Abstract
Somatization is a phenomenon in which the individual experiences physical symptoms attributable to mental projections. It is a widely used term in common parlance to figuratively describe a stressful situation. Syndromes directly related to the mind have been described; pathologies are influenced by somatization. However, the extent of somatization is also related to social and cultural factors. In fact, each culture expresses varying levels of somatization characteristic of the country of origin. A disease can even manifest with different symptoms in different ethnic groups. The migration process arises from the need for change on the part of those who undertake it and culminates in the integration of the person in the host country. This process induces changes in the person of a psychological nature, which also affects somatization. In fact, the most integrated subjects show levels of somatization comparable to those of the host country. These considerations support the thesis that psychological changes are an integral part of health and can affect the development of organic and somatized pathologies.
1. Introduction
Somatization is responsible for the influence of the mind on the human body. Although the concept of somatization is associated with concern for physical symptoms, it is widely demonstrated that various disorders of a psychological nature significantly affect the clinical history of numerous pathologies. The complexity of these relationships has led to the field of psycho-neuro-endocrine-immunology (PNEI), which studies the interactions between the central nervous, endocrine, and immune systems and their effect on human and animal behavior. The effects of various mental illnesses (post-traumatic stress disorders, affective and eating disorders, etc.) are also responsible for altering interoceptive processes, or perception of internal information, such as breathing, gastrointestinal peristalsis, and sense of hunger, which can lead to sensitization phenomena [1].
Somatization, therefore, represents a modality that the mind uses to communicate with the body. In other words, the externalization of mental suffering is manifested in unique and multiple ways [2].
Several mental pathologies closely related to this phenomenon have been described, such as depression, anxiety, and post-traumatic stress disorder [3,4,5]. This mechanism is individual but is affected by cultural and social habits. Normally, somatization levels are higher in women with low socioeconomic levels and education [6,7,8]. However, the extent of somatization is also associated with cultural phenomena. Cultural differences play an important role in somatization since it is expressed and experienced socio-culturally [9]. For example, Puerto Ricans define particularly stressful events as “ataque de nervios” (attack of nerves) with both physical and behavioral symptoms typically displayed [10]. In addition, the sociomoral situation, personality, and language influence how a disease is labeled [11].
In Western societies, somatic distress is subordinate to the mind and is considered a manifestation of psychological distress [12]. In other cultures, however, this approach is very different.
For example, among non-Western cultures, the Chinese and East Indians manifest somatic symptoms more frequently and are often associated with depressive pictures [13]. In these populations, this modality is frequently used to communicate psychological distress [14]. This is not surprising considering how widespread Hindu, Buddhist, and Confucian traditions are in these cultures, where psychological and somatic distress are synonymous concepts [12]. In China, until the 1980s, psychology was given little consideration, and most psychiatric patients were defined as neurasthenic. Patients were diagnosed with “shenjing shuairuo”, or neurological weakness, which includes a series of somatic symptoms such as insomnia, fatigue, and dizziness along with cognitive symptoms such as poor memory or unpleasant thoughts and emotional symptoms such as irritability, excitability, or nervousness, as well as depressive-type symptoms [15]. For this reason, a social support system called “guanxi” is well established from a young age. This system comprises a complex social and economic relationship that represents a useful point of reference and a rescue net in case of need [16].
Other countries, such as Japan, provide similar social support in traditional culture, typically consisting of a network of extended families; this behavior was particularly useful in improving the somatic symptoms associated with depression in Japanese immigrants who identified with traditional culture [17].
Collectivism is very present in Russia and contrasts with the mostly individualistic conception of European countries. The characteristics of Russian collectivism are different still from Asian ones [18], likely because they arise from the need to contrast the harsh climate, impervious geophysical contexts (mountains, swamps, dense forests, etc.), hostile incursions, and history of serfdom [19]. Social support is enforced as unsolicited encouragement, care, and information [20], as well as unsolicited advice on health and practical matters [21]. The approach to the person is pragmatic and minimizes interpersonal harmony and autonomy [22]. In contrast to collectivism, however, a network of corrupt and individualistic connections described as a phenomenon called blat is used to obtain goods and services beyond formal procedures [16]. It is also interesting to note that Russians exert less control over their negative emotional expression with strangers, but more control over people they know, compared to American, Japanese, and Korean groups [19].
The dominant lifestyle in African cultures is collective, although a part of the population prefers individualized lifestyles; it is difficult to obtain objective assessments when quantitative measures are used, and specific comparisons are often required [23] since there is a tendency towards compliance [24]. However, it has also been found in these populations that pathologies such as depression are often expressed in somatic terms [13].
Given our broad research question and the heterogeneous body of literature and evidence currently available, we opted for the scoping review methodology. The main objectives investigated were related to the concept of acculturation of cultures in various communities and the concept of somatization as a culturally characterizing element.
Regarding the concept of acculturation and culture, the purpose of this study was not to be limited exclusively to the geographical borders of a nation but to analyze the acculturation of culturally divergent groups of people (including the deaf community, Asian American women with breast cancer, immigrants from the Chernobyl area, Ghanaian teachers, intragenerational social mobility, etc.). The extent of somatization was then assessed based on the acculturation process according to the conclusions reported in the various papers.
2. Materials and Methods
The primary emphasis of a scoping review is on the breadth and relevance of the literature, thus including both qualitative and quantitative evidence. The quality of evidence in the included studies is of secondary concern and often difficult to operationalize due to the inclusion of such wide-ranging literature in scoping reviews.
The present review employed the scoping review methodology outlined by Arksey and O’Malley [25], with five stages: (1) developing a research question, (2) searching literature by using inclusion and exclusion criteria, (3) selecting articles, (4) charting data extracted from included articles, and (5) collating, summarizing, and reporting the findings.
Articles matching the search criteria (somatization, medically unexplained symptoms, or functional disease and acculturation) were retrieved on PubMed until July 2021.
A total of 269 articles were identified. A first selection was made, and four articles with an irrelevant title, nine articles without abstracts, two duplicates, and four articles written in a language other than English were excluded. The abstracts of the remaining 250 articles were analyzed. Forty-seven articles were excluded because the abstracts were not relevant. The remaining 203 articles were then analyzed, and 43 articles matching the search criteria were identified [2,3,4,5,6,7,8,10,11,12,13,14,17,19,23,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52].
3. Results
Chinese migrant populations were the most analyzed [3,4,7,12,14,27,30,31,45,46,53], followed by Latin populations [6,10,26,29,34,37,41,48,49,50]. The scales used to assess somatization and acculturation are different, with just a few studies having used the same, but all are self-assessment questionnaires to provide a standardized measure of an individual’s current psychological and/or psychopathological status.
The scales for assessing somatization differed. The most used was the Symptom Checklist-90 Revised (SCL-90R) (11 items), followed by the Brief Symptom Inventory (4 items). Other specific scales used were the Behavioural Assessment System for Children-2nd Edition [4], Hamilton Depression Scale (HAM-D) [32], Hamilton Anxiety Scale (HAM-A) [32,49], Brief Psychiatric Rating Scale (BPRS) [32], Semi-Structured Korean Interview Guide for Depression [11], PERI Demoralization Scale and Social Support Network Inventory [13], Hopkins Symptoms Checklist-25, Harvard Trauma Questionnaire [43], Impact of Event Scale [43], Memorial Symptom Assessment Scale [45,51], Harvard Trauma Questionnaire-Part I [43], PHQ-14 (PHQ somatic symptom scale) [48].
Table 1 shows some somatic aspects described. However, no study has evaluated the concomitant presence of syndromes directly related to the mind (e.g., irritable bowel syndrome, chronic fatigue syndrome), and only one study has evaluated pathologies that are affected by it, such as asthma [51]. Figure 1 shows how all the factors interact together causing a particular type of stress called acculturative stress.

Table 1.
Characteristics of populations cited in the studies are included.
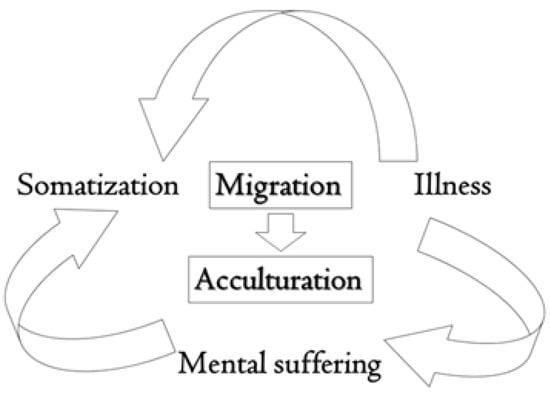
Figure 1.
This diagram highlights the influence and interdependence of migration and acculturation on somatization. In migrants, a particular type of stress called acculturative stress accompanies the migratory process and manifests itself with high levels of somatization.
Acculturation was assessed on different scales as well. The most used was the Suinn Lew Acculturation Scale [12,23,44]. Other scales were Acculturation Scale (Parker) [3], Acculturation Rating Scale for Mexican Americans [7], Behavioural Acculturation Scale [7], Asian American Family Conflict Scale [30], Brief Perceived Ethnic Discrimination Scale-Community Version (PEDQ-CV) [2], Everyday Discrimination Scale [33], Abbreviated Multidimensional Acculturation Scale (AMAS) [4], and Brief Acculturation Rating Scale for Mexican Americans-II (Spanish Version) [34].
4. Discussion
Somatization means transferring a psychological discomfort into somatic symptoms, which imply a disease that needs to be treated [54].
Immigration is a social, political, and economic event that leads people to leave their own country voluntarily or be forced to another land with different customs and cultures.
These people have to adapt to a new life and new habits. This is a process that can lead to clashes of culture and identity. In fact, adapting to a new culture often means modifying and transforming one’s identity and personality [55].
Immigrants want or need to create their own home in a new place, with people usually of different habits and culture. This period can be indefinite or limited in time for study or work reasons (Peace Corps, international students, embassy staff, etc.). Refugees and asylum seekers are people who have been violently forced to uproot themselves from their countries of origin for various reasons: wars, political problems, racial or gender laws, religious issues.
Immigrants are people who have made a relatively free choice to relocate from one country, region or area to another. Theirs is a permanent decision to make their home in a new place. Sojourners are people who make a sustained but time-limited visit to live in another country. For example, Peace Corps workers, international students, and embassy staff can be considered sojourners. More recently, those entering countries as ‘guest workers’ on specific limited-time visa categories can also be considered in this category. Refugees and asylum seekers are people who have been forced to move from their home countries for various reasons.
The acculturation process in migrants and in future generations may be affected by mechanisms already modeled and tested in the cultural evolution literature, which could eliminate cultural variation between groups [56,57,58,59,60,61,62].
Immigration often leads a population with its cultural identity, ethnicity, habits, and customs to move to a territory with a different way of life. This can lead to a slow or fast change in the migrant population, which is reflected in the way of life, habits, and new laws and customs. Although genetic changes occur very slowly, there are still changes in psycho-physical conditions. In fact, cultural traits can change within a few generations. This is the process that tends to maintain cultural variation between groups, even if they undergo frequent migrations [63,64].
Somatization is expressed by individuals inconsistently and subjectively and is affected by the influence of various factors. Among these, a non-negligible aspect is attributed to the cultural context [30]; according to some interpretations, cultural groups systematically differ in their tendency to somatize instead of psychologizing their emotional distress [29,39].
The acculturation process is usually a major source of stress. Economic difficulties, discrimination, loss of social, family and support networks, and language gaps significantly affect mental health and psychological well-being, family and social relationships, development processes and more [65,66,67].
The phenomenon of migration leads to comparing one’s wealth of knowledge and visions of the world with different realities. Through this acculturative process, which is particularly stressful for the migrant and of variable duration and intensity, in favorable cases, a new balance is achieved, associated with good integration and an improvement in somatization concerning the extent of acculturation [36]. Different models of acculturation have been described where both the host culture and culture of origin can play principal roles. From this perspective, the concept of biculturalism is defined by an individual acquiring the host country’s culture while preserving the culture of their country of origin. Interestingly, biculturalism in specific groups has been associated with reduced somatization [33]. However, although the bicultural approach is associated with better integration, the process is quite complex [68,69]. Migrations are often heterogeneous phenomena and can include different dynamics that do not allow univocal conclusions to be drawn. The trauma suffered during migration, for example, could increase the incidence of somatization. For this reason, much attention has been given to the mental health of refugees because past experiences of war and violence, which add to the stressors of migration, could make them more vulnerable to PTSD (post-traumatic stress disorder), chronic pain, and somatic symptoms [70,71]. However, protective factors have also emerged: for those with strong religious beliefs, for example, a buffer role has been found when exposed to traumas of the migratory process of refugees [2].
The scientific evidence emphasizes the effects of migratory experiences on the mental health of migrants. In fact, specific stressors produce symptoms of anguish, anxiety, and depression through their cumulative effect. The traumatic events suffered during the whole migration process (before, during and after) are the main culprits, in addition to the change in place [72].
There is evidence that the risk of developing post-traumatic stress disorder (PTSD) is increased in clandestine migrants with pre-migration poverty [73]. This risk has also increased in poor neighborhoods and in post-migration discrimination [55,74]. Protective factors include a positive family environment and social support. Mental health effects in resettled refugee children in high-income countries were documented in a review in association with exposure to trauma, abusive parents, loss of one or more parents, host country discrimination, neighborhood violence, school isolation, and loss of one or more parents. On the other hand, the psychological well-being of the host environment, social support, stable settlement and religious beliefs were shown to be protective factors [75].
Family relationships are important for the development of a person during growth. In this context, the acculturation of parents shows direct correlations with the somatization of their children [76]. In fact, during the migratory and acculturation process, migrants must learn to recreate a new balance with a new social identity and self-image, often in difficult contexts. They have to find compromises between their new and old culture and learn to use new and different systems, sometimes without any support [77]. This mode prompts most parents to become bicultural. In this way, after evaluating which cognitions or practices of their own culture are more useful, they will modify the less suitable ones by choosing to acquire those of the new culture through experiences of deconstruction and reorganization. These individuals, if they reach a good balance, will manage to live harmoniously in certain situations with the culture of origin and the host culture [78,79,80,81].
Another interesting characteristic that has emerged from various works is that somatization in the migrant not only represents the expression of a transitory phase relating to acculturative stress but is also associated with psychological change. This is because the experiences lived by the migrant induce an adaptation in the individual that affects his way of somatizing [23]. Several studies emphasize that greater acculturation is associated with levels of somatization comparable to those of the host country [10,44]. This consideration is particularly evident in the studies with comparative group interviews conducted in both the migrant’s language of origin and in the host country’s language, which is indicative of acculturation [82]. These considerations underline the fact that the acculturation process induces changes of a psychological nature about somatic symptoms. The acculturation process, however, is complex, and it is not always possible to fully understand the dynamics. Indeed, conflicting studies have also been noted [7,12,83].
Social stress can induce somatic symptoms; this is possible even if an identifiable psychiatric disorder is not diagnosed [29,43,47,84]. Managing these symptoms is not always easy and can, in turn, create other problems such as emotional suppression or inhibition that can lead to further somatic discomfort. Emphasizing these symptoms, however, could distract attention away from recognizing social or interpersonal problems, thereby creating an additional psychosocial disadvantage [11].
Depressive symptoms in Latinas in the United States attributable to depression are not easily diagnosed, as cultural factors influence how they are presented [85,86]. In fact, their discomfort is often expressed in somatic symptoms through physical pain [87,88]. Since it is not always possible to identify them from a medical point of view, health resources are often used unnecessarily. Somatic symptoms in general are frequently associated with mental health problems. In the migrant, they can derive from stress factors that many Latinas may encounter. In Latinas, they can result from stressors that they may encounter. If untreated, persistent somatic symptoms can negatively affect physical and mental health [89].
Stress has also been recognized as an important risk factor for health-related conditions [90,91,92]. It is widely documented that psychosocial stressors are related to the development of organic diseases [93,94]; in particular, the stress experienced in childhood can influence the risks of various chronic physical diseases [95].
5. Conclusions
The migration process induces changes in the psyche that affect the nature of somatization. This change is also related to the acculturation process. The evaluation of somatization is measured according to non-specific symptoms, although several pathologies are closely related. The extent of symptoms and the subjective and objective expressions of diseases are now quantified in an increasingly reliable and specific manner by clinometry. Creating an updated rating scale that includes psychosomatic pathologies following the most recent clinimetric assessments would allow for a better understanding of the influence of socio-cultural contexts on the psyche in the genesis and management of mental-related pathologies, such as in the criteria for psychosomatic research. In this way, it would be possible to deploy treatment strategies more sensitive to specific cultures. There is evidence of how adapting the type of intervention to the cultural model can increase pro-social behavior and reduce children’s anxiety, hyperactivity, and somatization.
Author Contributions
A.B. and F.N. contributed to the research of this manuscript; A.B., A.G. and L.P. contributed to the writing and editing of this manuscript; M.S. supervised the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Available upon request from the corresponding author.
Conflicts of Interest
The authors declare that they have no conflict of interest regarding the publication of this paper.
References
- D’Alessandro, G.; Cerritelli, F.; Cortelli, P. Sensitization and interoception as key neurological concepts in osteopathy and other manual medicines. Front. Neurosci. 2016, 10, 100. [Google Scholar] [CrossRef]
- Mölsä, M.; Kuittinen, S.; Tiilikainen, M.; Honkasalo, M.; Punamäki, R. Mental health among older refugees: The role of trauma, discrimination, and religiousness. Aging Ment. Health 2017, 21, 829–837. [Google Scholar] [CrossRef]
- Jiang, L. Health Service Use Among Chinese American Older Adults: Is There a Somatization Effect? J. Am. Geriatr. Soc. 2019, 67, 584–589. [Google Scholar] [CrossRef]
- Huang, K.Y.; Cheng, S.; Calzada, E.; Brotman, L.M. Symptoms of anxiety and associated risk and protective factors in young Asian American children. Child Psychiatry Hum. Dev. 2012, 43, 761–774. [Google Scholar] [CrossRef][Green Version]
- Kim, H.H.; Lee, Y.J.; Kim, H.K.; Kim, J.E.; Kim, S.J.; Bae, S.M.; Cho, S.J. Prevalence and Correlates of Psychiatric Symptoms in North Korean Defectors. Psychiatry Investig. 2011, 8, 173. [Google Scholar] [CrossRef]
- Shiroma, P.R.; Alarcon, R.D. Time for healing: Somatization among chronically mentally ill immigrants. J. Cult. Divers. 2011, 18, 3. [Google Scholar]
- Mak, W.W.S.; Zane, N.W.S. The phenomenon of somatization among community Chinese Americans. Soc. Psychiatry Psychiatr. Epidemiol. 2004, 39, 967–974. [Google Scholar] [CrossRef]
- Escobar, J.I.; Burnam, M.A.; Karno, M.; Forsythe, A.; Golding, J.M. Somatization in the Community. Arch. Gen. Psychiatry 1987, 44, 713–718. [Google Scholar] [CrossRef]
- Kirmayer, L.J. Cultural variations in the response to psychiatric disorders and emotional distress. Soc. Sci. Med. 1989, 29, 327–339. [Google Scholar] [CrossRef]
- Feldman, J.M.; Ortega, A.N.; Koinis-Mitchell, D.; Kuo, A.A.; Canino, G. Child and family psychiatric and psychological factors associated with child physical health problems: Results from the Boricua Youth Study. J. Nerv. Ment. Dis. 2010, 198, 272. [Google Scholar] [CrossRef]
- Young, K.; Pang, C. Symptoms of depression in elderly korean immigrants: Narration and the healing process. Cult. Med. Psychiatry 1998, 22, 93–122. [Google Scholar]
- Kagawa-singer, M.; Wellisch, D.K.; Durvasula, R. Impact of breast cancer on asian american and anglo american women. Cult. Med. Psychiatry 1997, 21, 449–480. [Google Scholar] [CrossRef]
- Levav, I. Somatic Symptoms Among Older Soviet Immigrants: An Exploratory Study. Sampling 1989, 35, 350–360. [Google Scholar]
- Dhingra, L.; Lam, K.; Homel, P.; Chen, J.; Chang, V.T.; Zhou, J.; Chan, S.; Lam, W.L.; Portenoy, R. Pain in Underserved Community-Dwelling Chinese American Cancer Patients: Demographic and Medical Correlates. Oncologist 2011, 16, 523–533. [Google Scholar] [CrossRef]
- Parker, G.; Sc, D.; Gladstone, G.; Hons, B.A.; Chee, K.T.; Psych, M.R.C. Reviews and Overviews Depression in the Planet’s Largest Ethnic Group: The Chinese. Am. J. Psychiatry 2001, 158, 857–864. [Google Scholar] [CrossRef]
- Ledeneva, A. Blat and Guanxi: Informal practices in Russia and China. Comp. Stud. Soc. Hist. 2008, 50, 118–144. [Google Scholar] [CrossRef]
- Harada, N.; Takeshita, J.; Ahmed, I.; Chen, R.; Petrovitch, H.; Ross, G.W.; Masaki, K. Does cultural assimilation influence prevalence and presentation of depressive symptoms in older Japanese American men? the Honolulu-Asia aging study. Am. J. Geriatr. Psychiatry 2012, 20, 337–345. [Google Scholar] [CrossRef]
- Oyserman, D.; Coon, H.M.; Kemmelmeier, M. Rethinking individualism and collectivism: Evaluation of theoretical assumptions and meta-analyses. Psychol. Bull. 2002, 128, 3. [Google Scholar] [CrossRef]
- Jurcik, T.; Chentsova-dutton, Y.E.; Solopieieva-jurcikova, I.; Ryder, A.G. Russians in Treatment: The Evidence Base Supporting Cultural Adaptations. J. Clin. Psychol. 2013, 69, 774–791. [Google Scholar] [CrossRef]
- Chentsova Dutton, Y.E. Butting in vs. being a friend: Cultural differences and similarities in the evaluation of imposed social support. J. Soc. Psychol. 2012, 152, 493–509. [Google Scholar] [CrossRef]
- Chentsova-Dutton, Y.E.; Vaughn, A. Let Me Tell You What to Do: Cultural Differences in Advice-Giving. J. Cross Cult. Psychol. 2012, 43, 687–703. [Google Scholar] [CrossRef]
- Chirkov, V.I.; Ryan, M.R. Parent and teacher autonomy-support in Russian and US adolescents: Common effects on well-being and academic motivation. J. Cross Cult. Psychol. 2001, 32, 618–635. [Google Scholar] [CrossRef]
- Ofori-Atta, A.M.L.; Linden, W. The effect of social change on causal beliefs of mental disorders and treatment preferences in Ghana. Soc. Sci. Med. 1995, 40, 1231–1242. [Google Scholar] [CrossRef]
- Crittenden, K.S.; Bae, H.; Un, C.; Fugita, S.S.; Lamug, C.B. A Cross-Cultural Study of Self-Report Depressive Symptoms among College Students. J. Cross Cult. Psychol. 1992, 23, 163–178. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. Theory Pract. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Cariello, A.N.; Perrin, P.B. Influence of resilience on the relations among acculturative stress, somatization, and anxiety in latinx immigrants. Brain Behav. 2020, 10, 1–11. [Google Scholar] [CrossRef]
- Eisenbruch, M. Depression in the Chinese: The impact of acculturation. Psychol. Med. 2005, 35, 1475–1483. [Google Scholar]
- David, M.; Borde, T.; Siedentopf, F. Do immigration and acculturation have an impact on hyperemesis gravidarum? Results of a study in Berlin / Germany. J. Psychosom. Obstet. Gynecol. 2012, 33, 78–84. [Google Scholar] [CrossRef]
- Garcini, L.M.; Brown, R.L.; Chen, M.A.; Saucedo, L.; Fite, A.M.; Ye, P.; Ziauddin, K.; Fagundes, C.P. Bereavement among widowed Latinos in the United States: A systematic review of methodology and findings Bereavement among widowed Latinos in the United States: A systematic review of methodology and findings. Death Stud. 2019, 45, 342–353. [Google Scholar] [CrossRef]
- Ahmad, F.; Maule, C.; Wang, J.; Fung, W.L.A. Symptoms and Experience of Depression among Chinese Communities in the West: A Scoping Review. Harv. Rev. Psychiatry 2018, 26, 340–351. [Google Scholar] [CrossRef]
- Juang, L.P.; Cookston, J.T. Acculturation-Based and Everyday Parent-Adolescent Conflict Among Chinese American Adolescents: Longitudinal Trajectories and Implications for Mental Health. J. Fam. Psychol. 2012, 26, 916–927. [Google Scholar] [CrossRef]
- Westermeyer, J.; Bouafuely, M.; Neider, J.; Callies, A. Somatization Among Refugees: An Epidemiologie Study. Psychosomatics 1989, 30, 34–43. [Google Scholar] [CrossRef]
- Lambez, T.; Nagar, M.; Shoshani, A.; Nakash, O. The Association Between Deaf Identity and Emotional Distress Among Adolescents. J. Deaf. Stud. Deaf. Educ. 2020, 25, 1–10. [Google Scholar] [CrossRef]
- Letamendi, A.M.; Ayers, C.R.; Ruberg, J.L.; Singley, D.B.; Wilson, J.; Chavira, D.; Palinkas, L.; Wetherell, J.L. Illness Conceptualizations Among Older Rural Mexican-Americans with Anxiety and Depression. J. Cross Cult. Gerontol. 2013, 28, 421–433. [Google Scholar] [CrossRef]
- Cervantes, R.C.; Salgado de Snyder, V.N.; Padilla, A.M. Posttraumatic stress in immigrants from Central America and Mexico. Hosp. Community Psychiatry 1989, 40, 615–619. [Google Scholar] [CrossRef][Green Version]
- Westermeyer, J.; Neider, J.; Callies, A. Psychosocial adjustment of hmong refugees during their first decade in the united states: A longitudinal study. J. Nerv. Ment. Dis. 1989, 177, 132–139. [Google Scholar] [CrossRef]
- Barcons-castel, N.; Fornieles-deu, A.; Costas-moragas, C. International Adoption: Assessment of Adaptive and Maladaptive Behavior of Adopted Minors in Spain. Span. J. Psychol. 2011, 14, 123–132. [Google Scholar] [CrossRef]
- Beiser, M.; Goodwill, A.M.; Albanese, P.; Mcshane, K.; Nowakowski, M. Predictors of immigrant children ’ s mental health in Canada: Selection, settlement contingencies, culture, or all of the above? Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 743–756. [Google Scholar] [CrossRef]
- Beirens, K.; Fontaine, J.R.J. Somatic complaint differences between Turkish immigrants and Belgians: Do all roads lead to Rome? Ethn. Health 2011, 16, 37–41. [Google Scholar] [CrossRef]
- Cwikel, J.; Abdelgani, A.; Goldsmith, J.R.; Quastel, M. Two-year Follow-up Study of Stress-related Disorders among Immigrants to Israel from the Chernobyl Area. Environ. Health Perspect. 1997, 105, 3–8. [Google Scholar]
- Bzostek, S.; Goldman, N.; Pebley, A. Why do Hispanics in the USA report poor health? Soc. Sci. Med. 2007, 65, 990–1003. [Google Scholar] [CrossRef] [PubMed]
- Cwikel, J.; Rozovski, U. Coping With The Stress Of Immigration Among New Immigrants To Israel From Commonwealth Of Independent States ( Cis ) Who Were Exposed To Chernobyl: The Effect Of Age *. Int. J. Aging Hum. Dev. 1998, 46, 305–318. [Google Scholar] [CrossRef] [PubMed]
- Yeomans, P.D.; Herbert, J.D.; Forman, E.M. Symptom Comparison Across Multiple Solicitation Methods Among Burundians With Traumatic Event Histories. J. Trauma. Stress 2008, 21, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Parker, G.; Chan, B.; Tully, L. Depression and help-seeking in a western sample of ‘highly acculturated’ Chinese and controls. J. Affect. Disord. 2006, 94, 239–242. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.H.Y.; Gomez, S.L.; Brown, R.L.; Kimberly, D.; Laura, A.; Ellen, H.; Yulia, C.D.; Marc, D.S. Factors associated with Chinese American and white cancer survivors’ physical and psychological functioning. Health Psychol. 2019, 38, 455. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.; Chi, I.; Plassman, B.L.; Guo, M. Depressive symptoms and health problems among Chinese immigrant elders in the US and Chinese elders in China. Aging Ment. Health 2010, 14, 37–41. [Google Scholar] [CrossRef]
- Szabo, A.; Ward, C.; Fletcher, G.J.O. Stress appraisal, information processing strategies, and somatic symptoms: A longitudinal study with immigrants. J. Health Psychol. 2019, 24, 650–660. [Google Scholar] [CrossRef]
- Leathers, C.; Kroenke, K.; Flanagan, M.; Diaz, S.; Gruber, R.; Tran, G.; Driver, D. Somatic, Anxiety, and Depressive (SAD) Symptoms in Young Adult Latinx Immigrants: Prevalence and Predictors. J. Immigr. Minor. Health 2021, 23, 956–964. [Google Scholar] [CrossRef]
- Dunlop, B.W.; Still, S.; Loparo, D.; Aponte-Rivera, V.; Johnson, B.N.; Schneider, R.L.; Nemeroff, C.B.; Mayberg, H.S.; Craighead, W.E. Somatic symptoms in treatment—naïve Hispanic and non—Hispanic patients with major depression. Depress. Anxiety 2019, 37, 1–10. [Google Scholar] [CrossRef]
- Green, R.; Polotsky, A.J.; Wildman, R.P.; McGinn, A.P.; Lin, J.; Derby, C.; Johnston, J.; Ram, K.T.; Crandall, C.J.; Thurston, R.; et al. Menopausal symptoms within a Hispanic cohort: SWAN, the Study of Women’s Health Across the Nation. Climacteric 2010, 13, 376–384. [Google Scholar] [CrossRef]
- Park, S.K.; Stotts, N.A.; Douglas, M.K.; Donesky-cuenco, D.; Carrieri-kohlman, V. Care of Patients with Pulmonary Disorders Symptoms and functional performance in Korean immigrants with asthma or chronic obstructive pulmonary disease. Hear. Lung J. Acute. Crit. Care 2012, 41, 226–237. [Google Scholar] [CrossRef] [PubMed]
- Jonsson, F.; Sebastian, M.S.; Hammarström, A.; Gustafsson, P.E. Intragenerational social mobility and functional somatic symptoms in a northern Swedish context: Analyses of diagonal reference models. Int. J. Equity Health 2017, 16, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Berkman, L.F. Physical health and the social environment: A social epidemiological perspective. Relev. Soc. Sci. Med. 1981, 1, 51–75. [Google Scholar]
- Lipowski, Z.J. Somatization: The experience and communication of psychological distress as somatic symptoms. Psychother. Psychosom. 1987, 47, 160–167. [Google Scholar] [CrossRef]
- Hodgetts, D.; Stolte, O.; Sonn, C.; Drew, N.; Carr, S.; Nikora, L.W. Social Psychology and Everyday Life; Bloomsbury Publishing: London, UK, 2020. [Google Scholar]
- Mesoudi, A. Migration, acculturation, and the maintenance of between-group cultural variation. PLoS ONE 2018, 13, e0205573. [Google Scholar] [CrossRef]
- Arora, P.G.; Alvarez, K.; Huang, C.; Wang, C. A Three-Tiered Model for Addressing the Mental Health Needs of Immigrant-Origin Youth in Schools. J. Immigr. Minor. Health 2021, 23, 151–162. [Google Scholar] [CrossRef]
- Brandl, E.J.; Dietrich, N.; Mell, N.; Winkler, J.G.; Gutwinski, S.; Bretz, H.J.; Schouler-Ocak, M. Attitudes towards psychopharmacology and psychotherapy in psychiatric patients with and without migration background. BMC Psychiatry 2020, 20, 1–10. [Google Scholar] [CrossRef]
- Hall, G.C.N. Mental and Behavioral Health of Immigrants in the United States: Cultural, Environmental, and Structural Factors; Academic Press: Cambridge, MA, USA, 2020. [Google Scholar]
- Tian, Y.; Ming, H.; Huang, S.; Zhang, H. Discrimination Increases the Association Between Parental and Adolescent Allostatic Load in Chinese Rural-to-Urban Migrants. J. Adolesc. Health 2020, 66, 499–505. [Google Scholar] [CrossRef]
- Horse, A.J.Y.; Santos-lozada, A.R. Foreign-born Hispanic women′s health patterns in allostatic load converge to US-born Hispanic women at a slower tempo compared with men. Womens Health Issues 2020, 29, 222–230. [Google Scholar]
- Schumann, M.; Bug, M.; Kajikhina, K.; Koschollek, C.; Bartig, S.; Lampert, T.; Santos-Hövener, C. SSM—Population Health The concept of acculturation in epidemiological research among migrant populations: A systematic review. SSM-Popul. Health 2020, 10, 100539. [Google Scholar] [CrossRef]
- Berry, J.W. A Psychology of Immigration. J. Soc. Issues 2001, 57, 615–631. [Google Scholar] [CrossRef]
- Dondi, A.; Piccinno, V.; Morigi, F.; Sureshkumar, S.; Gori, D.; Lanari, M. Food Insecurity and Major Diet—Related Morbidities in Migrating Children: A Systematic Review. Nutrients 2020, 12, 379. [Google Scholar] [CrossRef] [PubMed]
- Fuligni, A.J.; Witkow, M.; Garcia, C. Ethnic identity and the academic adjustment of adolescents from Mexican, Chinese, and European backgrounds. Dev. Psychol. 2005, 41, 799. [Google Scholar] [CrossRef]
- Walsh, S.; Shulman, S.; Feldman, B.; Maurer, O. The Impact of Immigration on the Internal Processes and Developmental Tasks of Emerging Adulthood. J. Youth Adolesc. 2005, 34, 413–426. [Google Scholar] [CrossRef]
- Richter, K.; Baumgärtner, L.; Niklewski, G.; Peter, L.; Köck, M.; Kellner, S. Sleep disorders in migrants and refugees: A systematic review with implications for personalized medical approach. EPMA J. 2020, 11, 251–260. [Google Scholar] [CrossRef]
- Ward, C.; Leong, C.H.; Low, M. Personality and Sojourner Adjustment: An Exploration of the Big Five and the Cultural Fit Proposition. J. Cross Cult. Psychol. 2004, 35, 137–151. [Google Scholar] [CrossRef]
- Szabo, A.; Ward, C.; Fletcher, G.J.O. Identity Processing Styles During Cultural Transition: Construct and Measurement. J. Cross Cult. Psychol. 2016, 47, 483–507. [Google Scholar] [CrossRef]
- Kirmayer, L.J.; Narasiah, L.; Munoz, M.; Rashid, M.; Ryder, A.G.; Guzder, J.; Hassan, G.; Rousseau, C.; Pottie, K. Common mental health problems in immigrants and refugees: General approach in primary care. CMAJ 2011, 183, 959–967. [Google Scholar] [CrossRef]
- Palic, S.; Elklit, A. Psychosocial treatment of posttraumatic stress disorder in adult refugees: A systematic review of prospective treatment outcome studies and a critique. J. Affect. Disord. 2011, 131, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Desjarlais, R.R. World Mental Health: Problems and Priorities in Low-Income Countries; Oxford University Press: New York, NY, USA, 1995. [Google Scholar]
- Gatt, J.M.; Alexander, R.; Emond, A.; Foster, K.; Hadfield, K.; Mason-Jones, A.; Reid, S.; Theron, L.; Ungar, M.; Wouldes, T.A.; et al. Trauma, Resilience, and Mental Health in Migrant and Non-Migrant Youth: An International Cross-Sectional Study Across Six Countries. Front. Psychiatry 2020, 10, 997. [Google Scholar] [CrossRef] [PubMed]
- Perreira, K.M.; Ornelas, I. Painful passages: Traumatic experiences and post-traumatic stress among U.S. immigrant Latino adolescents and their primary caregivers. Int. Migr. Rev. 2013, 47, 976–1005. [Google Scholar] [CrossRef] [PubMed]
- Fazel, M.; Reed, R.V.; Panter-Brick, C.; Stein, A. Mental health of displaced and refugee children resettled in high-income countries: Risk and protective factors. Lancet 2012, 379, 266–282. [Google Scholar] [CrossRef] [PubMed]
- Costigan, C.L.; Dokis, D.P. Relations between parent-child acculturation differences and adjustment within immigrant chinese families. Child Dev. 2006, 77, 1252–1267. [Google Scholar] [CrossRef]
- Bornstein, M.H.; Bohr, Y.; Hamel, K. Immigration, Acculturation, and Parenting. In Encyclopedia on Early Childhood Development; Tremblay, R.E., Boivin, M., Peters, R.D.e.V., Bornstein, M.H., Eds.; Centre of Excellence for Early Childhood Development: Montreal, QC, Canada, 2020; Available online: https://www.child-encyclopedia.com/immigration/according-experts/immigration-acculturation-and-parenting (accessed on 1 December 2020).
- Chia, A.L.; Costigan, C.L. Understanding the multidimensionality of acculturation among Chinese Canadians. Can. J. Behav. Sci. 2006, 38, 311. [Google Scholar] [CrossRef]
- Ryder, A.G.; Alden, L.E.; Paulhus, D.L. Is acculturation unidimensional or bidimensional? A head-to-head comparison in the prediction of personality, self-identity, and adjustment. J. Pers. Soc. Psychol. 2000, 79, 49. [Google Scholar] [CrossRef]
- Tamis-LeMonda, C.S.; Sze, I.N.L.; Ng, F.F.Y.; Kahana-Kalman, R.; Yoshikawa, H. Maternal teaching during play with four-year-olds: Variation by ethnicity and family resources. Merrill Palmer Q. 2013, 59, 361–398. [Google Scholar] [CrossRef]
- Rogala, A.; Szczepaniak, M.; Michalak, N.; Andersson, G. Internet-based self-help intervention aimed at increasing social self-efficacy among internal migrants in Poland: Study protocol for a randomized controlled trial. Internet Interv. 2020, 21, 100322. [Google Scholar] [CrossRef]
- Cuellar, I.; Harris, L.; Jasso, R. An acculturation scale for Mexican American normal and clinical populations. Hisp. J. Behav. Sci. 1980, 2, 199–217. [Google Scholar]
- Lanzara, R.; Scipioni, M.; Conti, C. A Clinical-Psychological Perspective on Somatization Among Immigrants: A Systematic Review. Front. Psychol. 2019, 9, 2792. [Google Scholar] [CrossRef]
- Bustamante, L.H.U.; Cerqueira, R.O.; Leclerc, E.; Brietzke, E. Stress, trauma, and posttraumatic stress disorder in migrants: A comprehensive review. Rev. Bras. Psiquiatr. 2018, 40, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Alegría, M.; Canino, G.; Shrout, P.E.; Woo, M.; Duan, N.; Vila, D.; Torres, M.; Chen, C.; Meng, X.L. Prevalence of mental illness in immigrant and non-immigrant U.S. Latino groups. Am. J. Psychiatry 2008, 165, 359–369. [Google Scholar] [CrossRef]
- Lewis-Fernández, R.; Das, A.K.; Alfonso, C.; Weissman, M.M.; Olfson, M. Depression in US Hispanics: Diagnostic and management considerations in family practice. J. Am. Board Fam. Pract. 2005, 18, 282–296. [Google Scholar] [CrossRef]
- Bauer, A.M.; Chen, C.N.; Alegría, M. Prevalence of physical symptoms and their association with race/ethnicity and acculturation in the United States. Gen. Hosp. Psychiatry 2012, 34, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Interian, A.; Allen, L.A.; Gara, M.A.; Escobar, J.I.; Díaz-Martínez, A.M. Somatic complaints in primary care: Further examining the validity of the patient health questionnaire (PHQ-15). Psychosomatics 2006, 47, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Loeb, T.B.; Joseph, N.T.; Wyatt, G.E.; Zhang, M.; Chin, D.; Thames, A.; Aswad, Y. Predictors of Somatic Symptom severity: The role of cumulative history of trauma and adversity in a diverse community sample. Psychol. Trauma Theory Res. Pract. Policy 2018, 10, 491. [Google Scholar] [CrossRef] [PubMed]
- Mauss, D.; Li, J.; Schmidt, B.; Angerer, P.; Jarczok, M.N. Measuring allostatic load in the workforce: A systematic review. Ind. Health 2015, 53, 5–20. [Google Scholar] [CrossRef]
- Miller, R.; Tomita, Y.; Ing, K.; Ong, C.; Shibanuma, A. Mental well- being of international migrants to Japan: A systematic review. BMJ Open 2019, 9, 1–8. [Google Scholar] [CrossRef]
- Mengistu, B.S. Acculturation and mental health among adult forced migrants: A meta-narrative systematic review protocol. Syst. Rev. 2019, 8, 1–8. [Google Scholar] [CrossRef]
- Glaser, R.; Kiecolt-Glaser, J.K. Stress-induced immune dysfunction: Implications for health. Nat. Rev. Immunol. 2005, 5, 243–251. [Google Scholar] [CrossRef]
- Gouin, J.P.; MacNeil, S. Attachment style and changes in systemic inflammation following migration to a new country among international students. Attach. Hum. Dev. 2019, 21, 38–56. [Google Scholar] [CrossRef]
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults: The Adverse Childhood Experiences (ACE)Study. Am. J. Prev. Med. 2019, 56, 774–786. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).