
Health-Related Quality-of-Life among Pregnant Women after First, Second, and Multiple Cesarean Sections in the Perinatal Period: A Short-Term Longitudinal Study

 ,
,  ,
,
Abstract
1. Introduction
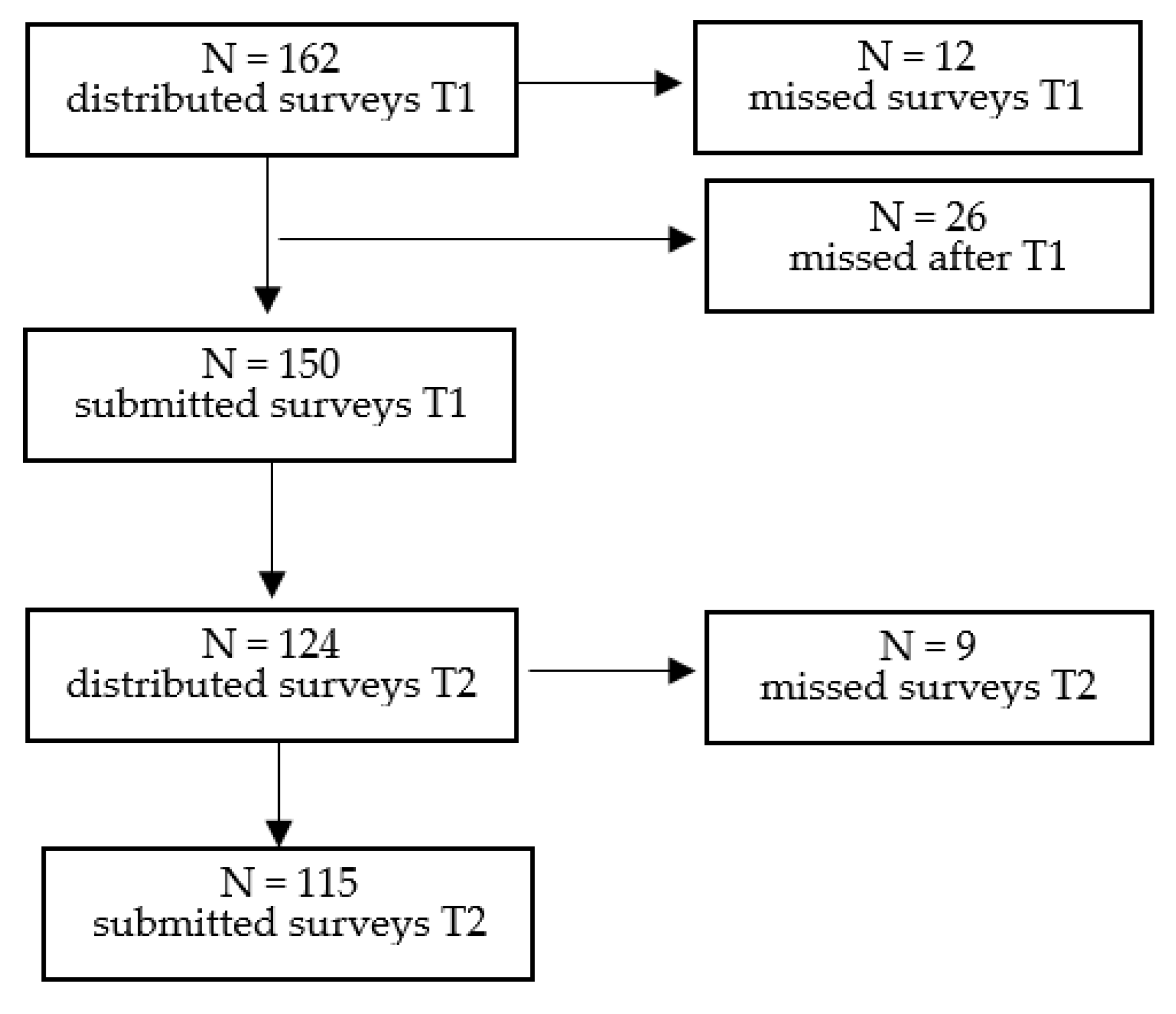
2. Materials and Methods
2.1. Health-Related Quality-of-Life Assessment
2.2. Obstetric Outcomes
2.3. Operation and Anesthetic Outcomes
2.4. Inclusion and Exclusion Criteria
2.5. Statistical Analysis
3. Results
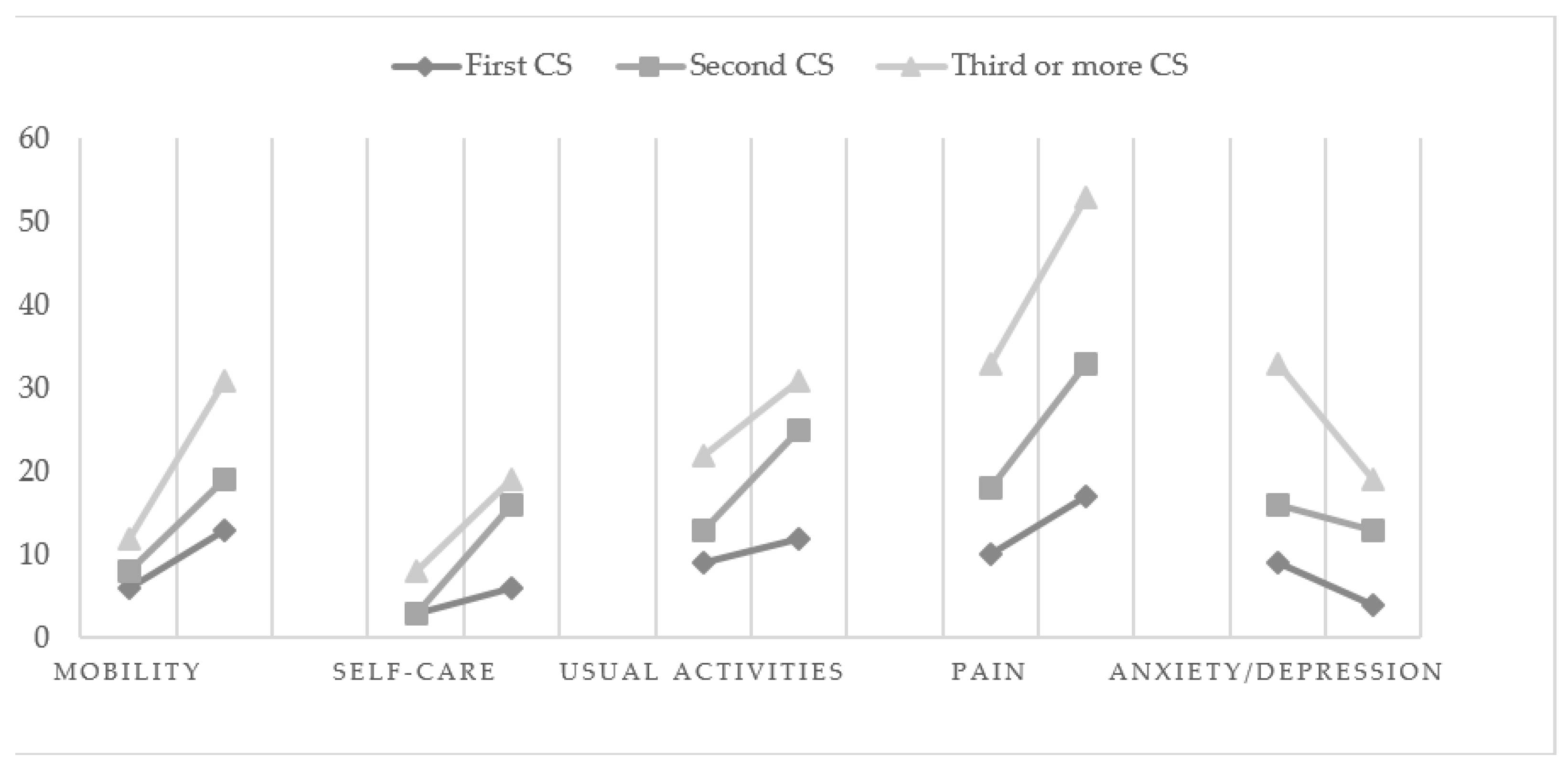
3.1. Health Problems
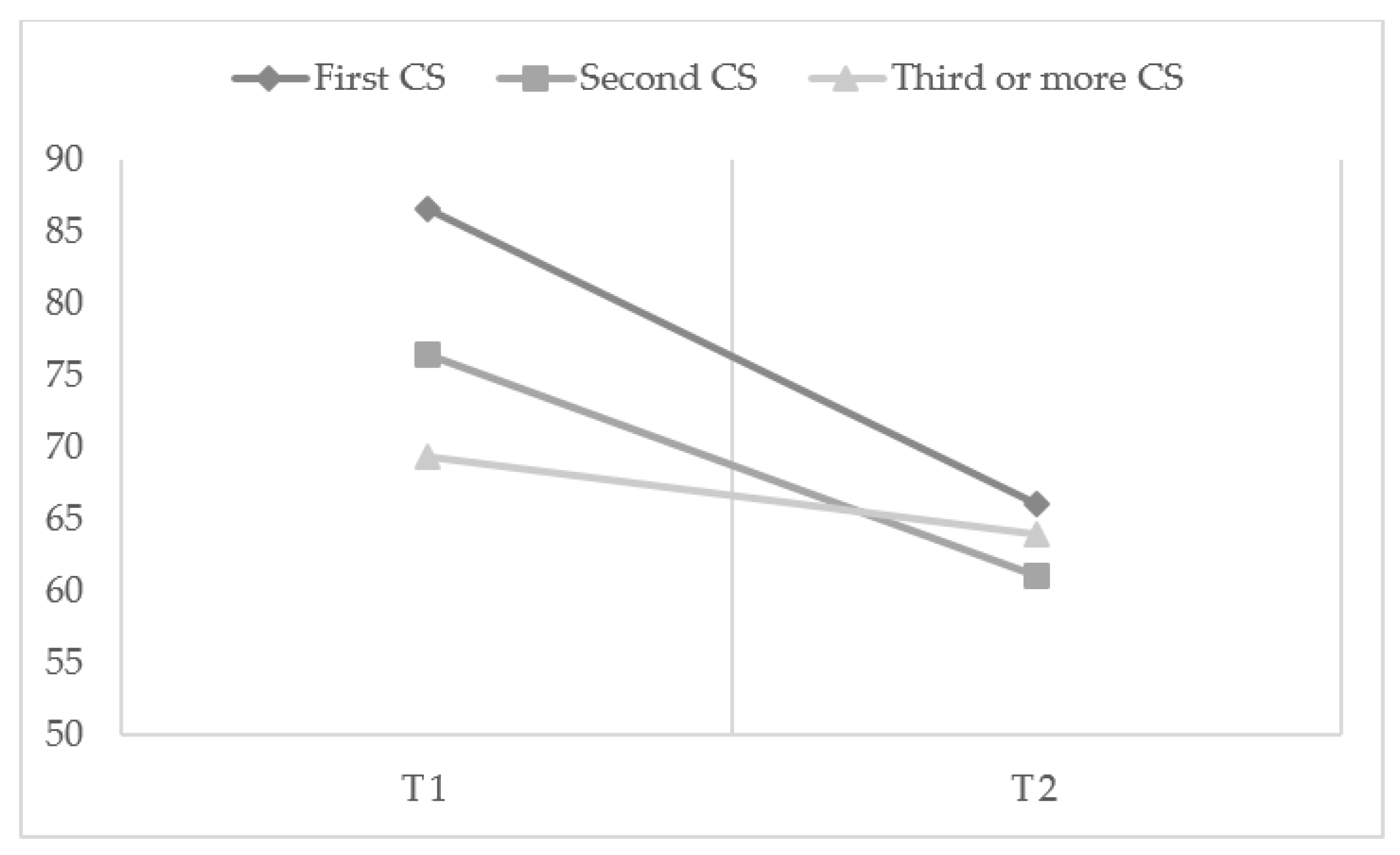
3.2. EQ-VAS Scores
4. Discussion
4.1. Implications for Practice and/or Policy
4.2. Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wielgoś, M.; Bomba-Opoń, D.; Bręborowicz, G.H.; Czajkowski, K.; Dębski, R.; Leszczyńska-Gorzelak, B.; Oszukowski, P.; Radowicki, S.; Zimmer, M. Recommendations of the Polish Society of Gynecologists and Obstetricians Regarding Caesarean Sections. Ginekol. Pol. 2018, 89, 644–657. [Google Scholar] [CrossRef] [PubMed]
- Betran, A.P.; Torloni, M.R.; Zhang, J.J.; Gülmezoglu, A.M. WHO Statement on Caesarean Section Rates. BJOG 2016, 123, 667–670. [Google Scholar] [CrossRef] [PubMed]
- Polish Ministry of Health Rządowy Program Kompleksowej Ochrony Zdrowia Prokreacyjnego w Polsce w 2021-2023 r.—Ministerstwo Zdrowia—Portal Gov.Pl. Available online: https://www.gov.pl/web/zdrowie/program-kompleksowej-ochrony-zdrowia-prokreacyjnego-w-polsce-w-2021-r (accessed on 15 October 2022).
- Mascarello, K.C.; Horta, B.L.; Silveira, M.F. Maternal Complications and Cesarean Section without Indication: Systematic Review and Meta-Analysis. Rev. Saude Publica 2017, 51, S1518–S8787. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Carroli, G.; Zavaleta, N.; Donner, A.; Wojdyla, D.; Faundes, A.; Velazco, A.; Bataglia, V.; Langer, A.; Narváez, A.; et al. Maternal and Neonatal Individual Risks and Benefits Associated with Caesarean Delivery: Multicentre Prospective Study. Br. Med. J. 2007, 335, 1025–1029. [Google Scholar] [CrossRef]
- Ilska, M.; Banaś, E.; Gregor, K.; Brand-Salmerii, A.; Ilski, A.; Cnota, W. Vaginal Delivery or Caesarean Section—Severity of Early Symptoms of Postpartum Depression and Assessment of Pain in Polish Women in the Early Puerperium. Midwifery 2020, 87, 102731. [Google Scholar] [CrossRef]
- Creanga, A.A.; Bateman, B.T.; Butwick, A.J.; Raleigh, L.; Maeda, A.; Kuklina, E.; Callaghan, W.M. Morbidity Associated with Cesarean Delivery in the United States: Is Placenta Accreta an Increasingly Important Contributor? Am. J. Obs. Gynecol. 2015, 213, 384.e1–384.e11. [Google Scholar] [CrossRef]
- Cnota, W.; Banas, E.; Dziechcinska-Poletek, D.; Janowska, E.; Jagielska, A.; Piela, B.; Czuba, B. “The Killer Placenta”—A Threat to the Lives of Young Women Giving Birth by Cesarean Section. Ginekol. Pol. 2022, 93, 314–320. [Google Scholar] [CrossRef]
- Kohler, S.; Sidney Annerstedt, K.; Diwan, V.; Lindholm, L.; Randive, B.; Vora, K.; de Costa, A. Postpartum Quality of Life in Indian Women after Vaginal Birth and Cesarean Section: A Pilot Study Using the EQ-5D-5L Descriptive System. BMC Pregnancy Childbirth 2018, 18, 427. [Google Scholar] [CrossRef]
- Niklasson, B.; Georgsson Öhman, S.; Segerdahl, M.; Blanck, A. Risk Factors for Persistent Pain and Its Influence on Maternal Wellbeing after Cesarean Section. Acta Obs. Gynecol. Scand. 2015, 94, 622–628. [Google Scholar] [CrossRef]
- Marshall, N.E.; Fu, R.; Guise, J.M. Impact of Multiple Cesarean Deliveries on Maternal Morbidity: A Systematic Review. Am. J. Obs. Gynecol. 2011, 205, 262.e1–262.e8. [Google Scholar] [CrossRef]
- Grivell, R.M.; Dodd, J.M. Short- and Long-Term Outcomes after Cesarean Section. Expert Rev. Obstet. Gynecol. 2014, 6, 205–215. [Google Scholar] [CrossRef]
- Torkan, B.; Parsay, S.; Lamyian, M.; Kazemnejad, A. Postnatal Quality of Life in Women after Normal Vaginal Delivery and Caesarean Section. BMC Pregnancy Childbirth 2009, 9, 4. [Google Scholar] [CrossRef] [PubMed]
- Bobek, M.; Humaj-Grysztar, M.; Matuszyk, D.; Put, M. Quality of life assessment of the primiparas in early postpartum period depending on the mode of delivery. Polski Przegląd Nauk Zdrowiu 2018, 2, 154–160. [Google Scholar] [CrossRef]
- Van der Woude, D.A.A.; Pijnenborg, J.M.A.; de Vries, J. Health Status and Quality of Life in Postpartum Women: A Systematic Review of Associated Factors. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 185, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Petrou, S.; Kim, S.W.; McParland, P.; Boyle, E.M. Mode of Delivery and Long-Term Health-Related Quality-of-Life Outcomes: A Prospective Population-Based Study. Birth 2017, 44, 110–119. [Google Scholar] [CrossRef] [PubMed]
- Sadat, Z.; Taebi, M.; Saberi, F.; Kalarhoudi, M.A. The Relationship between Mode of Delivery and Postpartum Physical and Mental Health Related Quality of Life. Iran. J. Nurs. Midwifery Res. 2013, 18, 499. [Google Scholar] [PubMed]
- Golicki, D.; Jakubczyk, M.; Niewada, M.; Wrona, W.; Busschbach, J.J.V. Valuation of EQ-5D Health States in Poland: First TTO-Based Social Value Set in Central and Eastern Europe. Value Health 2010, 13, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Ghaffari, S.; Dehghanpisheh, L.; Tavakkoli, F.; Mahmoudi, H. The Effect of Spinal versus General Anesthesia on Quality of Life in Women Undergoing Cesarean Delivery on Maternal Request. Cureus 2018, 10, e3715. [Google Scholar] [CrossRef]
- Kram, J.J.F.; Montgomery, M.O.; Moreno, A.C.P.; Romdenne, T.A.; Forgie, M.M. Family-Centered Cesarean Delivery: A Randomized Controlled Trial. Am. J. Obs. Gynecol. MFM 2021, 3, 100472. [Google Scholar] [CrossRef]
- Radtke, L.; Dukatz, R.; Biele, C.; Paping, A.; Sameez, K.; Klapp, C.; Henrich, W.; Dückelmann, A.M. Charité Caesarean Birth Improves Birth Experience in Planned and Unplanned Caesarean Sections While Maintaining Maternal and Neonatal Safety: A Prospective Cohort Study. Clin. Exp. Obs. Gynecol. 2022, 49, 124. [Google Scholar] [CrossRef]
- Makoha, F.W.; Felimban, H.M.; Fathuddien, M.A.; Roomi, F.; Ghabra, T. Multiple Cesarean Section Morbidity. Int. J. Gynecol. Obstet. 2004, 87, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Qublan, H.S.; Tahat, Y. Multiple Cesarean Section. The Impact on Maternal and Fetal Outcome. Saudi. Med. J. 2006, 27, 210–214. [Google Scholar] [PubMed]
- Olieman, R.M.; Siemonsma, F.; Bartens, M.A.; Garthus-Niegel, S.; Scheele, F.; Honig, A. The Effect of an Elective Cesarean Section on Maternal Request on Peripartum Anxiety and Depression in Women with Childbirth Fear: A Systematic Review. BMC Pregnancy Childbirth 2017, 17, 195. [Google Scholar] [CrossRef] [PubMed]
- Sobande, A.; Eskandar, M. Multiple Repeat Caesarean Sections: Complications and Outcomes. J. Obstet. Gynaecol. Can. 2006, 28, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Yaman Tunc, S.; Agacayak, E.; Sak, S.; Basaranoglu, S.; Goruk, N.Y.; Turgut, A.; Tay, H.; Elci, E.; Gul, T. Multiple Repeat Caesarean Deliveries: Do They Increase Maternal and Neonatal Morbidity? J. Matern. Fetal Neonatal Med. 2016, 30, 739–744. [Google Scholar] [CrossRef]
- Uyanikoglu, H.; Karahan, M.A.; Turp, A.B.; Agar, M.; Tasduzen, M.E.; Sak, S.; Erdal Sak, M. Are Multiple Repeated Cesarean Sections Really as Safe? J. Matern. Fetal Neonatal Med. 2016, 30, 482–485. [Google Scholar] [CrossRef]
- Biler, A.; Ekin, A.; Ozcan, A.; Inan, A.H.; Vural, T.; Toz, E. Is It Safe to Have Multiple Repeat Cesarean Sections? A High Volume Tertiary Care Center Experience. Pak. J. Med. Sci. 2017, 33, 1074. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Group 1 n (%) | Group 2 n (%) | Group 3 n (%) | Test; p | |
|---|---|---|---|---|
| Age (years) M (SD) | 30.64 (3.10) a | 32.14 (4.51) a | 34.48 (4.80) b | T = 12.47 |
| p = 0.002 | ||||
| Relationship status | χ2 = 14.12 p = 0.007 | |||
| Married | 14 (82.4) | 32 (94.1) | 44 (68.8) | |
| In a relationship | 1 (5.9) | 2 (5.9) | 18 (28.1) | |
| None | 2 (11.8) a | 0 (0.0) | 2 (3.1) | |
| Financial status | χ2 = 6.57 p = 0.160 | |||
| Below average | 1 (5.9) | 4 (11.8) | 4 (6.8) | |
| Average | 11 (64.7) | 28 (82.4) | 40 (67.8) | |
| Above average | 5 (29.4) | 2 (5.9) | 15 (25.4) | |
| Education | χ2 = 11.68 p = 0.06 | |||
| Primary school | 0 (0.0) | 0 (0.0) | 9 (14.5) | |
| Vocational | 0 (0.0) | 2 (5.9) | 7 (11.3) | |
| High school | 4 (25.0) | 11 (32.4) | 14 (22.6) | |
| Postgrad | 12 (75.0) | 21 (61.8) | 32 (51.6) | |
| Work | χ2 = 20.14 p < 0.001 | |||
| Yes, full-time job | 15 (88.2) | 30 (88.2) | 31 (49.2) | |
| Yes, part-time job | 1 (5.9) | 2 (5.9) | 8 (12.5) | |
| No | 1 (5.9) | 2 (5.9) | 24 (37.5) |
| Group 1 n (%) | Group 2 n (%) | Group 3 n (%) | Test; p | |
|---|---|---|---|---|
| Obstetric Characteristic | ||||
| BMI, M (SD) | 28.84 (6.12) | 29.78 (5.91) | 28.65 (28.65) | T = 0.48 p = 0.786 |
| Gestational age at delivery (weeks) | ||||
| M (SD) | 37.82 (1.50) | 37.61 (1.92) | 37.37 (1.75) | T = 2.01 p = 0.366 |
| Unplanned pregnancy | χ2 = 12.56 p = 0.002 | |||
| No | 10 (58.8) | 30 (88.2) | 33 (51.6) | |
| Yes | 7 (41.2) | 4 (11.8) | 30 (46.9) | |
| Miscarriages | χ2 = 1.47 p = 0.372 | |||
| Yes | 4 (23.5) | 10 (29.4) | 24 (37.5) | |
| No | 13 (76.5) | 24 (70.5) | 40 (62.5) | |
| High-risk pregnancy | χ2 = 6.34 p = 0.175 | |||
| Yes | 6 (35.3) | 13 (38.2) | 37 (57.8) | |
| No | 7 (41.2) | 17 (50.0) | 19 (29.7) | |
| Unsure | 4 (23.5) | 4 (11.8) | 8 (12.5) | |
| Chronic medical conditions | χ2 = 1.74 p = 0.580 | |||
| Yes | 7 (41.2) | 8 (23.5) | 18 (28.1) | |
| No | 10 (58.8) | 26 (76.5) | 46 (71.9) | |
| Prenatal diagnosis of placental abnormalities | χ2 = 0.13 p = 0.831 | |||
| Yes | 2 (11.8) | 4 (11.8) | 9 (14.1) | |
| No | 15 (88.2) | 30 (88.2) | 55 (85.9) | |
| Hospital stay (days) M (SD) | 9.82 (13.03) | 8.17 (9.26) | 10.51 (13.09) | T = 3.44 p = 0.179 |
| Premature birth | χ2 = 0.61 p = 0.736 | |||
| Yes | 4 (23.5) | 5 (14.7) | 12 (18.8) | |
| No | 13 (76.5) | 29 (85.3) | 52 (81.3) | |
| Operation Characteristic | ||||
| Anesthesia | χ2 = 3.07 p = 0.215 | |||
| General | 0 (0.0) | 4 (11.8) | 10 (15.6) | |
| Regional (spinal/epidural) | 17 (100) | 30 (88.20 | 54 (84.4) | |
| Type of incision | χ2 = 10.81 p = 0.004 | |||
| horizontal | 13 (76.5) | 20 (58.8) | 23 (35.9) | |
| vertical | 4 (23.5) | 14 (41.2) | 41 (64.1) | |
| Adhesions | χ2 = 9.82 p = 0.007 | |||
| Yes | 1 (2.5) | 10 (29.4) | 29 (45.3) | |
| No | 16 (94.1) | 24 (70.6) | 35 (54.7) | |
| Blood loss M (SD) | 270.58 (91.95) | 485.29 (542.09) | 440.62 (396.80) | T = 12.69 p = 0.002 |
| Operation time M (SD) | 40.29 (10.52) a | 56.82 (24.19) b | 56.82 (32.28) b | T = 8.70 p = 0.013 |
| Cesarean hysterectomy | χ2 = 2.06 p = 0.357 | |||
| Yes | 0 (0.0) | 4 (11.8) | 6 (9.4) | |
| No | 17 (100) | 30 (88.2) | 58 (90.6) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilska, M.; Kołodziej-Zaleska, A.; Banaś-Fiebrich, E.; Brandt-Salmeri, A.; Janowska-Tyc, E.; Łyszczarz, A.; Rzewiczok, J.; Piela, B.; Cnota, W. Health-Related Quality-of-Life among Pregnant Women after First, Second, and Multiple Cesarean Sections in the Perinatal Period: A Short-Term Longitudinal Study. Int. J. Environ. Res. Public Health 2022, 19, 16747. https://doi.org/10.3390/ijerph192416747
Ilska M, Kołodziej-Zaleska A, Banaś-Fiebrich E, Brandt-Salmeri A, Janowska-Tyc E, Łyszczarz A, Rzewiczok J, Piela B, Cnota W. Health-Related Quality-of-Life among Pregnant Women after First, Second, and Multiple Cesarean Sections in the Perinatal Period: A Short-Term Longitudinal Study. International Journal of Environmental Research and Public Health. 2022; 19(24):16747. https://doi.org/10.3390/ijerph192416747
Chicago/Turabian StyleIlska, Michalina, Anna Kołodziej-Zaleska, Ewa Banaś-Fiebrich, Anna Brandt-Salmeri, Ewa Janowska-Tyc, Anna Łyszczarz, Justina Rzewiczok, Bogusława Piela, and Wojciech Cnota. 2022. "Health-Related Quality-of-Life among Pregnant Women after First, Second, and Multiple Cesarean Sections in the Perinatal Period: A Short-Term Longitudinal Study" International Journal of Environmental Research and Public Health 19, no. 24: 16747. https://doi.org/10.3390/ijerph192416747
APA StyleIlska, M., Kołodziej-Zaleska, A., Banaś-Fiebrich, E., Brandt-Salmeri, A., Janowska-Tyc, E., Łyszczarz, A., Rzewiczok, J., Piela, B., & Cnota, W. (2022). Health-Related Quality-of-Life among Pregnant Women after First, Second, and Multiple Cesarean Sections in the Perinatal Period: A Short-Term Longitudinal Study. International Journal of Environmental Research and Public Health, 19(24), 16747. https://doi.org/10.3390/ijerph192416747