
Play Badminton Forever: A Systematic Review of Health Benefits

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Selection
2.4. Data Extraction
2.5. Assessment of Study Methodological Quality
3. Results
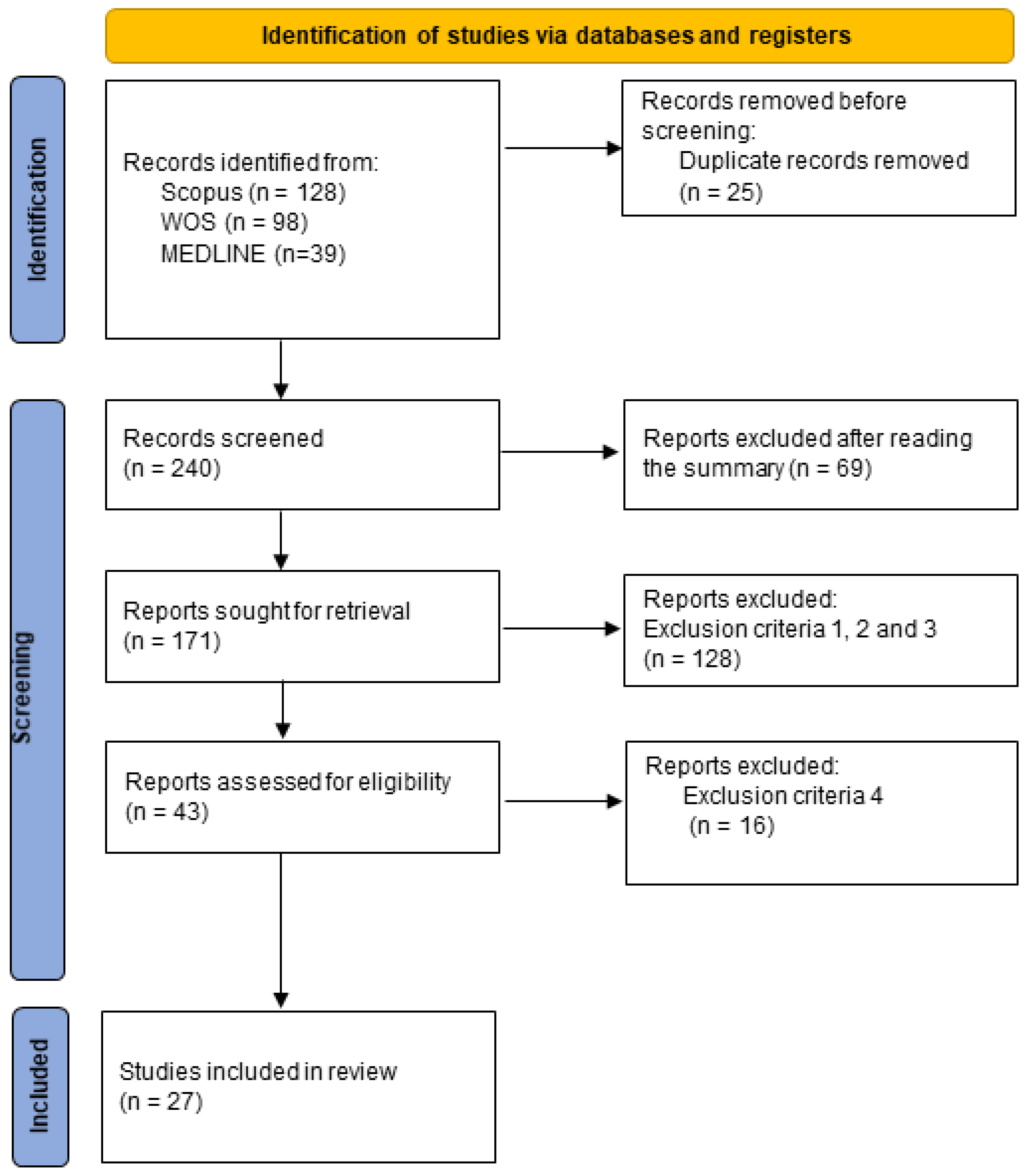
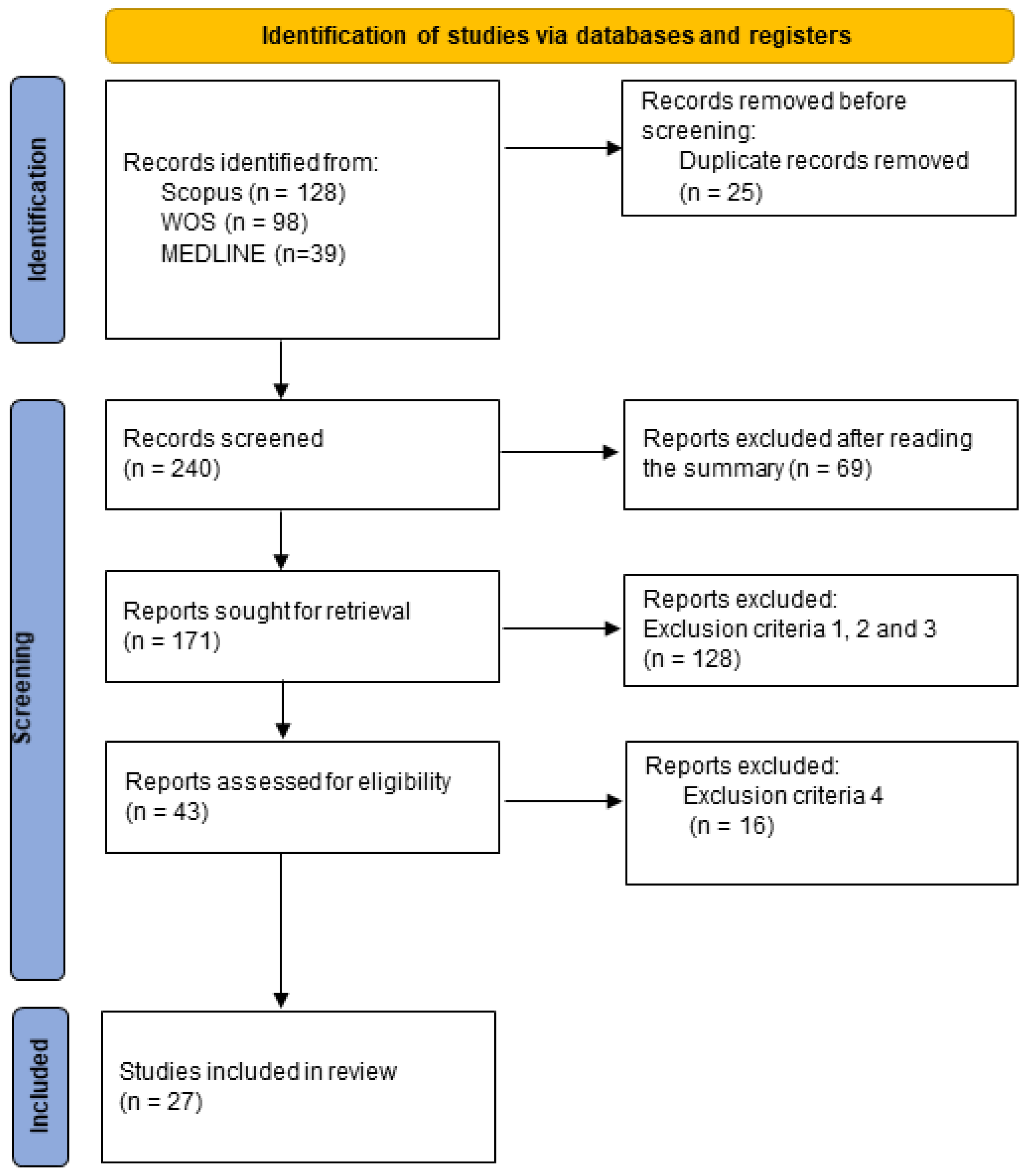
3.1. Database Searches
3.2. Description of Included Studies
3.3. Findings Pertaining to the Characteristics of Selected Studies
4. Discussion
4.1. Physical Health Benefits
4.2. Mental Health Benefits
4.3. Social Health Benefits
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Basic Documents, 45th ed.; World Health Organization: Geneva, Switzerland, 2005; Available online: https://apps.who.int/iris/handle/10665/43134 (accessed on 15 December 2020).
- De La Guardia, M.A.; Ruvalcaba, J.C. La salud y sus determinantes, promoción de la salud y educación sanitaria. J. Negat. No Posit. Results 2020, 5, 81–90. [Google Scholar] [CrossRef]
- Casazola, J. La salud y sus determinantes: Crisis socioambiental y relaciones sociales de discriminación. Pacha Derecho Y Vis. 2021, 2, 33–40. [Google Scholar]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World. World Health Organization. 2019. Available online: https://apps.who.int/iris/handle/10665/327897 (accessed on 15 December 2020).
- Wilke, J.; Mohr, L.; Tenforde, A.S.; Edouard, P.; Fossati, C.; González-Gross, M.; Sánchez Ramírez, C.; Laiño, F.; Tan, B.; Pillay, J.D.; et al. A Pandemic within the Pandemic? Physical Activity Levels Substantially Decreased in Countries Affected by COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 2235. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Zeng, N.; Ye, S. Associations of Sedentary Behavior with Physical Fitness and Academic Performance among Chinese Students Aged 8–19 Years. Int. J. Environ. Res. Public Health 2019, 16, 4494. [Google Scholar] [CrossRef] [Green Version]
- Ströhle, A. Physical activity, exercise, depression and anxiety disorders. J. Neural. Transm. 2009, 116, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Meyer, T.; Broocks, A. Therapeutic impact of exercise on psychiatric diseases. Guidelines for exercise testing and prescription. Sports Med. 2000, 30, 269–279. [Google Scholar] [CrossRef]
- Otto, M.W.; Church, T.S.; Craft, L.L.; Greer, T.L.; Smits, J.A.; Trivedi, M.H. Exercise for mood and anxiety disorders. J. Clin. Psychiatry 2007, 9, 287–294. [Google Scholar] [CrossRef]
- Segar, M.; Jayaratne, T.; Hankon, J.; Richardson, C.R. Fitting fitness into women’s lives: Effects of a gender-tailored physical activity intervention. Womens Health 2002, 12, 338–347. [Google Scholar] [CrossRef] [Green Version]
- Werneck, A.O.; Silva, D.R.; Malta, D.C.; Souza-Júnior, P.R.B.; Azevedo, L.O.; Barros, M.B.A.; Szwarcwald, C.L. Physical inactivity and elevated TV-viewing reported changes during the COVID-19 pandemic are associated with mental health: A survey with 43,995 Brazilian adults. J. Psychosom. Res. 2021, 140, 110292. [Google Scholar] [CrossRef]
- Lee, I.-M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.C.; Pate, R.R.; Lavie, C.J.; Sui, X.; Church, T.S.; Blair, S.N. Leisure-time running reduces all-cause and cardiovascular mortality risk. Am. J. Cardiol. 2014, 64, 472–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, R.A.; Riethmuller, A.; Hesketh, K.; Trezise, J.; Batterham, M.; Okely, A.D. Promoting fundamental movement skill development and physical activity in early childhood settings: A cluster randomized controlled trial. Pediatr. Exerc. Sci. 2011, 23, 600–615. [Google Scholar] [CrossRef]
- Bellows, L.L.; Davies, P.L.; Anderson, J.; Kennedy, C. Effectiveness of a physical activity intervention for Head Start preschoolers: A randomized intervention study. Am. J. Occup. Ther. 2013, 67, 28–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carbonell, T.; Antoñanzas, J.L.; Lope Álvarez, Á. La educación física y las relaciones sociales en educación primaria. IJODAEP 2018, 2, 269–282. Available online: https://dialnet.unirioja.es/servlet/articulo?codigo=6432668&orden=0&info=link (accessed on 15 December 2020). [CrossRef] [Green Version]
- Lassandro, G.; Trisciuzzi, R.; Palladino, V.; Carriero, F.; Giannico, O.V.; Tafuri, S.; Valente, R.; Gianfelici, A.; Accettura, D.; Giordano, P. Psychophysical health and perception of well-being between master badminton athletes and the adult Italian population. Acta Biomed. 2021, 92, e2021253. [Google Scholar] [CrossRef]
- Jimenez, M. El bádminton de competición: Una revisión actual. EFDeportes 2010, 149. Available online: http://www.efdeportes.com (accessed on 20 January 2021).
- Madison Beach Volley Tour. 10 Deportes más Practicados en el Mundo. Available online: https://beachvolleytour.es/10-deportes-mas-practicados-en-el-mundo (accessed on 21 March 2022).
- Kwan, M.; Cheng, C.L.; Tang, W.T.; Rasmussen, J. Measurement of badminton racket deflection during a stroke. Sports Eng. 2010, 12, 143–153. [Google Scholar] [CrossRef]
- Phomsoupha, M.; Laffaye, G. The science of badminton: Game characteristics Anthropometry, Physiology, Visual Fitness and Biomechanics. Sports Med. 2015, 45, 473–495. [Google Scholar] [CrossRef]
- Cabello-Manrique, D.; González-Badillo, J.J. Analysis of the characteristics of competitive badminton. Br. J. Sports Med. 2003, 37, 62–66. [Google Scholar] [CrossRef] [Green Version]
- Blanca-Torres, J.C.; Ortega, E.; Nikolaidis, P.T.; Torres-Luque, G. Bibliometric analysis of scientific production in badminton. J. Hum. Sport Exerc. 2020, 15, 267–282. [Google Scholar] [CrossRef]
- Campos, L.M.; Sasai Morimoto, L.M.; Ribas da Silva, S.; Cabello-Manrique, D. A scientometric study about badminton applied to sports science research. In Science and Racket Sports VI; Kondrič, M., Cabello, D., Pinthong, M., Eds.; Mahidol University: Nakhon Pathom, Thailand, 2019; pp. 173–185. [Google Scholar]
- Chen, C.-C.; Ryuh, Y.-J.; Donald, M.; Rayner, M. The impact of badminton lessons on health and wellness of young adults with intellectual disabilities: A pilot study. Int. J. Dev. Disabil. 2021, 1–10. [Google Scholar] [CrossRef]
- Stovba, I.R.; Stolyarova, N.V.; Petrozak, O.L.; Ishmatova, A.R. Benefits of badminton driven academic physical education model for female students. Teor. Prak. Fiz. Kult. 2019, 2019, 54–56. Available online: https://www.scopus.com/inward/record.uri?eid=2-s2.0-85071149003&partnerID=40&md5=9682b01f06de672a22cbe4c2d463fe6f (accessed on 15 December 2020).
- Chan, B.C.L.; Lee, B. Wellbeing and personality through sports: A qualitative study of older badminton players in two cultures. Qual. Res. Sport Exerc. Health 2020, 12, 350–362. [Google Scholar] [CrossRef]
- Ng, S.S.W.; Leung, T.K.S.; Ng, P.P.K.; Ng, R.K.H.; Wong, A.T.Y. Activity participation and perceived health status in patients with severe mental illness: A prospective study. East Asian Arch. Psychiatry 2020, 30, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Gijon-Nogueron, G.; Ortega-Avila, A.B.; Kaldau, N.C.; Fahlstrom, M.; Felder, H.; Kerr, S.; King, M.; McCaig, S.; Marchena-Rodriguez, A.; Cabello-Manrique, D. Data Collection Procedures and Injury Definitions in Badminton: A Consensus Statement According to the Delphi Approach. Clin. J. Sport Med. 2022, 10.1097/JSM.0000000000001048. [Google Scholar] [CrossRef]
- Marchena-Rodriguez, A.; Gijon-Nogueron, G.; Cabello-Manrique, D.; Ortega-Avila, A.B. Incidence of injuries among amateur badminton players: A cross-sectional study. Medicine 2020, 99, e19785. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. J. Sports Sci. 2021, 35, 1098–1106. [Google Scholar] [CrossRef]
- Pluim, B.M.; Staal, J.B.; Marks, B.L.; Miller, S.; Miley, D. Health benefits of tennis. Br. J. Sports Med. 2007, 41, 760–768. [Google Scholar] [CrossRef]
- Euroinnova. Clasificación de las Etapas de la Vida por Edad. Available online: https://www.euroinova.edu.es/blog/etapas-de-la-vida-por-edad (accessed on 21 March 2022).
- Lee, E.-J.; So, W.-Y.; Youn, H.-S.; Kim, J. Effects of School-Based Physical Activity Programs on Health-Related Physical Fitness of Korean Adolescents: A Preliminary Study. Int. J. Environ. Health Res. 2021, 18, 2976. [Google Scholar] [CrossRef]
- Mohammed, M.H.H. The effect of three sport games in physical education on the health-related fitness of male university students. Eur. Phy. Educ. Rev. 2020, 24, 251–258. [Google Scholar] [CrossRef]
- Esen, H.T.; Arslan, F. The examination of postural variables in adolescents who are athletes and non-athletes. Int. J. Appl. Exerc. Physiol. 2020, 9, 140–147. Available online: https://www.proquest.com/docview/2426494395/abstract/6E930F6CCB1F470APQ/1?accountid=14542 (accessed on 20 January 2021).
- Duncan, M.J.; Noon, M.; Lawson, C.; Hurst, J.; Eyre, E. The Effectiveness of a Primary School Based Badminton Intervention on Children’s Fundamental Movement Skills. Sports 2020, 8, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buzzelli, A.A.; Draper, J.A. Examining the motivation and perceived benefits of pickleball participation in older adults. J. Aging Phys. Act. 2020, 28, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Nassef, Y.; Lee, K.J.; Nfor, O.N.; Tantoh, D.M.; Chou, M.C.; Liaw, Y.P. The Impact of Aerobic Exercise and Badminton on HDL Cholesterol Levels in Adult Taiwanese. Nutrients 2019, 11, 515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarutta, E.; Tarasova, N.; Markossian, G.; Khodzhabekyan, N.; Harutyunyan, S.; Georgiev, S. The state and dynamics of the wavefront of the eye in children with different refractions engaged in regular sport activities (badminton). Russ. Ophthalmol. J. 2019, 12, 49–58. [Google Scholar] [CrossRef]
- Takahashi, S.; Grove, P.M. Comparison of the effects of running and badminton on executive function: A within-subjects design. PLoS ONE 2019, 14, e0216842. [Google Scholar] [CrossRef] [Green Version]
- Schnohr, P.; O’Keefe, J.H.; Holtermann, A.; Lavie, C.J.; Lange, P.; Jensen, G.B.; Marott, J.L. Various leisure-time physical activities associated with widely divergent life expectancies: The copenhagen city heart study. Mayo Clin. Proc. 2018, 93, 1775–1785. [Google Scholar] [CrossRef]
- Dogruel, D.; Altintas, D.U.; Yilmaz, M. Effects of physical exercise on clinical and functional parameters in children with asthma. Cukurova Med. J. 2018, 43, 457–462. [Google Scholar] [CrossRef] [Green Version]
- Hung, C.; Tseng, J.; Chao, H.; Hung, T.; Wang, H. Effect of acute exercise mode on serum brain-derived neurotrophic factor (BDNF) and task switching performance. J. Clin. Med. Res. 2018, 7, 301. [Google Scholar] [CrossRef] [Green Version]
- Patterson, S.; Pattison, J.; Legg, H.; Gibson, A.M.; Brown, N. The impact of badminton on health markers in untrained females. J. Sports Sci. 2017, 35, 1098–1106. [Google Scholar] [CrossRef]
- Deka, P.; Berg, K.; Harder, J.; Batelan, H.; McGrath, M. Oxygen cost and physiological responses of recreational badminton match play. J. Sports Med. Phys. Fit. 2017, 57, 760–765. [Google Scholar] [CrossRef] [PubMed]
- Akin, S.; Kilinç, F.; Söyleyici, Z.; Göçmen, N. Investigation of the effects of badminton exercises on attention development in autistic children. Eur. J. Phys. Educ. Sport Sci. 2017, 3, 106–118. [Google Scholar] [CrossRef]
- Liao, K.; Meng, F.; Chen, Y. The relationship between action inhibition and athletic performance in elite badminton players and non-athletes. J. Hum. Sport Exerc. 2017, 12, 574–581. [Google Scholar] [CrossRef] [Green Version]
- Yan, W.; Li, Y. The influence of different sports on college students’ physical health. In Proceedings of the 2015 International Conference on Management Science and Innovative Education (Msie 2015), Xi’an, China, 12–13 December 2015. [Google Scholar]
- Dube, S.P.; Mungal, S.U.; Kulkarni, M.B. Simple visual reaction time in badminton players: A comparative study. Natl J Physiol. Pharm. Pharmacol. 2015, 5, 18–20. [Google Scholar] [CrossRef] [Green Version]
- Zhao, W.; Liu, K.; Li, S.; Wu, H.; Li, J. Physical education affecting on cognition and emotion: Moderate badminton training improve self-esteem, depression, and spatial memory in non-athlete junior college female students. WIT Trans. Ecol. Environ. 2014, 57, 831–838. [Google Scholar] [CrossRef]
- Stefanelli, M.L. Badminton, a sport with a potential to increase the adherence of adolescents to the physical education programme in secondary school good practices in health promotion and innovative strategies. Pensar Prática 2014, 17, 1–13. [Google Scholar] [CrossRef]
- Kim, J.; Heo, J.; Kim, J. The benefits of in-group contact through physical activity involvement for health and well-being among Korean immigrants. Int. J. Qual. Stud. Health Well-Being 2014, 9, 23517. [Google Scholar] [CrossRef] [Green Version]
- Lam, M.H.S.; Cheung, S.Y.; Chow, B.C. The effects of tai-chi-soft-ball training on physical functional health of chinese older adult. J. Hum. Sport Exerc. 2011, 6, 540–553. [Google Scholar] [CrossRef] [Green Version]
- Tervo, T.; Nordstrom, P.; Nordstrom, A. Effects of badminton and ice hockey on bone mass in young males: A 12-year follow-up. Bone 2010, 47, 666–672. [Google Scholar] [CrossRef]
- Zung, W.W.K. A self-rating depression scale. Arch. Psychiatry 1965, 12, 63–70. [Google Scholar] [CrossRef]
- Bandura, A. Self-Efficacy: The Exercise of Control; Freeman: New York, NY, USA, 1997. [Google Scholar]
- Overall, L.E.; Gorham, D.R. The Brief Psychiatric Rating Scale. Psychol. Rep. 1969, 10, 799–812. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-15: Validity of a new measure for evaluating the severity of somatic symptoms. Psychosom. Med. 2002, 64, 258–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Ng, S.S.; Lo, A.W.; Leung, T.K.; Chan, F.S.; Wong, A.T.; Lam, R.W.; Tsang, D.K.Y. Translation and validatio n of the Chinese version of the short Warwick-Edinburgh Mental Well-being Scale for patients with mental illness in Hong Kong. East Asian Arch. Psychiatry 2014, 24, 3–9. [Google Scholar] [PubMed]
- Caro, F.G.; Burr, J.A.; Caspi, E.; Mutchler, J.E. Motives That Bridge Diverse Activities of Older People. Act. Adapt. Aging 2010, 34, 115–134. [Google Scholar] [CrossRef]
- Ulrich, D.A. Test of Gross Motor Development-2; Prod-Ed: Austin, TX, USA, 2000. [Google Scholar]
- Juniper, E.F. Pediatric Asthma Quality of Life Questionnaire. Qual. Life Res. 1996, 5, 35–46. [Google Scholar] [CrossRef]
- Hung, C.L.; Huang, C.J.; Tsai, Y.J.; Chang, Y.K.; Hung, T.M. Neuroelectric and behavioral effects of acute exercise on task switching in children with attention-deficit/hyperactivity disorder. Front. Psychol. 2016, 7, 1589. [Google Scholar] [CrossRef] [Green Version]
- Markland, D.; Ingledew, D.K. The measurament of exercise motives: Factorial validity and invariance across gender of a revised Exercise Motivations Inventory. Br. J. Health Psychol. 1997, 2, 361–376. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Logan, G.D. On the ability to inhibit thought and action: A users’ guide to the stop signal paradigm. In Inhibitory Processes in Attention, Memory, and Language; Dagenbach, D., Carr, T.H., Eds.; Academic Press: San Diego, CA, USA, 1994; pp. 189–239. [Google Scholar]
- Beck, A.T. The development of depression: A cognitive model. In The Psychology of Depression: Contemporary Theory and Research; Friedman, R.J., Katz, M.M., Eds.; Winston & Sons: Washington, DC, USA, 1974. [Google Scholar]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.E. The State-Trait Anxiety Inventory (Test Manual); Consulting Psychologists Press: Palo Alto, CA, USA, 1970. [Google Scholar]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965. [Google Scholar]
- Fillenbaum, G.G. Multidimensional Functional Assessment of Older Adults: The Duke Older Americans Resources and Services Procedures; Lawrence Erlbaum Association: Hillsdale, MI, USA, 1988. [Google Scholar]
- Fernández-Fernández, J.; de la Aleja Tellez, J.G.; Moya-Ramón, M.; Cabello-Manrique, D.; Méndez-Villanueva, A. Gender differences in game responses during badminton match play. J. Strength Cond. Res. 2013, 27, 2396–2404. [Google Scholar] [CrossRef]
- Diamond, A. Executive functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| # | Authors | Year | Country | Sport | Sample | Population and Age | Duration of Intervention |
|---|---|---|---|---|---|---|---|
| 1 | Lee et al. [34] | 2021 | South Korea | AB | 120 high school students (65 M/55 W) | Teenagers. a:18.95 | 15 weeks per sport, three times a week, 35 min a session. |
| 2 | Chen et al. [25] | 2021 | USA | AB | 18 participants with intellectual disabilities (14 M/4 W) | Young people. a:22.28 | Ten lessons of 50 min, twice a week. |
| 3 | Lassandro et al. [17] | 2021 | Italy | PB | 30 professional players | Adults. Age range of 18–69 | - |
| 4 | Ng et al. [28] | 2020 | China | RB | 84 patients (35 M/49 W) | Adults. a:36.7 | - |
| 5 | Mohammed [35] | 2020 | Saudi Arabia | AB | 346 M (FVC = 169; BC = 97; CG = 80) | Teenagers. (CG = a:19.61 ± 1.24 years; FVC= a:18.24 ± 0.56 years; BC = a:19.34 ± 0.68 years) | Twice a week for eight weeks, 50 min per session. |
| 6 | Chan and Lee [27] | 2020 | UK | PB | 6 (4 M/2 W) | Adults and the elderly. a: 59.50 ± 6.37 years | - |
| 7 | Esen and Arslan [36] | 2020 | Turkey | AB | 68 M (BA =14; BX = 12; JD = 14; TA = 14; NA = 15) | Teenagers. (BA = a:13.43 ± 0.94 years); BX = a:14 ± 1.71 years); JD = a:14.50 ± 1.95 years); TA = a:15.38 ± 0.96 years); NA = a:14.67 ± 0.49 years | - |
| 8 | Duncan et al. [37] | 2020 | UK | AB | 124 children (67 M/57 W) | Children. m:8.5 ± 1.9 years | Six weeks, one session a week, 60 min per session |
| 9 | Buzzelli and Draper [38] | 2020 | USA | RB | 3012 participants (1822 M/1190 W) | Elderly. m:63.17 years | - |
| 10 | Nassef et al. [39] | 2019 | Taiwan | RB | 7797 people (3559 M/4238 W) | Adults and the elderly. 30–70 years | - |
| 11 | Tarutta et al. [40] | 2019 | Russia | RB | 40 children with refractive errors of +6.63 a −6.75 D | Children. a:9.24 ± 1.06 years | 6 months |
| 12 | Takahashi and Grove [41] | 2019 | Australia | RB | 20 participants (8 M/12 W) | Young people. a:20.9 ± 0.2 years | 3 days, ten minutes each day |
| 13 | Stovba et al. [26] | 2019 | Russia | AB | 40 students W | Teenagers. Age range 17–18 years | 2 times a week, 90 min per session. |
| 14 | Schnohr et al. [42] | 2018 | Denmark | RB | 8577 (65% M, 35% W) | Young, adults and the elderly. Age range of 20–93 years. (BA = 44 ± 14 years). | - |
| 15 | Dogruel et al. [43] | 2018 | Turkey | AB | 73 children (32 M/41 W) suffering from asm (SW = 27, SB = 26, ATL = 11, BA = 9) | Children and adolescents. a:12 ± 2.3 years | - |
| 16 | Hung et al. [44] | 2018 | Taiwan | RB | 20 students W | Young people. a:23.15 ± 2.48 years | Two sessions of 30 min separated by a period of 7 days. |
| 17 | Patterson et al. [45] | 2017 | UK | RB | 36 W healthy and untrained pre-menopausal | Adults. M:34.3 ± 6.9 years | 8 weeks |
| 18 | Deka et al. [46] | 2017 | USA | RB | 14 players W | Adults. M:35.9 ± 6.62 years | - |
| 19 | Akin et al. [47] | 2017 | Turkey | AB | 3 girls with autistic spectrum disorder | Children and adolescents. a:12.6 ± 1.5 years | Adaptation exercises for two weeks and badminton exercises for 10 weeks. |
| 20 | Liao et al. [48] | 2017 | Taiwan | PB | 42 badminton players (28 M/14 W) and 15 non-athletes (7 M/8 W) | Youth and adults. (BA = a:22.7 ± 1.5 years, NA = a:26.1 ± 2.6 years) | 30 min |
| 21 | Yan and Li [49] | 2015 | China | AB | 92 individuals of both sexes | Young people. M:20 years | 15 weeks of training in five sports (basketball, badminton, qigong, aerobics and dancing) |
| 22 | Dube et al. [50] | 2015 | India | AB | 100 M (50 belonging to the study group and 50 to the control group) | Teenagers and young people. Age range 18–22 years | - |
| 23 | Zhao et al. [51] | 2014 | China | AB | 60 W non-athletic junior university students | Adolescents. a: 18.9 years | 20 weeks, 4 days a week, 60 min a day |
| 24 | Stefanelli [52] | 2014 | Uruguay | RB | 100 participants | Adolescents. Age range 12–13 years | 9 months |
| 25 | Kim et al. [53] | 2014 | USA | RB | 13 participants | Adolescents. Over 18 years old | |
| 26 | Lam et al. [54] | 2011 | China | RB | 66 elderly individuals (27 M/39 W) | Elderly. Age range 65–75 years | 10 weeks, two training sessions per week, 60 min per session |
| 27 | Tervo et al. [55] | 2010 | Sweden | PB | 92 participants M (48 IH players, 19 BA players and 25 CP). | Teenagers and adults. Study outset: IH = 17 ± 0.4, BA players = 17.8 ± 2.5 and CP 16.9 ± 0.6. Study end: 29.0 ± 0.7 in IH players, 29.3 ± 3 in BA players and 29 ± 0.5 in CP players | - |
| # | Design | Aim | Intervention | Variables | Instruments | Conclusion/Benefits |
|---|---|---|---|---|---|---|
| 1 | E (EG) | To investigate whether PA school programs (badminton and table tennis) affect health-related physical fitness. | Badminton and table tennis PA school program | Strength, power, cardiorespiratory fitness, flexibility, body mass index (BMI). | Dynamometer. Horizontal jump, shuttle race test, sit and reach test, stadiometer | Improved muscle strength, power, cardiorespiratory fitness (endurance), flexibility and total health-related fitness score. |
| 2 | E (EG/CG) | To assess the impact of badminton classes on the health and wellbeing of young adults with intellectual disabilities. | Introductory shuttle time badminton lessons | Resting heart rate (HR), blood pressure, circumference/waist, motor performance, motor skills, depression, self-confidence | Tensiometer (OMRON-BP742N), tape measure, emotiv COPD, 6-min walking test (PM6M), individual assessment of badminton skill, depression scale [56], short scale of self-efficacy [57]. | There was a reduction in resting heart rate, an improvement in 6-min walk test performance and badminton skills. Increased frontal alpha asymmetry, which may have been due to decreased depressive symptoms in the exercise group. |
| 3 | L | To compare indicators of wellbeing and health perceptions between badminton master athletes and the adult population | - | Perception of physical and psychological health | Questionnaire on perceived quality of life, included within the Italian surveillance database “PASSI” of 2014–2017 | Significantly better perceptions were detected in high-level athletes compared with the general Italian population. Badminton improved health, psychological wellbeing and social engagement. |
| 4 | L | To examine associations between severe mental illness, general health symptoms, mental wellbeing and activity levels. | - | Patients’ somatic and mental health | Brief psychiatric assessment scale (BPRS) [58], health questionnaire (PHQ-15) [59], Pittsburgh Sleep Quality Index (PSQI) [60], mental wellbeing scale (C-SWEMWBS) [61], motivation for general activity (GAMM) [62]. | Engagement in badminton and tai chi was considered a predictor of motivation for general activity, one month after the end of the program. |
| 5 | E (2 EG/1CG) | To determine the effect of different Physical Education courses based on different sports or games on the health of university students. | Badminton training | Cardiovascular fitness, muscular endurance, explosive power, body composition, flexibility. | Cooper test, sit-ups, standing jump length, sit and stretch test | Significant improvements in all measured fitness parameters, except for body composition. |
| 6 | L | To explore the lived experiences of older people and the meaning of participation in sports, wellbeing and personality. | - | Wellbeing and personal development. | Semi-structured interviews | Improved personal development, self-expression and mood regulation. Sports participation supports wellbeing and continuous personal development in adulthood. |
| 7 | T | To check the postural differences between students who play sports (boxing, judo, taekwondo and badminton) and those who do not. | - | BMI, posture | Precision weighing instrument, B.A.K (body analysis capture) | Non-athletes had more postural asymmetries than athletes who engaged in sports such as badminton. |
| 8 | E. (EG/CG) | To examine the effects of a program on fundamental movement skills. | Structured shuttle time program | Motor skills, basic physical qualities. | Thick motor development test-2 (TGM-2) [63], Smart Speed Doors | Improvement in the quality and outcome of motor skills, with these being more significant in children aged 6–7 years. |
| 9 | T | To identify motivations for and perceived benefits of participating in pickleball in older adults. | - | Intrinsic and extrinsic motivations towards PA. Orientations towards success, perceived benefits. | Sports motivation scale. Task and ego orientation towards sport questionnaire, quality and importance of recreational services, developed by the National Intramural and Recreational Sports Association | Participants were more inclined towards the task than ego, more intrinsically motivated to perform such tasks and felt that engagement increased their desire for competition, general wellbeing and PA. |
| 10 | T | To compare high-density lipoprotein cholesterol levels between three groups of participants aged 30–70 years and classified according to physical exercise status: No exercise/aerobic/badminton. | - | Demographic, biochemical and lifestyle variables. | Data (demographic, biochemical and lifestyle) obtained from the Taiwan Biobank database. | Badminton engagement was associated with higher levels of high-density lipoprotein cholesterol. Higher HDL-C (high-density lipoprotein cholesterol) led to a lower risk of coronary heart disease. |
| 11 | E (EG) | To compare the level of aberrations, wavefront structure and its response to cycloplegia in children with different refraction profiles after a badminton program. | Badminton engagement. | Aberrations of the eye wavefront. | Aberrometer OPD-Scan III | Regular badminton engagement produced significant changes in wavefront aberrations, which is indicative of a strengthening of the ligaments of the lens and normalization of the tone of the ciliary muscle. |
| 12 | E (EG) | To compare the effects of badminton and running on inhibitory function. | Running, playing badminton and resting sitting down. | Aerobic capacity, heart rate, range of perceived exertion, volitional exhaustion, inhibitory function. | Motor treadmill, indirect calorimetry system (MetaMax-3B), Polar heart rate monitor (Model RS800cx), reverse Stroop task | A single session of complex exercise (badminton) produced greater benefits to inhibitory function than one session of simple exercise (running). |
| 13 | E (EG/CG) | To analyse the benefits of an academic physical education model, based on badminton, on the physical qualities and anthropometric characteristics of students. | Badminton-driven academic Physical Education model. | Physical qualities, anthropometric characteristics. | Push-ups in prone position, standing long jump, seated push-ups, 100 metre sprint test and 2000 metre race, circumference (size) and length measurements | The program improved speed by 10%, flexibility by 12%, endurance by 6% and power by 8%. It was also beneficial for body shaping, increasing the muscle mass of sport-specific limbs. |
| 14 | L | To examine the impact on life expectancy of participation in various sports. | - | PA levels, alcohol consumption, diabetes, blood pressure, cardiorespiratory fitness, strength, self-rated health, social network, vital exhaustion. | PA questionnaire, sphygmomanometer, electrocardiogram, blood tests | Badminton engagement increased life expectancy by 6.2 years when compared with a sedentary group. |
| 15 | L | To investigate the effect of regular exercise on asthma symptoms, quality of life and lung function in children with asthma. | - | Asthma symptoms, forced expiratory volume. Physical, mental and social disorders. | Asthma measurement form, Quality of life questionnaire in children with asthma (PAQLQ) [64], spirometer | Badminton engagement significantly improved asthma symptoms and increased forced expiratory volume. |
| 16 | E (EG) | To compare the effect of badminton engagement and running on brain-derived neurotrophic factor (BDNF) production and task change performance. | Badminton session | Cardiac frequency, perceived effort, haematocrit level, brain-derived neurotrophic factor, cognitive performance, reaction time. | Wireless heart rate monitor (BioHarness Team System), perceived effort scale, venous blood machine, task change paradigm [65]. | Badminton led to higher levels of brain-derived neurotrophic factor compared with running. Demonstrated benefits of practising open skills (badminton) on brain-derived neurotrophic factor and executive function. |
| 17 | E (2EG/1CG) | To examine the effects of engaging in 8 weeks of recreational badminton in untrained women. | Badminton training | Physiological parameters, vertical jump, Height and body mass, body fat percentage, body density, exercise motivations, physical self-esteem. | Microvettes (CB300), Randox Monza UK analyser, Biosen C-Line Analyzer (EKF Diagnostics), sphygmomanometer (Omron M5), treadmill, Erymetro (Oxycon Pro), force platforms (PS2142), BODPOD scales, anthropometric tape (Lufkin W606 PM), reasons for exercise questionnaire (EMI-2; [66]). Physical self-perception. | Increased VO2max to exhaustion, vertical jump height, social commitment and motivation towards exercise. Decreased blood pressure and heart rate at rest and during submaximal running. |
| 18 | L | To determine oxygen consumption during an RB match and intensity, measured according to American College of Sports Medicine criteria and categorised as moderate or vigorous. | Badminton matches | Aerobic capacity, lactate concentration, range of perceived exertion, step count, heart rate, energy expenditure | Portable metabolic system, lactate analyser, Borg scale [67], pedometer, Polar watch and chest strap | RB was categorised as being of vigorous intensity, providing a potential means of meeting recommended PA levels and improving aerobic fitness. |
| 19 | E (EG) | To investigate the effect of simplified badminton exercises on the development of attention and retention level in individuals with autistic spectrum disorder. | Badminton Exercise Program | Level of care, mental retention capacity | Attention test, visual memory test, effect test. | A positive effect was achieved in the level of attention, development of eye contact, prolonged focusing on objects and attention development. |
| 20 | E (EG/CG) | To investigate the effect of expertise on action inhibition in badminton players and non-athletes. | Cognitive tests | Motor inhibition | Stop sign paradigm [68] | Badminton players were more likely to successfully inhibit their responses during stop trials, with responses being better in those who competed at higher levels. |
| 21 | E (EG) | To examine the effect of five sports on the physical health of students following fifteen weeks of training. | Special training in five different sports | Vital capacity, resistance, velocity, grip strength, squats, jumps, sit-ups | “China’s National Student Physical Health Standard” (CNSPFS). | Badminton had a beneficial effect on heart and lung function, speed and flexibility. In addition, it led to significant improvements in flexibility in girls. |
| 22 | T | To compare the visual reaction time of badminton players with control individuals of the same age. | - | Visual reaction time | Visual reaction time recorder | Badminton is beneficial in terms of improving hand-eye reaction time, muscle coordination, cognitive functions, alertness and concentration. |
| 23 | E (EG/CG) | To assess the effects of 20 weeks of aerobic exercise on symptoms of depression, anxiety and self-esteem in non-athlete university students. | Aerobic badminton exercise | Depression, anxiety, self-esteem | Depression inventory [69], inventory of state-trait anxiety [70], self-esteem inventory [71]. | Students who performed badminton exercises significantly decreased levels of depression and anxiety and improved their self-esteem. |
| 24 | L | To examine whether badminton facilitates the “participation” of adolescents in other activities. | School year dedicated to badminton | Level of effective participation | Observation | Participation in badminton classes may be a strategic and determining factor of increasing and maintaining adherence to PE classes. |
| 25 | L | To examine the benefits of PA engagement in members of the same ethnic group. | - | Perceived benefits | Interview | Korean immigrant participants gained various social and cultural benefits. Highlight the psychological benefits perceived by participants. |
| 26 | E (EG/CG) | to investigate the effects of a combined Tai Chi and badminton training program on the functional physical health of older people. | Combined tai chi and badminton training | Functional physical health, strength, flexibility, agility, balance, aerobic resistance, hand–eye coordination | Activities of daily living scale (OARS-IADL) [72], physical fitness test for seniors, hand grip strength test, AAHPER fitness test | Functional physical health, manipulative skills and self-perceived functional health were improved. In addition, the program can serve as a tool to slow down inevitable biological degradation as individuals aged. |
| 27 | L | To investigate the influence of different types of PA using weights on bone mineral density and evaluate final residual benefits. | - | Bone mineral density, fatty acid profile, vitamin D, markers of bone metabolism. | Lunar DPX-L dual energy X-ray absorber, liquid chromatograph HP1100 | Data indicated higher bone mineral density in the neck of the femur, humerus, lumbar spine and legs of badminton players relative to hockey players. |
| Population | Articles | Percentage |
|---|---|---|
| Children | n = 4 | 14.8% |
| Adolescents | n = 11 | 40.7% |
| Young people | n = 7 | 25.9% |
| Adults | n = 8 | 29.6% |
| Elderly | n = 5 | 18.5% |
| Type of Health | Number of Articles | Percentage |
|---|---|---|
| Physical health | n =17 | 63% |
| Mental health | n =10 | 37% |
| Social health | n =8 | 29.6% |
| Type of Health | Specific Benefits | Population and Gender |
|---|---|---|
| Physical Health | Improvements in heart function | Adult women, young women and men, and young women and men with intellectual disabilities [25,45,49] |
| Improvements in lung function (breathing capacity) | Adults of both sexes, young people of both sexes, children and adolescents of both sexes [43,44,45,46,49] | |
| Strengthens the ligaments of the lens | Children with various optical refractions [40] | |
| Reduces postural asymmetries between those who engage in and do not engage in sport. | Adolescents of both sexes [36] | |
| Lower risk of coronary heart disease | Adults and elderly men and women [39] | |
| Body shape benefits | Adolescent girls (16) | |
| Strengthens functional physical health and self-perceived functional health and slows biological degradation | Elderly men and women [54] | |
| Increases bone mineral density in the neck of the femur, humerus and lumbar spine | Adolescent males as they progress into adulthood [55] | |
| Increases life expectancy beyond other sports such as football, cycling and swimming. | Young, adult and elderly men and women [42] | |
| Improves basic physical abilities (speed, flexibility, endurance and strength) | Adolescents of both sexes [26,34,35] | |
| Improves speed | Young men and women [49] | |
| Improves flexibility | Young women [50] | |
| Improves vertical jump | Adult women [44] | |
| Better muscle coordination | Adolescents and young men [50] | |
| Improves manipulative skills | Elderly men and women [54] | |
| Improves motor skills | Boys and girls, with the most significant changes in the youngest children [37] | |
| Mental health | Improves inhibition | Young people and adults of both sexes [41,48] |
| Improves cognitive function, alertness and concentration | Male adolescents and young adults [50] | |
| Improves attention | Children and adolescents of both sexes with autistic spectrum disorder [47] | |
| Reduces depressive symptoms | Young men and women with intellectual disabilities and adolescent girls [25,51] | |
| Predictor of general motivation for activity | Adult patients of both sexes referred to occupational therapy [28] and adolescents [52] | |
| Social Health | Improves social relationships | Adult women [45] and professional players [18] |
| Supports personal development and mood regulation | Adults and elderly men and women [27] | |
| Increases intrinsic motivation | Elderly men and women [38] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cabello-Manrique, D.; Lorente, J.A.; Padial-Ruz, R.; Puga-González, E. Play Badminton Forever: A Systematic Review of Health Benefits. Int. J. Environ. Res. Public Health 2022, 19, 9077. https://doi.org/10.3390/ijerph19159077
Cabello-Manrique D, Lorente JA, Padial-Ruz R, Puga-González E. Play Badminton Forever: A Systematic Review of Health Benefits. International Journal of Environmental Research and Public Health. 2022; 19(15):9077. https://doi.org/10.3390/ijerph19159077
Chicago/Turabian StyleCabello-Manrique, David, Juan Angel Lorente, Rosario Padial-Ruz, and Esther Puga-González. 2022. "Play Badminton Forever: A Systematic Review of Health Benefits" International Journal of Environmental Research and Public Health 19, no. 15: 9077. https://doi.org/10.3390/ijerph19159077
APA StyleCabello-Manrique, D., Lorente, J. A., Padial-Ruz, R., & Puga-González, E. (2022). Play Badminton Forever: A Systematic Review of Health Benefits. International Journal of Environmental Research and Public Health, 19(15), 9077. https://doi.org/10.3390/ijerph19159077