
Delusional Disorder in Old Age: A Hypothesis-Driven Review of Recent Work Focusing on Epidemiology, Clinical Aspects, and Outcomes

 ,
,  ,
, 

Abstract
:1. Introduction
Aim
- (1)
- That incidence and prevalence and severity of symptoms increase with age;
- (2)
- That in old age, women are more vulnerable to DD than men;
- (3)
- That brain changes and cognitive defects predict poor treatment response;
- (4)
- That DD in old age is associated with self-harm and harm to others.
2. Materials and Methods
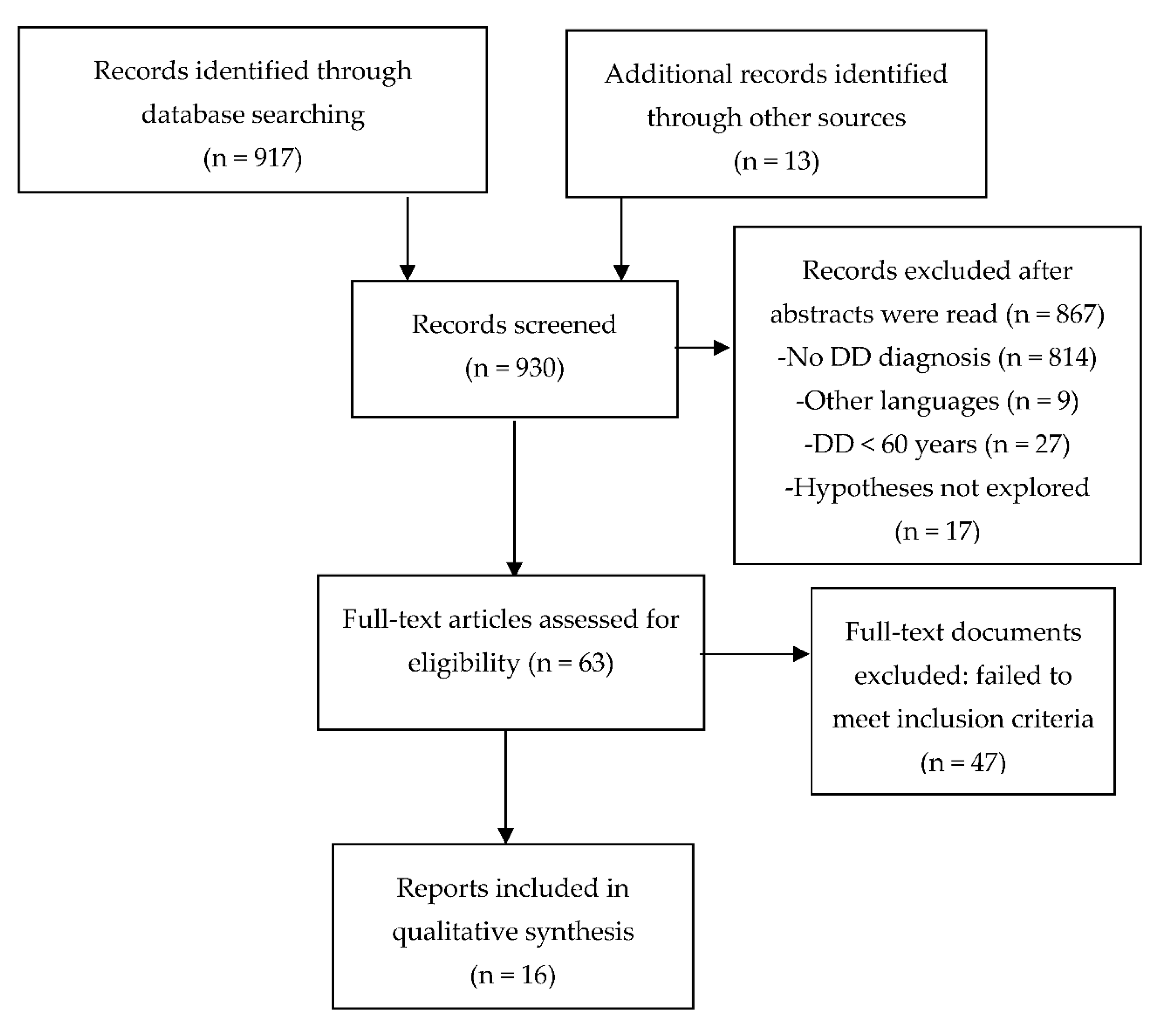
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Data Collection and Extraction
2.4. Data Synthesis
3. Results
3.1. Prevalence and Sex Ratio in Elderly DD (Hypothesis 1 and 2)
3.2. Relationship of Brain Structure, Cognition and Treatment Response (Hypothesis 3)
3.3. DD in Old Age Is Associated with Self-Harm and Harm to Others (Hypothesis 4)
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peralta, V.; Cuesta, M.J. An empirical study of five sets of diagnostic criteria for delusional disorder. Schizophr. Res. 2019, 209, 164–170. [Google Scholar] [CrossRef] [PubMed]
- González-Rodríguez, A.; Guàrdia, A.; Seeman, M.V.; Monreal, J.A. Optimizing treatment of delusional disorder: New goals for a new era. Curr. Top. Pharmacol. 2021, 25, 61–68. [Google Scholar]
- Kendler, K.S. The clinical features of paranoia in the 20th century and their representation in diagnostic criteria from DSM-III through DSM-5. Schizophr. Bull. 2017, 43, 332–343. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Copeland, J.R.; Dewey, M.E.; Scott, A.; Gilmore, C.; Larkin, B.A.; Cleave, N.; McCracken, C.F.; McKibbin, P.E. Schizophrenia and delusional disorder in older age: Community prevalence, incidence, comorbidity, and outcome. Schizophr. Bull. 1998, 24, 153–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wustmann, T.; Pillmann, F.; Friedemann, J.; Piro, J.; Schmeil, A.; Marneros, A. The clinical and sociodemographic profile of persistent delusional disorder. Psychopathology 2012, 45, 200–202. [Google Scholar] [CrossRef] [PubMed]
- De Portugal, E.; González, N.; del Amo, V.; Haro, J.M.; Díaz-Caneja, C.M.; de Dios Luna del Castillo, J.; Cervilla, J.A. Empirical redefinition of delusional disorder and its phenomenology: The DELIREMP study. Compr. Psychiatry 2013, 54, 243–255. [Google Scholar] [CrossRef]
- Muñoz-Negro, J.E.; Ibanez-Casas, I.; de Portugal, E.; Ochoa, S.; Dolz, M.; Haro, J.M.; Ruiz-Veguilla, M.; de Dios Luna Del Castillo, J.; Cervilla, J.A. A dimensional comparison between delusional disorder, schizophrenia and schizoaffective disorder. Schizophr. Res. 2015, 169, 248–254. [Google Scholar] [CrossRef]
- Ibanez-Casas, I.; De Portugal, E.; Gonzalez, N.; McKenney, K.A.; Haro, J.M.; Usall, J.; Perez-Garcia, M.; Cervilla, J.A. Deficits in executive and memory processes in delusional disorder: A case-control study. PLoS ONE 2013, 8, e67341. [Google Scholar]
- Peralta, V.; Cuesta, M.J. Characteristics and clinical correlates of dimensions of delusional experience in schizophrenia and delusional disorder. Schizophr. Res. 2016, 176, 404–410. [Google Scholar] [CrossRef]
- Tampi, R.R.; Young, J.; Hoq, R.; Resnick, K.; Tampi, D.J. Psychotic disorders in late life: A narrative review. Ther. Adv. Psychopharmacol. 2019, 9, 2045125319882798. [Google Scholar] [CrossRef]
- Howard, R.; Rabins, P.V.; Seeman, M.V.; Jeste, D.V.; the International Late-Onset Schizophrenia Group. Late-onset schizophrenia and very-late-onset schizophrenia-like psychosis: An international consensus. Am. J. Psychiatry 2000, 157, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Jagsch, C.; Hofer, A. Diseases of the schizophrenia spectrum disorder in old age: Diagnostic and therapeutic challenges. Z. Gerontol. Geriatr. 2018, 51, 744–750. [Google Scholar] [CrossRef] [PubMed]
- Gardijan, N.; Szücs, A. Late life psychotic disorders: Clinical aspects. Rev. Med. Suisse 2016, 12, 1561–1564. [Google Scholar] [PubMed]
- Colijn, M.A.; Nitta, B.H.; Grossberg, G.T. Psychosis in later life: A review and update. Harv. Rev. Psychiatry 2015, 23, 354–367. [Google Scholar] [CrossRef]
- Castro-de-Araujo, L.F.; Machado, D.B.; Barreto, M.L. Care-seeking as a proxy indicator of the mental health of elderly Brazilians. Braz. J. Psychiatry 2020, 42, 591–598. [Google Scholar] [CrossRef]
- González-Rodríguez, A.; Molina-Andreu, O.; Penadés, R.; Garriga, M.; Pons, A.; Catalán, R.; Bernardo, M. Delusional disorder over the reproductive life span: The potential influence of menopause on the clinical course. Schizophr. Res. Treat. 2015, 2015, 979605. [Google Scholar] [CrossRef] [Green Version]
- Meesters, P.D.; de Haan, L.; Comijs, H.C.; Stek, M.L.; Smeets-Janssen, M.M.; Weeda, M.R.; Eikelenboom, P.; Smit, J.H.; Beekman, A.T. Schizophrenia spectrum disorders in later life: Prevalence and distribution of age at onset and sex in a Dutch catchment area. Am. J. Geriatr. Psychiatry 2012, 20, 18–28. [Google Scholar] [CrossRef]
- Nagendra, J.; Snowdon, J. An Australian study of delusional disorder in late life. Int. Psychogeriatr. 2020, 32, 453–462. [Google Scholar] [CrossRef]
- Krämer, J.; Huber, M.; Mundinger, C.; Schmitgen, M.M.; Pycha, R.; Kirchler, E.; Macina, C.; Karner, M.; Hirjak, D.; Kubera, K.M.; et al. Abnormal cerebellar volume in somatic vs. non-somatic delusional disorders. Cerebellum Ataxias 2020, 7, 2. [Google Scholar] [CrossRef] [Green Version]
- Dua, D.; Grover, S. Delusion of pregnancy for 21 years in an elderly woman: A case report and review of literature. Ind. Psychiatry J. 2020, 29, 342–344. [Google Scholar]
- Wolf, R.C.; Hildebrandt, V.; Schmitgen, M.M.; Pycha, R.; Kirchler, E.; Macina, C.; Karner, M.; Hirjak, D.; Kubera, K.M.; Romanov, D.; et al. Aberrant gray matter volume and cortical surface in paranoid-type delusional disorder. Neuropsychobiology 2020, 79, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Van Assche, L.; Van Aubel, E.; Van de Ven, L.; Bouckaert, F.; Luyten, P.; Vandenbulcke, M. The neuropsychological profile and phenomenology of late onset psychosis: A cross-sectional study on the differential diagnosis of very-late-onset-schizophrenia-like psychosis, dementia with Lewy bodies and Alzheimer’s type dementia with psychosis. Arch. Clin. Neuropsychol. 2019, 34, 183–199. [Google Scholar] [CrossRef] [PubMed]
- D’Auria, A.; Wiseman, T.; Varghese, A.; Espiridion, E.D. Refractory delusional parasitosis in a 70-year-old woman. Cureus 2018, 10, e3120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fond, G.; Fajula, C.; Dassa, D.; Brunel, L.; Lançon, C.; Boyer, L. Potentially inappropriate psychotropic prescription at discharge is associated with lower functioning in the elderly psychiatric inpatients. A cross-sectional study. Psychopharmacology 2016, 233, 2549–2558. [Google Scholar] [CrossRef] [PubMed]
- Harris, B.S.; Kotsopoulos, E.J.; Yamin, S. Phenotypic cognitive impairment in late-onset delusional disorder. Int. Psychogeriatr. 2014, 26, 965–975. [Google Scholar] [CrossRef]
- Wolf, R.C.; Huber, M.; Depping, M.S.; Thomann, P.A.; Karner, M.; Lepping, P.; Freudenmann, R.W. Abnormal gray and white matter volume in delusional infestation. Prog. Neuropsychopharmacol. Biol. Psychiatry 2013, 46, 19–24. [Google Scholar] [CrossRef]
- Ukai, K.; Kimura, H.; Arao, M.; Aleksic, B.; Yamauchi, A.; Ishihara, R.; Iritani, S.; Kurita, K.; Ozaki, N. Effectiveness of low-dose milnacipran for a patient suffering from pain disorder with delusional disorder (somatic type) in the orofacial region. Psychogeriatrics 2013, 13, 99–102. [Google Scholar] [CrossRef] [Green Version]
- Machado, C.R.; Fragoeiro, C.; Passos, M. Delusional jealousy: How can treatment be improved? A Case Report. Rev. Colomb. Psiquiatr. 2021, 17, S0034-7450(21)00028-7. [Google Scholar] [CrossRef]
- Weise, J.; Schomerus, G.; Speerforck, S. The SARS-CoV-2 pandemic and an attempted suicide of a patient with delusional disorder. Psychiatr. Prax. 2020, 47, 218–220. [Google Scholar]
- Snowdon, J. Delusional disorder and risk of suicide. Ann. Clin. Case Rep. 2017, 2, 1479. [Google Scholar]
- Seeman, M.V. Pseudocyesis, delusional pregnancy, and psychosis: The birth of a delusion. World J. Clin. Cases 2014, 2, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Nosratzehi, T. Burning mouth syndrome: A review of therapeutic approach. J. Complementary Integr. Med. 2022, 19, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Cardno, A.G.; McGuffin, P. Genetics and delusional disorder. Behav. Sci. Law 2006, 24, 257–276. [Google Scholar] [CrossRef] [PubMed]
- Oh, H.; Koyanagi, A. Immigrant status and psychotic experiences in the United States: Revisiting an immigrant paradox. Psychol. Med. 2021, 4, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Leaune, E.; Dealberto, M.J.; Luck, D.; Grot, S.; Zeroug-Vial, H.; Poulet, E.; Brunelin, J. Ethnic minority position and migrant status as risk factors for psychotic symptoms in the general population: A meta-analysis. Psychol. Med. 2019, 49, 545–558. [Google Scholar] [CrossRef] [PubMed]
- Post, G.; Veling, W.; GROUP Investigators. Sexual minority status, social adversity and risk for psychotic disorders-results from the GROUP study. Psychol. Med. 2019, 51, 770–776. [Google Scholar] [CrossRef]
- Seeney, S.; Air, T.; Zannettino, L.; Galletly, C. Psychosis, socioeconomic disadvantage, and health service use in South Australia: Findings from the Second Australian National Survey of Psychosis. Front. Public Health 2015, 3, 259. [Google Scholar] [CrossRef] [Green Version]
- Gogla, S.; Grieb, A.; Jang, A.; Gordon, M.R.; Coverdale, J. Medical considerations in delusion of pregnancy: A systematic review. J. Psychosom. Obs. Gyn. 2020, 43, 51–57. [Google Scholar]
- Saffron, M.; Gresswell, D.M.; Merdian, H.L. Psychosis and deafness in forensic settings: How are hallucinations and delusions shaped by experiences of being deaf? Int. J. Forensic Ment. Health 2020, 19, 165–182. [Google Scholar]
- González-Rodríguez, A.; Seeman, M.V. Pharmacotherapy for schizophrenia in postmenopausal women. Expert Opin. Pharmacother. 2018, 19, 809–821. [Google Scholar] [CrossRef]
- Trabert, W. 100 years of delusional parasitosis. Psychopathology 1995, 28, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Ferreira da Silva, W.L.F.; Gomes, L.C.; Silva Silvério, M.; Teles da Cruz, D. Factors associated with non-adherence to pharmacotherapy in older people in primary health care in Brazil: A systematic review. Rev. Bras. Geriatr. Gerontol. 2021, 24, e210156. [Google Scholar]
- González-Rodríguez, A.; Monreal, J.A.; Seeman, M.V. Factors influencing adherence to antipsychotic medications in women with delusional disorder: A narrative review. Curr. Pharm. Des. 2022, 28, 1281–1293. [Google Scholar] [CrossRef] [PubMed]
- Lapid, M.I.; Ho, J.B. Challenging our beliefs about delusional disorder in late life. Int. Psychogeriatr. 2020, 32, 423–425. [Google Scholar] [CrossRef]
- Gournellis, R.; Oulis, P.; Rizos, E.; Chourdaki, E.; Gouzaris, A.; Lykouras, L. Clinical correlates of age of onset in psychotic depression. Arch. Gerontol. Geriatr. 2011, 52, 94–98. [Google Scholar] [CrossRef]
- Liu, Y.; Yang, M.; Ding, Y.; Wang, H.; Zhang, H.; Wang, D.; Zhuang, T.; Ji, M.; Cui, Y.; Wang, H. Analysis of potentially inappropriate medication based on drug-drug interactions in older adults with psychiatric disorders: A retrospective study. Res. Sq. 2022. Under revision for BMC Psychiatry. [Google Scholar] [CrossRef]
- Skelton, M.; Khokhar, W.A.; Thacker, S.P. Treatments for delusional disorder. Cochrane Database Syst. Rev. 2015, 5, 1–33. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Authors and Year of Publication | Study Design | Method | Women (%), Age [Mean, (SD)] | Hypothesis Addressed |
|---|---|---|---|---|
| Hypotheses 1 and 2 | ||||
| Castro-de-Araujo et al., 2020 [16] | Register study of mental-illness prevalence by diagnosis in the elderly | Outpatient visit rates of seniors over age 60 throughout Brazil | F = 340.250 (30.3%) | Suggests, but does not prove, higher-than-expected prevalence of DD in Brazilian seniors. No male/female differences are mentioned |
| González-Rodríguez et al., 2015 [17] | Prospective observational study of women with DD, to determine the effect of pre- and postmenopausal onset | Consecutive cases of women assessed at baseline and after 24 months. | 80 (100%) 57 completed 2-year follow up. Premenopausal onset = 25 Postmenopausal onset + 55 | Women’s onset is more often postmenopausal, with symptom differences between pre- and postmenopausal onset |
| Meesters et al., 2012 [18] | Case register study to determine 1 year prevalence, onset ages and sex ratios of patients with psychosis aged 60 and over | Search of the computerized mental health records over 1 year in Amsterdam | DD: n = 8 (4.4%) | 1 year prevalence of DD in old age was 0.03% and in women, was found only in those with onset over age 40. Very small numbers. |
| Hypothesis 3 | ||||
| Nagendra and Snowdon, 2020 [19] | Retrospective 12-year study of 55 DD patients over age 65 to study the effect of treatment | Follow up after a mean duration of 36.6 months | F = 39 (71%) Age = 74.5 (7.65) | Treatment response was 55%. Six patients developed cognitive impairments at follow up, but no association with treatment response was mentioned. |
| Krämer et al., 2020 [20] | Cross-sectional study designed to study cerebellar dysfunction in psychosis, including somatic and nonsomatic DD | Structural MRI in DD somatic type, DD nonsomatic type, schizophrenia and healthy controls | DD somatic type: 8 (6 women) mean age: 72.6 (9.3) Nonsomatic DD: 13 females mean age: 55.9 | Substantial cerebellar impairment, particularly in DD somatic type, related to age but no mention of treatment response |
| Dua and Grover, 2020 [21] | Case report of DD of long duration, with MRI brain changes | Woman with long-term delusion of pregnancy and resistance to treatment | 75-year-old woman with DD (delusions of pregnancy ICD-10) for 19 years | MRI brain changes potentially associated with lack of treatment response |
| Wolf et al., 2020 [22] | Case series of patients with DD paranoid type in search of brain correlates | Brain structural neuroimaging study of patients and matched healthy controls | 14 patients Sex unspecified | Aberrant gray-matter volume in right prefrontal regions in paranoid type-DD. |
| Van Asche et al., 2019 [23] | Case register study to differentiate 3 groups of late-life psychoses on the basis of symptoms, neuropsychological profile | Comparison of symptoms and neuropsychological profiles of functional and organic psychoses | n= 57 in very-late-onset SZ-like group. 77.8% were women. Mean age: 79.25 | Differences found in symptoms but not in cognitive profiles. Neither treatment responses nor sex differences were studied |
| D’Auria et al., 2018 [24] | Case report of DD lasting 15 years with cortical atrophy and nonresponse to Rx | Woman with DD nonresponsive to psychotherapy and pharmacotherapy | 70-year-old woman with a 15-year history of delusional parasitosis. | CT: microvascular ischemic cortical changes and nonresponse. |
| Fond et al., 2016 [25] | Retrospective 1-year study of cognition-impairing medications on function of patients aged 65 and over | Chart review of function in elderly psychiatric patients at hospital discharge | Total: n = 327 F = 62% Mean age: 73.9 | Cognition-impairing medications may reduce function. Precise diagnosis was unclear in this study |
| Harris et al., 2014 [26] | Case series comparing cognitive deficits fin late-onset DD with those in Alzheimer’s disease | Memory clinic cases (19 DD, 20 AD) assessed by a comprehensive neuropsychological battery | Total DD: n = 19 Sex not specified | Significant cognitive impairment found in late onset DD, but correlation with treatment response was not attempted |
| Wolf et al., 2013 [27] | Case series of patients with somatic DD to determine presence of neural correlates | Brain structural neuroimaging study of patients and matched controls | 16 patients with delusion of parasitosis; 9 were women. Mean age: 74.1 | Gray- and white-matter volume differences were found. Rx response not studied |
| Ukai et al., 2013 [28] | Case report of effective treatment of long-term somatic-type DD with brain changes | 10-year history of DD somatic type (orofacial region) who, after many different treatment trials, responded. | Age: early 70s | Brain changes on MRI. Good response after 10 years due to milnacipran (25 mg/day) |
| Hypothesis 4 | ||||
| Machado et al., 2021 [29] | Case report of male DD in old age and the threat of violence | Case of DD jealous type, with potential aggression, and adverse effects of antipsychotics | 76-year-old man | DD can lead to physical aggression. The case also illustrates adverse effects of antipsychotics. |
| Weise et al., 2020 [30] | Case report of stress-induced delusions, a suicide attempt and medication-free Rx | Woman with complex paranoid delusions and a suicide attempt triggered by stress | Age: mid-sixties woman with persecutory delusions (ICD-10) | Points to the threat of suicide in DD |
| Snowdon, 2017 [31] | Case report: Woman with DD, hyperthyroidism and multiple suicide attempts | DD persecutory type, suicide attempts, eventual good response to treatment | Age: 65 | Points out suicide risk in DD |
| (1) Incidence and prevalence of DD in old age | |
| Prevalence of DD is underestimated in service-based studies. Higher rates of DD in this group are found in register studies. | |
| (2) Gender aspects of DD in old age | |
| Cases in women tend to begin after menopause. | |
| (3) DD in old age is associated with brain changes and cognitive defects that may impair treatment | |
| Microvascular ischemic findings (lacunar infarcts), cortical atrophy, alterations in gray- and white-matter volumes, and cerebellar dysfunctions have been reported, sometimes associated with poor treatment response. | |
| (4) Self-harm and aggression in DD in old age | |
| Prevention of suicide and violence in DD requires targeted intervention. | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-Rodríguez, A.; Seeman, M.V.; Izquierdo, E.; Natividad, M.; Guàrdia, A.; Román, E.; Monreal, J.A. Delusional Disorder in Old Age: A Hypothesis-Driven Review of Recent Work Focusing on Epidemiology, Clinical Aspects, and Outcomes. Int. J. Environ. Res. Public Health 2022, 19, 7911. https://doi.org/10.3390/ijerph19137911
González-Rodríguez A, Seeman MV, Izquierdo E, Natividad M, Guàrdia A, Román E, Monreal JA. Delusional Disorder in Old Age: A Hypothesis-Driven Review of Recent Work Focusing on Epidemiology, Clinical Aspects, and Outcomes. International Journal of Environmental Research and Public Health. 2022; 19(13):7911. https://doi.org/10.3390/ijerph19137911
Chicago/Turabian StyleGonzález-Rodríguez, Alexandre, Mary V. Seeman, Eduard Izquierdo, Mentxu Natividad, Armand Guàrdia, Eloïsa Román, and José A. Monreal. 2022. "Delusional Disorder in Old Age: A Hypothesis-Driven Review of Recent Work Focusing on Epidemiology, Clinical Aspects, and Outcomes" International Journal of Environmental Research and Public Health 19, no. 13: 7911. https://doi.org/10.3390/ijerph19137911
APA StyleGonzález-Rodríguez, A., Seeman, M. V., Izquierdo, E., Natividad, M., Guàrdia, A., Román, E., & Monreal, J. A. (2022). Delusional Disorder in Old Age: A Hypothesis-Driven Review of Recent Work Focusing on Epidemiology, Clinical Aspects, and Outcomes. International Journal of Environmental Research and Public Health, 19(13), 7911. https://doi.org/10.3390/ijerph19137911