
Effectiveness of Health Information Package Program on Knowledge and Compliance among Pregnant Women with Anemia: A Randomized Controlled Trial


Abstract
:1. Introduction
2. Materials and Methods
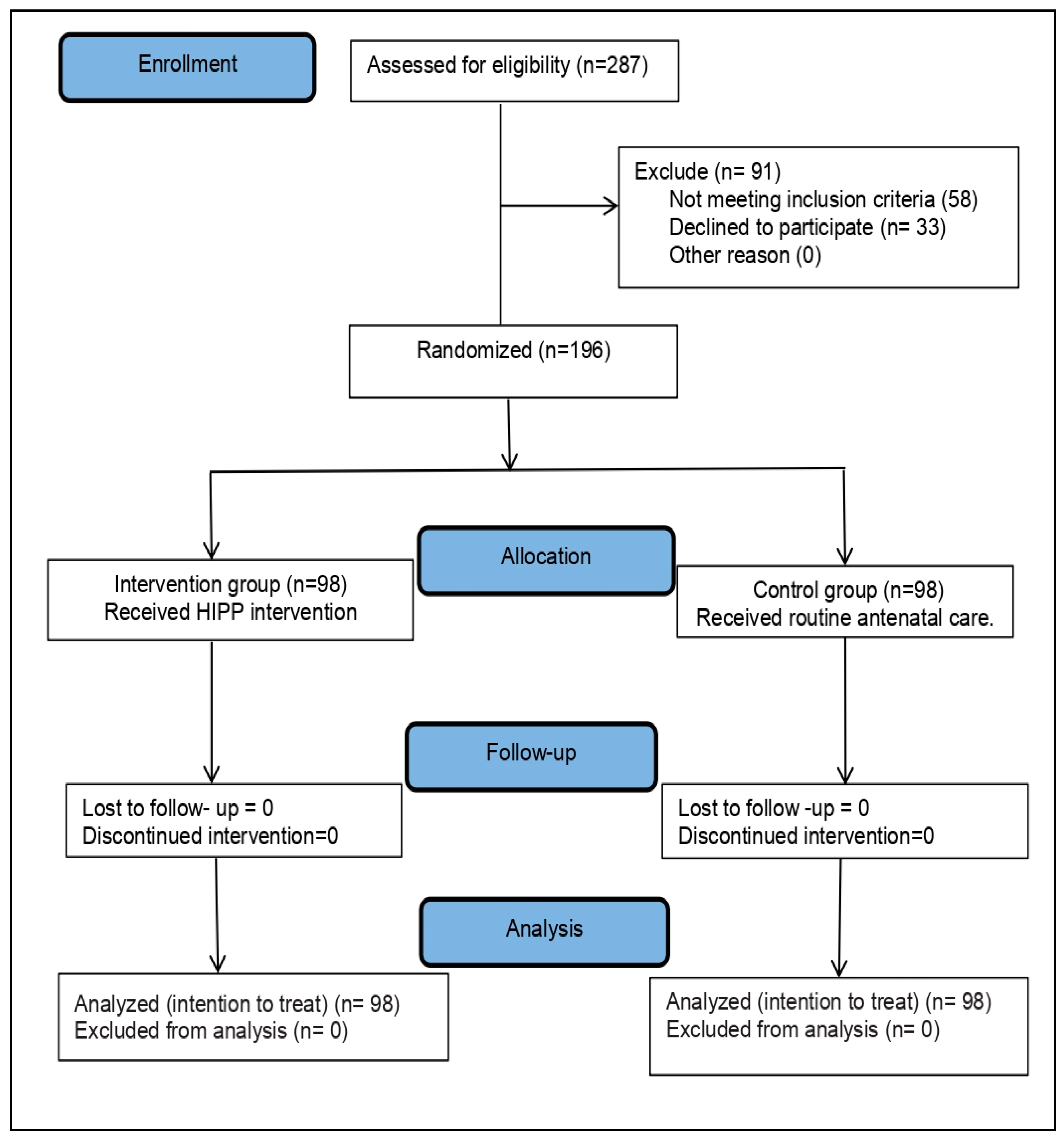
2.1. Design and Participants
2.2. Instruments
2.2.1. Socio-Demographic and Health-Related Information
2.2.2. Structured Knowledge Interview Schedule (SKIS)
2.2.3. The Food Selection Ability Checklist
2.2.4. Compliance with IFA Supplementation
2.3. Intervention
2.4. Data Collection
2.5. Statistical Analysis
2.6. Ethical Consideration
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Anemia Reduction Efforts among Women of Reproductive Age: Impact, Achievement of Targets, and the Way Forward for Optimizing Efforts; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/publications/i/item/9789240012202 (accessed on 17 June 2021).
- Al-Jawaldeh, A.; Taktouk, M.; Doggui, R.; Abdollahi, Z.; Achakzai, B.; Aguenaou, H.; Al-Halaika, M.; Almamary, S.; Barham, R.; Coulibaly-Zerbo, F.; et al. Are Countries of the Eastern Mediterranean Region on Track towards Meeting the World Health Assembly Target for Anemia? A Review of Evidence. Int. J. Environ. Res. Public Health 2021, 18, 2449. [Google Scholar] [CrossRef]
- Owais, A.; Merritt, C.; Lee, C.; Bhutta, Z.A. Anemia among Women of Reproductive Age: An Overview of Global Burden, Trends, Determinants, and Drivers of Progress in Low- and Middle-Income Countries. Nutrients 2021, 13, 2745. [Google Scholar] [CrossRef]
- Lebso, M.; Anato, A.; Loha, E. Prevalence of anemia and associated factors among pregnant women in Southern Ethiopia: A community based cross-sectional study. PLoS ONE 2017, 12, e0188783. [Google Scholar] [CrossRef] [PubMed]
- Nahrisah, P.; Somrongthong, R.; Viriyautsahakul, N.; Viwattanakulvanid, P.; Plianbangchang, S. Effect of Integrated Pictorial Handbook Education and Counseling on Improving Anemia Status, Knowledge, Food Intake, and Iron Tablet Compliance among Anemic Pregnant Women in Indonesia: A Quasi-Experimental Study. J. Multidiscip. Healthc. 2020, 13, 43–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Health Observatory Data Repository. In Prevalence of Anemia in Women: Estimates by Country; World Health Organization: Geneva, Switzerland, 2016; Available online: https://apps.who.int/gho/data/view.main.GSWCAH28v (accessed on 17 June 2021).
- Hwalla, N.; Al Dhaheri, A.S.; Radwan, H.; Alfawaz, H.A.; Fouda, M.A.; Al-Daghri, N.M.; Zaghloul, S.; Blumberg, J.B. The Prevalence of Micronutrient Deficiencies and Inadequacies in the Middle East and Approaches to Interventions. Nutrients 2017, 9, 229. [Google Scholar] [CrossRef]
- World Health Survey-Saudi Arabia (KSAWHS), Final Report. Ministry of Health. 2019. Available online: https://www.moh.gov.sa/en/Ministry/Statistics/Population-Health-Indicators/Documents/World-Health-Survey-Saudi-Arabia.pdf (accessed on 17 June 2021).
- Georgieff, M.K. Iron deficiency in pregnancy. Am. J. Obstet. Gynecol. 2020, 223, 516–524. [Google Scholar] [CrossRef]
- Juul, S.E.; Derman, R.J.; Auerbach, M. Perinatal Iron Deficiency: Implications for Mothers and Infants. Neonatology 2019, 115, 269–274. [Google Scholar] [CrossRef]
- Derso, T.; Abera, Z.; Tariku, A. Magnitude and associated factors of anemia among pregnant women in Dera District: A cross-sectional study in northwest Ethiopia. BMC Res. Notes 2017, 10, 359. [Google Scholar] [CrossRef]
- Arab, H.; Gari, A.; Almomen, A.; Elawad, M.; Obaid, M.B.; Ghamdi, M.A.; Bondagji, N.S.; Kurdi, W. Practical Guidance on Managing Iron Deficiency in Women of Childbearing Age–A Saudi Arabian Expert Consensus. Med. J. Obstet. Gynecol. 2019, 7, 1127. [Google Scholar]
- Annan, R.A.; Gyimah, L.A.; Apprey, C.; Edusei, A.K.; Asamoah-Boakye, O.; Aduku, L.; Azanu, W.; Lutterodt, H.E. Factors associated with iron deficiency anaemia among pregnant teenagers in Ashanti Region, Ghana: A hospital-based prospective cohort study. PLoS ONE 2021, 16, e0250246. [Google Scholar] [CrossRef]
- Tuncalp, Ö.; Rogers, L.M.; Lawrie, T.A.; Barreix, M.; Peña-Rosas, J.P.; Bucagu, M.; Neilson, J.; Oladapo, O.T. WHO recommendations on antenatal nutrition: An update on multiple micronutrient supplements. BMJ Glob. Health 2020, 5, e003375. [Google Scholar] [CrossRef] [PubMed]
- Peña-Rosas, J.P.; De-Regil, L.M.; Garcia-Casal, M.N.; Dowswell, T.; Viteri, F.E. Daily oral iron supplementation during pregnancy. Cochrane Database Syst. Rev. 2015, 7, CD004736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abraha, I.; Bonacini, M.I.; Montedori, A.; Di Renzo, G.C.; Angelozzi, P.; Micheli, M.; Germani, A.; Carloni, D.; Scaccetti, A.; Palmieri, G.; et al. Oral iron-based interventions for prevention of critical outcomes in pregnancy and postnatal care: An overview and update of systematic reviews. J. Evid.-Based Med. 2019, 12, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Siabani, S.; Siabani, S.; Siabani, H.; Moeini Arya, M.; Rezaei, F.; Babakhani, M. Determinants of Compliance with Iron and Folate Supplementation among Pregnant Women in West Iran: A Population Based Cross-Sectional Study. J. Fam. Reprod. Health 2018, 12, 197–203. [Google Scholar]
- Ugwu, E.O.; Olibe, A.O.; Obi, S.N.; Ugwu, A.O. Determinants of compliance to iron supplementation among pregnant women in Enugu, Southeastern Nigeria. Niger. J. Clin. Pract. 2014, 17, 608–612. [Google Scholar] [CrossRef] [Green Version]
- Khorshid, M.R.; Afshari, P.; Abedi, P. The effect of SMS messaging on the compliance with iron supplementation among pregnant women in Iran: A randomized controlled trial. J. Telemed. Telecare 2014, 20, 201–206. [Google Scholar] [CrossRef]
- Sendeku, F.W.; Azeze, G.G.; Fenta, S.L. Adherence to iron-folic acid supplementation among pregnant women in Ethiopia: A systematic review and meta- analysis. BMC Pregnancy Childbirth 2020, 20, 138. [Google Scholar] [CrossRef]
- Al Bahhawi, T.; Doweri, A.A.; Sawadi, R.M.; Awaji, M.Y.; Jarad, M.M.; Sulays, Z.Y.; Madkor, K.A. Consumption habits of pregnant women in the Jazan region, Saudi Arabia: A descriptive study. BMC Res. Notes 2018, 11, 817. [Google Scholar] [CrossRef] [Green Version]
- Noronha, J.A.; Bhaduri, A.; Bhat, H.V.; Kamath, A. Interventional study to strengthen the health promoting behaviours of pregnant women to prevent anaemia in southern India. Midwifery 2013, 29, e35–e41. [Google Scholar] [CrossRef]
- Abujilban, S.; Hatamleh, R.; Al- Shuqerat, S. The impact of a planned health educational program on the compliance and knowledge of Jordanian pregnant women with anemia. Women Health 2019, 59, 748–759. [Google Scholar] [CrossRef]
- Habib, F.; Alabdin, E.H.Z.; Alenazy, M.; Nooh, R. Compliance to iron supplementation during pregnancy. J. Obstet. Gynaecol. 2009, 29, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: New York, NY, USA, 1977; pp. 1–14. ISBN 0-8058-0283-5. [Google Scholar]
- Hasneezah, H.; Rosliza, A.M.; Salmiah, M.S.; Appanah, G. The effectiveness of theory-based intervention to improve haemoglobin levels among women with anaemia in pregnancy. Med. J. Malays. 2020, 75, 626–634. [Google Scholar]
- Sunuwar, D.R.; Sangroula, R.K.; Shakya, N.S.; Yadav, R.; Chaudhary, N.K.; Pradhan, P. Effect of nutrition education on Hb level in pregnant women: A quasi-experimental study. PLoS ONE 2019, 14, e0213982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seshan, V.; Alkhasawneh, E.; Al Kindi, S.; Al Simadi, F.A.; Arulappan, J. Can Gestational Anemia be alleviated with Increased Awareness of its Causes and Management Strategies? Implications for Health Care Services. Oman Med. J. 2018, 33, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Widyawati, W.; Jans, S.; Bor, H.H.; van Dillen, J.; Lagro-Janssen, A.L. The Effectiveness of a New Model in Managing Pregnant Women with Iron Deficiency Anemia in Indonesia: A Nonrandomized Controlled Intervention Study. Birth 2015, 42, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Alfawaz, H.A.; Khan, N.; AlOteabi, N.; Hussain, S.D.; Al-Daghri, N.M. Factors associated with dietary supplement use in Saudi pregnant women. Reprod. Health 2017, 14, 104. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health (MOH); Saudi Arabia. MOH Portal, Awareness Platform, Women’s Health during Pregnancy. 2021. Available online: https://www.moh.gov.sa/en/awarenessplateform/WomensHealth/Pages/DuringPregnancy.aspx (accessed on 17 June 2021).
- Yamashita, T.; Roces, R.; Ladines-Llave, C.; Reyes Tuliao, M.T.; Wanjira Kamau, M.; Yamada, C.; Tanaka, Y.; Shimazawa, K.; Iwamoto, S.; Matsuo, H. Maternal Knowledge Associated with the Prevalence of Iron and Folic Acid Supplementation among Pregnant Women in Muntinlupa, Philippines: A Cross-Sectional Study. Patient Prefer. Adherence 2021, 15, 501–510. [Google Scholar] [CrossRef]
- Workineh, Y.; Semachew, A.; Ayalew, E.; Temesgen, W.A. Compliance to Iron-Folic Acid Supplementation and Its Association with the Number of ANC Visits in Ethiopia: Systematic Review and Meta-Analysis. Adv. Prev. Med. 2019, 2019, 3602585. [Google Scholar] [CrossRef] [Green Version]
- Assefa, H.; Abebe, S.M.; Sisay, M. Magnitude and factors associated with adherence to Iron and folic acid supplementation among pregnant women in Aykel town, Northwest Ethiopia. BMC Pregnancy Childbirth 2019, 19, 296. [Google Scholar] [CrossRef]


{kind=link}
| Socio-Demographics | Total (n = 196) | Intervention (n = 98) | Control (n = 98) | Test of Sig. | p | |||
|---|---|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | |||
| Age (Years) | ||||||||
| <25 | 98 | 50.0 | 45 | 45.9 | 53 | 54.1 | χ2 = 1.777 | 0.411 |
| 25–34 | 75 | 38.3 | 42 | 42.9 | 33 | 33.7 | ||
| 35–45 | 23 | 11.7 | 11 | 11.2 | 12 | 12.2 | ||
| Mean ± SD | 25.93 ± 5.30 | 25.76 ± 5.42 | 26.10 ± 5.19 | |||||
| Educational Level | ||||||||
| Primary | 40 | 20.4 | 21 | 21.4 | 19 | 19.4 | χ2 = 1.081 | 0.582 |
| Intermediate and Secondary | 47 | 24.0 | 26 | 26.5 | 21 | 21.4 | ||
| University and Postgraduates | 109 | 55.6 | 51 | 52.0 | 58 | 59.2 | ||
| Occupation | ||||||||
| Housewife | 99 | 50.5 | 54 | 55.1 | 45 | 45.9 | χ2 = 1.670 | 0.434 |
| Working | 47 | 24.0 | 21 | 21.4 | 26 | 26.5 | ||
| Students | 50 | 25.5 | 23 | 23.5 | 27 | 27.6 | ||
| Family Monthly Income | ||||||||
| Poor: <SAR 5000 (<EUR 1170) | 10 | 5.1 | 7 | 7.1 | 3 | 3.1 | χ2 = 4.583 | 0.101 |
| Average: SAR 5000 < SAR 1000 (EUR 1170 < EUR 2340) | 128 | 65.8 | 68 | 69.4 | 60 | 61.2 | ||
| Good: ≥SAR 1000 (≥EUR 2340) | 58 | 29.6 | 23 | 23.5 | 35 | 35.7 | ||
| Parity | χ2 = 1.074 | 0.783 | ||||||
| Nullipara | 74 | 37.8 | 40 | 40.8 | 34 | 34.7 | ||
| Primipara | 74 | 37.8 | 36 | 36.7 | 38 | 38.8 | ||
| Multipara | 30 | 15.3 | 13 | 13.3 | 17 | 17.3 | ||
| Grand Multipara | 18 | 9.2 | 9 | 9.2 | 9 | 9.2 | ||
| Pregnancy Intervals | χ2 = 0.330 | |||||||
| Short: <2 years | 108 | 55.1 | 56 | 57.1 | 52 | 53.1 | 0.566 | |
| Adequate: ≥2 years | 88 | 44.9 | 42 | 42.9 | 46 | 46.9 | ||
| Antenatal Follow-up | 146 | 74.5 | 76 | 77.6 | 70 | 71.4 | χ2 = 0.967 | 0.326 |
| Variable | Outcome | Pretest | Posttest | Mean Difference | Z | p | Effect Size Eta | Level |
|---|---|---|---|---|---|---|---|---|
| Mean (SD.) | Mean (SD.) | |||||||
| Knowledge (0–71) | Intervention | 25.14 ± 10.13 | 54.33 ± 10.92 | 29.18 | 8.201 * | <0.001* | 0.773 | Intermediate |
| Control | 23.55 ± 8.15 | 24.79 ± 10.19 | 1.23 | 0.527 | 0.598 | 0.012 | No effect | |
| U (p0) | 4217.0 (0.070) | 441.5 * (<0.001 *) | ||||||
| Food Selection Ability (0–53) | Intervention | 13.41 ± 3.99 | 21.80 ± 5.81 | 8.39 | 7.874 * | <0.001 * | 0.617 | Intermediate |
| Control | 12.67 ± 2.35 | 13.02 ± 2.90 | 0.35 | 1.298 | 0.194 | 0.019 | No effect | |
| U (p0) | 4626.500 (0.410) | 677.0 * (<0.001 *) | ||||||
| Hb Level | Intervention | 9.96 ± 0.30 | 11.16 ± 0.50 | 1.20 | 8.620 * | <0.001 * | 0.850 | Large |
| Control | 9.99 ± 0.32 | 10.01 ± 0.37 | 0.02 | 1.841 | 0.066 | 0.037 | No effect | |
| U (p0) | 4593.500 ≥ (0.584) | 245.50 * (<0.001 *) |
| Compliance | Intervention (n = 98) | Control (n = 98) | Test of Sig. | p | ||
|---|---|---|---|---|---|---|
| No. | % | No. | % | |||
| Poor < 45 (<50%) | 2 | 2.1 | 17 | 17.3 | χ2 = 19.104 | <0.001 * |
| Partial 45–67 (50–74) | 7 | 7.1 | 16 | 16.3 | ||
| High 68–90 (≥75–100%) | 89 | 90.8 | 65 | 66.4 | ||
| Number of IFA Tablets Taken, Mean ± SD. | 82.31 ± 8.71 | 66.78 ± 13.82 | U = 1366.0 * | <0.001 * | ||
| Parameter | Univariate | # Multivariate | ||
|---|---|---|---|---|
| p | B (95% C.I) | p | B (95% C.I) | |
| Age (Years) | 0.048 * | −0.371 (−0.739–−0.003) | 0.880 | −0.026 (−0.365–0.313) |
| Educational Level | <0.001 * | 6.148 (3.844–8.451) | 0.001 * | 4.631 (2.018–7.244) |
| Family Monthly Income | 0.349 | 1.743 (−1.915–5.401) | ||
| Parity | 0.003 * | −2.991 (−4.963–−1.019) | 0.893 | 0.317 (−4.325–4.959) |
| Pregnancy Interval | 0.494 | 1.370 (−2.575–5.314) | ||
| Antenatal Follow-up | 0.009 * | −5.935 (−10.361–−1.508) | 0.906 | 0.293 (−4.577–5.164) |
| Knowledge | <0.001 * | 0.319 (0.257–0.381) | 0.069 | 0.106 (−0.008–0.220) |
| Food Selection Ability | <0.001 * | 0.639 (0.503–0.776) | 0.594 | 0.059 (−0.277–0.159) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elsharkawy, N.B.; Abdelaziz, E.M.; Ouda, M.M.; Oraby, F.A. Effectiveness of Health Information Package Program on Knowledge and Compliance among Pregnant Women with Anemia: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 2724. https://doi.org/10.3390/ijerph19052724
Elsharkawy NB, Abdelaziz EM, Ouda MM, Oraby FA. Effectiveness of Health Information Package Program on Knowledge and Compliance among Pregnant Women with Anemia: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(5):2724. https://doi.org/10.3390/ijerph19052724
Chicago/Turabian StyleElsharkawy, Nadia B., Enas M. Abdelaziz, Marwa M. Ouda, and Fatma A. Oraby. 2022. "Effectiveness of Health Information Package Program on Knowledge and Compliance among Pregnant Women with Anemia: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 5: 2724. https://doi.org/10.3390/ijerph19052724