
Factors Influencing the Practice of Healthy Living as an Integrated Indicator of the Elderly’s Drinking, Smoking, and Walking Patterns: Using Korea Community Health Surveys


Abstract
:1. Introduction
1.1. Rationale for the Study
1.2. Theoretical Framework
2. Materials and Methods
2.1. Data Source
2.2. Papulation
2.3. Study Variables
2.3.1. Dependent Variable
2.3.2. Independent Variables
2.4. Data Collection
2.5. Data Analysis
2.6. Ethical Considerations
3. Results
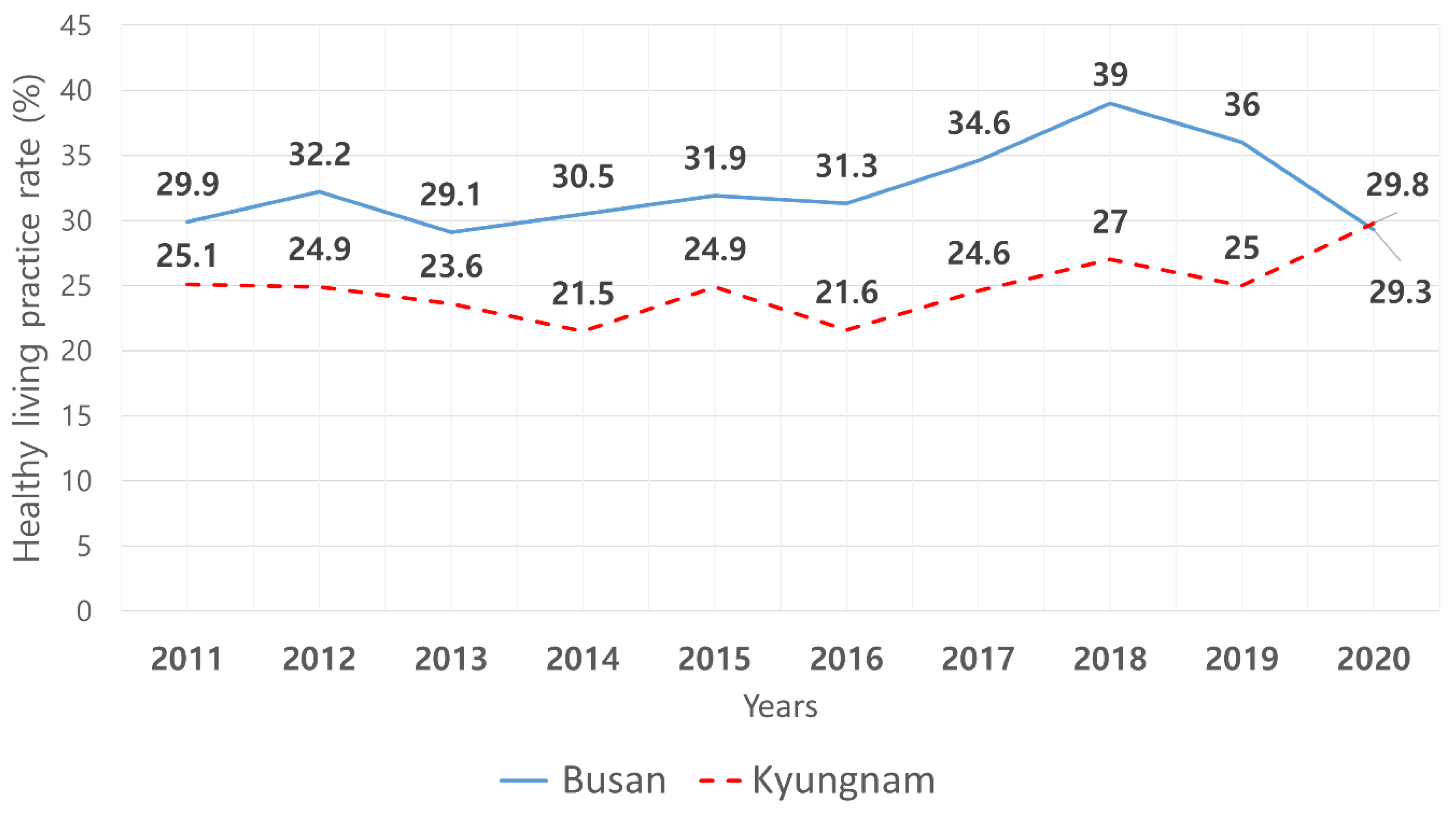
3.1. Differences in Healthy Lifestyle Practice between Busan and Gyeongnam Regions
3.2. Predictors of Healthy Lifestyle Practice in Older Adults in Busan and Gyeongnam
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Action Plan for the Prevention and Control of NCDs 2013–2020; World Health Organization: Geneva, Switzerland, 2013. Available online: https://www.who.int/publications/i/item/9789241506236 (accessed on 30 October 2021).
- Statistics Korea. 2020 Statics for the Elderly; Statistics Korea: Daejeon, Korea, 2020. Available online: http://kostat.go.kr/portal/korea/kor_nw/1/1/index.board?bmode=read&aSeq=385322 (accessed on 20 November 2021).
- Park, E.J.; Jun, J.; Kim, N.S. The association of multiple risky health behaviors with self-reported poor health, stress, and depressive symptom. Health Soc. Welf. Rev. 2015, 35, 136–157. [Google Scholar]
- Korea Centers for Disease Control and Prevention. Guideline of Use Raw Data about 2017 Community Health Survey; Korea Center for Disease Control and Prevention: Chungju, Korea, 2017. Available online: https://chs.kdca.go.kr/chs/mnl/mnlBoardMain.do (accessed on 30 October 2021).
- Korea Centers for Disease Control and Prevention. 2018 National Health and Nutrition Examination Survey; Korea Center for Disease Control and Prevention: Chungju, Korea, 2018. Available online: https://health.kdca.go.kr/healthinfo/biz/pblcVis/details.do (accessed on 30 October 2021).
- Kang, E.J. Clustering of lifestyle behaviors of Korean adults using smoking, drinking and physical activity. Health Soc. Welf. Rev. 2007, 2, 44–66. [Google Scholar]
- Jeong, J.Y.; Kim, C.; Shin, M.; Ryu, S.Y.; Hong, J.; Kim, N.H.; Hwang, T.Y.; Kim, H.; Kim, K.Y.; Lee, H.; et al. Factors related with regional variations of health behaviors and health status: Based on Community Health Survey and regional characteristic data. Korea Public Health Res. 2017, 43, 91–108. [Google Scholar]
- Jeong, C.R.; Kim, J.M.; Park, C.Y.; Shin, E.; Tchoe, B. Determinants of healthy living practice: Country approach. Health Policy Manag. 2020, 30, 376–385. [Google Scholar]
- Gyeongnam Provincial Office. About Gyeongnam. Changwon: Gyeongnam Provincial Office; Gyeongnam Provincial Office: Changwon, Korea. Available online: https://www.gyeongnam.go.kr/index.gyeong?menuCd=DOM_000000106002001002 (accessed on 30 October 2021).
- Son, J.S.; Jo, H.; Kim, C.B.; Kim, S.M.; Min, I.G.; Kong, I.D. An approach to reduce the regional gap of health equity: What factors influence walking practices between two district by social ecological model? Korean J. Health Promot. 2018, 35, 35–51. [Google Scholar] [CrossRef]
- Dolansky, M.; Moore, S.M. Effects of cardiac rehabilitation on older adult’s recovery outcomes following coronary artery bypass surgery. J. Cardiopulm. Rehabil. 2004, 24, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Hyun, H.S.; Lee, I.S. Body Mass Index (BMI)-Related Factors of Community-Dwelling Elders: Comparison between Early and Late Elderly People. J. Korean Acad. Community Health Nurs. 2013, 24, 62. [Google Scholar] [CrossRef]
- Tak, Y.-J.; Lee, J.-G.; Kim, Y.-J.; Lee, S.Y.; Jung, D.-W.; Yi, Y.-H.; Cho, Y.-H.; Choi, E.-J.; Lee, S.-H.; Hwang, H.-L.; et al. Excessive Sodium Intake and Related Factors According to Energy Intakes among Korean Elderly: A Nationwide Cross-Sectional Study. J. Korean Geriatr. Soc. 2014, 18, 185–198. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.S. The study of the impact of the family type on the health-promoting behavior and physical and mental health of elderly people. Health Soc. Welf. Rev. 2014, 34, 400–429. [Google Scholar]
- Lee, Y.H.; Kim, H.K.; Kwon, G.H. Compliance with a low-salt diet, sodium intake, and preferred salty taste in the hypertensive elderly. J. Korean Public Health Nurs. 2010, 24, 311–322. [Google Scholar]
- Yi, Y.H.; Kim, Y.J.; Cho, D.Y. Family type and health behaviors in elderly: Korean National Health and Nutrition Examination Survey (KNHANES), 2010–2012. Korean J. Health Serv. Manag. 2014, 8, 199–207. [Google Scholar] [CrossRef]
- Kim, A.; Jeon, H.O. The influence of health behaviors and sleep-related factors on cognitive function in the elderly hypertensive patients. J. Korean Acad.-Ind. Coop. Soc. 2015, 16, 7078–7088. [Google Scholar]
- Jung, Y.J.; Lee, S.K. The study on the causality among built environment, social relationship and health of the elderly. J. Korean Reg. Dev. Assoc. 2015, 27, 75–94. [Google Scholar]
- Song, Y.; Nam, E. The influence of social capital and health behaviors on self-rated health in South Korea. Korean J. Health Educ. Promot. 2009, 26, 1–13. [Google Scholar]
- Kim, J.H.; Park, J. The effect of social capital on health-related quality of life using the data 2019 community health survey. J. Agric. Med. Community Health 2021, 46, 280–294. [Google Scholar]
- Kang, D. Research on social capital in Busan and social companies. Senshu Soc. Cap. Rev. 2013, 4, 211–225. [Google Scholar]
- United Nation. Identifying Assessing Encouraging Developing Your Local Social Capital; Sustainable Development Goal Partnership Platform: New York, NY, USA, 2021; Available online: https://sustainabledevelopment.un.org/partnership/?p=11706 (accessed on 20 December 2021).
- Zhang, L.; Ding, Z.; Qiu, L.; Li, A. Falls and risk factors of fall for urban and rural community-dwelling older adults in China. BMC Geriatr. 2019, 19, 379. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.H. The regional health inequity, and individual and neighborhood level health determinants. Health Soc. Welf. Rev. 2016, 36, 345–384. [Google Scholar]
- Lee, S.J.; Shim, M.S. Effects of health literacy and unmet health care needs on health promotion behavior among elderly in the community. J. Korean Public Health Nurs. 2020, 34, 238–250. [Google Scholar]
- Kim, J.E.; Hahm, M.I. Associated between residential are and unmet healthcare needs due to physical accessibility. Health Policy Manag. 2021, 31, 197–206. [Google Scholar]
- An, Y.I.; Choi, D.H.; Lee, T.Y.; Park, S.J.; Jung, M.C.; Jang, H.; Shim, G.H. Association between self-reported health status and influenza vaccination in Korean adults: Analysis of the 2014–2015 Korea national health and nutrition examination survey. Korean J. Fam. Pract. 2021, 11, 247–255. [Google Scholar] [CrossRef]
- Simsek, H.; Doganay, S.; Budak, R.; Ucku, R. Relationship of socioeconomic status with health behaviors and self-perceived health in the elderly: A community-based study, Turkey. Geriatr. Gerontol. Int. 2014, 14, 960–968. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.S.; Lee, H.; Kim, M.W. The correlates of influenza vaccination among Korean elderly men and women. J. Acad. Community Health Nurs. 2011, 22, 45–55. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Category | Variables | Busan † | Gyeongnam † |
|---|---|---|---|
| Gender | ● | ● | |
| Age | ● | ● | |
| Demographic characteristics | Education level | ● | ● |
| Income (KRW 1000) | ○ | ○ | |
| Spouse | ● | ◐ | |
| Daily sleep times (per week) | ◐ | ○ | |
| Frequency of breakfast (last week) | ○ | ○ | |
| Low-salt diet | ● | ● | |
| BMI | ◐ | ○ | |
| Health-related characteristics | Diagnosed hypertension | ◐ | ○ |
| Diagnosed diabetes mellitus | ○ | ○ | |
| Subjective perceived health | ● | ● | |
| Stress | ○ | ○ | |
| Depressive mood experience | ○ | ○ | |
| Health-related characteristics | Limited daily activity | ● | ● |
| Neighbours’ trust | ○ | ◐ | |
| Mutual aid | ○ | ○ | |
| Social network (neighbours) | ○ | ◐ | |
| Social network (family) | ○ | ○ | |
| Interpersonal factor | Social network (friends) | ○ | ◐ |
| Religious activity | ● | ● | |
| Socialize activity | ○ | ◐ | |
| Free/Leisure activity | ○ | ○ | |
| Charity activity | ○ | ○ | |
| Overall safety level | ○ | ○ | |
| Satisfaction with natural environment | ○ | ○ | |
| Satisfaction with life environment | ◐ | ○ | |
| Satisfaction with public transportation | ○ | ○ | |
| Community factor | Cancer screening | ◐ | ○ |
| Health screening | ○ | ○ | |
| Vaccination | ◐ | ◐ | |
| Utilized public healthcare | ○ | ○ | |
| Unmet medical needs | ○ | ◐ | |
| Falling accident | ◐ | ○ |
| Variables | Busan | Gyeongnam | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Yes (n = 306) | No | χ2 or t | p | Yes (n = 229) | No | χ2 or t | p | |||
| (n = 6724) | (n = 7562) | |||||||||
| n † (% ‡) or | n † (% ‡) or | n † (% ‡) or | n † (% ‡) or | |||||||
| M ± SE ‡ | M ± SE ‡ | M ± SE ‡ | M ± SE ‡ | |||||||
| Personal factor | Gender | male | 43,482 (9.0) | 437,360 (91.0) | 292.16 | <0.001 | 20,060 (6.1) | 308,765 (93.9) | 206.5 | <0.001 |
| female | 3331 (0.6) | 562,782 (99.4) | 2128 (0.5) | 410,213 (99.5) | ||||||
| Age | ≥75 | 9502 (2.5) | 364,177 (97.5) | 33.97 | <0.001 | 4146 (1.5) | 267,168 (98.5) | 33.28 | <0.001 | |
| 65–74 | 37,310 (5.5) | 635,966 (94.5) | 18,043 (3.8) | 451,810 (96.2) | ||||||
| Mean ± SD | 70.33 ± 0.29 | 72.85 ± 0.09 | 70.44 ± 0.34 | 73.01 ± 0.10 | ||||||
| Education level | ≤Elementary | 14,269 (3.1) | 445,740 (96.9) | 23.6 | <0.001 | 6869 (1.8) | 377,386 (98.2) | 42.01 | <0.001 | |
| ≥Middle school | 32,259 (5.5) | 553,152 (94.5) | 15,319 (4.3) | 341,592 (95.7) | ||||||
| Spouse | Yes | 36,669 (5.4) | 647,278 (94.6) | 25.15 | <0.001 | 16,282 (3.4) | 462,547 (96.6) | 8.1 | 0.042 | |
| No | 10,038 (2.8) | 352,825 (97.2) | 5906 (2.2) | 256,431 (97.8) | ||||||
| Daily Sleep times | ≤6 | 8557 (3.1) | 263,461 (96.9) | 10.15 | 0.007 | 4359 (2.3) | 188,479 (97.7) | 5.07 | 0.087 | |
| ≥7 | 38,256 (4.9) | 736,681 (95.1) | 17,829 (3.2) | 530,499 (96.8) | ||||||
| Low salt diet | Yes | 42,107 (4.2) | 955,268 (95.8) | 20.62 | <0.001 | 20,068 (2.8) | 693,444 (97.2) | 22.7 | <0.001 | |
| No | 4706 (9.5) | 44,875 (90.5) | 2120 (7.7) | 25,535 (92.3) | ||||||
| BMI | <18.5 | 1985 (5.7) | 32,614 (94.3) | 17.89 | 0.002 | 1365 (4.2) | 30,932 (95.8) | 2.85 | 0.463 | |
| 18.5~25.0 | 34,943 (5.1) | 644,808 (94.9) | 15,037 (3.1) | 468,665 (96.9) | ||||||
| ≥26.0 | 92,77 (2.9) | 309,895 (97.1) | 5559 (2.6) | 204,855 (97.4) | ||||||
| Diagnosed | Yes | 20,251 (3.9) | 501,278 (96.1) | 5.66 | 0.045 | 10,832 (2.9) | 364,251 (97.1) | 0.31 | 0.662 | |
| Hypertension | No | 26,562 (5.1) | 498,777 (94.9) | 11356 (3.1) | 354,727 (96.9) | |||||
| Subjective perceived health | Good | 15,312 (7.2) | 197,578 (92.8) | 49.6 | <0.001 | 8370 (5.3) | 149,941 (94.7) | 45.15 | <0.001 | |
| Moderate | 22,798 (4.8) | 450,888 (95.2) | 9037 (2.9) | 302,452 (97.1) | ||||||
| Bad | 8703 (2.4) | 351,677 (97.6) | 4781 (1.8) | 266,584 (98.2) | ||||||
| Limited daily activity | Yes | 37,571 (5.3) | 667,044 (94.7) | 25.1 | <0.001 | 18,507 (3.7) | 477,214 (96.3) | 29.64 | <0.001 | |
| No | 9241 (2.7) | 333,098 (97.3) | 3681 (1.5) | 241,764 (98.5) | ||||||
| Variables | Busan | Gyeongnam | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Yes (n = 306) | No | χ2 or t | p | Yes (n = 229) | No | χ2 or t | p | |||
| (n = 6724) | (n = 7562) | |||||||||
| n † (% ‡) or | n † (% ‡) or | n † (%‡) or | n † (% ‡) or | |||||||
| M ± SE ‡ | M ± SE ‡ | M ± SE ‡ | M ± SE ‡ | |||||||
| Interpersonal factor | Neighbors trust | Yes | 32,260 (4.4) | 70,6881 (95.6) | 0.47 | 0.579 | 15,324 (4.3) | 561,947 (95.7) | 11.9 | 0.016 |
| No | 12,965 (4.7) | 259,959 (95.3) | 6694 (2.7) | 149,411 (97.3) | ||||||
| Social network (neighbors) | Yes | 27,689 (4.1) | 648,062 (95.9) | 4.25 | 0.093 | 19,025 (3.2) | 567,373 (96.8) | 6.27 | 0.048 | |
| No | 19,123 (5.2) | 351,376 (94.8) | 3164 (2.0) | 150,977 (98.0) | ||||||
| Social network | Yes | 26,362 (4.1) | 617,196 (95.9) | 3.69 | 0.102 | 16,527 (3.4) | 463,034 (96.6) | 10 | 0.018 | |
| (friends) | No | 20,450 (5.1) | 382,946 (94.9) | 5662 (2.2) | 255,521 (97.8) | |||||
| Religious activity | Yes | 9181 (2.6) | 347,342 (97.4) | 30.56 | <0.001 | 2526 (1.4) | 172,011 (98.6) | 19.77 | <0.001 | |
| No | 37,632 (5.4) | 652,800 (94.6) | 19,663 (3.5) | 546,967 (96.5) | ||||||
| Socialize activity | Yes | 30,932 (4.9) | 601,825 (95.1) | 4.38 | 0.072 | 15,082 (3.7) | 397,076 (96.3) | 14.88 | 0.004 | |
| No | 15,880 (3.8) | 398,318 (96.2) | 7107 (2.7) | 321,902 (97.8) | ||||||
| Variables | Busan | Gyeongnam | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Yes (n = 306) | No | χ2 or t | p | Yes (n = 229) | No | χ2 or t | p | |||
| (n = 6724) | (n = 7562) | |||||||||
| n † (% ‡) or | n † (% ‡) or | n † (% ‡) or | n † (% ‡) or | |||||||
| M ± SE ‡ | M ± SE ‡ | M ± SE ‡ | M ± SE ‡ | |||||||
| Community factor | Satisfaction with life environment | Yes | 38,332 (7.3) | 889,976 (92.7) | 16.18 | 0.001 | 19,471 (2.9) | 647,835 (97.1) | 0.7 | 0.485 |
| No | 8389 (4.1) | 106,425 (95.9) | 2518 (3.5) | 70,279 (96.5) | ||||||
| Cancer screening | Yes | 29,932 (5.5) | 709,403 (94.5) | 7.13 | 0.025 | 15,724 (3.0) | 509,513 (97.0) | 0 | 0.983 | |
| No | 16,881 (4.0) | 290,347 (96.0) | 6464 (3.0) | 208,576 (97.0) | ||||||
| Vaccination | Yes | 36,776 (6.7) | 863,962 (93.3) | 14.08 | 0.001 | 16,881 (5.5) | 628,333 (94.5) | 25.88 | 0.001 | |
| No | 9841 (4.1) | 135,956 (95.9) | 5307 (2.6) | 90,376 (97.4) | ||||||
| Unmet medical needs | Yes | 2693 (5.4) | 47,096 (94.6) | 0.72 | 0.556 | 21,423 (3.1) | 669,862 (96.9) | 4.12 | 0.036 | |
| No | 44,119 (4.4) | 953,046 (95.6) | 766 (1.5) | 49,116 (98.5) | ||||||
| Falling accident | Yes | 4800 (3.1) | 151,182 (96.9) | 5.6 | 0.047 | 2897 (2.4) | 117,182 (97.6) | 1.75 | 0.365 | |
| No | 42,012 (4.7) | 848,960 (95.3) | 19,291 (3.1) | 601,796 (96.9) | ||||||
| Variables | Busan | Gyeongnam | ||||||
|---|---|---|---|---|---|---|---|---|
| (n = 7030) | (n = 7229) | |||||||
| OR | 95% CI | p | OR | 95% CI | p | |||
| Personal factor | Gender | Male | 0.06 | 0.03–0.09 | <0.001 | 0.06 | 0.03–0.12 | <0.001 |
| Female | 1 | 1 | ||||||
| Age | ≥75 | 0.44 | 1.31–1.61 | <0.001 | 0.32 | 0.19–0.53 | <0.001 | |
| 65–74 | 1 | 1 | ||||||
| Education level | ≤Elementary | 0.82 | 0.60–1.14 | 0.243 | 0.91 | 0.63–1.34 | 0.644 | |
| ≥Middle school | 1 | 1 | ||||||
| Spouse | Yes | 1.26 | 0.88–1.80 | 0.206 | 1.94 | 1.26–2.99 | 0.003 | |
| No | 1 | 1 | ||||||
| Daily sleep times | ≤6 | 1.18 | 0.82–1.71 | 0.37 | 1.19 | 0.75–1.88 | 0.469 | |
| (per week) | ≥7 | 1 | 1 | |||||
| Low salt diet | Yes | 1.82 | 1.16–2.86 | 0.01 | 2.3 | 1.15–4.62 | 0.019 | |
| No | 1 | 1 | ||||||
| Weight control (BMI) | <18.5 | 0.56 | 0.27–1.17 | 0.122 | 0.5 | 0.21–1.17 | 0.11 | |
| 18.5~25.0 | 0.62 | 0.43–0.91 | 0.014 | 0.89 | 0.53–1.50 | 0.665 | ||
| ≥26.0 | 1 | 1 | ||||||
| Diagnosed | Yes | 1.05 | 0.78–1.41 | 0.748 | 0.76 | 0.51–1.13 | 0.171 | |
| Hypertension | No | 1 | 1 | |||||
| Subjective perceived health | Good | 0.39 | 0.25–0.62 | <0.001 | 0.41 | 0.24–0.69 | 0.001 | |
| Moderate | 0.57 | 0.37–0.88 | 0.012 | 0.63 | 0.38–1.04 | 0.07 | ||
| Bad | 1 | 1 | ||||||
| Limited of daily activity | Yes | 0.95 | 0.59–1.52 | 0.827 | 0.8 | 0.50–1.28 | 0.353 | |
| No | 1 | 1 | ||||||
| Variables | Busan | Gyeongnam | ||||||
|---|---|---|---|---|---|---|---|---|
| (n = 7030) | (n = 7229) | |||||||
| OR | 95% CI | p | OR | 95% CI | p | |||
| Interpersonal factors | Neighbors trust | Yes | 0.94 | 0.65–1.36 | 0.729 | 2.73 | 1.81–4.12 | <0.001 |
| No | 1 | 1 | ||||||
| Social network (neighbors) | Yes | 1.17 | 0.85–1.61 | 0.332 | 0.54 | 0.32–0.91 | 0.021 | |
| No | 1 | 1 | ||||||
| Social network (friends) | Yes | 1.22 | 0.90–1.64 | 0.202 | 0.71 | 0.48–1.06 | 0.092 | |
| No | 1 | 1 | ||||||
| Religious activity | Yes | 2.06 | 1.44–2.93 | <0.001 | 2.53 | 1.58–4.06 | <0.001 | |
| No | 1 | 1 | ||||||
| Socialize activity | Yes | 0.64 | 0.47–0.88 | 0.006 | 0.6 | 0.41–0.88 | 0.01 | |
| No | 1 | 1 | ||||||
| Variables | Busan (n = 7030) | Gyeongnam (n = 7229) | ||||||
|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | |||
| Community factors | Satisfaction with life environment | Yes | 1.72 | 1.14–2.59 | 0.009 | 1.22 | 0.70–2.12 | 0.493 |
| No | 1 | 1 | ||||||
| Cancer screening | Yes | 1.3 | 0.89–1.90 | 0.175 | 1.06 | 0.59–1.93 | 0.837 | |
| No | 1 | 1 | ||||||
| Health screening | Yes | 0.98 | 0.65–1.49 | 0.931 | 0.81 | 0.41–1.62 | 0.555 | |
| No | 1 | 1 | ||||||
| Vaccination | Yes | 1.59 | 1.13–2.23 | 0.008 | 2.46 | 1.50–4.04 | <0.001 | |
| No | 1 | 1 | ||||||
| Unmet medical needs | Yes | 0.92 | 0.45–1.87 | 0.811 | 2 | 1.00–4.01 | 0.05 | |
| No | 1 | 1 | ||||||
| Falling accident | Yes | 1.61 | 1.02–2.53 | 0.039 | 1.24 | 0.71–2.18 | 0.445 | |
| No | 1 | 1 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, E.; Choo, I.; Noh, Y. Factors Influencing the Practice of Healthy Living as an Integrated Indicator of the Elderly’s Drinking, Smoking, and Walking Patterns: Using Korea Community Health Surveys. Int. J. Environ. Res. Public Health 2022, 19, 1936. https://doi.org/10.3390/ijerph19041936
Kim E, Choo I, Noh Y. Factors Influencing the Practice of Healthy Living as an Integrated Indicator of the Elderly’s Drinking, Smoking, and Walking Patterns: Using Korea Community Health Surveys. International Journal of Environmental Research and Public Health. 2022; 19(4):1936. https://doi.org/10.3390/ijerph19041936
Chicago/Turabian StyleKim, Eunha, Inhee Choo, and Yunhwan Noh. 2022. "Factors Influencing the Practice of Healthy Living as an Integrated Indicator of the Elderly’s Drinking, Smoking, and Walking Patterns: Using Korea Community Health Surveys" International Journal of Environmental Research and Public Health 19, no. 4: 1936. https://doi.org/10.3390/ijerph19041936