
Co-Design of an eHealth Intervention to Reduce Cardiovascular Disease Risk in Male Taxi Drivers: ManGuard



Abstract
1. Introduction
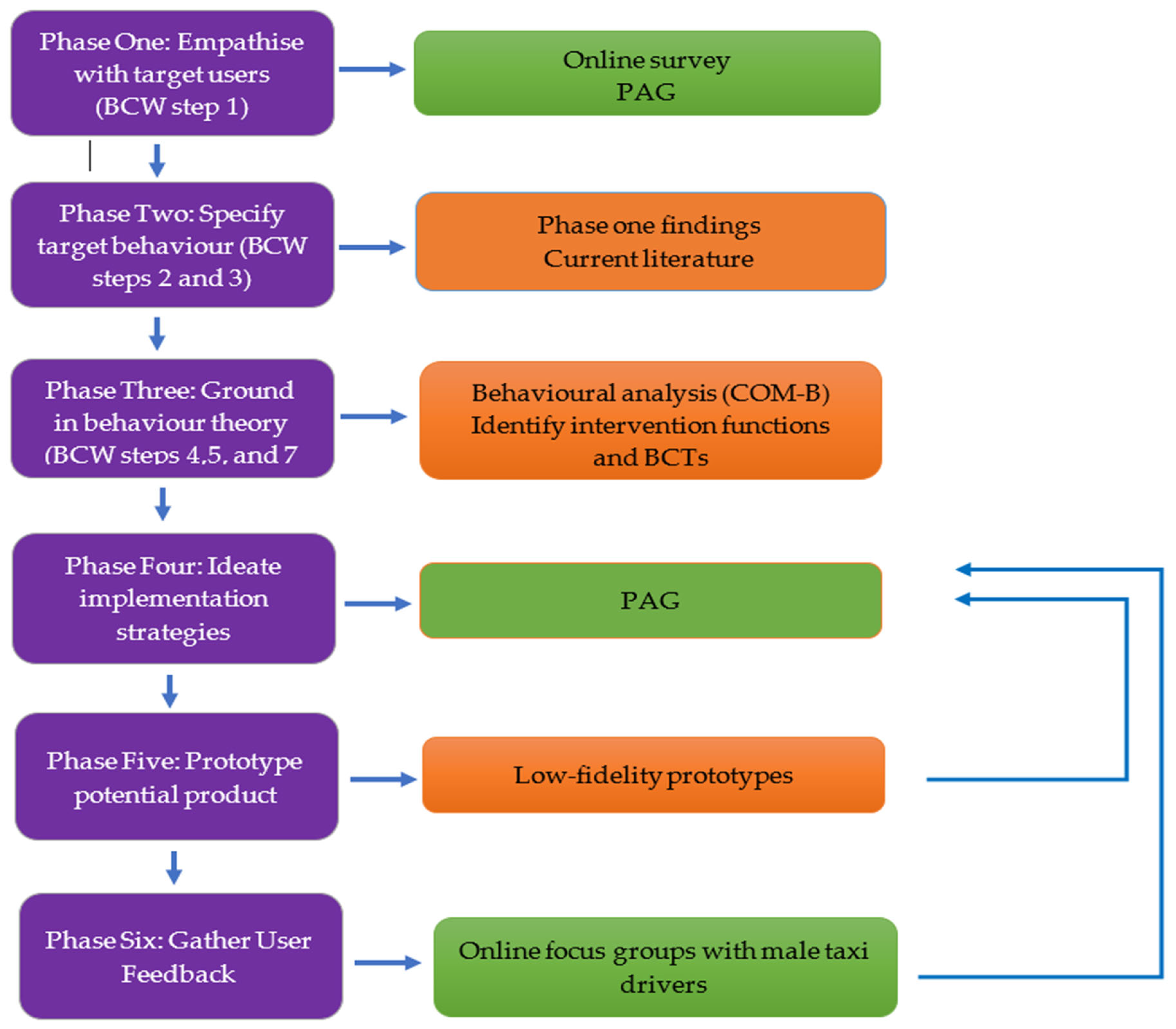
2. Methods
2.1. Phase 1: Empathize with Target Users
2.1.1. Step One: Online Survey
2.1.2. Step Two: Project Advisory Group
- (i)
- A PhD student with expertise in clinical exercise physiology
- (ii)
- A nurse with expertise in cardiovascular nursing and rehabilitation
- (iii)
- A psychologist with expertise in cardiovascular care
- (iv)
- A health services researcher with expertise in developing and evaluating health/social care interventions
- (v)
- A computer scientist/software developer
- (vi)
- A mental health researcher and member of the Men’s Health Forum in Ireland (MHFI)
- (vii)
- Two male taxi drivers.
2.2. Phase 2: Specify Target Behaviours
- Impact of behaviour change: The likely impact that changing the behaviour could have on the population;
- Likelihood of changing behaviour: The likelihood of the population being able to change the behaviour (capability, opportunity, and motivation);
- Spill over score: The possible spill over each behaviour change could have on another behaviour;
- Measurement score: How easy will it be to measure change in the behaviour.
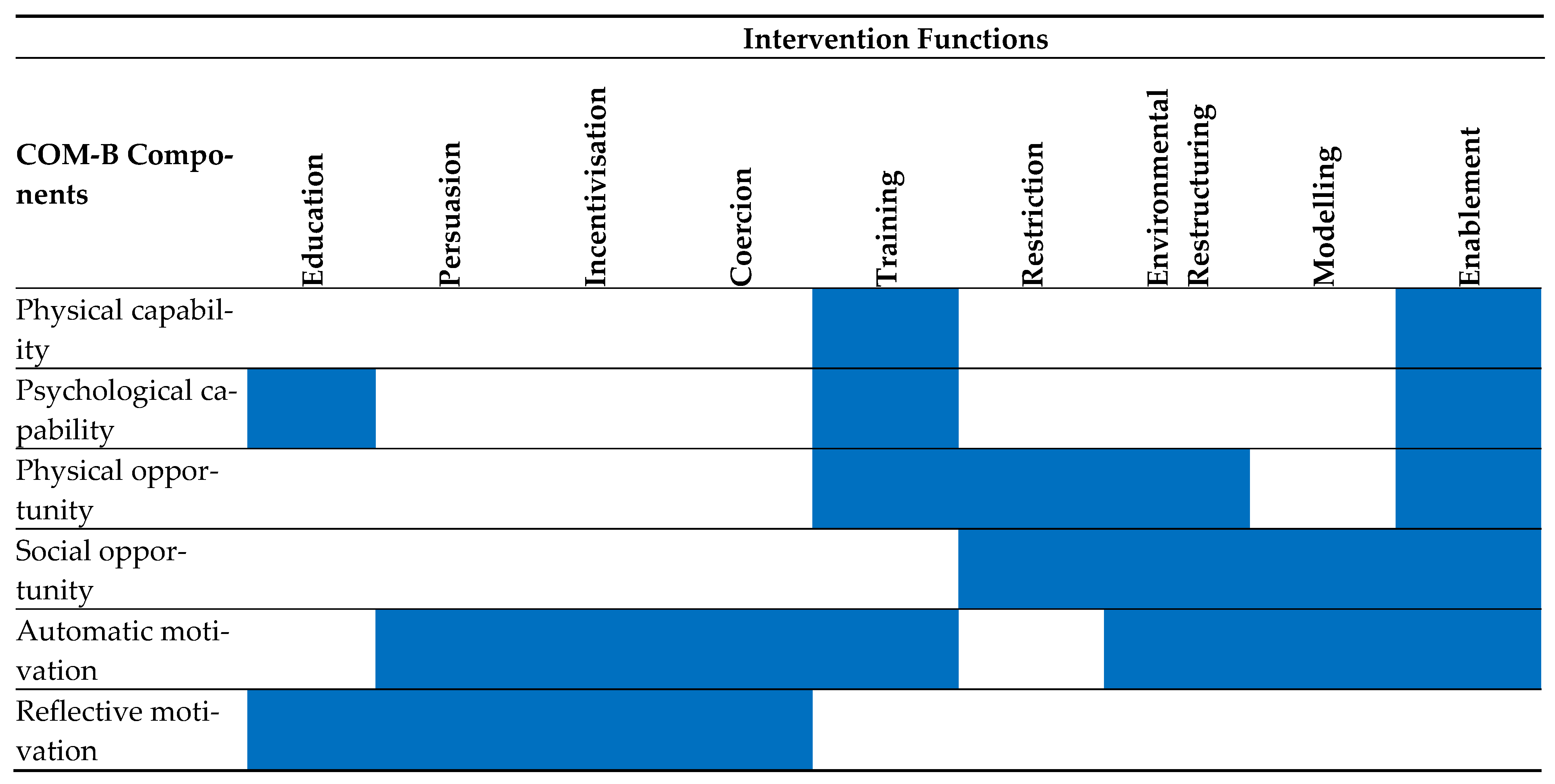
2.3. Phase 3: Ground in Behavioural Theory
2.4. Phase 4. Ideate Implementation Strategies
2.5. Phase 5. Prototype of Potential Products
2.6. Phase 6. Gather User Feedback
3. Results
3.1. Phase 1: Empathize with Target Users
3.1.1. Step One: Online Survey
3.1.2. Step Two: Project Advisory Group
3.2. Phase 2: Specify Target Behaviours
3.3. Phase 3: Ground in Behavioural Theory
3.4. Phases 4 and 5: Ideate Implementation Strategies and Prototype of Potential Products
3.5. Phase 6: Gather User Feedback
3.5.1. Program Design
“Simpler the better.”[F1, P1]
“You know what’s good as well, I like apps… during the night if I’m reading… the writing turns white and all the white that you have there is black which makes it easier to read… if it’s all lit up like, it’s more annoying.”[F1, P2]
“So, would you also have an option for someone to type it in? ‘Cos some people aren’t very good with sliders? Sliders is definitely more visual, but if you have like, if you’re using your mobile phone for it and you’ve got arthritis or something it can be very hard using those slider things…”[F2, P1]
“Yeah, I like it (slider), but as (P1) said, you can get some people who want to be really specific and you’re trying to get it right in the middle but struggling.”[F2, P2]
“I think it looks perfect. I think it looks clean, plain, it’s simple, you know, ManGuard, driving men’s wellbeing… like what else could you want? And then you’ve got a taxi logo there in the middle to act as an A as such, so no I think that’s perfect.”[F2, P2]
“All black the way it is, white writing, suits me down to the ground, that’s simple and clean.”[F2, P3]
“Yeah, I like that. I don’t like those flashy ones with loads of colour. It stands out well.”[F2, P1]
3.5.2. Program Features
“It makes it a bit more interesting I think than going onto a page that’s just full of static text… The pop-up thing is an added bonus to stay on the page, you know?”[F1, P2]
“Who’s going to monitor that messaging system?… All of us will know about taxi forums… there’s no concern to anybody… So, somebody needs to, you know, stop that.”[F1, P2]
“What you’re saying is, if we have a problem that you would normally put on a forum for people, we would just send the question to you and… Yeah, probably better [than a social forum].”[F2, P1]
“You know you’ve got one award, you might be a wee bit motivated to get two, but personally, I’d just be happy enough… if my target was 400 steps a day, if I hit that target that’s fine, you know what I mean?”[F1, P2]
“I would keep them in because I know that there is people who like to see that stuff.”[F1, P1]
3.5.3. Program Content
“We have to remember its aimed at taxi drivers, so a lot of taxi drivers are going to be using this app in between jobs. So, you start reading something, then a job pops up. Say you have to go for straight away, so you don’t wanna be halfway down a three-page item that you lose your place when you come back to it… So nice short, concise paragraphs.”[F1, P1]
“Or just put pictures in, taxi drivers love pictures.”[F1, P1]
“…if there’s too much to click, too much information… you can get lost… Keep the two things just as static pictures.”[F1, P1]
“If you’re going to say we are going to be with you all the time… I mean, is somebody monitoring this in the background? Because if you’re not, you’re not with us all the way…”[F1, P2]
“… that implies that you or somebody associated with you is going to be more or less monitoring what we’re putting in.”[F1, P1]
“I think that’s extremely realistic… I think that’s bang on.”[F2, P3]
“Have you been following me around or something? I eat and drink all of them.”[F3, P1]
“Really, I would say that’s the most important one to be honest here.”[F3, P1]
“Particularly over COVID, that one’s really brilliant… they were a forgotten industry and support… really were terribly supported.”[F3, P3]
3.5.4. Program Engagement
“…maybe, it’ll motivate us more if it was like when you get to level one you receive a £10 voucher, level 2 it’s £20…”[F1, P2]
“… keep it as little as possible on each page and you have to click to go to the next one. If you’re scrolling, again me personally, I get bored and start flicking through it and miss sections.”[F1, P1]
“It makes it a bit more interesting I think than going onto a page that just full of static text with maybe the odd video… The pop-up thing is an added bonus to stay on the page you know?”[F1, P2]
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation. Cardiovascular Diseases (cvds). Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 3 November 2021).
- George, J.; Rapsomaniki, E.; Pujades-Rodriguez, M.; Shah, A.D.; Denaxas, S.; Herrett, E.; Smeeth, L.; Timmis, A.; Hemingway, H. How does cardiovascular disease first present in women and men? Circulation 2015, 132, 1320–1328. [Google Scholar] [CrossRef] [PubMed]
- Brezinov, O.P.; Kivity, S.; Segev, S.; Sidi, Y.; Goldenberg, I.; Maor, E.; Klempfner, R. Gender-related cardiovascular risk in healthy middle-aged adults. Am. J. Cardiol. 2016, 118, 1669–1673. [Google Scholar] [CrossRef] [PubMed]
- Poó, F.M.; Ledesma, R.D.; López, S.S. The taxi industry: Working conditions and health of drivers, a literature review. Transp. Rev. 2018, 38, 394–411. [Google Scholar] [CrossRef]
- Chen, J.-C.; Chen, Y.-J.; Chang, W.P.; Christiani, D.D. Long driving time is associated with haematological markers of increased cardiovascular risk in taxi drivers. Occup. Environ. Med. 2005, 62, 890–894. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.C.; Delp, L. Health status, job stress and work-related injury among los angeles taxi drivers. Work 2014, 49, 705–712. [Google Scholar] [CrossRef]
- Apantaku-Onayemi, F.; Baldyga, W.; Amuwo, S.; Adefuye, A.; Mason, T.; Mitchell, R.; Blumenthal, D.S. Driving to better health: Cancer and cardiovascular risk assessment among taxi cab operators in chicago. J. Health Care Poor Underserved 2012, 23, 768–780. [Google Scholar] [CrossRef]
- De Oliveira, B.G.; Ribeiro, I.J.S.; Bomfim, E.S.; Casottie, C.A.; de Oliveira Boery, R.N.S.; Boery, E.N. Cardiovascular risk factors and quality of life of taxi drivers. J. Nurs. 2015, 9, 7797–7803. [Google Scholar]
- Elshatarat, R.A.; Burgel, B.J. Cardiovascular risk factors of taxi drivers. J. Urban Health. 2016, 93, 589–606. [Google Scholar] [CrossRef]
- Wu, W.-T.; Tsai, S.-S.; Wang, C.-C.; Lin, Y.-J.; Wu, T.-N.; Shih, T.-S.; Liou, S.-H. Professional driver’s job stress and 8-year risk of cardiovascular disease. Epidemiology 2019, 30 (Suppl. 1), S39–S47. [Google Scholar] [CrossRef]
- De Sena, J.E.A.; De Pontes, L.M.; Magno, U.; Ferreira, G.; Da Silva, J.M. Body composition and relationship with the level of physical activity of taxi drivers and postmen of João Pessoa-PB. Fit. Perform. J. 2008, 7, 20–25. [Google Scholar] [CrossRef]
- Bigert, C.; Gustavsson, P.; Hallqvist, J.; Hogstedt, C.; Lewné, M.; Plato, N.; Reuterwall, C.; Schéele, P. Myocardial infarction among professional drivers. Epidemiology 2003, 14, 333–339. [Google Scholar] [CrossRef]
- Gany, F.; Gill, P.; Baser, R.; Leng, J. Supporting South Asian taxi drivers to exercise through pedometers (step) to decrease cardiovascular disease risk. J. Urban Health 2014, 91, 463–476. [Google Scholar] [CrossRef]
- Rezaei Hachesu, V.; Naderyan Feli, S.; Zare Sakhvidi, M.J. Prevalence of cardiovascular risk factors among taxi drivers in yazd, iran. J. Community Health Res. 2017, 6, 200–206. [Google Scholar]
- Murray, K.E.; Buul, A.; Aden, R.; Cavanaugh, A.M.; Kidane, L.; Hussein, M.; Eastman, A.; Checkoway, H. Occupational health risks and intervention strategies for us taxi drivers. Health Promot. Int. 2019, 34, 323–332. [Google Scholar] [CrossRef]
- Ramukumba, T.S.; Mathikhi, M.S. Health assessment of taxi drivers in the city of tshwane. Curationis 2016, 39, a1671. [Google Scholar] [CrossRef]
- Vieira, M.C.; Sperandei, S.; Reis, A.C. Physical activity overcomes the effects of cumulative work time on hypertension prevalence among brazilian taxi drivers. J. Sports Med. Phys. Fit. 2016, 56, 631–638. [Google Scholar]
- Persu, A.; Andries, A.; Demedts, S.; Van Der Niepen, P.; Van De Borne, P. Elevated prevalence of arterial hypertension amongst belgian taxi drivers during the world hypertension day campaign 2006. J. Hypertens. 2006, 24, 2311–2312. [Google Scholar] [CrossRef]
- Choi, Y.H.; Chae, M.-J. Development and effects of smartphone app-based walking exercise program for taxi drivers: Based on Bandura’s self efficacy theory. J. Korean Acad. Nurs. 2020, 50, 242. [Google Scholar] [CrossRef]
- Van Gemert-Pijnen, L.; Kelders, S.M.; Kip, H.; Sanderman, R. eHealth Research, Theory and Development: A Multidisciplinary Approach; Routledge: London, UK, 2018. [Google Scholar]
- Muellmann, S.; Forberger, S.; Möllers, T.; Zeeb, H.; Pischke, C.R. Effectiveness of ehealth interventions for the promotion of physical activity in older adults: A systematic review protocol. Syst. Rev. 2016, 5, 47. [Google Scholar] [CrossRef]
- McMahon, J.; Thompson, D.R.; Pascoe, M.C.; Brazil, K.; Ski, C.F. Ehealth interventions for reducing cardiovascular disease risk in men: A systematic review and meta-analysis. Prev. Med. 2021, 145, 106402. [Google Scholar] [CrossRef]
- Knowlden, A.P.; Wilkerson, A.H.; Dunlap, K.B.; Stellefson, M.; Elijah, O.A. Systematic review of electronically delivered behavioral obesity prevention interventions targeting men. Obes. Rev. 2022, 23, e13456. [Google Scholar] [CrossRef] [PubMed]
- Duan, Y.; Shang, B.; Liang, W.; Du, G.; Yang, M.; Rhodes, R.E. Effects of ehealth-based multiple health behavior change interventions on physical activity, healthy diet, and weight in people with noncommunicable diseases: Systematic review and meta-analysis. J. Med. Internet Res. 2021, 23, e23786. [Google Scholar] [CrossRef] [PubMed]
- Kelders, S.M.; Kok, R.N.; Ossebaard, H.C.; Van Gemert-Pijnen, J.E. Persuasive system design does matter: A systematic review of adherence to web-based interventions. J. Med. Internet Res. 2012, 14, e152. [Google Scholar] [CrossRef] [PubMed]
- Ludden, G.D.; van Rompay, T.J.; Kelders, S.M.; van Gemert-Pijnen, J.E. How to increase reach and adherence of web-based interventions: A design research viewpoint. J. Med. Internet Res. 2015, 17, e172. [Google Scholar] [CrossRef] [PubMed]
- Visser, F.S.; Stappers, P.J.; Van Der Lugt, R.; Sanders, E.B.N. Contextmapping: Experiences from practice. CoDesign 2005, 1, 119–149. [Google Scholar] [CrossRef]
- Robertson, C.; Archibald, D.; Avenell, A.; Douglas, F.; Hoddinott, P.; van Teijlingen, E.; Boyers, D.; Stewart, F.; Boachie, C.; Fioratou, E.; et al. Systematic reviews of and integrated report on the quantitative, qualitative and economic evidence base for the management of obesity in men. Health Technol. Assess. 2014, 18, 1–424. [Google Scholar] [CrossRef]
- McDonald, M.D.; Hunt, K.; Sivaramakrishnan, H.; Moullin, J.; Avenell, A.; Kerr, D.A.; Birch, J.M.; Ntoumanis, N.; Quested, E. A systematic review examining socioeconomic factors in trials of interventions for men that report weight as an outcome. Obes. Rev. 2022, 23, e13436. [Google Scholar] [CrossRef]
- Van Gemert-Pijnen, J.E.; Nijland, N.; van Limburg, M.; Ossebaard, H.C.; Kelders, S.M.; Eysenbach, G.; Seydel, E.R. A holistic framework to improve the uptake and impact of ehealth technologies. J. Med. Internet Res. 2011, 13, e111. [Google Scholar] [CrossRef]
- Mummah, S.A.; Robinson, T.N.; King, A.C.; Gardner, C.D.; Sutton, S. Ideas (integrate, design, assess, and share): A framework and toolkit of strategies for the development of more effective digital interventions to change health behavior. J. Med. Internet Res. 2016, 18, e317. [Google Scholar] [CrossRef]
- Yardley, L.; Morrison, L.; Bradbury, K.; Muller, I. The person-based approach to intervention development: Application to digital health-related behavior change interventions. J. Med. Internet Res. 2015, 17, e30. [Google Scholar] [CrossRef]
- Heckler, E.; King, A.; Banerjee, B.; Robinson, T.; Alonso, M.; Cirimele, J. A Case Study of Bsued: Behavioral Science-Informed User Experience Design. In Proceedings of the SIGCHI Conference Extended Abstracts on Human Factors in Computing Systems, Vancouver, BC, Canada, 7–12 May 2011. [Google Scholar]
- Whittaker, R.; Merry, S.; Dorey, E.; Maddison, R. A development and evaluation process for mhealth interventions: Examples from new zealand. J. Health Commun. 2012, 17, 11–21. [Google Scholar] [CrossRef]
- Mummah, S.A.; King, A.C.; Gardner, C.D.; Sutton, S. Iterative development of vegethon: A theory-based mobile app intervention to increase vegetable consumption. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 90. [Google Scholar] [CrossRef]
- Pratt, M.K. What Is a Proof of Concept (poc)? Available online: https://searchcio.techtarget.com/definition/proof-of-concept-POC (accessed on 14 February 2022).
- Muellmann, S.; Forberger, S.; Möllers, T.; Bröring, E.; Zeeb, H.; Pischke, C.R. Effectiveness of ehealth interventions for the promotion of physical activity in older adults: A systematic review. Prev. Med. 2018, 108, 93–110. [Google Scholar] [CrossRef]
- Webb, T.L.; Joseph, J.; Yardley, L.; Michie, S. Using the internet to promote health behavior change: A systematic review and meta-analysis of the impact of theoretical basis, use of behavior change techniques, and mode of delivery on efficacy. J. Med. Internet Res. 2010, 12, e4. [Google Scholar] [CrossRef]
- Michie, S.; Van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef]
- Michie, S.; Atkins, L.; West, R. The Behaviour Change Wheel: A Guide to Designing Interventions; Silverback Publishing: London, UK, 2014. [Google Scholar]
- Croot, L.; O’Cathain, A.; Sworn, K.; Yardley, L.; Turner, K.; Duncan, E.; Hoddinott, P. Developing interventions to improve health: A systematic mapping review of international practice between 2015 and 2016. Pilot Feasibility Stud. 2019, 5, 127. [Google Scholar] [CrossRef]
- Muller, I.; Santer, M.; Morrison, L.; Morton, K.; Roberts, A.; Rice, C.; Williams, M.; Yardley, L. Combining qualitative research with ppi: Reflections on using the person-based approach for developing behavioural interventions. Res. Involv. Engagem. 2019, 5, 34. [Google Scholar] [CrossRef]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Walker, M.; Takayama, L.; Landay, J.A. High-fidelity or low-fidelity, paper or computer? Choosing attributes when testing web prototypes. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2002, 46, 661–665. [Google Scholar] [CrossRef]
- Hsieh, H.-F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Elo, S.; Kyngäs, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Erlingsson, C.; Brysiewicz, P. A hands-on guide to doing content analysis. Afr. J. Emerg. Med. 2017, 7, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Ding, D.; Mutrie, N.; Bauman, A.; Pratt, M.; Hallal, P.R.C.; Powell, K.E. Physical activity guidelines 2020: Comprehensive and inclusive recommendations to activate populations. Lancet 2020, 396, 1780–1782. [Google Scholar] [CrossRef]
- Mirpuri, S.; Riley, K.; Gany, F. Taxi drivers and modifiable health behaviors: Is stress associated? Work 2021, 69, 1283–1291. [Google Scholar] [CrossRef]
- Kanna, B.; Ukudeyeva, A.; Faiz, M.; Roques, E.; Washington, T.; Ramirez, L.; Shariff, M.A.; Espejo, M. Qualitative study of knowledge, perception, behavior and barriers associated with cardiovascular disease risk among overweight and obese hispanic taxi drivers of South Bronx, NYC. BMC Public Health 2020, 20, 683. [Google Scholar] [CrossRef]
- Chen, X.; Gu, X.; Li, T.; Liu, Q.; Xu, L.; Peng, B.; Wu, N. Factors influencing smoking behaviour of online ride-hailing drivers in china: A cross-sectional analysis. BMC Public Health 2021, 21, 1326. [Google Scholar] [CrossRef]
- Laraqui, O.; Laraqui, S.; Manar, N.; Ghailan, T.; Hammouda, R.; Deschamps, F.; Laraqui, C.E.H. Prevalence of consumption of psychoactive substances amongst moroccan taxi drivers. Med. Lav. 2018, 109, 297–307. [Google Scholar]
- Gavarkovs, A.G.; Burke, S.M.; Petrella, R.J. The physical activity–related barriers and facilitators perceived by men living in rural communities. Am. J. Men’s Health. 2017, 11, 1130–1132. [Google Scholar] [CrossRef]
- Burgel, B.J.; Elshatarat, R.A. Associations between daily-on-the job hassles with perceived mental exertion and depression symptoms in taxi drivers. Am. J. Ind. Med. 2019, 62, 791–802. [Google Scholar] [CrossRef] [PubMed]
- Davidson, S.; Wadley, G.; Reavley, N.; Gunn, J.; Fletcher, S. Psychological distress and unmet mental health needs among urban taxi drivers: A cross-sectional survey. Aust. N. Z. J. Psychiatry 2018, 52, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Useche, S.A.; Cendales, B.; Montoro, L.; Esteban, C. Work stress and health problems of professional drivers: A hazardous formula for their safety outcomes. PeerJ 2018, 6, e6249. [Google Scholar] [CrossRef] [PubMed]
- Hirooka, N.; Kusano, T.; Kinoshita, S.; Nakamoto, H. Influence of perceived stress and stress coping adequacy on multiple health-related lifestyle behaviors. Int. J. Environ. Res. Public Health 2021, 19, 284. [Google Scholar] [CrossRef] [PubMed]
- Moriarty, T.; Bourbeau, K.; Fontana, F.; McNamara, S.; Pereira da Silva, M. The relationship between psychological stress and healthy lifestyle behaviors during COVID-19 among students in a us midwest university. Int. J. Environ. Res. Public Health 2021, 18, 4752. [Google Scholar] [CrossRef]
- Roemmich, J.N.; Lambiase, M.J.; Balantekin, K.N.; Feda, D.M.; Dorn, J. Stress, behavior, and biology. Exerc. Sport Sci. Rev. 2014, 42, 145–152. [Google Scholar] [CrossRef]
- McNeill, E.; Hashemi, A.; Ramirez, J.; Roberts-Eversley, N.; Gany, F. Taxi drivers at risk: Tailoring nutrition and exercise materials. J. Community Health 2019, 44, 888–895. [Google Scholar] [CrossRef]
- Short, C.E.; Vandelanotte, C.; Dixon, M.W.; Rosenkranz, R.; Caperchione, C.; Hooker, C.; Karunanithi, M.; Kolt, G.S.; Maeder, A.; Ding, H.; et al. Examining participant engagement in an information technology-based physical activity and nutrition intervention for men: The manup randomized controlled trial. J. Med. Internet Res. Protoc. 2014, 3, e2. [Google Scholar] [CrossRef]
- Drew, R.J.; Morgan, P.J.; Kay-Lambkin, F.; Collins, C.E.; Callister, R.; Kelly, B.J.; Hansen, V.; Young, M.D. Men’s perceptions of a gender-tailored ehealth program targeting physical and mental health: Qualitative findings from the shed-it recharge trial. Int. J. Environ. Res. Public Health 2021, 18, 12878. [Google Scholar] [CrossRef]
- Morgan, P.J.; Scott, H.A.; Young, M.D.; Plotnikoff, R.C.; Collins, C.E.; Callister, R. Associations between program outcomes and adherence to social cognitive theory tasks: Process evaluation of the shed-it community weight loss trial for men. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 89. [Google Scholar] [CrossRef]
- McMahon, J.; Thompson, D.R.; Brazil, K.; Ski, C.F. An ehealth intervention (manguard) to reduce cardiovascular disease risk in male taxi drivers: Protocol for a feasibility randomised controlled trial. Pilot Feasibility Stud. 2022, 8, 209. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Potential Target Behaviours Relevant to Reducing CVD Risk in Taxi Drivers | Impact of Behaviour Change a | Likelihood of Changing Behaviour a | Spill Over Score a | Measurement Score a |
|---|---|---|---|---|
| Physical activity | Very promising | Promising | Very promising | Very promising |
| Dietary choices | Very promising | Promising | Unpromising but worth considering | Promising |
| Alcohol | Promising | Unpromising but worth considering | Promising | Promising |
| Smoking | Very promising | Unpromising but worth considering | Promising | Promising |
| Target Behaviour | Male taxi drivers need to move more as a means of countering the sedentary nature of the job |
| Who needs to perform the behaviour? | Male taxi drivers |
| What do they need to do differently to achieve the desired change? | Move more every day (steps and/or moderate-vigorous intensity physical activity) |
| When do they need to do it? | Everyday |
| Where do they need to do it? | Home Work Community |
| How often do they need to do it? | Everyday |
| With whom do they need to do it? | Alone Friends Peers Family |
| COM-B Components | What Needs to Happen for Target Behaviour to Occur? | Is There a Need for Change? |
|---|---|---|
| Psychological capability | Know the risks accompanied with a lack of physical activity on CVD | Change needed due to findings from the online survey indicating a lack of knowledge, with most taxi drivers believing that other factors present the greatest risk towards their likelihood of developing CVD rather than physical inactivity |
| Know what constitutes physical activity and the recommendations for how much they should aim to complete | Change needed due to survey responses demonstrating the belief that other behaviours are more pertinent to their risk of developing CVD, and therefore it is plausible that knowledge on the type/amount of physical activity needed to improve their risk is lacking | |
| Social opportunity | Seeing others in close social networks being physically active | Change needed due to taxi drivers rarely seeing each other/spending time together as they work individually, as well as spending long hours at work away from family and friends, indicating a potential lack of social support |
| Reflective motivation | Hold beliefs that being physically active will help reduce their risk of developing CVD | Change needed due to many taxi drivers indicating a belief that behaviours other than physical activity are putting them at higher risk of CVD development |
| Automatic motivation | Create established routines and habits to be more physically active | Change is needed to be more physically active due to unpredictable nature of the job |
| Behavioural analysis of the relevant COM-B components: | Psychological capability, social opportunity, reflective motivation, and automatic motivation need to change for target behaviour to improve. | |
| Results of COM-B Analysis | Appropriate Intervention Functions | BCTs Utilised to Bring about Change (BCTv1) * | Example of How the BCT Could Be Applied to the Intervention |
|---|---|---|---|
| Psychological Capabilities | Education, Enablement, Training | 2.2. Feedback on behaviour 3.1. Social support (unspecified) 4.1. Instruction on how to perform a behaviour 5.1. Information about health consequences | 2.2. Inform the user on how many steps they have walked on a given day/week 3.1. Advise the user on seeking social support to make behaviour change and stick to the improved levels of physical activity 4.1. Provide the user with pictures and videos to explain how to complete the behaviour of being physical active 5.1. Advise the user on the benefits of the behaviour for CVD risk reduction |
| Social opportunity | Enablement, Modelling, Environmental restructuring | 3.1. Social support (unspecified) 6.1. Demonstration of the behaviour 12.2. Restructuring the social environment | 3.1. Provide the user with the ability to seek social support from peers through the program 6.1. Provide the user with information, pictures, and videos to demonstrate the completion of physical activity 12.2. Advise the user to change their social environment towards increasing the time spent with others who will also be physically active |
| Reflective motivation | Education, Persuasion, Enablement | 1.1. Goal setting (behaviour) 1.2. Problem solving 1.3. Goal setting (outcome) 1.4. Action planning 1.6. Discrepancy between current behaviour and goal 2.2. Feedback on behaviour 2.3. Self-monitoring of behaviour 8.2. Behaviour substitution | 1.1. Provide the user with the opportunity to set goals to achieve each week, e.g., how many steps to complete per day/week 1.2. Advise the user to analyse factors that influence their ability to complete physical activity and generate strategies to help them overcome perceived barriers 1.3. Provide the user the opportunity to set a goal to be achieved as a result of increasing their physical activity levels, e.g., setting a weight loss goal to assess change as a result of being more active 1.4. Advise the user to set a plan on when they will choose to be physically active including the frequency, duration, and intensity 1.6. Provide the user with feedback to make them aware that they are struggling to achieve the goal they had set for themself 2.2 Provide the user with automated feedback on their progress, e.g., how many steps they have completed that day 2.3. Provide the opportunity for the user to record and monitor their progress over time 8.2. Advise the user to go for a walk rather than sitting down on the sofa to watch tv or sitting in their car while waiting for a fare |
| Automatic motivation | Persuasion, Incentivisation, Training | 8.3. Habit formation 9.1. Credible source 10.4. Social reward 10.6. Non-specific incentive | 8.3. Advise the user to incorporate physical activity into their routine at the same time each day, e.g., plan to have a break at the same time on each working day and go for a walk during this time 9.1. Provide the user with credible/well known sources in favour of completing physical activity for reducing CVD risk 10.4. Provide the user with positive reinforcement messages when progress is achieved 10.6. Provide the user with positive reinforcement messages when progress is achieved and awards within the program, e.g., badges they can collect as the reach particular milestones |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McMahon, J.; Thompson, D.R.; Brazil, K.; Ski, C.F. Co-Design of an eHealth Intervention to Reduce Cardiovascular Disease Risk in Male Taxi Drivers: ManGuard. Int. J. Environ. Res. Public Health 2022, 19, 15278. https://doi.org/10.3390/ijerph192215278
McMahon J, Thompson DR, Brazil K, Ski CF. Co-Design of an eHealth Intervention to Reduce Cardiovascular Disease Risk in Male Taxi Drivers: ManGuard. International Journal of Environmental Research and Public Health. 2022; 19(22):15278. https://doi.org/10.3390/ijerph192215278
Chicago/Turabian StyleMcMahon, James, David R. Thompson, Kevin Brazil, and Chantal F. Ski. 2022. "Co-Design of an eHealth Intervention to Reduce Cardiovascular Disease Risk in Male Taxi Drivers: ManGuard" International Journal of Environmental Research and Public Health 19, no. 22: 15278. https://doi.org/10.3390/ijerph192215278
APA StyleMcMahon, J., Thompson, D. R., Brazil, K., & Ski, C. F. (2022). Co-Design of an eHealth Intervention to Reduce Cardiovascular Disease Risk in Male Taxi Drivers: ManGuard. International Journal of Environmental Research and Public Health, 19(22), 15278. https://doi.org/10.3390/ijerph192215278