
Effects of Personal Low-Frequency Stimulation Device on Myalgia: A Randomized Controlled Trial

 ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
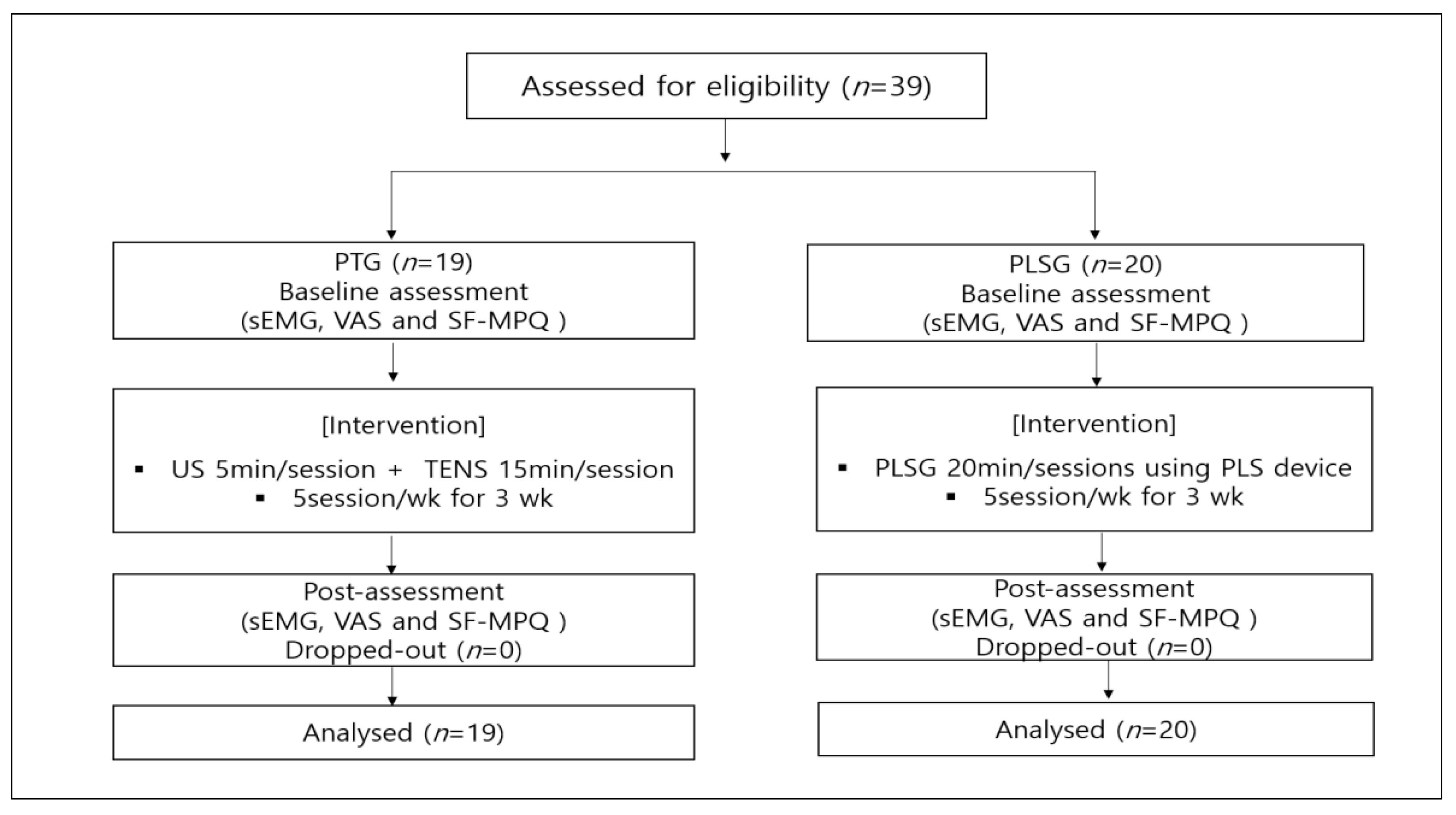
2.1. Participants
2.2. Experimental Design
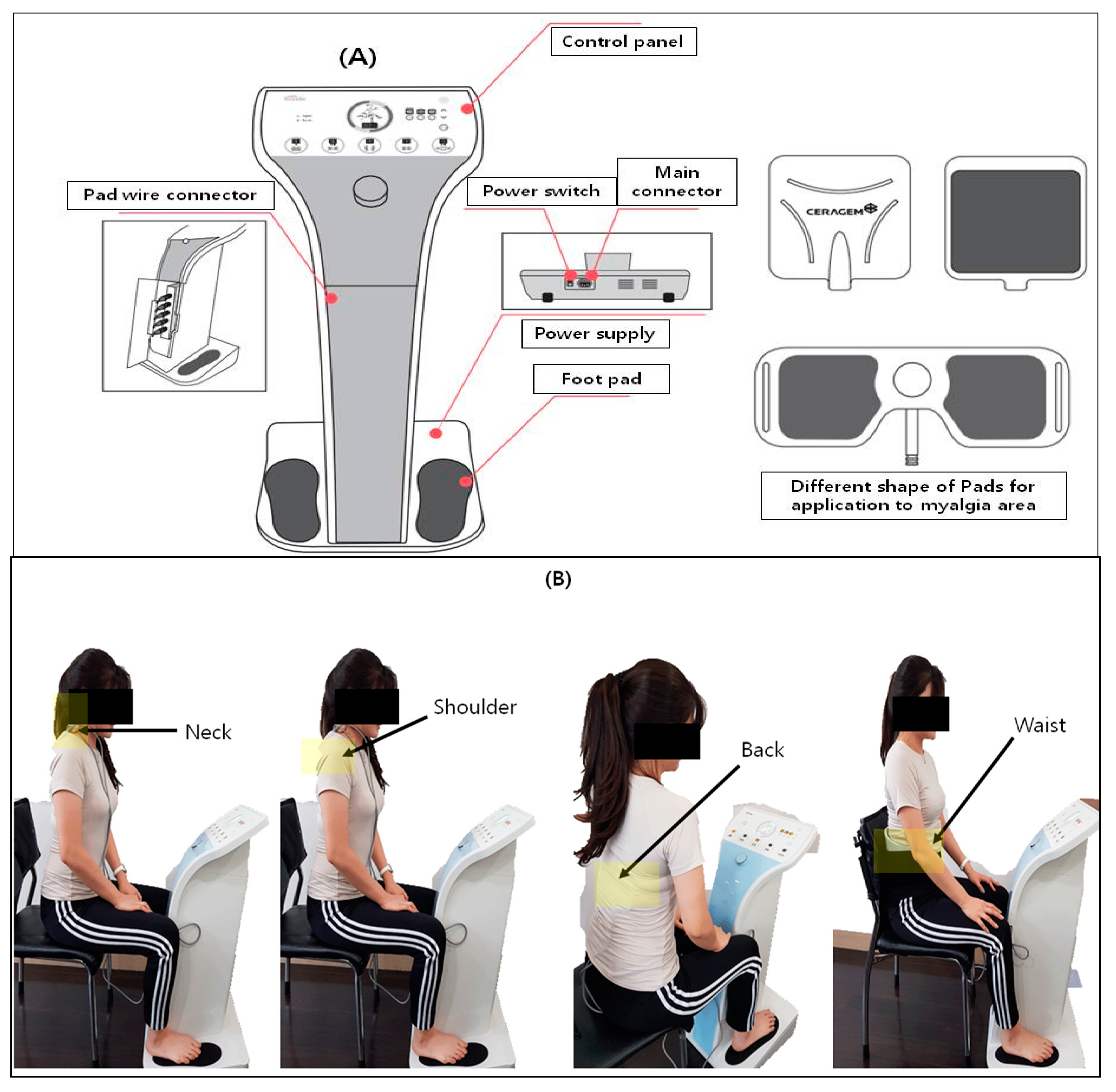
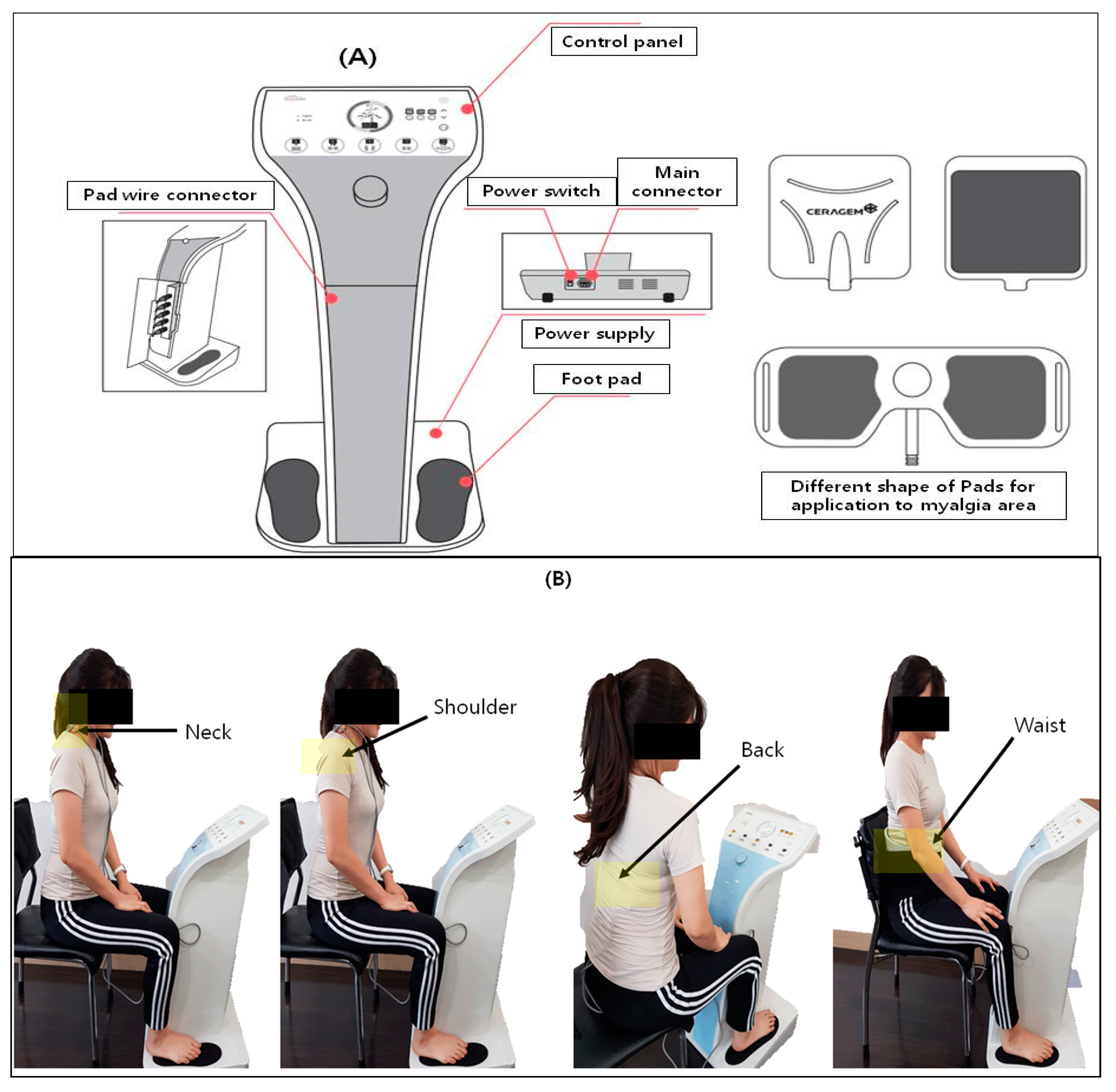
2.3. Experimental Device (PLS Device)
2.4. Sample Size
2.5. Outcomes Measures
2.5.1. Surface Electromyography
2.5.2. Subjective Pain
2.6. Data Analysis
3. Results
3.1. General Characteristics of Participants
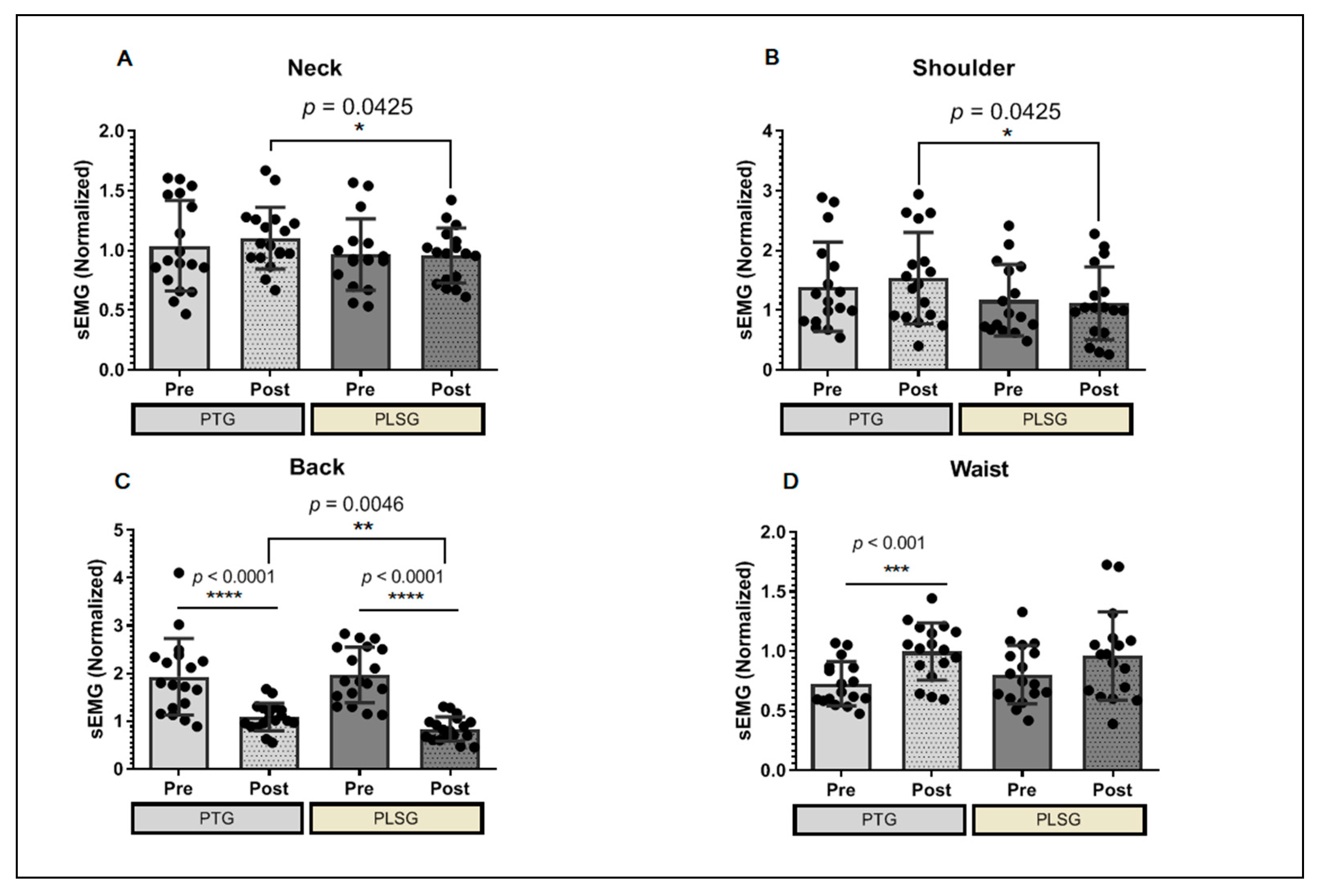
3.2. Changes in sEMG after PTG and PSLG
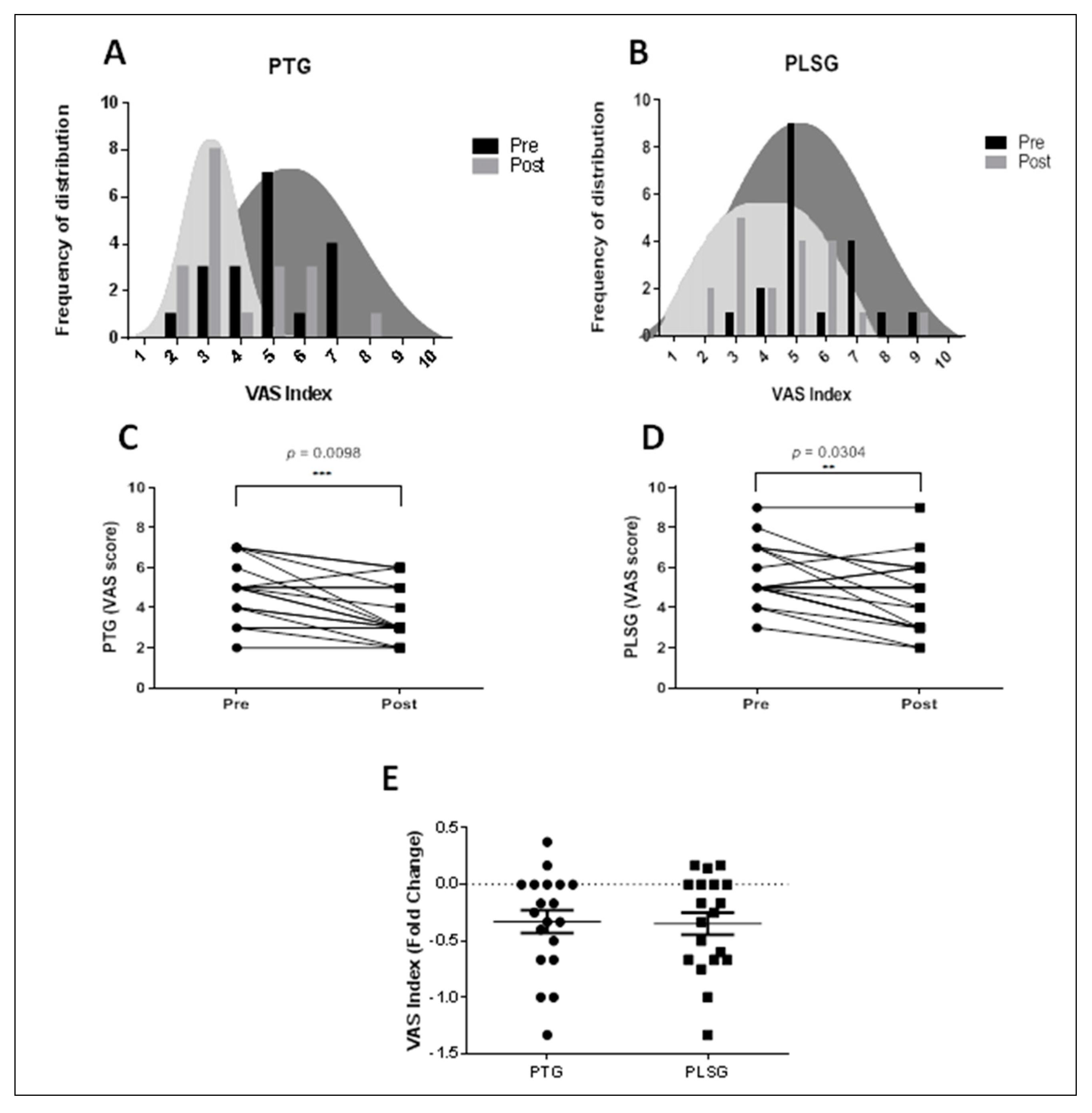
3.3. Changes in VAS Score after Treatment of PT and PLS
3.4. Changes in Subjective Pain Level (SF-MPQ Scores) after Treatment of PT and PLS
3.5. Safety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Punnett, L.; Wegman, D.H. Work-related musculoskeletal disorders: The epidemiologic evidence and the debate. J. Electromyogr. Kinesiol. 2004, 14, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Forde, M.S.; Punnett, L.; Wegman, D.H. Pathomechanisms of work-related musculoskeletal disorders: Conceptual issues. Ergonomics 2002, 45, 619–630. [Google Scholar] [CrossRef] [PubMed]
- Sundelin, G. Effects on physical performance and pain from three dynamic training programs for women with work-related trapezius myalgia. J. Rehabil. Med. 2001, 33, 162–169. [Google Scholar]
- De Meulemeester, K.E.; Castelein, B.; Coppieters, I.; Barbe, T.; Cools, A.; Cagnie, B. Comparing trigger point dry needling and manual pressure technique for the management of myofascial neck/shoulder pain: A randomized clinical trial. J. Manip. Physiol. Ther. 2017, 40, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Benlidayi, I.C. The effectiveness and safety of electrotherapy in the management of fibromyalgia. Rheumatol. Int. 2020, 40, 1571–1580. [Google Scholar] [CrossRef] [PubMed]
- Mutlu, B.; Paker, N.; Bugdayci, D.; Tekdos, D.; Kesiktas, N. Efficacy of supervised exercise combined with transcutaneous electrical nerve stimulation in women with fibromyalgia: A prospective controlled study. Rheumatol. Int. 2013, 33, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Castillo-Saavedra, L.; Gebodh, N.; Bikson, M.; Diaz-Cruz, C.; Brandao, R.; Coutinho, L.; Fregni, F. Clinically effective treatment of fibromyalgia pain with high-definition transcranial direct current stimulation: Phase II open-label dose optimization. J. Pain 2016, 17, 14–26. [Google Scholar] [CrossRef] [Green Version]
- Dailey, D.L.; Rakel, B.A.; Vance, C.G.; Liebano, R.E.; Amrit, A.S.; Bush, H.M.; Sluka, K.A. Transcutaneous electrical nerve stimulation reduces pain, fatigue and hyperalgesia while restoring central inhibition in primary fibromyalgia. Pain 2013, 154, 2554–2562. [Google Scholar] [CrossRef] [Green Version]
- Melzack, R.; Wall, P.D. Pain mechanisms: A new theory. Science 1965, 150, 971–979. [Google Scholar] [CrossRef]
- Lisi, T.L.; Sluka, K.A. A new electrochemical HPLC method for analysis of enkephalins and endomorphins. J. Neurosci. Methods 2006, 150, 74–79. [Google Scholar] [CrossRef]
- Leonard, G.; Goffaux, P.; Marchand, S. Deciphering the role of endogenous opioids in high-frequency TENS using low and high doses of naloxone. Pain 2010, 151, 215–219. [Google Scholar] [CrossRef] [Green Version]
- Leemans, L.; Elma, Ö.; Nijs, J.; Wideman, T.H.; Siffain, C.; den Bandt, H.; Beckwée, D. Transcutaneous electrical nerve stimulation and heat to reduce pain in a chronic low back pain population: A randomized controlled clinical trial. Braz. J. Phys. Ther. 2021, 25, 86–96. [Google Scholar] [CrossRef]
- Király, M.; Gömöri, E.; Kiss, R.; Nógrádi, N.; Nusser, N.; Hodosi, K.; Bender, T. Effects of various types of ultrasound therapy in hip osteoarthritis-a double-blind, randomized, controlled, follow-up study. Physiother. Theory Pract. 2021, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Vance, C.G.T.; Rakel, B.A.; Blodgett, N.P.; DeSantana, J.M.; Amendola, A.; Zimmerman, M.B.; Sluka, K.A. Effects of transcutaneous electrical nerve stimulation on pain, pain sensitivity, and function in people with knee osteoarthritis: A randomized controlled trial. Phys. Ther. 2012, 92, 898–910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, L.; Tan, K.; Lin, X.; Yi, H.; Wang, X.; Zhang, J.; Lin, L. Multicenter, randomized, double-blind, controlled trial of transcutaneous electrical nerve stimulation for pancreatic cancer related pain. Medicine 2021, 100, e23748. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.H. The changes of range of motion of lumbar region and muscle activities of lumbar extensor during trunk motions between subjects with low back pain and healthy subjects. Phys. Ther. Korea 2006, 13, 61–69. [Google Scholar]
- Scott, J.; Huskisson, E.C. Vertical or horizontal visual analogue scales. Ann. Rheum. Dis. 1979, 38, 560. [Google Scholar] [CrossRef] [PubMed]
- Melzack, R. The short-form McGill pain questionnaire. Pain 1987, 30, 191–197. [Google Scholar] [CrossRef]
- Hu, H.; Yang, W.; Zeng, Q.; Chen, W.; Zhu, Y.; Liu, W.; Zhang, Y. Promising application of Pulsed Electromagnetic Fields (PEMFs) in musculoskeletal disorders. Biomed. Pharmacother. 2020, 131, 110767. [Google Scholar] [CrossRef]
- Wang, T.; Xie, W.; Ye, W.; He, C. Effects of electromagnetic fields on osteoarthritis. Biomed. Pharmacother. 2019, 118, 109282. [Google Scholar] [CrossRef]
- Assiotis, A.; Sachinis, N.P.; Chalidis, B.E. Pulsed electromagnetic fields for the treatment of tibial delayed unions and nonunions. A prospective clinical study and review of the literature. J. Orthop. Surg. Res. 2012, 7, 24. [Google Scholar]
- Sayilir, S. The short-term effects of TENS plus therapeutic ultrasound combinations in chronic neck pain. Complement. Ther. Clin. Pract. 2018, 31, 278–281. [Google Scholar] [CrossRef]
- Yilmaz, M.; Tarakci, D.; Tarakci, E. Comparison of high-intensity laser therapy and combination of ultrasound treatment and transcutaneous nerve stimulation on cervical pain associated with cervical disc herniation: A randomized trial. Complement. Ther. Med. 2020, 49, 102295. [Google Scholar] [CrossRef]
- Neblett, R. Surface electromyographic (SEMG) biofeedback for chronic low back pain. Healthcare 2016, 4, 27. [Google Scholar] [CrossRef] [Green Version]
- Fejer, R.; Hartvigsen, J. Neck pain and disability due to neck pain: What is the relation? Eur. Spine J. 2008, 17, 80–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoyt, W.H.; Hunt, H.H., Jr.; De Pauw, M.A.; Bard, D.; Shaffer, F.; Passias, J.N.; Watt, K.C. Electromyographic assessment of chronic low-back pain syndrome. J. Am. Osteopath. Assoc. 1981, 80, 728–730. [Google Scholar]
- Ambroz, C.; Scott, A.; Ambroz, A.; Talbott, E.O. Chronic low back pain assessment using surface electromyography. J. Occup. Environ. Med. 2000, 42, 660–669. [Google Scholar] [CrossRef] [PubMed]
- Nederhand, M.J.; IJzerman, M.J.; Hermens, H.J.; Baten, C.T.; Zilvold, G. Cervical muscle dysfunction in the chronic whiplash associated disorder grade II (WAD-II). Spine (Phila Pa 1976) 2000, 25, 1938–1943. [Google Scholar] [CrossRef]
- Gewandter, J.S.; Chaudari, J.; Ibegbu, C.; Kitt, R.; Serventi, J.; Burke, J.; Mohile, N.A. Wireless transcutaneous electrical nerve stimulation device for chemotherapy-induced peripheral neuropathy: An open-label feasibility study. Supportive Care Cancer 2019, 27, 1765–1774. [Google Scholar] [CrossRef]
- Carbonario, F.; Matsutani, L.A.; Yuan, S.L.; Marques, A.P. Effectiveness of high-frequency transcutaneous electrical nerve stimulation at tender points as adjuvant therapy for patients with fibromyalgia. Eur. J. Phys. Rehabil. Med. 2013, 49, 197–204. [Google Scholar] [PubMed]
- Yakşi, E.; Ketenci, A.; Baslo, M.B.; Orhan, E.K. Does transcutaneous electrical nerve stimulation affect pain, neuropathic pain, and sympathetic skin responses in the treatment of chronic low back pain? A randomized, placebo-controlled study. Korean J. Pain. 2021, 34, 217–228. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | PTG (n = 19) | PLSG (n = 20) |
|---|---|---|
| Age (years) | 53.00 ± 14.82 | 58.95 ± 5.39 |
| BMI (kg/m2) | 23.18 ± 2.79 | 25.26 ± 4.61 |
| VAS (score) | 4.84 ± 1.50 | 5.50 ± 1.57 |
| Duration of pain (months) | 68.05 ± 68.01 | 102.10 ± 151.10 |
| Group | Pre-Test M ± SD | Post-Test M ± SD | Adjusted Post-Test M ± SE | F-Value | ƞ2 | |
|---|---|---|---|---|---|---|
| SF-MPQ | PTG (n = 19) | 6.26 ± 2.31 | 5.11 ± 2.26 | 6.23 ± 0.25 | 6.558 * | 0.154 |
| PLSG (n = 20) | 8.55 ± 3.56 | 6.35 ± 3.67 | 5.23 ± 0.25 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, Y.-S.; Ko, M.-H.; Cho, I.-Y.; Kim, C.-S.; Bajgai, J.; Jang, H.-Y.; Kim, K.-E.; Lee, K.-J.; Lee, M. Effects of Personal Low-Frequency Stimulation Device on Myalgia: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 735. https://doi.org/10.3390/ijerph19020735
Yoon Y-S, Ko M-H, Cho I-Y, Kim C-S, Bajgai J, Jang H-Y, Kim K-E, Lee K-J, Lee M. Effects of Personal Low-Frequency Stimulation Device on Myalgia: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(2):735. https://doi.org/10.3390/ijerph19020735
Chicago/Turabian StyleYoon, Yong-Soon, Myoung-Hwan Ko, Il-Young Cho, Cheol-Su Kim, Johny Bajgai, Hong-Young Jang, Ka-Eun Kim, Kyu-Jae Lee, and Mihyun Lee. 2022. "Effects of Personal Low-Frequency Stimulation Device on Myalgia: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 2: 735. https://doi.org/10.3390/ijerph19020735