
Analysis of the Elderly’s Preferences for Choosing Medical Service Facilities from the Perspective of Accessibility: A Case Study of Tertiary General Hospitals in Hefei, China


Abstract
:1. Introduction
1.1. The Elderly and Their Medical Decisions
1.2. Hypothesis and Aims of the Study
2. Methodology
2.1. One-to-One Interviews at the Hospital
2.2. OD Cost Matrix Analysis
2.3. Telephone Follow-Up Interviews
2.4. Statistical Analysis
- (1)
- In order to analyze the preference for hospital distance among the elderly with different attributes, the chi-squared test was performed on their basic attributes of the elderly and perceived importance of distance. The elderly’s preference for distance, or, namely, the importance of distance, was used as the dependent variable. The elderly’s attributes of gender, age, household registration type, number of people at home, number of generations at home, education background, original occupation, number of children, household per capita annual income, medical insurance type, travel activity status, residence place, and number of private cars owned were used as independent variables (see Appendix A Table A3 for assignment of variables). Upon the chi-squared test, statistically significant attributes (p < 0.05) were screened out. Then, multiple correspondence analysis was performed again on these significant attributes and the preference for distance.
- (2)
- In order to analyze the regularity of the elderly’s behaviors in seeking medical treatment nearby, the chi-squared test was also firstly performed on the data. The elderly’s actual behaviors, or, namely, whether or not they chose the nearest hospital, was used as the dependent variable, and the attributes of the elderly were used as independent variables (see Table A3 for assignment of variables), thus identifying the relationship between the elderly’s attributes and their behaviors in seeking medical treatment.
- (3)
- In order to find out the factors associated with the elderly’s behaviors in seeking medical treatment nearby, statistical analysis was conducted for the elderly’s evaluation on accessibility under different means of transportation and their actual behaviors (whether they chose the nearest hospital) on the basis of the data obtained from telephone interviews. The assignment of variables are referred to in Table A3. After the statistically significant accessibility factors were screened out through the chi-squared test, regression analysis was performed again to finally identify the accessibility factors related to the elderly’s actual behaviors.
3. Results and Analysis
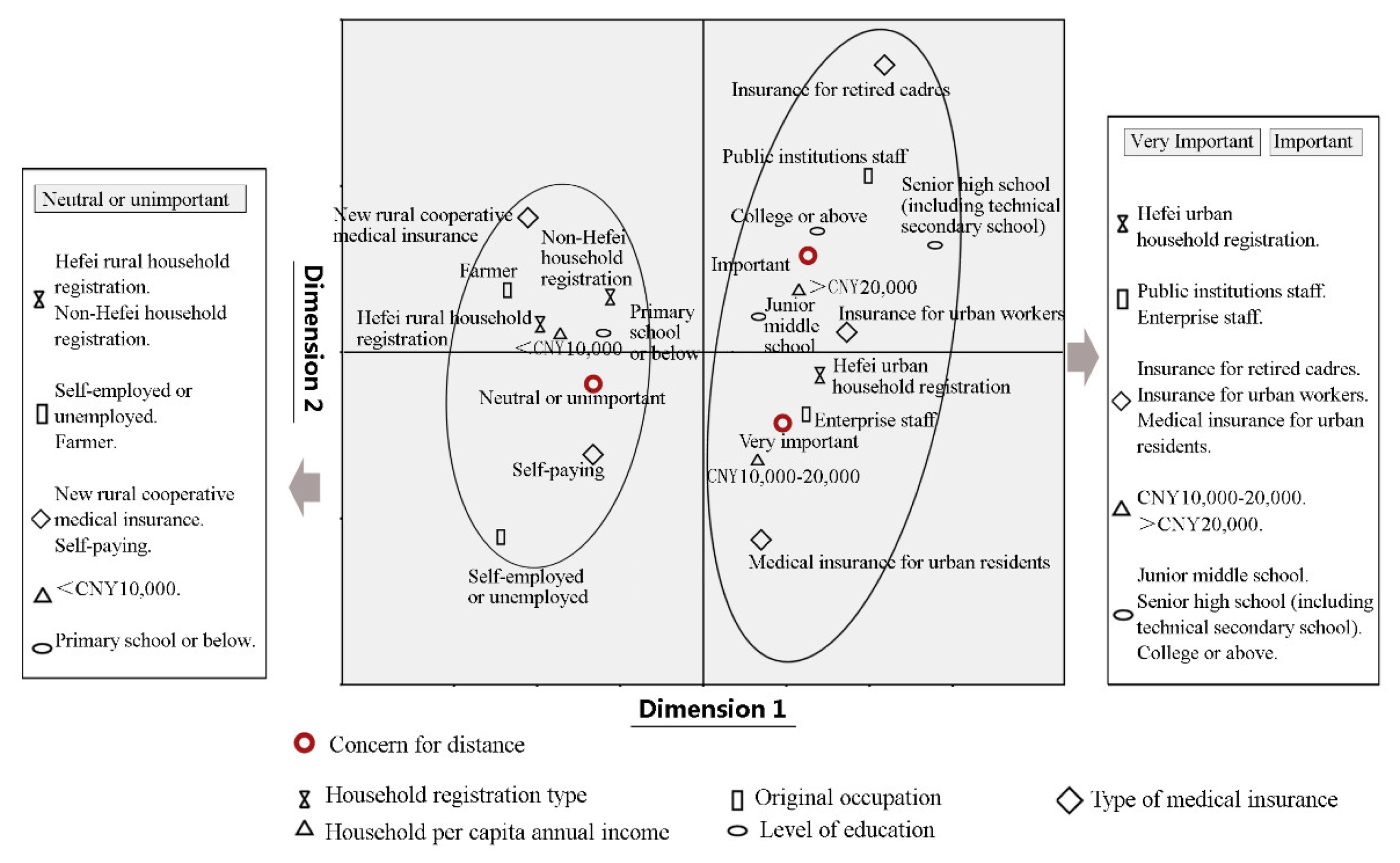
3.1. Elderly Preferences for Distance
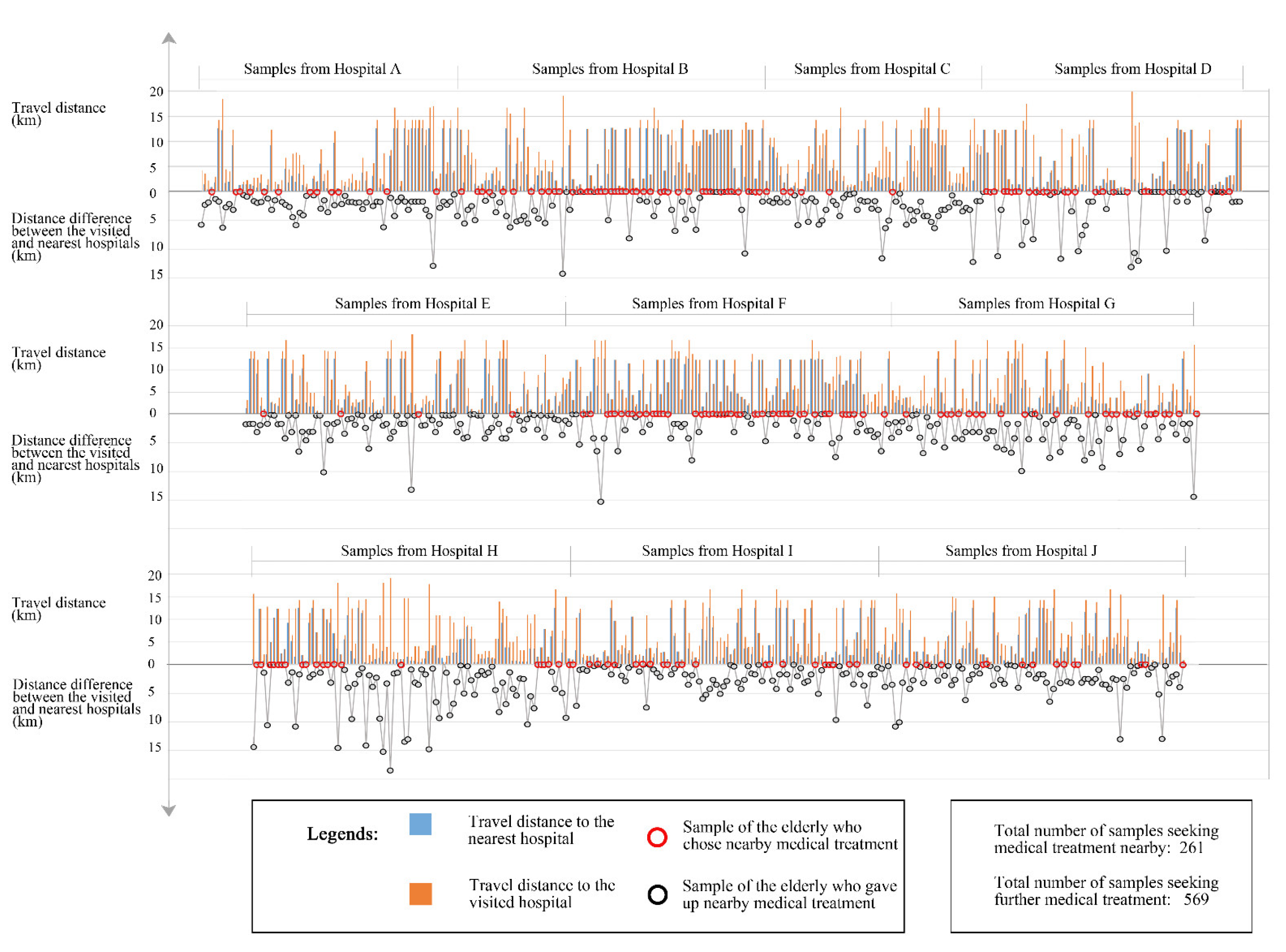
3.2. Regularity of Choosing Nearby Medical Treatment for Older People
3.3. Association between Hospital Accessibility Factors and Elderly Behavior
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Categories of Indicators | Details about the Indicators | Standard |
|---|---|---|
| Beds | Approved number of beds | ≥500 |
| Number of actually available beds | ≥500 | |
| Average bed occupancy | 93–100% | |
| Health professionals | Ratio of health professionals to available beds | ≥1.2:1 |
| The ratio of total nurses of hospital to available beds | ≥0.4:1 | |
| The ratio of nurses in the ward to available beds | ≥0.4:1 | |
| The ratio of full-time staff in charge of hospital infection management to available beds | Not less than 4 professionals in case the hospital’s beds are ≤500 | |
| Resources of relevant departments | (1) Emergency Medicine Department | |
| The ratio of fixed emergency physicians to emergency physicians on duty | ≥75% | |
| The ratio of fixed emergency nurses to emergency nurses on duty | ≥75% | |
| (2) Department of Critical Care Medicine | ||
| The ratio of available beds in the Department of Critical Care Medicine to available beds in hospital | ≥5% | |
| The ratio of physicians to available beds in Department of Critical Care Medicine | ≥0.8:1 | |
| The ratio of nurses to available beds in Department of Critical Care Medicine | ≥3:1 | |
| (3) Anesthesiology department | ||
| The number of anesthesiologists and operating rooms (including the number of operating rooms for painless diagnosis and treatment) in the Anesthesiology department | ≥2:1 | |
| The ratio of anesthesiologists to the average annual general anesthesia operations | ≥1:400 | |
| (4) Traditional Chinese Medicine Department | ||
| The ratio of available beds in the Traditional Chinese Medicine Department to available beds in the hospital | ≥3% | |
| The ratio of physicians to available beds in the Traditional Chinese Medicine Department | ≥0.4:1 | |
| The ratio of nurses to available beds in the Traditional Chinese Medicine Department | ≥0.4:1 | |
| (5) Rehabilitation Medicine Department | ||
| The ratio of available beds in the Rehabilitation Medicine Department to available beds in the hospital | ≥2% | |
| The ratio of physicians to available beds in the rehabilitation department | ≥0.2:1 | |
| The ratio of rehabilitation specialists to available beds in the Rehabilitation Medicine Department | ≥0.3:1 | |
| The ratio of nurses to available beds in the Rehabilitation Medicine Department | ≥0.3:1 | |
| (6) Infectious Diseases Department | ||
| The ratio of fixed physicians to physicians on duty in the Infectious Diseases Department | ≥75% | |
| The ratio of nurses to the number of nurses on duty in the Infectious Diseases Department | ≥75% | |
| The ratio of available beds in the Infectious Diseases Department to available beds in the hospital | ≥3% | |
| The ratio of convertible infectious disease beds to available beds in the hospital | ≥15% | |
| (7) Department of Geriatric Medicine | ||
| Number of available beds in the Department of Geriatric Medicine | ≥20 | |
| The ratio of geriatricians to available beds in the Department of Geriatric Medicine | ≥0.3:1 | |
| The ratio of nurses to available beds in the Department of Geriatric Medicine | ≥0.6:1 | |
| Operation indicators | Ratio of annual surgeries in related operating departments to discharges | ≥65% |
| Available bed occupancy | 93–100% | |
| Proportion of personnel expenditure in business expenditure | ≥35% | |
| Scientific research indicators | Number of clinical converted new technologies | Gradual improvement within the review cycle |
| Number of relevant national clinical patents | Gradual improvement within the review cycle | |
| Hospital | Number of Questionnaires Distributed | Number of Excluded Questionnaires | Number of Included Questionnaires | |
|---|---|---|---|---|
| The Questionnaires Were Invalid | The Respondents Were from Outside Hefei Urban City | |||
| A | 100 | 8 | 18 | 74 |
| B | 100 | 9 | 5 | 86 |
| C | 100 | 16 | 21 | 63 |
| D | 100 | 12 | 17 | 71 |
| E | 100 | 1 | 8 | 91 |
| F | 100 | 2 | 3 | 95 |
| G | 100 | 5 | 11 | 84 |
| H | 100 | 3 | 6 | 91 |
| I | 100 | 5 | 8 | 87 |
| J | 100 | 2 | 10 | 88 |
| Total | 1000 | 170 | 830 | |
| Variable | Variable Assignment |
|---|---|
| Gender | 1 = Male, 2 = Female |
| Age | 1 = 60–70, 2 = 71–80, 3 ≥ 80 |
| Household registration type | 1 = Hefei urban household registration, 2 = Hefei rural household registration, 3 = non-Hefei household registration |
| Number of people living at home | 1 = 1, 2 = 2, 3 ≥ 3 |
| Number of generations living at home | 1 = one generation, 2 = two generations, 3 = three or more generations |
| Level of education | 1 = primary school or below, 2 = junior middle school, 3 = senior high school (including technical secondary school), 4 = college or above |
| Original occupation | 1 = public institutions staff, 2 = enterprise staff, 3 = self-employed or unemployed, 4 = farmer |
| Number of children | 1 = none, 2 =1, 3 = 2, 4 ≥ 3 |
| Household per capita annual income | 1 ≤ CNY 10,000, 2 = CNY 10,000–20,000, 3 ≥ CNY 20,000 |
| Type of medical insurance | 1 = medical insurance for retired cadres, 2 = medical insurance for urban workers, 3 = medical insurance for urban residents, 4 = new rural cooperative medical insurance, 5 = self-paying |
| Travel activity status | 1 = travel independently without the aid of auxiliary devices, 2 = travel independently with the aid of auxiliary devices, 3 = cannot travel independently |
| Place of residence | 1 = within the First Ring, 2 = between the First and the Second Ring, 3 = outside the Second Ring, within the urban area |
| Number of private cars owned | 1 = none, 2 = 1, 3 = 2 |
| Importance of distance | 1 = very important, 2 = important, 3 = neutral or not important |
| Whether to choose the nearest hospital | 1 = yes, 2 = no |
| Convenience of station | 1 = convenient, 2 = neutral, 3 = inconvenient |
| Road congestion | 1 = not congested, 2 = neutral, 3 = congested |
| Convenience of parking | 1 = convenient, 2 = neutral, 3 = inconvenient |
| Barrier-free facilities on the way | 1 = complete, 2 = neutral, 3 = incomplete |
References
- The State Council. Opinions on Formulating and Implementing Elderly Care Service Projects. 2017. Available online: http://www.gov.cn/zhengce/content/2017-06/16/content_5203088.htm (accessed on 15 May 2022).
- Dai, B. The old age health security in rural China: Where to go? Int. J. Equity Health 2015, 14, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Malik, V.; Hu, F.B. Health insurance in China: After declining in the 1990s, coverage rates rebounded to near-universal levels by 2011. Health Aff. 2017, 36, 1452–1460. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Short, S.E. Health insurance coverage rates in 9 provinces in china doubled from 1997 to 2006, with a dramatic rural upswing. Health Aff. 2011, 30, 2419–2426. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Tang, W.; Zhang, X.; Zhang, Y.; Zhang, L. National health insurance development in China from 2004 to 2011: Coverage versus benefits. PLoS ONE 2015, 10, e0124995. [Google Scholar] [CrossRef]
- Kaambwa, B.; Ratcliffe, J.; Shulver, W.; Killington, M.; Taylor, A.; Crotty, M.; Kidd, M.R. Investigating the preferences of older people for telehealth as a new model of health care service delivery: A discrete choice experiment. J. Telemed. Telecare 2016, 23, 301–313. [Google Scholar] [CrossRef] [Green Version]
- Du, M.; Cheng, L.; Li, X.; Yang, J. Factors affecting the travel mode choice of the urban elderly in healthcare activity: Comparison between core area and suburban area. Sustain. Cities Soc. 2020, 52, 101868. [Google Scholar] [CrossRef]
- Jana, A.; Ohmori, N.; Harata, N. Choice based on accessibility & social determinants–a case of elderly health care decision and health trips in India. In Proceedings of the 13th International Conference on Mobility and Transport for Elderly and Disabled Persons’ TRANSED, New Delhi, India, 9–21 September 2012. [Google Scholar]
- Teng, Y.-H.; Teng, J.-J.; Lee, M.-Y.; Hsieh, M.-H.; Chen, Y.-J.; Lin, J.-Y.; Lee, M.-C. Determinants of emergency medical utilization among the elderly population in Taiwan: A national longitudinal cohort study. Arch. Gerontol. Geriatr. 2013, 56, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Chai, Y. Urban Elderly Activity Space in China; Science Press: Beijing, China, 2010. [Google Scholar]
- Yang, Y.-T.; Iqbal, U.; Ko, H.-L.; Wu, C.-R.; Chiu, H.-T.; Lin, Y.-C.; Lin, W.; Hsu, Y.-H.E. The relationship between accessibility of healthcare facilities and medical care utilization among the middle-aged and elderly population in Taiwan. Int. J. Qual. Health Care 2015, 27, 222–231. [Google Scholar] [CrossRef] [Green Version]
- Olness, K.; Loue, S. Coping with daily living: Housing, finances, transportation, medical care. Care Manag. J. 2004, 5, 221–227. [Google Scholar] [CrossRef]
- Patil, S.D.; Angadi, M.M.; Mayappanavar, R.; Saravanan, E. A study of factors associated with health seeking behaviour of elderly in rural field practice area of Shri B. Int. J. Health Sci. Res. 2014, 4, 43–47. [Google Scholar]
- Zhou, J.; Chai, Y. Advances in spatial behavior of the elderly in China. Prog. Geogr. 2013, 32, 722–732. [Google Scholar]
- Gao, Y.; Li, Z. Optimization and adjustment of multilevel medical facilities for the elderly from the perspective of accessibility. J. Urban Plan. Dev. 2022, 148, 05022011. [Google Scholar] [CrossRef]
- Love, D.; Lindquist, P. The geographical accessibility of hospitals to the aged: A geographic information systems analysis within Illinois. Health Serv. Res. 1995, 29, 629–651. [Google Scholar] [PubMed]
- Ingram, D.R. The concept of accessibility: A search for an operational form. Reg. Stud. 1971, 5, 101–107. [Google Scholar] [CrossRef]
- Baxter, R.; Lenzi, G. The measurement of relative accessibility. Reg. Stud. 1975, 9, 15–26. [Google Scholar] [CrossRef]
- Kirby, H.R. Accessibility indices for abstract road networks. Reg. Stud. 1976, 10, 479–482. [Google Scholar] [CrossRef]
- Wachs, M.; Kumagai, T. Physical accessibility as a social indicator. Socio-Econ. Plan. Sci. 1973, 7, 437–456. [Google Scholar] [CrossRef]
- Nam, Y.C.; Park, K.O. The present condition of nursing home & accessibility to health center and hospital from nursing home in rural area by web GIS analysis. J. Korean Inst. Rural. Archit. 2010, 12, 29–36. [Google Scholar]
- Silva ME, C.; Johnson, M.P. Improving geographic accessibility to community-based health facilities in Davao City through location-allocation models. Acta Med. Philipp. 2009, 43, 18–24. [Google Scholar]
- Ye, Z.; Wen, Z.; Tian, Z.; Liu, Q.; Li, Y.; He, F.; Liu, Z. Analysis on the operation mode of community health service centers established by large tertiary first-class hospitals and district governments. Chin. Health Serv. Manag. 2020, 037, 13–15. [Google Scholar]
- Wei, L. Continuity-fragmentation-integration: Historical review of health service delivery modes from three-level health service networks in rural China. Chin. J. Health Policy 2014, 7, 24–30. [Google Scholar] [CrossRef]
- National Health Commission. Notice of the National Health Commission on the Issuance of Tertiary Hospital Evaluation Standards (2020 Edition). 2020. Available online: http://www.gov.cn/zhengce/zhengceku/2020-12/28/content_5574274.htm (accessed on 9 April 2022).
- Zhang, F.; Li, D.; Ahrentzen, S.; Zhang, J. Assessing spatial disparities of accessibility to community-based service resources for Chinese older adults based on travel behavior: A city-wide study of Nanjing, China. Habitat. Int. 2019, 88, 101984. [Google Scholar] [CrossRef]
- Sun, S.; Xie, Z.; Yu, K.; Jiang, B.; Zheng, S.; Pan, X. COVID-19 and healthcare system in China: Challenges and progression for a sustainable future. Glob. Health 2021, 17, 1–8. [Google Scholar] [CrossRef] [PubMed]
- National Development and Reform Commission. Implementation Plan for the Constructing Efficient and High-Quality Medical and Health Service System During the 14th Five-Year Plan. 2021. Available online: https://www.ndrc.gov.cn/xxgk/zcfb/tz/202107/t20210701_1285212.html?code=&state=123 (accessed on 25 May 2022).
- Hefei Municipal Government. The Administrative Division. 2018. Available online: http://www.hefei.gov.cn/mlhf/sq/csgk/xzqh/index.html (accessed on 12 December 2021).
- Gao, Y.; Li, Z.; Zhu, G.; Zheng, Z. Spatial allocation of urban medical facilities for the elderly in China: With Hefei City as example. China City Plan. Rev. 2019, 28, 6–17. [Google Scholar]
- Hefei Municipal Government. The 13th Five-Year Plan for the Establishment of Medical Institutions in Hefei. 2017. Available online: http://zwgk.hefei.gov.cn/zwgk/public/spage.xp?doAction=view&indexno=002990482/201704-00081 (accessed on 10 October 2021).
- Hefei Municipal Bureau of Statistics. Statistical Annual Report of 2017: Culture, Education and Health. 2018. Available online: http://tjj.hefei.gov.cn/tjnj/2018nj/11569151.html (accessed on 12 December 2021).
- Li, Z.; Liu, R.; Liu, H. PASS Tests for Efficacy and Sample Size Estimates; Electronic Industry Press: Beijing, China, 2020. [Google Scholar]
- Wu, M. Questionnaire Statistical Analysis Practice; Chongqing University Press: Chongqing, China, 2010. [Google Scholar]
- Zhan, J.; Fu, H. Hospital reputation, spatial distance and patient choice-evidence from hospital discharge data. China Econ. Q. 2022, 22, 43–364. [Google Scholar]
- Pan, C. Hospital reputation and patient behavior. Health Econ. Res. 2006, 8, 50. [Google Scholar]
- Dou, K.; Zhan, Q. Accessibility analysis of urban emergency shelters: Comparing gravity model and space syntax. In Proceedings of the International Conference on Remote Sensing, Environment and Transportation Engineering, Nanjing, China, 24–26 June 2011; pp. 5681–5684. [Google Scholar]
- Jiang, A. A computational algorithm of urban accessibility based on experiential taxi path. Prog. Geogr. 2012, 31, 711–716. [Google Scholar]
- Rotar, A.S.; Pop, I.; Matei, F.; Andronie, L.; Vatca, A.; Cioban, A. Modelling a logistic problem by creating an origin-destination cost matrix using GIS technology. Bull. Univ. Agric. Sci. Vet. Med. Cluj-Napoca. Hortic. 2014, 71, 2014. [Google Scholar]
- Widyawan Prakasa, B.; Putra, D.W.; Kusumawardani, S.S.; Habibie, F. Big data analytic for estimation of origin-destination matrix in Bus Rapid Transit system. In Proceedings of the 2017 3rd International Conference on Science and Technology-Computer (ICST), Yogyakart, Indonesia, 11–12 July 2017. [Google Scholar]
- Yang, H.; Meng, Q.; Bell MG, H. Simultaneous estimation of the origin-destination matrices and travel-cost coefficient for congested networks in a stochastic user equilibrium. Transp. Sci. 2001, 35, 107–123. [Google Scholar] [CrossRef]
- Zhang, W.; Dong, W. Advanced Tutorial on SPSS Statistical Analysis; Higher Education Press: Beijing, China, 2004. [Google Scholar]
| Means of Transportation | Category of Accessibility Evaluation | Evaluation Index | Criteria of Evaluation Index |
|---|---|---|---|
| Public transportation | Total time | Time (min) | Time spent from home to the station/waiting time/riding time/time for transfer/time spent from the station to the hospital/other required timings |
| Total cost | Cost (CNY) | Fare/other required expenses | |
| Number of transfers | N | Number of transfers | |
| Convenience of station | Convenient/neutral/inconvenient | Distance from home to the station/distance from the station to the hospital | |
| Road congestion | Not congested/neutral/congested | Number of intersections and waiting time at intersections/number of passable lanes on the way/density of vehicles on the road/traffic order on the way | |
| Barrier-free facilities on the way | Complete/neutral/incomplete | Barrier-free setting on the way from home to the station/setting in the station/setting on the vehicle/setting on the way of transfer/setting on the way from the station to the hospital | |
| Private motor vehicle | Total time | Time (min) | Time spent from home to the parking lot/driving time/time spent in the process of parking/time spent from the parking lot to the hospital/other required timings |
| Total cost | Cost (CNY) | Fuel cost/toll/parking cost/other required expenses | |
| Road congestion | Not congested/neutral/congested | Number of intersections and waiting time at intersections/number of passable lanes on the way/density of vehicles on the road/traffic order on the way | |
| Convenience of parking | Convenient/neutral/inconvenient | Number of parking spaces/distance between the parking lot and the hospital | |
| Barrier-free facilities on the way | Complete/neutral/incomplete | Barrier-free setting in the parking lot/setting on the way from the parking lot to the hospital | |
| Non-motorized vehicle | Total time | Time (min) | Time spent from home to the parking lot/riding time/time spent in the process of parking/time spent from the parking lot to the hospital/other required timings |
| Total cost | Cost (CNY) | Rental fee for the vehicle/electricity or other consumption expenses/parking cost/other required expenses | |
| Road congestion | Not congested/neutral/congested | Number of intersections and waiting time at intersections/number of passable lanes on the way/density of vehicles on the road/traffic order on the way | |
| Convenience of parking | Convenient/neutral/inconvenient | Number of parking spaces/distance between the parking lot and the hospital | |
| Mixed-mode of transportation | Total time | Time (min) | Time spent from home to the station or parking lot/waiting time/riding or driving time/time for transfer/time spent in the process of parking/time spent from the station or parking lot to the hospital/other required timings |
| Total cost | Cost (CNY) | Fare/fuel, electricity or other consumption expenses/toll/rental fee for the vehicle/parking cost/other required expenses | |
| Number of transfers | N | Number of transfers | |
| Convenience of station | Convenient/neutral/inconvenient | Distance from home to the station/distance from the station to the hospital | |
| Road congestion | Not congested/neutral/congested | Number of intersections and waiting time at intersections/number of passable lanes on the way/density of vehicles on the road/traffic order on the way | |
| Convenience of parking | Convenient/neutral/inconvenient | Number of parking spaces/distance between the parking lot and the hospital | |
| Barrier-free facilities on the way | Complete/Neutral/Incomplete | Barrier-free setting on the way from home to the station/setting in the station/setting on the vehicle/setting on the way of transfer/setting on the way from the station to the hospital/setting in the parking lot/setting on the way from the parking lot to the hospital | |
| Walking | Total time | Time (min) | Time spent on the way |
| Total cost | Cost (CNY) | Expenses on the way | |
| Road congestion | Not congested/neutral/congested | Number of intersections and waiting time at intersections/density of pedestrians on the road/traffic order on the way | |
| Barrier-free facilities on the way | Complete/neutral/incomplete | Barrier-free setting on the way |
| Variable | Values | Number (N) | Percentage (%) | Variable | Values | Number (N) | Percentage (%) |
|---|---|---|---|---|---|---|---|
| Gender | Male | 486 | 58.6 | Number of children | None | 9 | 1.1 |
| Female | 344 | 41.4 | 1 | 137 | 16.5 | ||
| Age | 60–70 | 352 | 42.4 | 2 | 335 | 40.4 | |
| ≥3 | 349 | 42.0 | |||||
| 71–80 | 320 | 38.6 | Household per capita annual income | <CNY 10,000 (<USD 1480) | 246 | 29.6 | |
| >80 | 158 | 19.0 | CNY 10,000–20,000 (USD 1480–2960) | 252 | 30.4 | ||
| Household registration type | Hefei urban household registration | 445 | 53.6 | >CNY 20,000 (>USD 2960) | 332 | 40.0 | |
| Hefei rural household registration | 218 | 26.3 | Type of medical insurance | Medical insurance for retired cadres | 60 | 7.2 | |
| Non-Hefei household registration | 167 | 20.1 | Medical insurance for urban workers | 278 | 33.5 | ||
| Number of people living at home | 1 | 89 | 10.7 | Medical insurance for urban residents | 171 | 20.6 | |
| 2 | 428 | 51.6 | New rural cooperative medical insurance | 297 | 35.8 | ||
| ≥3 | 313 | 37.7 | Self-paying | 24 | 2.9 | ||
| Number of generations living at home | One generation | 512 | 61.7 | Travel activity status | Travel independently without the aid of auxiliary devices | 335 | 40.4 |
| Two generations | 87 | 10.5 | Travel independently with the aid of auxiliary devices | 326 | 39.3 | ||
| Three or more generations | 231 | 27.8 | Cannot travel independently | 169 | 20.4 | ||
| Level of education | Primary school or below | 427 | 51.4 | Place of residence | Within the First Ring | 256 | 30.8 |
| Junior middle school | 281 | 33.9 | Between the First and the Second Ring | 343 | 41.3 | ||
| Senior high school (including technical secondary school) | 79 | 9.5 | |||||
| College or above | 43 | 5.2 | Outside the Second Ring, within the urban area | 231 | 27.8 | ||
| Original occupation | Public institutions staff | 168 | 20.2 | ||||
| Enterprise staff | 256 | 30.8 | Number of private cars owned | None | 329 | 39.6 | |
| Self-employed or unemployed | 135 | 16.3 | 1 | 420 | 50.6 | ||
| Farmer | 271 | 32.7 | ≥2 | 81 | 9.8 |
| Distance Importance (Variable Assignment) | Number (N) | Percentage (%) |
|---|---|---|
| Very important (1) | 115 | 13.9 |
| Important (2) | 591 | 71.2 |
| Neutral (3) | 113 | 13.6 |
| Unimportant (4) | 10 | 1.2 |
| Very unimportant (5) | 1 | 0.1 |
| Total | 830 | 100.0 |
| Variable | Values | Importance of Distance N (%) | χ2 Value (p-Value) | |||
|---|---|---|---|---|---|---|
| Very Important | Important | Neutral or Not Important | ||||
| Elderly attribute | Gender | Male | 74 (15.2) | 342 (70.4) | 70 (14.4) | −0.445 (0.656) |
| Female | 41 (11.9) | 249 (72.4) | 54 (15.7) | |||
| Age | 60~70 | 47 (13.4) | 254 (72.2) | 51 (14.4) | 9.995 (0.119) | |
| 71~80 | 54 (16.9) | 226 (70.6) | 40 (12.5) | |||
| >80 | 14 (8.9) | 111 (70.2) | 33 (20.9) | |||
| Household registration type | Hefei urban household registration | 71 (16.0) | 334 (75.0) | 40 (9.0) | 17.240 (0.000) | |
| Hefei rural household registration | 30 (13.8) | 140 (64.2) | 48 (22.0) | |||
| Non-Hefei household registration | 14 (8.4) | 117 (70.1) | 36 (21.5) | |||
| Number of people living at home | 1 | 17 (19.1) | 58 (65.2) | 14 (15.7) | 0.360 (0.835) | |
| 2 | 61 (14.3) | 315 (73.6) | 52 (12.1) | |||
| ≥3 | 37 (11.8) | 218 (69.6) | 58 (18.6) | |||
| Number of generations living at home | One generation | 78 (15.2) | 369 (72.1) | 65 (12.7) | 2.726 (0.256) | |
| Two generations | 6 (6.9) | 71 (81.6) | 10 (11.5) | |||
| Three or more generations | 31 (13.4) | 151 (65.4) | 49 (21.2) | |||
| Level of education | Primary school or below | 49 (11.5) | 296 (69.3) | 82 (19.2) | 12.013 (0.007) | |
| Junior middle school | 43 (15.3) | 209 (74.4) | 29 (10.3) | |||
| Senior high school (including technical secondary school) | 18 (22.8) | 49 (62.0) | 12 (15.2) | |||
| College or above | 5 (11.6) | 37 (86.1) | 1 (2.3) | |||
| Original occupation | Public institutions staff | 37 (22.1) | 119 (70.8) | 12 (7.1) | 31.919 (0.000) | |
| Enterprise staff | 30 (11.7) | 200 (78.1) | 26 (10.2) | |||
| Self-employed or unemployed | 27 (20.0) | 93 (68.9) | 15 (11.1) | |||
| Farmer | 21 (7.7) | 179 (66.1) | 71 (26.2) | |||
| Number of children | None | 1 (11.1) | 6 (66.7) | 2 (22.2) | 7.139 (0.068) | |
| 1 | 24 (17.5) | 100 (73.0) | 13 (9.5) | |||
| 2 | 36 (10.7) | 258 (77.1) | 41 (12.2) | |||
| ≥3 | 54 (15.5) | 227 (65.0) | 68 (19.5) | |||
| Household per capita annual income | <CNY 10,000 | 17 (6.9) | 181 (73.6) | 48 (19.5) | 41.138 (0.000) | |
| CNY 10,000–20,000 | 51 (20.2) | 171 (67.9) | 30 (11.9) | |||
| >CNY 20,000 | 47 (14.1) | 239 (72.0) | 46 (13.9) | |||
| Type of medical insurance | Medical insurance for retired cadres | 13 (21.7) | 46 (76.7) | 1 (1.6) | 19.107 (0.000) | |
| Medical insurance for urban workers | 26 (9.4) | 218 (78.4) | 34 (12.2) | |||
| Medical insurance for urban residents | 31 (18.1) | 115 (67.3) | 25 (14.6) | |||
| New rural cooperative medical insurance | 39 (13.1) | 205 (69.0) | 53 (17.9) | |||
| Self-paying | 6 (25.0) | 7 (29.2) | 11 (45.8) | |||
| Travel activity status | Travel independently without the aid of auxiliary devices | 47 (14.0) | 234 (69.9) | 54 (16.1) | 2.868 (0.238) | |
| Travel independently with the aid of auxiliary devices | 26 (8.0) | 271 (83.1) | 29 (8.9) | |||
| Cannot travel independently | 42 (24.9) | 86 (50.9) | 41 (24.2) | |||
| Place of residence | Within the First Ring | 33 (12.8) | 197 (77.0) | 26 (10.2) | 2.904 (0.574) | |
| Between the First and the Second Ring | 42 (12.2) | 255 (74.3) | 46 (13.5) | |||
| Outside the Second Ring, within the urban area | 40 (17.3) | 139 (60.2) | 52 (22.5) | |||
| Number of private cars owned | None | 49 (14.9) | 209 (63.5) | 71 (21.6) | 3.014 (0.222) | |
| 1 | 38 (9.0) | 333 (79.3) | 49 (11.7) | |||
| ≥2 | 28 (34.6) | 49 (60.5) | 4 (4.9) | |||
| Factor | Actural Behavior N (%) | χ2 Value (p-Value) | |||
|---|---|---|---|---|---|
| Choosing the Nearest Hospital | Not Choosing the Nearest Hospital | ||||
| Distance preference | Importance of distance | Very important | 35 (30.4) | 80 (69.6) | 3.102 (0.212) |
| Important | 195 (33.0) | 396 (67.0) | |||
| Neutral or not important | 31 (25.0) | 93 (75.0) | |||
| Elderly attribute | Gender | Male | 157 (32.3) | 329 (67.7) | 0.401 (0.527) |
| Female | 104 (30.2) | 240 (69.8) | |||
| Age | 60~70 | 114 (32.4) | 238 (67.6) | 0.816 (0.665) | |
| 71~80 | 102 (31.9) | 218 (68.1) | |||
| >80 | 45 (28.5) | 113 (71.5) | |||
| Household registration type | Hefei urban household registration | 135 (30.3) | 310 (69.7) | 0.817 (0.665) | |
| Hefei rural household registration | 69 (31.7) | 149 (68.3) | |||
| Non-Hefei household registration | 57 (34.1) | 110 (65.9) | |||
| Number of people living at home | 1 | 32 (36.0) | 57 (64.0) | 1.132 (0.568) | |
| 2 | 135 (31.5) | 293 (68.5) | |||
| ≥3 | 94 (30.0) | 219 (70.0) | |||
| Number of generations living at home | One generation | 166 (32.4) | 346 (67.6) | 2.019 (0.568) | |
| Two generations | 29 (33.3) | 58 (60.7) | |||
| Three or more generations | 66 (28.6) | 165 (71.4) | |||
| Level of education | Primary school or below | 155 (36.3) | 272 (63.7) | 14.856 (0.002) | |
| Junior middle school | 83 (29.5) | 198 (70.5) | |||
| Senior high school (including technical secondary school) | 17 (21.5) | 62 (78.5) | |||
| College or above | 6 (14.0) | 37 (86.0) | |||
| Original occupation | Public institutions staff | 49 (29.2) | 119 (70.8) | 3.515 (0.319) | |
| Enterprise staff | 92 (35.9) | 164 (64.1) | |||
| Self-employed or unemployed | 39 (28.9) | 96 (71.1) | |||
| Farmer | 81 (29.9) | 190 (70.1) | |||
| Number of children | None | 2 (22.2) | 7 (77.8) | 2.688 (0.611) | |
| 1 | 42 (30.7) | 95 (69.3) | |||
| 2 | 104 (31.0) | 231 (69.0) | |||
| ≥3 | 113 (32.2) | 236 (67.8) | |||
| Household per capita annual income | <CNY 10,000 | 68 (27.6) | 178 (72.4) | 6.048 (0.196) | |
| CNY 10,000–20,000 | 91 (36.1) | 161 (63.9) | |||
| >CNY 20,000 | 102 (30.7) | 230 (69.3) | |||
| Type of medical insurance | Medical insurance for retired cadres | 15 (25.0) | 45 (75.0) | 2.554 (0.635) | |
| Medical insurance for urban workers | 85 (30.6) | 193 (69.4) | |||
| Medical insurance for urban residents | 52 (30.4) | 119 (69.6) | |||
| New rural cooperative medical insurance | 102 (34.3) | 195 (65.7) | |||
| Self-paying | 7 (29.2) | 17 (70.8) | |||
| Travel activity status | Travel independently without the aid of auxiliary devices | 89 (26.6) | 246 (73.4) | 6.964 (0.031) | |
| Travel independently with the aid of auxiliary devices | 109 (33.4) | 217 (66.6) | |||
| Cannot travel independently | 63 (37.3) | 106 (62.7) | |||
| Place of residence | Within the First Ring | 66 (25.8) | 190 (74.2) | 10.781 (0.005) | |
| Between the First and the Second Ring | 104 (30.3) | 239 (69.7) | |||
| Outside the Second Ring, within the urban area | 91 (39.4) | 140 (60.6) | |||
| Number of private cars owned | None | 95 (28.9) | 234 (71.1) | 2.854 (0.240) | |
| 1 | 135 (32.1) | 285 (67.9) | |||
| ≥2 | 31 (38.3) | 50 (61.7) | |||
| Total Time | Total Cost | Number of Transfers | Convenience of Station | Road Congestion | Barrier-Free Facilities on the Way | ||||
|---|---|---|---|---|---|---|---|---|---|
| Public transportation | Whether or not to choose the nearest hospital | χ2 value | 22.455 | 5.241 | 39.816 | 37.082 | 16.009 | 1.505 | |
| p-value | 0.664 | 0.073 | 0.000 | 0.000 | 0.042 | 0.471 | |||
| Private motor vehicle | Total time | Total cost | Road congestion | Convenience of parking | Barrier-free facilities on the way | ||||
| Whether or not to choose the nearest hospital | χ2 value | 20.180 | 2.330 | 12.294 | 0.819 | 2.330 | |||
| p-value | 0.447 | 0.802 | 0.002 | 0.664 | 0.802 | ||||
| Non-motorized vehicle | Total time | Total cost | Road congestion | Convenience of parking | |||||
| Whether or not to choose the nearest hospital | χ2 value | 11.538 | 5.764 | 6.951 | 3.030 | ||||
| p-value | 0.241 | 0.674 | 0.031 | 0.220 | |||||
| Mixed-mode of transportation | Total time | Total cost | Number of transfers | Convenience of station | Road congestion | Convenience of parking | Barrier-free facilities on the way | ||
| Whether or not to choose the nearest hospital | χ2 value | 9.787 | 17.969 | 12.621 | 20.443 | 8.149 | 3.587 | 5.116 | |
| p-value | 0.550 | 0.082 | 0.002 | 0.009 | 0.017 | 0.166 | 0.077 | ||
| Walking | Total time | Total cost | Road congestion | Barrier-free facilities on the way | |||||
| Whether or not to choose the nearest hospital | χ2 value | 13.266 | 11.058 | 8.873 | 3.765 | ||||
| p-value | 0.151 | 0.136 | 0.012 | 0.152 |
| Mode of Transportation | Variable | Regression Coefficient | OR Value | p-Value |
|---|---|---|---|---|
| Public transportation | Number of transfers | 0.887 | 2.428 | 0.000 |
| Convenience of station | 0.001 | 1.001 | 0.016 | |
| Road congestion | 0.401 | 1.494 | 0.034 | |
| Private motor vehicle | Road congestion | 0.686 | 1.986 | 0.001 |
| Non-motorized vehicle | Road congestion | 1.022 | 2.777 | 0.025 |
| Mixed-mode of transportation | Number of transfers | 1.411 | 4.102 | 0.006 |
| Convenience of station | 0.004 | 1.004 | 0.003 | |
| Road congestion | 1.173 | 3.231 | 0.012 | |
| Walking | Road congestion | 0.795 | 2.215 | 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Z.; Gao, Y.; Yu, L.; Choguill, C.L.; Cui, W. Analysis of the Elderly’s Preferences for Choosing Medical Service Facilities from the Perspective of Accessibility: A Case Study of Tertiary General Hospitals in Hefei, China. Int. J. Environ. Res. Public Health 2022, 19, 9432. https://doi.org/10.3390/ijerph19159432
Li Z, Gao Y, Yu L, Choguill CL, Cui W. Analysis of the Elderly’s Preferences for Choosing Medical Service Facilities from the Perspective of Accessibility: A Case Study of Tertiary General Hospitals in Hefei, China. International Journal of Environmental Research and Public Health. 2022; 19(15):9432. https://doi.org/10.3390/ijerph19159432
Chicago/Turabian StyleLi, Zao, Yanyan Gao, Li Yu, Charles L. Choguill, and Weiyi Cui. 2022. "Analysis of the Elderly’s Preferences for Choosing Medical Service Facilities from the Perspective of Accessibility: A Case Study of Tertiary General Hospitals in Hefei, China" International Journal of Environmental Research and Public Health 19, no. 15: 9432. https://doi.org/10.3390/ijerph19159432
APA StyleLi, Z., Gao, Y., Yu, L., Choguill, C. L., & Cui, W. (2022). Analysis of the Elderly’s Preferences for Choosing Medical Service Facilities from the Perspective of Accessibility: A Case Study of Tertiary General Hospitals in Hefei, China. International Journal of Environmental Research and Public Health, 19(15), 9432. https://doi.org/10.3390/ijerph19159432