Abstract
We assessed the effectiveness of a walking exercise-focused health promotion program based on an information–motivation–behavioral skills model. This intervention study employed a non-equivalent control group pre-test/post-test design. We recruited 44 middle-aged women (22 per group) who visited two health check-up centers in G city of South Korea. The intervention included information (health education), personal motivation (pedometer monitoring, setting goals, and keeping an exercise log), social motivation (group discussion and support, telephone counseling), and behavioral skills (walking exercise) components. Ten sessions of this program involved three face-to-face and seven online interactions via mobile instant messaging. As primary outcomes (health behavior), physical activity level and health-promoting lifestyle were measured by standardized scales. As secondary outcomes (health status), physiological indicators by body measurements and perceived stress by a scale were produced. We used the chi-squared test, independent t-test, and Mann–Whitney U test for the analysis. After the intervention, in the experimental group, the level of physical activity (Z = −2.065, p = 0.039) and health-promoting lifestyle improved (t = 3.344, p = 0.002), and both waist circumference (t = −4.328, p < 0.001) and perceived stress (t =−3.578, p < 0.001) decreased. In conclusion, our theory-based intervention has advantages in terms of high standardization potential, high availability, and improvement of health behavior and health status. In future, this approach will be useful for devising interventions that meet the health needs of people who are concerned about quality of life in the second half of life.
1. Introduction
In the midst of the health care challenges of an extending lifespan and an aging population, there is growing interest in staying healthy throughout life [1]. According to data from Statistics Korea in 2020, life expectancy was 83.5 years, which is about 21 years higher than in 1970 (62.3 years) [2]. In particular, the life expectancy of women is now 86.5 years, which is 6 years longer than that of men (80.5 years) [2]. These data suggest the importance of preparing for later life.
Midlife, the period in which one transitions from the first to the second half of the life course, is pivotal for health management [3]. Middle-aged adults may place their physical and mental health at risk by making various changes based on re-evaluation of the past; this is often characterized as a “midlife crisis” [3,4], which is associated with unhealthy behavior and reduced life satisfaction [5]. Middle age, along with age-related physical decline, leads to changes in heart health and cardiovascular risk profile [6]. It is also associated with the onset of functional limitations, and the transition to disability may occur with the risk of osteoporosis and concomitant fractures [6]. In particular, middle-aged women experience various physical and psychological symptoms as they go through menopause, which negatively affect quality of life [7,8]. However, middle age also offers new opportunities and challenges [9]. It is possible to balance gains and losses, and meaningfully connect one’s previous and current life circumstances [9]. Middle-aged women may require assistance to improve their health so that the second half of the life course is of a high quality.
Health management during middle age determines the quality of the rest of one’s life, and effective health-promoting measures are important during this period [10]. In a cohort study analyzing the 10-year outcomes of health promotion programs (n = 10,248; mean age 41.2 ± 10.8 years; female 68.1%), the behaviors most important for good health were a low-fat diet, aerobic exercise, smoking cessation, and sufficient sleep [11]. Previous studies have reported that interventions targeting health promotion have positive effects on the health behaviors, health risk factors, and physical/mental health status of middle-aged women. In an intervention study for postmenopausal women, health education with a focus on health-promoting lifestyle modifications was effective in enhancing their adherence to health-promoting behaviors and improving menopause symptoms, anthropometric adiposity indices, cardiovascular disease risk indicators, hand grip strength, and gait speed [12]. Health education, focused on a health-promoting lifestyle, has also been effective in improving the overall quality of life of postmenopausal women [13]. A study on middle-aged Korean women showed that a health-promoting lifestyle had a direct mediating effect on the relationship between menopausal symptoms and depression [14]. These findings show the benefits of a health promotion approach to improving the health behavior and health status of middle-aged women.
Walking exercise has been suggested as an effective and safe health promotion activity with high adherence and wide-ranging health benefits [15]. In a randomized controlled trial of an urban forest-walking program for office workers, physical activity level, health-promoting behavior, and quality of life all improved [16]. In a study including a large group of middle-aged South Korean women, regular walking was associated with reductions in perceived stress and depression, and a greater capacity for activity [17]. Regular walking exerted positive effects on body weight, fat mass, blood biochemical markers, and physical activity parameters in middle-aged women [18,19]. Therefore, health promotion interventions that include walking may improve the health behavior and health status of middle-aged women.
Physical inactivity is one of the major modifiable risk factors for mortality and is a key target of interventions aimed at promoting health [20]. Compared to their physically less active counterparts, physically active individuals across all ethnicities and ages exhibit higher levels of cardiorespiratory fitness, health, and well-being, and have lower risks of various chronic medical conditions [20]. A cross-sectional epidemiologic study of a UK population found that physically active people had better mental health in terms of symptoms of depression/anxiety and mental well-being [21]. In a meta-analysis, postmenopausal women had higher cardiovascular disease risk factors, morbidity, and mortality than women of reproductive age, and physical activity lowered the risk [22]. Therefore, we selected the level of physical activity as a target outcome based on health promotion interventions.
We adopted the information–motivation–behavioral skills (IMB) model as a theoretical basis for designing effective health promotion interventions [23]. This psychological model considers information, motivation, and behavioral skills as fundamental determinants of health behavior [23]. The IMB model has been useful in devising health education or training programs to improve health behaviors [24,25,26,27,28]. In addition, a meta-analysis study of electronic health interventions to promote physical activity in older people suggested this as an effective and safe intervention strategy [29]. In particular, instant messaging and social networks, which allow users to exchange instant messages online or via mobile devices, are gaining traction in the field of health research [30]. Additionally, to apply electronic health interventions effectively to older adults, consideration should be given to reducing the barriers they face, and utilizing facilitators [31]. Therefore, we additionally adopted the online method using mobile instant messengers (MIM), and used the offline method in parallel to reflect the barriers and facilitation factors.
This study aimed to provide a health promotion program centered on walking exercise based on an information–motivation–behavioral skills model for middle-aged women, and to confirm its effect on health behavior and health status. The hypotheses of this study were as follows:
The experimental group will have an increased level of physical activity.
The experimental group will have an improved health-promoting lifestyle.
The experimental group will have improved physiological indicators, such as body mass index, waist circumference, and blood pressure.
The experimental group will have lower perceived stress.
2. Conceptual Framework
Our health promotion intervention was based on the IMB model of Fisher et al. (2006) [23]. We designed intervention strategies that correspond to the main components of the IMB model, to reinforce healthy behaviors as follows: information (health education), personal motivation (pedometer monitoring, setting goals, and keeping an exercise log), social motivation (group discussion and support, telephone counseling), and behavioral skills (walking exercise) (Figure 1). We created educational materials delivered weekly through group training or instant messaging throughout the program. Health motivation was divided into personal and social domains according to the IMB model [23]. To reinforce personal motivation, we gave each participant a pedometer and asked them to keep an exercise log. In terms of social motivation, we provided emotional support and helped set goals via telephone counselling and group training. Behavioral skills for adhering to healthy behaviors are assumed to determine whether even well-informed and motivated individuals can maintain healthy behaviors [23]. In this study, regular walking exercise was selected as a behavioral skill for health behavior. Primary and secondary outcome variables were established to identify the effects of interventions, including health information, health motivation, and behavioral skill components. Primarily, this walking exercise-centered health promotion program was expected to improve the health behavior, identified by physical activity level and health-promoting lifestyle. Secondarily, it was hypothesized that the experimental group after the intervention would show improvements in physiological indicators and perceived stress.
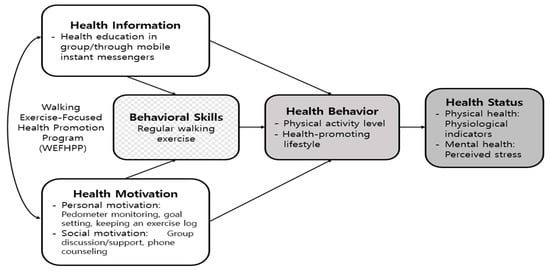
Figure 1.
Conceptual framework of this study.
3. Materials and Methods
3.1. Study Design
This intervention study used a non-equivalent control group pre-/post-test design to explore the effects of a health promotion program for middle-aged women.
3.2. Ethical Considerations
The study began only after approval had been obtained from the Institutional Review Board (approval no. 2-1041055-AB-N-01-2017-0034). The purpose, procedure, duration, research methods, anticipated results, and applications of the study were fully explained to all participants in advance, and they were informed that they were free to leave the study at any time. The written informed consent forms and completed questionnaires were kept in a safe that was accessible only to the researchers. At the end of the program, we rewarded the experimental group for participation (pedometer and small gift certificate), and provided the control group with a pedometer and health education.
3.3. Study Sample
The target population were Korean women aged 40–59 years in the community (8,285,456 people as of 2021) [32]. The inclusion criteria were as follows: middle-aged women who agreed to participate in the study; those able to participate in the program for 10 weeks, and who had no physical impairments, were able to read/write/communicate, had no previous experience in walking exercise programs, and had not participated in any other physical activity programs at the time of the program. The exclusion criteria were as follows: unstable blood pressure control; did not engage in walking for more than 2 weeks in the experimental group or participated in other physical activity programs in the control group.
Participants were recruited via posters when they visited one of two health check-up centers in G city. The optimal sample size for t-test analysis was calculated using G*Power software (ver. 3.1.2) [33]. The effect size was based on a prior study of the effects of health-promoting programs (education and exercise) on middle-aged women [34]. For a one-sided significance level of 0.05, power (1−β) of 0.80, and effect size of 0.80, the experimental and control groups each required 21 subjects. Assuming a dropout rate of about 18% (as in a previous walking program) [35], we recruited 25 experimental and 26 control subjects. We assigned an experimental group and a control group via a randomization method. After notifying the participants in advance that they would be randomized to either the experimental group or the control group, a coin toss was performed to determine the group assignment for each participant. The coin tossing was stopped when the target number of people in either group was met. The remaining applicants were placed in an unpopulated group. Four participants dropped out because of personal reasons (hospitalization or employment-related) and three were found to have provided inappropriate questionnaire responses so were excluded after study completion. Finally, data from 22 participants in each group were analyzed.
3.4. Data Collection
Data were collected from September to November 2017. The visit times of the participants were adjusted to prevent contact between the experimental and control groups. The intervention period was early autumn (at which time outdoor activities are not affected by excessively cold or hot conditions). A pre-test and post-test were conducted to confirm the change in the effect index before and after the intervention. The data collection methods used were structured questionnaires and body measurements for the experimental and control groups. For personal motivation, we provided participants with a pedometer, which they wore around their waist. Each pedometer was equipped with a function to check the number of steps and to estimate calories burned by entering the user’s height, weight, and average stride length.
3.5. Research Progress
3.5.1. Pretesting
Pretesting involved a self-reported structured questionnaire on general characteristics, physical activity, health-promoting behaviors, and perceived stress. Participants were asked to overnight fast after the previous evening’s dinner and visit the center in the morning for body composition measurements. Height, weight, waist circumference, and blood pressure were measured by a trained research assistant who was a nurse with more than 3 years of experience at the check-up centers. In this case, an automatic height/weight scale (BSM330, Biospace, Seoul, Korea), a soft string ruler, and an automatic blood pressure monitor for adults (JPN600, Omron, Japan) were used. The experimental group was asked to wear a pedometer from the time they woke up in the morning to just before going to bed, record the number of steps per week and calories burned per week, and report it via instant messaging.
3.5.2. Treatment: Walking Exercise-Focused Health Promotion Program (WEFHPP)
The WEFHPP was devised by modifying the walking exercise program developed for office workers by Choi (2012) for middle-aged women [36], based on the IMB model. The structure and content of each session of this program are shown in Table 1. A total of 10 sessions of the WEFHPP consisted of 3 face-to-face sessions (Sessions 1, 6, and 10) and 7 online sessions (Sessions 2–5 and 7–9). The offline session was held in the health examination center room by the first author, and the online session was conducted through instant messages. One session was held each week for 10 weeks. Nine health education sessions (conducted face-to-face or via instant messaging) were also completed from Sessions 1 to 9. We sent instant messages weekly during the online session. The messages were about how to walk properly, personalized exercise method and intensity, stretching, nutrition, how to manage stress, and how to increase daily activity level. Additional materials in the form of documents and videos were attached depending on the subject. To maintain personal motivation, participants were asked to monitor the numbers of steps taken and calories burned using the pedometer, and to create daily exercise logs. The exercise log included records of exercise content (walking, jogging, aerobics, etc.), exercise steps, exercise time, and total number of steps. Participants were also asked to set a weekly walking goal and self-evaluate it. For social motivation, three group discussions, two individual telephone counseling sessions, and continuous group support were provided. The content validity of the program was 0.95, as determined by six experts comprising two internal medicine specialists, one family medicine specialist, and three nursing professors.

Table 1.
Contents of each session of the health promotion program.
3.5.3. Post-Testing
Post-testing was performed during week 10 (final intervention session). The pretest questionnaires and physical measurements were repeated.
3.6. Instruments
3.6.1. Physical Activity Level
We used the Korean version of the International Physical Activity Questionnaire Short Form (IPAQ-SF) [37]. In a study on Korean adults, the Spearman Rho coefficients and kappa values for test–retest reliability for seven components (days and minutes of vigorous, moderate, and walking exercise, and minutes spent sitting) were 0.43~0.65 and 0.37~0.62, respectively [38]. The Spearman Rho coefficient for all items in this study was 0.77. The total physical activity level was obtained by summing the walking, moderate, and vigorous activity times over the past 7 days. Questionnaire data were converted into metabolic equivalent task minutes per week (MET∙min/wk) using the average MET score for each type of activity. The weighted physical activity score was calculated as follows: duration × frequency per week × MET intensity (walking = 3.3 METs, moderate physical activity = 4.0 METs, vigorous physical activity = 8.0 METs).
3.6.2. Health-Promoting Lifestyle
We used the Korean translation of the Health-Promoting Lifestyle Profile–II (HPLP-II) questionnaire introduced by Walker et al. [39,40,41]. The HPLP-II has 52 items and six categories: nutrition, physical activity, health responsibility, stress management, interpersonal relations, and spiritual growth. Items are scored on a four-point scale (1 = never, 2 = sometimes, 3 = often, 4 = routinely), and total scores range from 52 to 208. A higher score indicates a healthier lifestyle. The reliability (Cronbach’s α) value was 0.93 in the study of Hwang [39] and 0.92 in the present study.
3.6.3. Physiological Indicators
Body mass index (BMI, weight in kilograms divided by height in meters squared), waist circumference, and blood pressure were measured, as in previous walking programs [16,35]. Relevant pre- and post-testing values were measured and compared by trained nurses who were blinded to group assignments. All body measurements were performed using the same instruments, at the same time of day and location. Blood pressure was measured twice on the upper arm at the height of the heart, 10 min apart, after each participant had rested in a chair for at least 10 min. The average value was used in the analysis.
3.6.4. Perceived Stress
We used the validated 10-item Korean version of the Perceived Stress Scale (PSS) [42,43]. Items were scored on a five-point scale (0 = never, 1 = almost never, 2 = sometimes, 3 = fairly often, 4 = very often), and total scores ranged from 0 to 40. A higher score indicates a higher level of perceived stress. In Korea, the Cronbach’s α values (internal consistency) were 0.77 and 0.74 for negative and positive items, respectively [43]. In this study, the Cronbach’s α for all questions was 0.73.
3.7. Data Analyses
The data were statistically analyzed using SPSS for Windows software (ver. 22.0) and are presented as frequencies, percentages, and means with standard deviations. The Kolmogorov–Smirnov test was initially used to determine whether variables were normally distributed; a non-parametric test was performed if this was not the case. The independent t-test and the Mann–Whitney U test were employed to compare homogeneities between the experimental and control groups. The internal consistency (reliability) of the measurement tools was evaluated by calculating Cronbach’s α values and Spearman–Brown coefficients.
4. Results
4.1. Homogeneity Test
According to the pre-test data, the two groups did not differ significantly in terms of general characteristics or physical measurements, i.e., they were homogeneous (Table 2). Physical activity level, health-promoting behaviors (exercise and nutrition), and diastolic blood pressure were not normally distributed, so those data were analyzed using the Mann–Whitney U test.
Table 2.
Between-group comparisons of general characteristics and outcome variables at baseline (N = 44).
4.2. Hypothesis Testing: Differences between Groups
Compared with the control group, the experimental group exhibited a significantly increased physical activity level (p = 0.035), improved health-promoting lifestyle (p = 0.002), decreased waist circumference (p < 0.001), and reduced perceived stress (p < 0.001) (Table 3). Among the subcategories of health-promoting lifestyles, there were between-group differences in physical activity (p < 0.001), nutrition (p = 0.006), and stress management (p = 0.012).
Table 3.
Between-group differences of outcome variables after intervention (N = 44).
5. Discussion
Our health promotion intervention (WEFHPP) was designed to enhance the healthy lives of middle-aged women. This program had a significant effect on improving physical activity levels, a health-promoting lifestyle, waist circumference, and perceived stress. Previous health intervention studies using the IMB model [24,25,26,27,28] also reported positive effects in improving health behavior and health status. Therefore, the IMB model is highly recommended as a theoretical basis for health promotion programs.
The WEFHPP included 7 online sessions using MIM out of a total of 10 sessions, and was mainly used as a means of health education and group support. Instant messaging has been applied as a safe and effective means in the field of health care education and intervention [44,45,46,47]. A systematic review of mobile apps for cancer pain management found that instant messaging interventions were highly effective for controlling pain [48]. Our study demonstrates that e-health strategies via instant messaging are beneficial in terms of their safe adoption, even in a pandemic situation, and their effectiveness as a delivery mode of exercise programs or health promotion interventions for middle-aged women.
The WEFHPP was found to improve overall physical activity level (p = 0.035) and health-promoting lifestyle (p = 0.002) as a primary outcome variable. In particular, among the sub-concepts of health-promoting lifestyle, there were statistically significant improvements in physical activity, nutrition, and stress management. By contrast, no significant group difference was found in the sub-activity category, which is thought to be due to the large individual difference within a small sample, so that no meaningful change was detected. This needs to be reexamined in repeated studies using more samples in future. In a randomized controlled trial of a walking exercise program for Korean office workers in their 30s and 40s (mostly women), the level of physical activity, health-promoting behavior, and quality of life improved, constituting similar results to this study [16]. A systematic review of physical activity interventions for African American women found that a healthy diet, walking, and social support promoted physical activity [49], which also supports our findings. In the WEFHPP, online education and group interaction, which provided enough materials on a variety of lifestyle-related topics through MIM, seems to have been useful in facilitating a shift to healthy behaviors and lifestyles on the part of participants. The ongoing personal and social motivation strategies used in this study may also have contributed to adherence to health behaviors on the part of participants. Indeed, the acquisition of behavioral skills, use of mobile devices, and goal-setting and feedback are effective in increasing physical activity [50,51,52]. However, a randomized clinical trial of a lifestyle-focused physical activity program for middle-aged African American women found that group meetings greatly increased physical activity and prevented weight gain, but motivational telephone calls did not provide any additional benefit [52]. Further studies are needed to assess various interventional delivery strategies and to evaluate their effectiveness.
The WEFHPP reduced participants’ waist circumference (p < 0.001) but did not significantly change their BMI or blood pressure. In a meta-analysis of the effects of walking on cardiovascular risk factors in subjects of various sexes and ages (adults and older), walking improved body weight, BMI, waist circumference, and blood pressure [53]. Recent studies found that the effects of walking were greater under certain conditions. The blood pressure of participants with higher baseline systolic pressure decreased to a greater extent than that of the other participants after guided walking exercises had been performed for >6 months [54]. After completing a 24-week walking exercise program, the BMI, waist circumference, and systolic and diastolic blood pressure of obese middle-aged women decreased significantly [55]. Pedometer-based walking exercises for overweight adults involving >10,000 steps/day improved body weight, waist circumference, and blood pressure [56,57]. As stated above, our relatively short-term program did not improve the BMI or blood pressure of the healthy middle-aged women. However, physiological indicators may have been maintained within the normal range, thereby preventing weight gain and hypertension. Our program significantly reduced waist circumference, so it has the potential to improve body image or prevent abdominal obesity. Therefore, regular walking exercise in daily life can influence physical health when incorporated with other lifestyle factors such as overall physical activity, nutrition and stress management.
Finally, our program suggests the potential for improved mental health by reducing perceived stress (p < 0.001). Stults-Kolehmainen and Sinha (2014) confirmed a correlation between psychological stress and lack of physical activity in a meta-analysis of 168 papers [58]. Physical activity relieved stress, and stress was negatively associated with physical exertion. Additionally, an intervention combining stress management and exercise was proposed based on those findings [58]. Our WEFHPP relieved stress and increased physical activity in a synergistic manner. A short-term, randomized crossover trial combining walking and relaxation interventions for healthy adults reduced blood pressure and stress [59]. As such, focusing on walking exercise and stress management in primary care settings will be effective in achieving health promotion outcomes.
The main strength of our study is that it is based on a theoretical framework that can induce effective behavioral changes using a variety of strategies and behavioral skills that can be easily applied in daily life. This has the advantages of being easy to apply in practice, as well as for developing other interventions for different subjects and purposes. However, we enrolled a small number of participants, all from the same region; studies with larger and more diverse populations are needed. Our study also has limitations in that we did not sufficiently control for various exogenous variables (diet, smoking, antihypertensive drugs) that may have influenced the outcome variables. This should be considered in future studies using multidimensional outcome variables. New challenges for middle-aged women research were presented based on the Seattle Middle-aged Women’s Health Study, which analyzed longitudinal data spanning up to 23 years [60]. The aim was to go beyond the menopause-focused perspective to an in-depth exploration of life events and coping styles, as a way to find balance [60]. To understand the health and life of middle-aged women more fully, qualitative research on these topics is required in various cultures in future. Furthermore, because health-promoting behaviors should be sustained over the long term, to lead to health outcomes, a cohort or longitudinal study is needed to confirm the long-term effects of interventions.
6. Conclusions
We explored the effects of a walking exercise-focused health promotion program based on the IMB model for middle-aged women living in the community. The level of physical activity and health-promoting behavior increased, while waist circumference and perceived stress decreased. Our theory-based intervention has advantages in terms of high standardization potential, high availability, and improvement of health behaviors and health status. In future, this approach will be useful for devising interventions that meet the health needs of people concerned about their quality of life in the second half of life.
Author Contributions
Conceptualization, S.Y. and H.K.; methodology, S.Y. and H.K.; formal analysis, S.Y.; investigation, S.Y.; data curation, S.Y.; writing—original draft preparation, S.Y. and H.K.; writing—review and editing, S.Y. and H.K.; project administration, S.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by the research fund of Chosun University, 2021.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of Chosun University (protocol code 2-1041055-AB-N-01-2017-0034; 25 July 2017).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Please contact the corresponding author for data availability.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Yang, S.; Park, S.; Kim, H. Effects of depression, expectations regarding aging on the health promoting lifestyle among health checkup examinee. J. Korea Contents Assoc. 2018, 18, 509–519. [Google Scholar]
- Statistics Korea. 2020 Life Tables for Korea; Statistics Korea: Seoul, Korea, 2021; Available online: https://kosis.kr/statisticsList/statisticsListIndex.do?menuId=M_01_01&vwcd=MT_ZTITLE&parmTabId=M_01_01&outLink=Y&entrType=#F_29.2 (accessed on 15 July 2022).
- Freund, A.M.; Ritter, J.O. Midlife crisis: A debate. Gerontology 2009, 55, 582–591. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.K. Influencing factors on mid-life crisis. Korean J. Adult Nurs. 2018, 30, 98–105. [Google Scholar] [CrossRef]
- Oh, E.T.; Oh, H.O. Relationship among mid-life crisis, health promotion behavior and life satisfaction. Korean J. Phys. Educ. 2011, 50, 325–336. [Google Scholar]
- Dias, J.M.; Subu, M.A.; Abraham, M.S.; Al Yateem, N. Women’s midlife health: Risk factors and disease burden for global health. In Handbook of Global Health; Kickbusch, I., Ganten, D., Moeti, M., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 1013–1042. [Google Scholar]
- Bang, S.Y.; Do, Y.S. Health-related quality of life of physical and mental health in middle-aged women. JKAIS 2020, 21, 161–169. [Google Scholar]
- Rathnayake, N.; Lenora, J.; Alwis, G.; Lekamwasam, S. Prevalence and severity of menopausal symptoms and the quality of life in middle-aged women: A study from Sri Lanka. Nurs. Res. Pract. 2019, 2019, 2081507. [Google Scholar] [CrossRef] [PubMed]
- Infurna, F.J.; Gerstorf, D.; Lachman, M.E. Midlife in the 2020s: Opportunities and challenges. Am. Psychol. 2020, 75, 470–485. [Google Scholar] [CrossRef]
- Park, B.J.; Shin, C.S.; Shin, W.S.; Chung, C.Y.; Lee, S.H.; Kim, D.J.; Kim, Y.H.; Park, C.E. Effects of forest therapy on health promotion among middle-aged women: Focusing on physiological indicators. Int. J. Environ. Res. Public Health 2020, 17, 4348. [Google Scholar] [CrossRef]
- Byrne, D.W.; Rolando, L.A.; Aliyu, M.H.; McGown, P.W.; Connor, L.R.; Awalt, B.M.; Holmes, M.C.; Wang, L.; Yarbrough, M.I. Modifiable healthy lifestyle behaviors: 10-year health outcomes from a health promotion program. Am. J. Prev. Med. 2016, 51, 1027–1037. [Google Scholar] [CrossRef]
- Rathnayake, N.; Alwis, G.; Lenora, J.; Lekamwasam, S. Impact of health-promoting lifestyle education intervention on health-promoting behaviors and health status of postmenopausal women: A quasi-experimental study from Sri Lanka. Biomed. Res. Int. 2019, 2019, 4060426. [Google Scholar] [CrossRef]
- Rathnayake, N.; Alwis, G.; Lenora, J.; Mampitiya, I.; Lekamwasam, S. Effect of health-promoting lifestyle modification education on knowledge, attitude, and quality of life of postmenopausal women. Biomed. Res. Int. 2020, 2020, 3572903. [Google Scholar] [CrossRef] [PubMed]
- Park, S. Mediating effect of a health-promoting lifestyle in the relationship between menopausal symptoms, resilience, and depression in middle-aged women. Health Care Women Int. 2020, 41, 967–983. [Google Scholar] [CrossRef]
- Hanson, S.; Jones, A. Is there evidence that walking groups have health benefits? A systematic review and meta-analysis. Br. J. Sports Med. 2015, 49, 710–715. [Google Scholar] [CrossRef] [PubMed]
- Bang, K.S.; Lee, I.S.; Kim, S.J.; Song, M.K.; Park, S.E. The effects of urban forest-walking program on health promotion behavior, physical health, depression, and quality of life: A randomized controlled trial of office-workers. J. Korean Acad. Nurs. 2016, 46, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Kang, I.; Cho, W.J. The influence on mental health status and health-related quality of life in middle-aged women by the regular walking exercise: By based on the Korea National Health and Nutrition Examination Survey (KNHANES VI). KSW 2016, 11, 207–215. [Google Scholar] [CrossRef]
- Kim, M.S.; Kim, S.H.; Lee, S.H. Effects of walking exercise for wellness convergence in the digital age: Based on physical activity. J. Digit. Converg. 2015, 13, 365–374. [Google Scholar] [CrossRef]
- Pilch, W.; Tota, Ł.; Piotrowska, A.; Śliwicka, E.; Czerwińska-Ledwig, O.; Zuziak, R.; Pilaczyńska-Szcześniak, Ł. Effects of nordic walking on oxidant and antioxidant status: Levels of calcidiol and proinflammatory cytokines in middle-aged women. Oxid. Med. Cell Longev. 2018, 2018, 6468234. [Google Scholar] [CrossRef]
- Fletcher, G.F.; Landolfo, C.; Niebauer, J.; Ozemek, C.; Arena, R.; Lavie, C.J. Promoting physical activity and exercise: JACC health promotion series. J. Am. Coll. Cardiol. 2018, 72, 1622–1639. [Google Scholar] [CrossRef]
- Jacob, L.; Tully, M.A.; Barnett, Y.; Lopez-Sanchez, G.F.; Butler, L.; Schuch, F.; Lopez-Bueno, R.; McDermott, D.; Firth, J.; Grabovac, I.; et al. The relationship between physical activity and mental health in a sample of the UK public: A cross-sectional study during the implementation of COVID-19 social distancing measures. Ment. Health Phys. Act. 2020, 19, 100345. [Google Scholar] [CrossRef]
- Colpani, V.; Baena, C.P.; Jaspers, L.; Van Dijk, G.M.; Farajzadegan, Z.; Dhana, K.; Tielemans, M.J.; Voortman, T.; Freak-Poli, R.; Veloso, G.G.V.; et al. Lifestyle factors, cardiovascular disease and all-cause mortality in middle-aged and elderly women: A systematic review and meta-analysis. Eur. J. Epidemiol. 2018, 33, 831–845. [Google Scholar] [CrossRef]
- Fisher, J.D.; Fisher, W.A.; Amico, K.R.; Harman, J.J. An information-motivation-behavioral skills model of adherence to antiretroviral therapy. Health Psychol. 2006, 25, 462–473. [Google Scholar] [CrossRef] [PubMed]
- Abay, H.; Kaplan, S. Evaluation of the effectiveness of a training program for coping with PMS symptoms based on IMB model in university students. Women Health 2021, 61, 550–561. [Google Scholar] [CrossRef]
- Lee, M.H.; Park, Y.H. The effectiveness of the information-motivation-behavioral skills model-based intervention on preventive behaviors against respiratory infection among community-dwelling older adults. Patient Educ. Couns. 2021, 104, 2028–2036. [Google Scholar] [CrossRef]
- Li, M.; Zhu, H. Application of intervention of information motivation behavior skill (IMB) model in the cardiac rehabilitation of patients with coronary heart disease. Pak. J. Med. Sci. 2022, 38, 1627–1632. [Google Scholar] [CrossRef] [PubMed]
- Maupome, A.L.; de los Muro Ma, Á.V.; Garduño Ma Luisa, M. Improving food choices when eating with peers: An IMB Model-based weight-loss intervention. Curr. Dev. Nutr. 2020, 4, 1327. [Google Scholar] [CrossRef]
- Si, M.; Su, X.; Jiang, Y.; Wang, W.; Zhang, X.; Gu, X.; Ma, L.; Li, J.; Zhang, S.; Ren, Z.; et al. Effect of an IMB Model-based education on the acceptability of HPV vaccination among college girls in mainland China: A cluster RCT. Cancer Control 2022, 29, 10732748211070719. [Google Scholar] [CrossRef]
- Kwan, R.Y.C.; Salihu, D.; Lee, P.H.; Tse, M.; Cheung, D.S.K.; Roopsawang, I.; Choi, K.S. The effect of e-health interventions promoting physical activity in older people: A systematic review and meta-analysis. Eur. Rev. Aging Phys. Act. 2020, 17, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Oseni, K.; Dingley, K.; Hart, P. Instant messaging and social networks: The advantages in online research methodology. Int. J. Inf. Educ. Technol. 2018, 8, 56–62. [Google Scholar] [CrossRef][Green Version]
- Wilson, J.; Heinsch, M.; Betts, D.; Booth, D.; Kay-Lambkin, F. Barriers and facilitators to the use of e-health by older adults: A scoping review. BMC Public Health 2021, 21, 1–12. [Google Scholar] [CrossRef]
- Ministry of the Interior and Safety. Population Status by Age for Korea; Resident Registration Demographics: Sejong, Korea, 2022. Available online: https://jumin.mois.go.kr/index.jsp# (accessed on 15 July 2022).
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Choi, H.J.; Suh, S.R. Effects of a health promotion program on healthy aging preparation for late middle-aged women. Korean J. Adult Nurs. 2015, 27, 594–603. [Google Scholar] [CrossRef]
- Choi, H.Y.; Yang, S.J. Effects of walking program based on social cognitive theory for office workers. Korean J. Adult Nurs. 2013, 25, 712–724. [Google Scholar] [CrossRef]
- Choi, H. Effects of a Walking Program for Office Workers. Ph.D. Thesis, Ewha Womans University, Seoul, Korea, 2012. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.Y.; Yang, Y.J.; Kim, B.S.; Kang, J.H. Validity and reliability of Korean version of International Physical Activity Questionnaire (IPAQ) short form. KJFM 2007, 28, 532–541. [Google Scholar]
- Hwang, W.J. Cardiovascular Disease in Korean Blue-Collar Workers: Actual Risk, Risk Perception, and Risk Reduction Behavior. Ph.D. Thesis, University of California, San Francisco, CA, USA, 2010. [Google Scholar]
- Walker, S.N.; Sechrist, K.R.; Pender, N.J. The Health Promoting Lifestyle Profile development and psychometric characteristics. Nurs. Res. 1987, 36, 76–80. [Google Scholar] [CrossRef]
- Walker, S.N.; Sechrist, K.R.; Pender, N.J. Health Promotion Model-Instruments to Measure Health Promoting Lifestyle: Health-Promoting Lifestyle Profile [HPLP II] (Adult Version). 1995. Available online: https://deepblue.lib.umich.edu/handle/2027.42/85349 (accessed on 15 July 2022).
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Park, J.O.; Seo, Y.S. Validation of the perceived stress scale (PSS) on samples of Korean university students. Korean J. Psychol. Gen. 2010, 29, 611–629. [Google Scholar]
- Ajuwon, A. Mobile Instant Messaging (MIM) to support teaching practice: Insights from a nurse tutor program in Nigeria. Malawi Med. J. 2018, 30, 120–126. [Google Scholar] [CrossRef]
- Morgan, G.; Melson, E.; Davitadze, M.; Ooi, E.; Zhou, D.; Hanania, T.; Chen, W.; Thomas, L.; Allison, I.; Ding, M.; et al. Utility of simulation via instant messaging–Birmingham advance (SIMBA) in medical education during COVID-19 pandemic. J. R. Coll. Physicians Edinb. 2021, 51, 168–172. [Google Scholar] [CrossRef]
- McCarthy, O.; Ahamed, I.; Kulaeva, F.; Tokhirov, R.; Saibov, S.; Vandewiele, M.; Standaert, S.; Leurent, B.; Edwards, P.; Palmer, M.; et al. A randomized controlled trial of an intervention delivered by mobile phone app instant messaging to increase the acceptability of effective contraception among young people in Tajikistan. Reprod. Health 2018, 15, 1–14. [Google Scholar]
- Wang, M.P.; Luk, T.T.; Wu, Y.; Li, W.H.; Cheung, D.Y.; Kwong, A.C.; Lai, V.; Chan, S.S.; Lam, T.H. Chat-based instant messaging support integrated with brief interventions for smoking cessation: A community-based, pragmatic, cluster-randomised controlled trial. Lancet Digit. Health 2019, 1, e183–e192. [Google Scholar] [CrossRef]
- Zheng, C.; Chen, X.; Weng, L.; Guo, L.; Xu, H.; Lin, M.; Xue, Y.; Lin, X.; Yang, A.; Yu, L.; et al. Benefits of mobile apps for cancer pain management: Systematic review. JMIR mHealth uHealth 2020, 8, e17055. [Google Scholar] [CrossRef] [PubMed]
- Bland, V.; Sharma, M. Physical activity interventions in African American women: A systematic review. Health Promot. Perspect. 2017, 7, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Conn, V.S.; Hafdahl, A.R.; Mehr, D.R. Interventions to increase physical activity among healthy adults: Meta-analysis of outcomes. Am. J. Public Health 2011, 101, 751–758. [Google Scholar] [CrossRef]
- Fanning, J.; Mullen, S.P.; McAuley, E. Increasing physical activity with mobile devices: A meta-analysis. J. Med. Internet Res. 2012, 14, e2171. [Google Scholar] [CrossRef]
- Wilbur, J.; Miller, A.M.; Fogg, L.; McDevitt, J.; Castro, C.M.; Schoeny, M.E.; Buchholz, S.W.; Braun, L.T.; Ingram, D.M.; Volgman, A.S.; et al. Randomized clinical trial of the women’s lifestyle physical activity program for African-American women: 24-and 48-week outcomes. Am. J. Health Promot. 2016, 30, 335–345. [Google Scholar] [CrossRef]
- Murtagh, E.M.; Nichols, L.; Mohammed, M.A.; Holder, R.; Nevill, A.M.; Murphy, M.H. The effect of walking on risk factors for cardiovascular disease: An updated systematic review and meta-analysis of randomised control trials. Prev. Med. 2015, 72, 34–43. [Google Scholar] [CrossRef]
- Mandini, S.; Conconi, F.; Mori, E.; Myers, J.; Grazzi, G.; Mazzoni, G. Walking and hypertension: Greater reductions in subjects with higher baseline systolic blood pressure following six months of guided walking. PeerJ 2018, 6, e5471. [Google Scholar] [CrossRef]
- Kim, D.Y.; Seo, B.D.; Kim, D.J. Effect of walking exercise on changes in cardiorespiratory fitness, metabolic syndrome markers, and high-molecular-weight adiponectin in obese middle-aged women. J. Phys. Ther. Sci. 2014, 26, 1723–1727. [Google Scholar] [CrossRef]
- Yuenyongchaiwat, K. Effects of 10,000 steps a day on physical and mental health in overweight participants in a community setting: A preliminary study. Braz. J. Phys. Ther. 2016, 20, 367–373. [Google Scholar] [CrossRef]
- Yuenyongchaiwat, K.; Pipatsitipong, D.; Sangprasert, P. Increasing walking steps daily can reduce blood pressure and diabetes in overweight participants. Diabetol. Int. 2018, 9, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Stults-Kolehmainen, M.A.; Sinha, R. The effects of stress on physical activity and exercise. Sports Med. 2014, 44, 81–121. [Google Scholar] [CrossRef] [PubMed]
- Matzer, F.; Nagele, E.; Lerch, N.; Vajda, C.; Fazekas, C. Combining walking and relaxation for stress reduction: A randomized cross-over trial in healthy adults. Stress Health 2018, 34, 266–277. [Google Scholar] [CrossRef] [PubMed]
- Thomas, A.J.; Mitchell, E.S.; Woods, N.F. The challenges of midlife women: Themes from the Seattle midlife women’s health study. Womens Midlife Health 2018, 4, 1–10. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).