, J.; Ma, L.; Huang, C. Factors Affecting the Use of Urban Green Spaces for Physical Activities: Views of Young Urban Residents in Beijing. Urban For. Urban Green. 2015, 14, 851–857. [Google Scholar] [CrossRef]
- Kaplan, S.; Talbot, J.F. Psychological Benefits of a Wilderness Experience. In Behavior and the Natural Environment; Altman, I., Wohlwill, J.F., Eds.; Springer: Boston, MA, USA, 1983; pp. 163–203. ISBN 978-1-4613-3541-2. [Google Scholar]
- Hailegiorgis, Y.G. Recreational Parks: Practices and Challenges in Hawassa City. J. Tour. Hosp. 2017, 6. [Google Scholar] [CrossRef]
- Radović-Marković, M. An aging workforce: Employment Opportunities and Obstacles. Cadmus 2013, 1, 142–155. [Google Scholar]
- Oude Mulders, J.; van Dalen, H.P.; Henkens, K.; Schippers, J. How Likely Are Employers to Rehire Older Workers After Mandatory Retirement? A Vignette Study Among Managers. De Econ. 2014, 162, 415–431. [Google Scholar] [CrossRef]
- Naegele, G.; Walker, A. A Guide to Good Practice in Age Management; Office for Official Publication of the European Communities: Luxembourg, 2006; ISBN 978-92-897-0934-7. [Google Scholar]
- Samorodov, A.; Bureau International du Travail, Employment and Training Department. Ageing and Labour Markets for Older Workers; Employment and Training Department, International Labour Office: Genèva, Switzerland, 1999; ISBN 978-92-2-111418-5. [Google Scholar]
- Shaikh, B.; Mazhar, A.; Khan, S.; Hafeez, A. Social Protection Strategies and Health Financing to Safeguard Reproductive Health for the Poor: Making a Case for Pakistan. J. Ayub Med. Coll. Abbottabad. 2013, 23, 126–130. [Google Scholar]
- Adato, M.; Bassett, L. Social Protection to Support Vulnerable Children and Families: The Potential of Cash Transfers to Protect Education, Health and Nutrition. AIDS Care 2009, 21, 60–75. [Google Scholar] [CrossRef]
- Levasseur, M.; Routhier, S.; Clapperton, I.; Doré, C.; Gallagher, F. Social Participation Needs of Older Adults Living in a Rural Regional County Municipality: Toward Reducing Situations of Isolation and Vulnerability. BMC Geriatr. 2020, 20, 456. [Google Scholar] [CrossRef]
- Novek, S.; Menec, V.; Tran, T.; Bell, S. Social Participation and Its Benefits; Centre on Aging, University of Manitoba: Winnipeg, MA, Canada, 2013; p. 84. [Google Scholar]
- MK, T. Ipoh Echo|Senior Citizens Club Perak. Available online: http://www.ipohecho.com.my/v4/article/2016/12/01/senior-citizens-club-perak (accessed on 6 May 2022).
- Loh, I. A Place to Socialise. Available online: https://www.thestar.com.my/metro/community/2015/11/04/a-place-to-socialise-ministry-hopes-to-have-activity-centres-for-senior-citizens-in-each-parliamenta (accessed on 6 May 2022).
- Levasseur, M.; Généreux, M.; Bruneau, J.-F.; Vanasse, A.; Chabot, É.; Beaulac, C.; Bédard, M.-M. Importance of Proximity to Resources, Social Support, Transportation and Neighborhood Security for Mobility and Social Participation in Older Adults: Results from a Scoping Study. BMC Public Health 2015, 15, 503. [Google Scholar] [CrossRef] [Green Version]
- Gottlieb, B.H.; Gillespie, A.A. Volunteerism, Health, and Civic Engagement among Older Adults. Can. J. Aging 2008, 27, 399–406. [Google Scholar] [CrossRef]
- Batista, L.; Cruz-Ledón, A. The Relationship between Civic Engagement and Health among Older Adults. In Proceedings of the South Florida Education Research Conference 2013, Portland, FL, USA, 17–18 July 2013. [Google Scholar]
- McBride, A. Civic Engagement, Older Adults, and Inclusion. Generations 2006, 30, 66–71. [Google Scholar]
- Cotten, S.R.; Ford, G.; Ford, S.; Hale, T.M. Internet Use and Depression among Older Adults. Comput. Hum. Behav. 2012, 28, 496–499. [Google Scholar] [CrossRef]
- Keeley, B. Human Capital: How What You Know Shapes Your Life; OECD Insights; OECD: Paris, France, 2007; ISBN 978-92-64-02908-8. [Google Scholar]
- Neves, B.B.; Fonseca, J.R.S.; Amaro, F.; Pasqualotti, A. Social Capital and Internet Use in an Age-Comparative Perspective with a Focus on Later Life. PLoS ONE 2018, 13, e0192119. [Google Scholar] [CrossRef]
- Organisation for Economic and Co-operation and Development (OECD). Understanding the Digital Divide; OECD Digital Economy Papers; OECD: Paris, France, 2001; Volume 49. [Google Scholar]
- Kamarudin, S.; Omar, S.; Bolong, J.; Osman, M.N.; Mahamed, M. ICT Development of Community in Rural Areas. Acad. Res. Int. 2019, 9, 118–126. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Overall (n = 1061) | City Center (n = 533) | Non-City Center (n = 528) | p-Value | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Age (years) (Mean, SD) | 68.69, 6.58 | 69.24, 6.92 | 68.13, 6.17 | 0.006 | |||
| 60–70 | 677 | 63.8 | 323 | 60.6 | 354 | 67.0 | 0.042 |
| 71–80 | 314 | 29.6 | 167 | 31.3 | 147 | 27.8 | |
| 81 and above | 70 | 6.6 | 43 | 8.1 | 27 | 5.1 | |
| Gender | |||||||
| Male | 505 | 47.6 | 254 | 47.7 | 251 | 47.5 | 0.970 |
| Female | 556 | 52.4 | 279 | 52.3 | 277 | 52.5 | |
| Marital status | |||||||
| Married | 875 | 82.5 | 442 | 82.9 | 433 | 82.0 | 0.694 |
| Unmarried | 186 | 17.5 | 91 | 17.1 | 95 | 18.0 | |
| Ethnicity | |||||||
| Malay | 381 | 35.9 | 198 | 37.1 | 183 | 34.7 | 0.296 |
| Chinese | 263 | 24.8 | 140 | 26.3 | 123 | 23.3 | |
| Indian | 402 | 37.9 | 189 | 35.5 | 213 | 40.3 | |
| Others | 15 | 1.4 | 6 | 1.1 | 9 | 1.7 | |
| Education | |||||||
| No formal education | 51 | 4.8 | 27 | 5.1 | 24 | 4.5 | 0.151 |
| Primary | 356 | 33.6 | 191 | 35.8 | 165 | 31.2 | |
| Secondary | 517 | 48.7 | 241 | 45.2 | 276 | 52.3 | |
| Tertiary | 137 | 12.9 | 74 | 13.9 | 63 | 11.9 | |
| Living status | |||||||
| Living alone | 71 | 6.7 | 40 | 7.5 | 31 | 5.9 | 0.287 |
| Not living alone | 990 | 93.3 | 493 | 92.5 | 497 | 94.1 | |
| Income, RM (Mean, SD) | 1221.1, 1488.1 | 1190.8, 1544.1 | 1251.6, 1430.2 | 0.507 | |||
| Less than RM 2000 | 931 | 87.7 | 468 | 87.8 | 463 | 87.7 | 0.818 |
| RM2001-RM 4800 | 101 | 9.5 | 49 | 9.2 | 52 | 9.8 | |
| More than RM4801 | 29 | 2.7 | 16 | 3.0 | 13 | 2.5 | |
| Perceived opinion Ipoh as a place for senior citizen to live | |||||||
| Good | 941 | 88.7 | 468 | 87.8 | 473 | 89.6 | |
| Moderate | 117 | 11.0 | 64 | 12.0 | 53 | 10.0 | 0.504 |
| Poor | 3 | 0.3 | 1 | 0.2 | 2 | 0.4 | |
| Duration of stay in Ipoh (years) | |||||||
| 6 months–10 years | 47 | 4.4 | 26 | 4.9 | 21 | 4.0 | 0.722 |
| 11–30 years | 210 | 19.8 | 104 | 19.5 | 106 | 20.1 | |
| 31–60 years | 301 | 28.4 | 157 | 29.5 | 144 | 27.3 | |
| More than 60 years | 503 | 47.4 | 246 | 46.2 | 257 | 48.7 | |
| Health condition | |||||||
| Healthy | 224 | 21.1 | 90 | 16.9 | 134 | 25.4 | 0.001 |
| Active but with underlying diseases | 785 | 74.0 | 409 | 76.7 | 376 | 71.2 | |
| Inactive/with restricted mobility | 52 | 4.9 | 34 | 6.4 | 18 | 3.4 | |
| Possess health care coverage/insurance | |||||||
| Yes | 401 | 37.8 | 199 | 37.3 | 202 | 38.3 | 0.757 |
| No or unsure | 660 | 62.2 | 334 | 62.7 | 326 | 61.7 | |
| Engagement of physical exercise in a week | |||||||
| Never | 196 | 18.5 | 95 | 17.8 | 101 | 19.1 | 0.598 |
| Sometimes (1–4 times) | 502 | 47.3 | 248 | 46.5 | 254 | 48.1 | |
| Frequently (5–7 times) | 363 | 34.2 | 190 | 35.6 | 173 | 32.8 | |
| Access the Internet | |||||||
| Yes | 521 | 49.1 | 262 | 49.2 | 259 | 49.1 | 0.973 |
| No | 540 | 50.9 | 271 | 50.8 | 269 | 50.9 | |
| Current employment status | |||||||
| Employed | 196 | 18.5 | 104 | 19.5 | 92 | 17.4 | 0.381 |
| Unemployed | 865 | 81.5 | 429 | 80.5 | 436 | 82.6 | |
| Intention to continue to work for as long as possible | |||||||
| Yes | 230 | 21.7 | 120 | 22.5 | 110 | 20.8 | 0.506 |
| No | 831 | 78.3 | 413 | 77.5 | 418 | 79.2 | |
| City Center | Non-City Center | Difference | Overall | p-Value | |||
| Domain | Elements | Valid n | Mean Gap % | Mean Gap % | Mean Gap % | Mean Gap % | |
| Housing (D1) | Equipped with home safety features | 990 | 33.6 | 39.3 | 5.7 | 36.4 | 0.064 |
| Affordable housing options | 958 | 64.8 | 62.3 | 2.5 | 63.6 | 0.424 | |
| Financial assistance for home modification and purchasing | 932 | 66.5 | 66.2 | 0.3 | 66.3 | 0.927 | |
| Overall mean gap percent score | 54.9 | 55.9 | 1.0 | 55.4 | 0.334 | ||
| Outdoor spaces and buildings (D2) | Accessible parks and recreational areas | 992 | 19.3 | 17.1 | 2.2 | 18.2 | 0.374 |
| Accessible public building and facilities | 1022 | 10.0 | 8.1 | 1.9 | 9.1 | 0.290 | |
| Rest rooms accessible to people with physical disabilities | 963 | 40.3 | 30.0 | 10.3 | 35.1 | 0.001 | |
| Well-maintained parks and facilities | 1022 | 26.8 | 16.5 | 10.3 | 21.7 | <0.001 | |
| Neighborhood watch program | 989 | 44.4 | 42.2 | 2.2 | 43.3 | 0.479 | |
| Overall mean gap percent score | 28.2 | 22.8 | 5.4 | 25.5 | 0.060 | ||
| Transportation and streets (D3) | Accessible public transportation | 919 | 48.6 | 48.9 | 0.3 | 48.7 | 0.931 |
| Affordable public transportation | 911 | 48.6 | 51.3 | 2.7 | 49.9 | 0.408 | |
| Public transport travel to key destinations | 921 | 50.6 | 47.3 | 3.3 | 49.0 | 0.305 | |
| Easy to read traffic signs | 1001 | 17.0 | 14.6 | 2.4 | 15.8 | 0.305 | |
| Priority parking bays for elderly | 986 | 83.5 | 84.0 | 0.5 | 83.8 | 0.841 | |
| Audio/visual pedestrian crossings | 982 | 57.1 | 57.1 | 0.0 | 57.1 | 0.993 | |
| Overall mean gap percent score | 50.9 | 50.5 | 0.2 | 50.7 | 0.906 | ||
| Health and wellness (D4) | Health and wellness programs | 927 | 53.6 | 55.9 | 2.3 | 54.8 | 0.483 |
| Conveniently located health facilities | 1044 | 8.1 | 6.4 | 1.7 | 7.3 | 0.277 | |
| Home visit by healthcare professionals | 978 | 78.0 | 79.9 | 1.9 | 78.9 | 0.453 | |
| Nursing home for older people | 971 | 16.4 | 28.3 | 11.9 | 22.3 | <0.001 | |
| A variety of healthcare professionals including specialists | 1030 | 27.2 | 34.7 | 7.5 | 30.9 | 0.009 | |
| Health care professionals who speak different languages | 1033 | 18.6 | 19.4 | 0.8 | 19.0 | 0.746 | |
| Respectful and helpful heath care staff | 1039 | 5.3 | 6.0 | 0.7 | 5.7 | 0.638 | |
| Overall mean gap percent score | 29.6 | 32.9 | 3.3 | 31.3 | 0.051 | ||
| Social participation, inclusion and education opportunities (D5) | Privilege for entertainment | 902 | 34.5 | 35.2 | 0.7 | 34.8 | 0.827 |
| Convenient location for entertainment | 862 | 17.2 | 19.6 | 2.4 | 18.4 | 0.360 | |
| A variety of cultural celebration | 955 | 24.0 | 35.9 | 11.9 | 29.8 | < 0.001 | |
| Social clubs for hobbies | 872 | 31.5 | 25.2 | 6.3 | 28.3 | 0.038 | |
| Overall mean gap percent score | 26.8 | 28.9 | 2.1 | 27.9 | 0.014 | ||
| Volunteering and civic engagement (D6) | A range of volunteer activities | 900 | 29.9 | 22.2 | 7.7 | 26.1 | 0.009 |
| Opportunity to participate in decision making bodies | 905 | 23.4 | 19.3 | 4.1 | 21.3 | 0.125 | |
| Overall mean gap percent score | 26.7 | 20.8 | 5.9 | 23.7 | 0.007 | ||
| Job opportunities (D7) | Flexible job opportunities | 968 | 41.3 | 40.3 | 1.0 | 40.8 | 0.770 |
| Overall mean gap percent score | 41.3 | 40.3 | 1.0 | 40.8 | 0.770 | ||
| Community and information (D8) | Readable written information | 987 | 30.5 | 24.8 | 5.7 | 27.7 | 0.047 |
| Telephone operator services adapted to the needs of seniors | 919 | 32.7 | 28.3 | 4.4 | 30.5 | 0.144 | |
| Free access to computers and internet | 861 | 56.0 | 49.0 | 7.0 | 52.4 | 0.039 | |
| Information available in different languages | 963 | 36.2 | 40.3 | 4.1 | 38.2 | 0.197 | |
| Overall mean gap percent score | 38.9 | 35.6 | 3.3 | 37.2 | 0.307 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, C.-T.; Lim, X.-J.; Supramaniam, P.; Chew, C.-C.; Ding, L.-M.; Rajan, P. Perceived Gap of Age-Friendliness among Community-Dwelling Older Adults: Findings from Malaysia, a Middle-Income Country. Int. J. Environ. Res. Public Health 2022, 19, 7171. https://doi.org/10.3390/ijerph19127171
Chang C-T, Lim X-J, Supramaniam P, Chew C-C, Ding L-M, Rajan P. Perceived Gap of Age-Friendliness among Community-Dwelling Older Adults: Findings from Malaysia, a Middle-Income Country. International Journal of Environmental Research and Public Health. 2022; 19(12):7171. https://doi.org/10.3390/ijerph19127171
Chicago/Turabian StyleChang, Chee-Tao, Xin-Jie Lim, Premaa Supramaniam, Chii-Chii Chew, Lay-Ming Ding, and Philip Rajan. 2022. "Perceived Gap of Age-Friendliness among Community-Dwelling Older Adults: Findings from Malaysia, a Middle-Income Country" International Journal of Environmental Research and Public Health 19, no. 12: 7171. https://doi.org/10.3390/ijerph19127171
APA StyleChang, C.-T., Lim, X.-J., Supramaniam, P., Chew, C.-C., Ding, L.-M., & Rajan, P. (2022). Perceived Gap of Age-Friendliness among Community-Dwelling Older Adults: Findings from Malaysia, a Middle-Income Country. International Journal of Environmental Research and Public Health, 19(12), 7171. https://doi.org/10.3390/ijerph19127171