
One-Year Impact of COVID-19 Lockdown-Related Factors on Cardiovascular Risk and Mental Health: A Population-Based Cohort Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
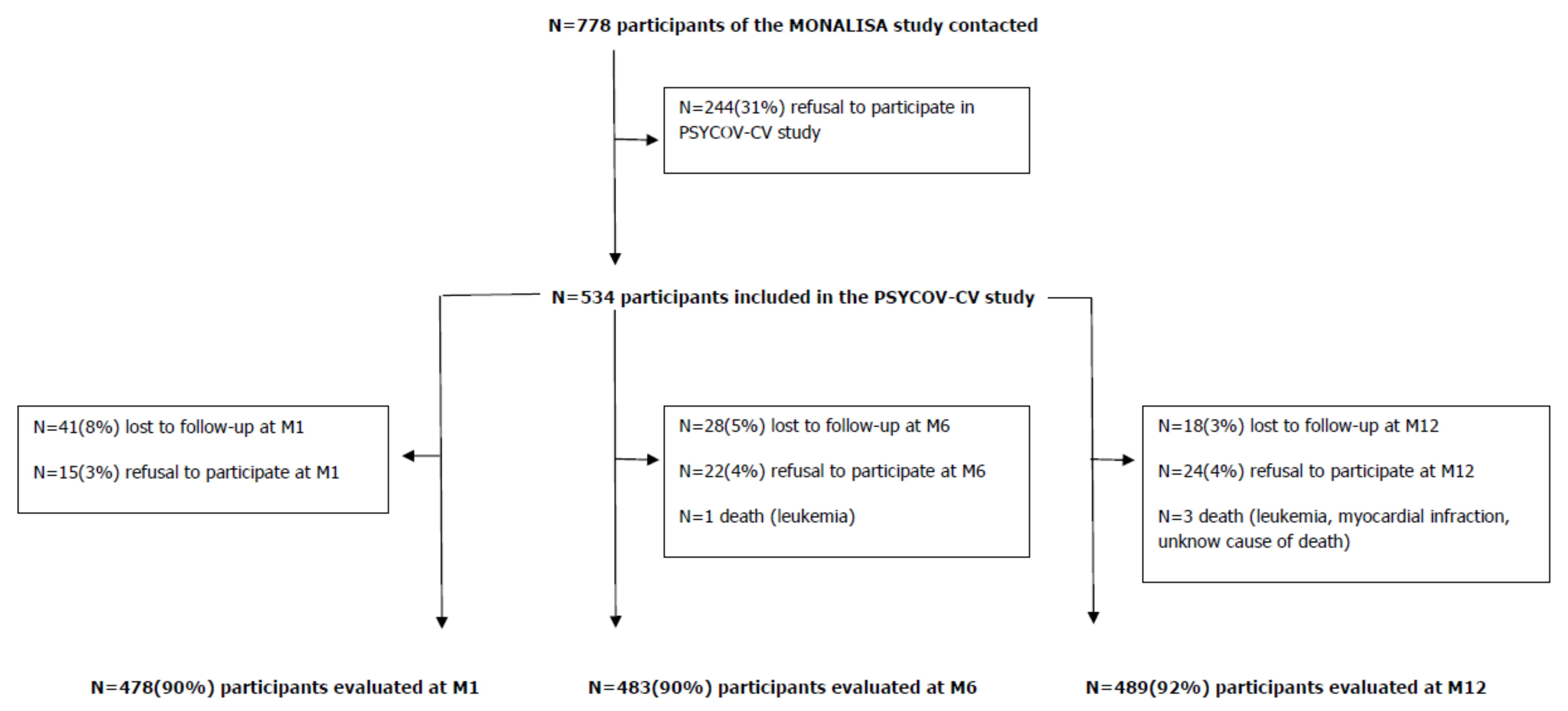
2.1. Study Population
2.2. Telephone Interviews
2.3. Definition of Endpoints and Analysis Sub-Populations
- (i)
- acute cardiovascular event (ischemic heart disease, atherosclerotic cerebrovascular disease, atherosclerosis in other arteries such as aorta or lower limb arteries, chronic heart failure) during the 12 months after lockdown;
- (ii)
- increased antihypertensive, lipid-lowering or hypoglycaemic physician-prescribed drug treatment (i.e., new or higher post-lockdown dosage prescription compared to pre-lockdown);
- (iii)
- reduced post-lockdown physical activity compared to pre-lockdown (≥15 min/week);
- (iv)
- weight gain (>2 kg) after lockdown (compared to pre-lockdown);
- (v)
- reduction in diet quality (i.e., increased post-lockdown consumption of sugary foods, alcohol, fat or carbohydrates, not compensated by increased fruit and vegetable, dairy (within a limit of 2.5 servings/day), or lean protein consumption); or
- (vi)
- increased smoking (≥1 cigarette/day) during the 12 months after lockdown (compared to pre-lockdown).
2.4. Statistical Analysis
2.4.1. Worsening Cardiovascular Risk during the 12-Month Post-Lockdown Follow-Up
2.4.2. Incident Depression and Anxiety during the 12-Month Post-Lockdown Follow-Up
3. Results
3.1. Characteristics of the Participants
3.2. Determinants of Worsening Cardiovascular Risk during the 12-Month Post-Lockdown Follow-Up
3.3. Determinants of Incident Depression and Anxiety during the 12-Month Post-Lockdown Follow-Up
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bérard, E.; Kai, S.H.Y.; Coley, N.; Bongard, V.; Ferrières, J. Lockdown-related factors associated with the worsening of cardiovascular risk and anxiety or depression during the COVID-19 pandemic. Prev. Med. Rep. 2021, 21, 101300. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Luykx, J.J.; Vinkers, C.H.; Tijdink, J.K. Psychiatry in Times of the Coronavirus Disease 2019 (COVID-19) Pandemic: An Imperative for Psychiatrists to Act Now. JAMA Psychiatry 2020, 77, 1097–1098. [Google Scholar] [CrossRef] [PubMed]
- Richter, D.; Riedel-Heller, S.; Zürcher, S.J. Mental health problems in the general population during and after the first lockdown phase due to the SARS-CoV-2 pandemic: Rapid review of multi-wave studies. Epidemiol. Psychiatr. Sci. 2021, 30, e27. [Google Scholar] [CrossRef]
- Turner, A.I.; Smyth, N.; Hall, S.J.; Torres, S.J.; Hussein, M.; Jayasinghe, S.U.; Ball, K.; Clow, A.J. Psychological stress reactivity and future health and disease outcomes: A systematic review of prospective evidence. Psychoneuroendocrinology 2020, 114, 104599. [Google Scholar] [CrossRef]
- Lippi, G.; Henry, B.M.; Bovo, C.; Sanchis-Gomar, F. Health risks and potential remedies during prolonged lockdowns for coronavirus disease 2019 (COVID-19). Diagnosis 2019, 7, 85–90. [Google Scholar] [CrossRef]
- Freiberg, A.; Schubert, M.; Starke, K.R.; Hegewald, J.; Seidler, A. A Rapid Review on the Influence of COVID-19 Lockdown and Quarantine Measures on Modifiable Cardiovascular Risk Factors in the General Population. Int. J. Environ. Res. Public Health 2021, 18, 8567. [Google Scholar] [CrossRef]
- Douglas, M.; Katikireddi, S.V.; Taulbut, M.; McKee, M.; McCartney, G. Mitigating the wider health effects of COVID-19 pandemic response. BMJ 2020, 369, m1557. [Google Scholar] [CrossRef]
- Bongard, V.; Dallongeville, J.; Arveiler, M.; Ruidavets, J.-B.; Amouyel, P.; Wagner, A.; Ferrières, J. Attainment of low-density lipoprotein cholesterol target in the French general population according to levels of cardiovascular risk: Insights from the MONA LISA study. Arch. Cardiovasc. Dis. 2013, 106, 93–102. [Google Scholar] [CrossRef] [Green Version]
- Bongard, V.; Arveiler, D.; Dallongeville, J.; Ruidavets, J.-B.; Wagner, A.; Simon, C.; Marécaux, N.; Ferrieres, J. Food groups associated with a reduced risk of 15-year all-cause death. Eur. J. Clin. Nutr. 2016, 70, 715–722. [Google Scholar] [CrossRef]
- Giovannelli, J.; Dallongeville, J.; Wagner, A.; Bongard, V.; Laillet, B.; Marecaux, N.; Ruidavets, J.B.; Haas, B.; Ferrieres, J.; Arveiler, D.; et al. Validation of a Short, Qualitative Food Frequency Questionnaire in French Adults Participating in the MONA LISA-NUT Study 2005–2007. J. Acad. Nutr. Diet. 2014, 114, 552–561. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Bu, F.; Bone, J.K.; Mitchell, J.J.; Steptoe, A.; Fancourt, D. Longitudinal changes in physical activity during and after the first national lockdown due to the COVID-19 pandemic in England. Sci. Rep. 2021, 11, 17723. [Google Scholar] [CrossRef]
- Navarro-Pérez, C.F.; Fernández-Aparicio, Á.; González-Jiménez, E.; Montero-Alonso, M.Á.; Schmidt-RioValle, J. Effects of COVID-19 lockdown on the dietary habits and lifestyle in a population in southern Spain: A cross-sectional questionnaire. Eur. J. Clin. Nutr. 2021, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Fancourt, D.; Steptoe, A.; Bu, F. Trajectories of anxiety and depressive symptoms during enforced isolation due to COVID-19 in England: A longitudinal observational study. Lancet Psychiatry 2021, 8, 141–149. [Google Scholar] [CrossRef]
- Saunders, R.; Buckman, J.E.J.; Fonagy, P.; Fancourt, D. Understanding different trajectories of mental health across the general population during the COVID-19 pandemic. Psychol. Med. 2021, 1–9. [Google Scholar] [CrossRef]
- Caroppo, E.; Mazza, M.; Sannella, A.; Marano, G.; Avallone, C.; Claro, A.; Janiri, D.; Moccia, L.; Janiri, L.; Sani, G. Will Nothing Be the Same Again? Changes in Lifestyle during COVID-19 Pandemic and Consequences on Mental Health. Int. J. Environ. Res. Public Health 2021, 18, 8433. [Google Scholar] [CrossRef]
- González-Sanguino, C.; Ausín, B.; Castellanos, M.; Saiz, J.; Muñoz, M. Mental health consequences of the COVID-19 outbreak in Spain. A longitudinal study of the alarm situation and return to the new normality. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 107, 110219. [Google Scholar] [CrossRef]
- Brülhart, M.; Klotzbücher, V.; Lalive, R.; Reich, S.K. Mental health concerns during the COVID-19 pandemic as revealed by helpline calls. Nature 2021, 600, 121–126. [Google Scholar] [CrossRef]
- Xu, Z.; Fan, J.; Ding, J.; Feng, X.; Tao, S.; Zhou, J.; Qian, L.; Tao, K.; Hambly, B.D.; Bao, S. The Impact of COVID-19 on Primary Care General Practice Consultations in a Teaching Hospital in Shanghai, China. Front. Med. 2021, 8, 642496. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Total N = 534 |
|---|---|
| Age (in years) during lockdown, mean (SD) | 66.60 (10.36) |
| Male gender, n (%) | 255 (47.8) |
| Number of persons living with participant—during lockdown, mean (SD) | 2.15 (1.12) |
| Home location—during lockdown | |
| Urban, n (%) | 328 (62.2) |
| Rural, n (%) | 199 (37.8) |
| Educational level | |
| <High school completion, n (%) | 201 (37.6) |
| ≥High school completion, n (%) | 321 (60.1) |
| Other, n (%) | 12 (2.2) |
| Professional activity—before lockdown | |
| Not Working, n (%) | 11 (2.1) |
| Working, n (%) | 203 (38.1) |
| Retired, n (%) | 319 (59.8) |
| Professional activity—during lockdown | |
| Working (out of home) without in-person contact with the public (e.g., dustmen), n (%) | 31 (5.8) |
| Working with in-person contact with the public (e.g., cashiers, nurses), n (%) | 43 (8.1) |
| Teleworking, n (%) | 74 (13.9) |
| Not working, n (%) | 386 (72.3) |
| Change in bedtime/wake-up time ≥ 2 h—during lockdown *, n (%) | 92 (17.4) |
| Having more time for oneself **—during lockdown, n (%) | 147 (31.0) |
| During the previous 7 days of lockdown, having a lifestyle that suits oneself | |
| No, n (%) | 20 (3.8) |
| Rather No, n (%) | 40 (7.5) |
| Rather Yes, n (%) | 135 (25.4) |
| Yes, n (%) | 336 (63.3) |
| Self-perceived risk of being contaminated by COVID-19 (on a scale from 1 to 10)—during lockdown, mean (SD) | 3.73 (2.30) |
| Estimated relationship with partner (on a scale from 1 to 10)—during lockdown, mean (SD) | 8.35 (1.53) |
| Worsening relationship with partner during lockdown, n (%) | 33 (8.6) |
| History of high blood pressure—before lockdown, n (%) | 169 (31.7) |
| History of hypercholesterolemia—before lockdown, n (%) | 128 (24.2) |
| History of diabetes—before lockdown, n (%) | 49 (9.2) |
| Increased antihypertensive, lipid-lowering or hypoglycaemic physician prescribed drug treatment—during lockdown, n (%) | 2 (0.4) |
| History of obesity—before lockdown, n (%) | 80 (15.0) |
| History of CVD—before lockdown, n (%) | 64 (12.0) |
| Family history of premature coronary disease ***—before lockdown, n (%) | 56 (11.8) |
| History of anxiety—before lockdown, n (%) | 157 (29.5) |
| Anxiety drug treatment—before lockdown, n (%) | 35 (6.6) |
| History of depression—before lockdown, n (%) | 49 (9.2) |
| Depression drug treatment—before lockdown, n (%) | 29 (5.4) |
| Anxiety: GAD-7—during lockdown, mean (SD) | 2.80 (3.45) |
| Anxiety: GAD-7—during lockdown | |
| No: 0–4 pts, n (%) | 409 (76.7) |
| Mild: 5–9 pts, n (%) | 89 (16.7) |
| Moderate: 10–14 pts, n (%) | 28 (5.3) |
| Severe: 15–21 pts, n (%) | 7 (1.3) |
| Depression: PHQ-9—during lockdown, mean (SD) | 2.92 (3.31) |
| Depression: PHQ-9—during lockdown | |
| No: 0–4 pts, n (%) | 410 (76.9) |
| Mild: 5–9 pts, n (%) | 95 (17.8) |
| Moderate: 10–14 pts, n (%) | 23 (4.3) |
| Moderately severe: 15–19 pts, n (%) | 5 (0.9) |
| Smoking—before lockdown | |
| Yes, regularly (everyday), n (%) | 50 (9.4) |
| Yes, occasionally (<1 cig/d), n (%) | 15 (2.8) |
| No, n (%) | 469 (87.8) |
| Smoking—during lockdown | |
| Yes, regularly (everyday), n (%) | 50 (9.7) |
| Yes, occasionally (<1 cig/d), n (%) | 7 (1.4) |
| No, n (%) | 458 (88.9) |
| Number of cigarettes/day—before lockdown, mean (SD) | 7.43 (6.89) |
| Number of cigarettes/day—during lockdown, mean (SD) | 8.46 (7.75) |
| Smoking—during lockdown | |
| Decreased, n (%) | 17 (3.2) |
| No change, n (%) | 496 (92.9) |
| Increased, n (%) | 21 (3.9) |
| Alcohol consumption—before lockdown | |
| No, n (%) | 183 (34.3) |
| ≥1 glass/week, n (%) | 209 (39.1) |
| ≥1 glass/day, n (%) | 142 (26.6) |
| Alcohol consumption—during lockdown | |
| No, n (%) | 203 (38.0) |
| ≥1 glass/week, n (%) | 182 (34.1) |
| ≥1 glass/day, n (%) | 149 (27.9) |
| Alcohol consumption (glasses/day)—before lockdown, mean (SD) | 0.77 (1.20) |
| Alcohol consumption (in glass/day)—during lockdown, mean (SD) | 0.81 (1.63) |
| Alcohol consumption—during lockdown | |
| Decreased, n (%) | 71 (13.3) |
| No change, n (%) | 400 (74.9) |
| Increased, n (%) | 63 (11.8) |
| Physical activity (min/week)—before lockdown, mean (SD) | 260.54 (322.67) |
| Physical activity (min/week)—during lockdown, mean (SD) | 276.55 (397.64) |
| Physical activity (min/week)—during lockdown | |
| Decreased, n (%) | 193 (36.3) |
| No change, n (%) | 154 (28.9) |
| Increased, n (%) | 185 (34.8) |
| Housework **** (min/week)—before lockdown, mean (SD) | 236.37 (290.23) |
| Housework **** (min/week)—during lockdown, mean (SD) | 288.33 (363.82) |
| Housework **** (min/week)—during lockdown | |
| Decreased, n (%) | 62 (11.9) |
| No change, n (%) | 303 (58.2) |
| Increased, n (%) | 156 (29.9) |
| Increased screen time (hours/day)—during lockdown, n (%) | 281 (53.1) |
| Diet quality—during lockdown | |
| Increased, n (%) | 133 (28.7) |
| No change, n (%) | 188 (40.6) |
| Decreased *****, n (%) | 142 (30.7) |
| Weight gain—during lockdown, n (%) | 138 (26.4) |
| Total N = 534 | |
|---|---|
| Increased physician-prescribed antihypertensive, lipid-lowering or hypoglycaemic drug treatment, n (%) | 56 (11.5) |
| Time of increased physician-prescribed antihypertensive, lipid-lowering or hypoglycaemic drug treatment | |
| M1, n (%) | 8 (14.3) |
| M6, n (%) | 23 (41.1) |
| M12, n (%) | 25 (44.6) |
| Decrease in physical activity (≥15 min/week), n (%) | 326 (65.1) |
| Time of decrease in physical activity (≥15 min/week) | |
| M1, n (%) | 189 (58.0) |
| M6, n (%) | 90 (27.6) |
| M12, n (%) | 47 (14.4) |
| Weight gain > 2 kg, n (%) | 131 (26.5) |
| Time of weight gain > 2 kg | |
| M1, n (%) | 53 (40.5) |
| M6, n (%) | 32 (24.4) |
| M12, n (%) | 46 (35.1) |
| Decrease * in diet quality, n (%) | 304 (60.8) |
| Time of decrease in diet quality | |
| M1, n (%) | 177 (58.2) |
| M6, n (%) | 83 (27.3) |
| M12, n (%) | 44 (14.5) |
| Increased smoking, n (%) | 42 (8.6) |
| Time of increased smoking | |
| M1, n (%) | 23 (54.8) |
| M6, n (%) | 10 (23.8) |
| M12, n (%) | 9 (21.4) |
| Depression (PHQ-9 > 4), n (%) | 172 (34.6) |
| Time of depression (PHQ-9 > 4) | |
| M1, n (%) | 92 (53.5) |
| M6, n (%) | 39 (22.7) |
| M12, n (%) | 41 (23.8) |
| Anxiety (GAD-7 > 4), n (%) | 175 (35.4) |
| Time of anxiety (GAD-7 > 4) | |
| M1, n (%) | 95 (54.3) |
| M6, n (%) | 48 (27.4) |
| M12, n (%) | 32 (18.3) |
| a. Factors independently associated with increased antihypertensive, lipid-lowering or hypoglycaemic drug treatment (N = 56/488 a) | ||
| Adjusted b Odds-Ratio (95% Confidence Interval) | p-Value | |
| Moderate depression (PHQ-9 ≥ 10) c—during lockdown | 5.08 (1.78–14.5) | 0.002 |
| Increased smoking—during lockdown | 5.94 (1.90–18.6) | 0.002 |
| Increased housework d—during lockdown | 0.42 (0.18–0.96) | 0.039 |
| History of high blood pressure—before lockdown | 2.94 (1.56–5.52) | 0.001 |
| History of diabetes—before lockdown | 3.48 (1.61–7.50) | 0.001 |
| b. Factors independently associated with decrease in physical activity ≥ 15 min/week (N = 161/314 e) | ||
| Adjusted b Odds-Ratio (95% Confidence Interval) | p-Value | |
| Depression (PHQ-9 ≥ 3 (median)) c—during lockdown | 1.76 (1.10–2.82) | 0.019 |
| Perceived self-risk of COVID-19 infection (on a scale from 1 to 10) f ≥ 4 (median)—during lockdown | 0.51 (0.32–0.82) | 0.006 |
| Decreased smoking—during lockdown | 0.29 (0.09–0.98) | 0.046 |
| Increasedscreen time—during lockdown | 1.75 (1.10–2.79) | 0.019 |
| Consumption of >3 glasses of alcohol/day—during lockdown | 1.49 (0.94–2.38) | 0.093 |
| c. Factors independently associated with weight gain >2 kg (N = 99/451 g) | ||
| Adjusted b Odds-Ratio (95% Confidence Interval) | p-Value | |
| Depression (PHQ-9 > 4) c—during lockdown | 1.85 (1.08–3.17) | 0.024 |
| During the last 7 days, lifestyle that didn’t suit the participant—during lockdown | 4.29 (1.54–12.0) | 0.005 |
| Perceived self-risk of COVID-19 infection (on a scale from 1 to 10) f > 2 (first quartile)—during lockdown | 0.58 (0.35–0.97) | 0.038 |
| Weight gain (0–2 kg)—during lockdown | 4.31 (2.51–7.40) | <0.001 |
| History of obesity—before lockdown | 2.34 (1.23–4.43) | 0.009 |
| Consumption ≥ 1 glass of alcohol/week—before lockdown | 2.27 (1.34–3.83) | 0.002 |
| d. Factors independently associated with decrease in diet quality h (N = 201/362 i) | ||
| Adjusted b Odds-Ratio (95% Confidence Interval) | p-Value | |
| Age ≥ 70 years | 1.96 (1.22–3.16) | 0.006 |
| Living with >2 people—during lockdown | 0.43 (0.25–0.75) | 0.003 |
| Having more time for oneself j—during lockdown | 2.04 (1.22–3.40) | 0.007 |
| Consumption of ≥1 glass of alcohol/week—during lockdown | 1.55 (0.98–2.46) | 0.058 |
| e. Factors independently associated with increased smoking ≥1 cigarette/day (N = 42/487) | ||
| Adjusted b Odds-Ratio (95% Confidence Interval) | p-Value | |
| Increased smoking—during lockdown | 14.2 (2.82–71.4) | 0.001 |
| Increased consumption of alcohol—during lockdown | 7.52 (2.22–25.5) | 0.001 |
| Increasedscreen time—during lockdown | 8.34 (2.31–30.1) | 0.001 |
| Smoking < 3 cigarettes/day—before lockdown (ref) | 1.00 | |
| Smoking ≥ 3 cigarettes/day—before lockdown | 0.11 (0.02–0.66) | 0.016 |
| Non-smokers—before lockdown | 0.01 (0.002–0.02) | <0.001 |
| a. Factors independently associated with depression (PHQ-9 > 4) (N = 79/362 a) | ||
| Adjusted b Odds-Ratio (95% Confidence Interval) | p-Value | |
| Female gender | 2.96 (1.61–5.43) | <0.001 |
| Anxiety (GAD-7 > 4) c—during lockdown | 2.26 (1.07–4.77) | 0.033 |
| Change in bedtime/wake-up time ≥ 2 h—during lockdown | 2.35 (1.13–4.88) | 0.022 |
| Living in a rural area—during lockdown | 1.70 (0.96–3.03) | 0.069 |
| Estimated relationship with partner (on a scale from 1 to 10) > 8 (median)—during lockdown | 0.56 (0.29–1.08) | 0.084 |
| Symptoms of depression (PHQ-9 = (2–4)) d—during lockdown | 1.65 (0.93–2.93) | 0.084 |
| Smoking > 2 cigarettes/day e—before lockdown | 3.24 (1.23–8.53) | 0.017 |
| Physician-prescribed anxiety drug treatment—before lockdown | 5.08 (1.14–22.6) | 0.033 |
| History of CVD—before lockdown | 2.09 (0.88–4.99) | 0.096 |
| b. Factors independently associated with anxiety (GAD-7 > 4) (N = 83/363 f) | ||
| Adjusted b Odds-Ratio (95% Confidence Interval) | p-Value | |
| Job (out of home) without in-person contact with the public during lockdown (e.g., dustmen) or teleworking (ref) | 1.00 | |
| Job with in-person contact with the public during lockdown (e.g., cashiers, nurses) | 3.38 (1.12–10.2) | 0.031 |
| No job during lockdown | 1.92 (0.89–4.13) | 0.096 |
| Anxiety (for each point of GAD-7) c—during lockdown | 1.91 (1.56–2.34) | <0.001 |
| Decreased alcohol consumption—during lockdown | 0.30 (0.10–0.90) | 0.032 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bérard, E.; Huo Yung Kai, S.; Coley, N.; Bongard, V.; Ferrières, J. One-Year Impact of COVID-19 Lockdown-Related Factors on Cardiovascular Risk and Mental Health: A Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 1684. https://doi.org/10.3390/ijerph19031684
Bérard E, Huo Yung Kai S, Coley N, Bongard V, Ferrières J. One-Year Impact of COVID-19 Lockdown-Related Factors on Cardiovascular Risk and Mental Health: A Population-Based Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(3):1684. https://doi.org/10.3390/ijerph19031684
Chicago/Turabian StyleBérard, Emilie, Samantha Huo Yung Kai, Nicola Coley, Vanina Bongard, and Jean Ferrières. 2022. "One-Year Impact of COVID-19 Lockdown-Related Factors on Cardiovascular Risk and Mental Health: A Population-Based Cohort Study" International Journal of Environmental Research and Public Health 19, no. 3: 1684. https://doi.org/10.3390/ijerph19031684
APA StyleBérard, E., Huo Yung Kai, S., Coley, N., Bongard, V., & Ferrières, J. (2022). One-Year Impact of COVID-19 Lockdown-Related Factors on Cardiovascular Risk and Mental Health: A Population-Based Cohort Study. International Journal of Environmental Research and Public Health, 19(3), 1684. https://doi.org/10.3390/ijerph19031684