
“No One Manages It; We Just Sign Them Up and Do It”: A Whole System Analysis of Access to Healthcare in One Remote Australian Community

 , , , ,
, , , , 
Abstract
:1. Introduction
1.1. Health System and Services: Funding, Service Delivery and Management
1.2. Health Inequality: Aboriginal and Torres Strait Islander People
1.3. Rural and Remote Health
1.4. Importance of Culturally Safe Care
1.5. Justification of Study
2. Methods
3. Results
- There are examples of both underservicing and overservicing which give insight into systemic barriers in interagency cooperation;
- Nurses, community health workers, Aboriginal health workers, teachers, and administration staff have an invaluable role in healthcare and improving patient access to health services and could be better supported through further funding and opportunities for specialised training;
- Visiting and telehealth services are critical components of the system that must be linked to existing community led primary care services.
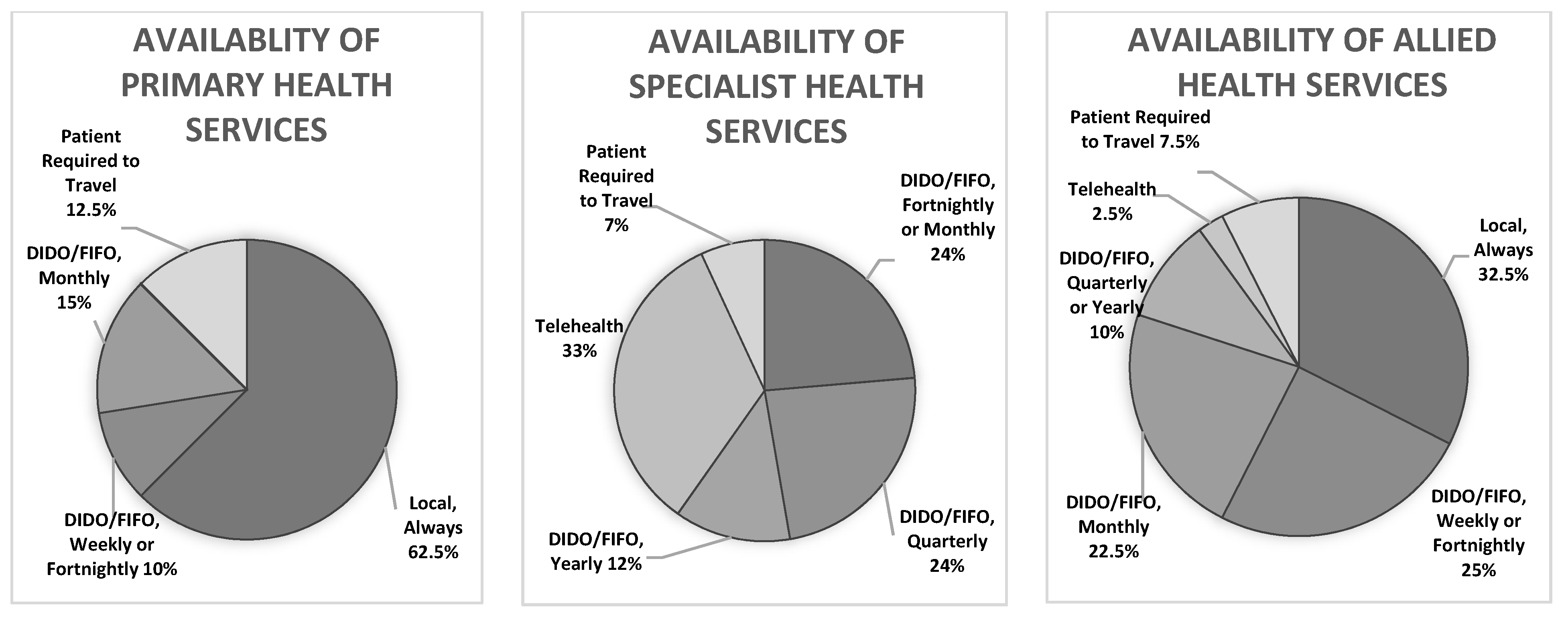
3.1. Service Availability
“He didn’t know he had diabetes… he nearly died; when he got to the doctor in [regional centre] he said ‘I don’t even know how you’re standing’… maybe need some sort of education for people who have been diagnosed cos he didn’t know anything about it”—School Staff, A
“We have a weekly interagency meeting where we talk about complex clients”—Health Service Manager, A
“There is a lack of integration of what [services] we’ve already got, no one is allowed to lead [interagency cooperation] … it’s not always in their interest to collaborate”—Health Service Manager, A
“There is a bit of a doubling up… someone decides we need one of these things–but don’t worry if its already somewhere else… so everyone’s sort of struggling to maintain their numbers”—Health Service Manager, B
“There’s a doubling up of counselling… we don’t communicate particularly, to know which day they’re there [another local health service] and which day they’re here. And I think it’d be really good if both those people could get together and … [organise days to come, coordinate care for shared patients]”—Health Service Manager, B
“Nurses go to the [other] school at least once a week… but they don’t do that for us”—School Staff, B
3.2. Reliance on Nurses, Aboriginal Health Workers, Community Health Workers, Teachers and Administration Staff
“I rely heavily on my Aboriginal education workers, because they’re the ones that put the foot in the door to build that relationship with the parents… and then those families don’t feel like they’re being judged or like they’ll be reported to [social services]”—School Staff, B
“As part of their employment, [nurses] have to do dialysis training, because you can’t meet the demands of the roster… Nurses have to do the First Line Emergency Care Course, they have to do first emergency care, they’re pretty highly trained because… we have so many varied things coming through the door”—Health Service Manager, A
“No one manages [Closing the Gap initiatives]; we just sign them up and do it”—Administration Staff
“If [Hospital in city] want to do a video conference, it’s done here at school. We sit in with them [the parents/carers], so we know what’s being said, because sometimes they use language that the parents don’t fully understand, then after the session… I explain what that actually means. And then in some cases we will implement programs at the school to help the parents”—School Staff, C
3.3. DIDO, FIFO and Telehealth
“I don’t know what the solution is, we just need to have services when they’re required”—School Staff, C
“I think as a town we have a lot of services that come here. If you’re in the city there are some of these people [specialists] you can’t get into for months and months. I’ve seen people here wanting to see the ENT walking straight in to see the ENT. That doesn’t happen anywhere else”—ACCHO staff
“[Telehealth], it’s the way to go, they’re putting so much money into it and the Chief Executive is so into it… with mental health [risk assessment support] it’s fantastic… [but it] isn’t happening properly yet…it’s not well coordinated and they’re not doing any consultation, but the technology is there”—Health Service Manager, B
4. Discussion
4.1. Service Availability
4.2. Reliance on Nurses, Community Health Workers, Teachers and Admin Staff
4.3. DIDO, FIFO and Telehealth
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Australian Institute of Health and Welfare. Australia’s Health 2020; Australian Institute of Health and Welfare: Canberra, Austrilia, 2020. Available online: https://www.aihw.gov.au/reports-data/australias-health (accessed on 20 October 2021).
- Healy, J.; Sharman, E.; Lokuge, B. Australia: Health System Review, Health Systems in Transition; World Health Organisation: Copenhagen, Denmark, 2006; Volume 8. [Google Scholar]
- Australian Institute of Health and Welfare. Health Expenditure Australia 2016–2017; Cat No.: HWE 74; Australian Government: Canberra, Austrilia, 2018.
- Pearson, O.; Schwartzkopff, K.; Dawson, A.; Hagger, C.; Karagi, A.; Davy, C.; Brown, A.; Braunack-Mayer, A. Aboriginal community controlled health organisations address health equity through action on the social determinants of health of Aboriginal and Torres Strait Islander peoples in Australia. BMC Public Health 2020, 20, 1859. [Google Scholar] [CrossRef] [PubMed]
- Campbell, M.A.; Hunt, J.; Scrimgeour, D.J.; Davey, M.; Jones, V. Contribution of Aboriginal Community-Controlled Health Services to improving Aboriginal health: An evidence review. Aust Health Rev. 2018, 42, 218–226. [Google Scholar] [CrossRef] [PubMed]
- National Indigenous Australians Agency. Infant and Child Mortality; Australian Institute of Health and Welfare: Canberra, Austrilia, 2020. Available online: https://www.indigenoushpf.gov.au/measures/1-20-infant-child-mortality (accessed on 14 June 2021).
- Australian Institute of Health and Welfare. Indigenous Health and Wellbeing; Australian Institute of Health and Welfare: Canberra, Austrilia, 2020. Available online: https://www.aihw.gov.au/reports/australias-health/indigenous-health-and-wellbeing (accessed on 14 June 2021).
- Australian Institute of Health and Welfare. Maternal Deaths in Australia; Australian Institute of Health and Welfare: Canberra, Austrilia, 2021. Available online: https://www.aihw.gov.au/reports/mothers-babies/maternal-deaths-in-australia (accessed on 14 June 2021).
- Gardiner-Garden, J. Closing the Gap; Parliament of Australia: Canberra, Australia, 2012. Available online: https://www.aph.gov.au/About_Parliament/Parliamentary_Departments/Parliamentary_Library/pubs/BriefingBook44p/ClosingGap (accessed on 14 June 2021).
- The Lowitja Institute. Close the Gap; The Close the Gap Campaign Steering Committee: Hawthorn, Australia, 2020; Available online: https://www.lowitja.org.au/content/Document/CtG2020_FINAL4_WEB%20(1).pdf (accessed on 20 October 2021).
- Australian Government. Closing the Gap in Partnership. In National Agreement on Closing the Gap; Australian Government: Canberra, Australia, 2020. [Google Scholar]
- Australian Institute of Health and Welfare. Rural & Remote Health; Cat No.: PHE 255; Australian Institute of Health and Welfare: Canberra, Australia, 2019. Available online: https://www.aihw.gov.au/getmedia/838d92d0-6d34-4821-b5da-39e4a47a3d80/Rural-remote-health.pdf.aspx?inline=true (accessed on 15 June 2021).
- Thomas, S.; Wakerman, J.; Humphreys, J. Ensuring equity of access to primary health care in rural and remote Australia—what core services should be locally available? Int. J. Equity Health 2015, 14, 111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- COAG Reform Council. Healthcare 2011–2012: Comparing Performance across Australia; COAG Reform Council: Canberra, Austrilia, 2013. Available online: https://www.ruralhealth.org.au/sites/default/files/documents/nrha-policy-document/policy-development/dev-coag-healthcare-2011-12-nrha-21-june-13.pdf (accessed on 20 October 2021).
- Smith, K.; Humphreys, J.; Wilson, M. Addressing the health disadvantage of rural populations: How does epidemiological evidence inform rural health policies and research? Aust. J. Rural Health 2008, 16, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. The Health and Welfare of Australia’s Aboriginal and Torres Strait Islander peoples 2015; Cat No.: IHW 147; Australian Institute of Health and Welfare: Canberra, Australia, 2015. Available online: https://www.aihw.gov.au/getmedia/584073f7-041e-4818-9419-39f5a060b1aa/18175.pdf.aspx?inline=true (accessed on 20 October 2021).
- Shahid, S.; Teng, T.; Bessarab, D.; Aoun, S.; Baxi, S.; Thompson, S. Factors contributing to delayed diagnosis of cancer among Aboriginal people in Australia: A qualitative study. BMJ Open 2016, 6, e010909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jennings, W.A.; Bond, C.C.; Hill, D.P.S. The power of talk and power in talk: A systematic review of Indigenous narratives of culturally safe healthcare communication. Aust. J. Prim. Health 2018, 24, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Ware, V.A. Improving the Accessibility of Health Services in Urban and Regional Settings for Indigenous People; Australian Institute of Health and Welfare: Canberra, Austrilia, 2013.
- Scott, J.; Scott, R.; Miller, W.; Stange, K.; Crabtree, B. Healing relationships and the existential philosophy of Martin Buber. Philos. Ethics. Humanit. Med. 2009, 4, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nolan-Isles, D.; Macniven, R.; Hunter, K.; Gwynn, J.; Lincoln, M.; Moir, R.; Dimitropoulos, Y.; Taylor, D.; Agius, T.; Finlayson, H.; et al. Enablers and Barriers to Accessing Healthcare Services for Aboriginal People in New South Wales, Australia. Int. J. Environ. Res. Public Health 2021, 18, 3014. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.; Dwyer, J.; Willis, E.; Pekarsky, B. Travelling to the city for hospital care: Access factors in country Aboriginal patient journeys. Aust. J. Rural Health 2014, 22, 109–113. [Google Scholar] [CrossRef]
- Macniven, R.; Hunter, K.; Lincoln, M.; O’Brien, C.; Jeffries, T.L., Jr.; Shein, G.; Saxby, A.; Taylor, D.; Agius, T.; Finlayson, H.; et al. Accessibility of Primary, Specialist, and Allied Health Services for Aboriginal People Living in Rural and Remote Communities: Protocol for a Mixed-Methods Study. JMIR Res. Protoc. 2019, 8, e11471. [Google Scholar] [CrossRef]
- Thomas, D.R. A General Inductive Approach for Analyzing Qualitative Evaluation Data. Am. J. Eval. 2006, 27, 237–246. [Google Scholar] [CrossRef]
- Australian Indigenous Health Info Net. Healthy for Life; Australian Indigenous Health Info Net: Perth, Austrilia, 2021; Available online: https://healthinfonet.ecu.edu.au/key-resources/programs-and-projects/?id=4 (accessed on 14 June 2021).
- Alcohol and Other Drugs Knowledge Centre. Blue Mountains Aboriginal Healthy For Life Program; Australian Indigenous Health Info Net: Perth, Austrilia, 2013. Available online: https://aodknowledgecentre.ecu.edu.au/key-resources/programs-and-projects/1297/?title=Blue%20Mountains%20Aboriginal%20Healthy%20For%20Life%20Program (accessed on 14 June 2021).
- Umoona Tjutagku Health Service. Healthy for Life; Umoona Tjutagku Health Service: Coober Pedy, Austrilia, 2021; Available online: https://www.uths.com.au/department-15-healthy-for-life.html (accessed on 14 June 2021).
- NSW Department of Education and Communities. Connected Communities Strategy; NSW Government: Sydney, Austrilia, 2011.
- Gwynne, K.; Lincoln, M. Developing the rural health workforce to improve Australian Aboriginal and Torres Strait Islander health outcomes: A systematic review. Aust. Health Rev. 2017, 41, 234–238. [Google Scholar] [CrossRef] [PubMed]
- Deroy, S.; Schütze, H. Factors supporting retention of health and wellbeing staff in Aboriginal health services: A strength-based case study. Hum. Resour. Health. 2021, 19, 35. [Google Scholar] [CrossRef] [PubMed]
- Jennings, N.; Lowe, G.; Tori, K. Nurse practitioner locums: A plausible solution for augmenting health care access for rural communities. Aust. J. Prim. Health 2021, 27, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Carey, T.; Sirett, D.; Wakerman, J.; Russell, D.; Humphreys, J. What principles should guide visiting primary health care services in rural and remote communities? Lessons from a systematic review. Aust. J. Rural Health 2018, 26, 146–156. [Google Scholar] [CrossRef] [PubMed]
- Hussain, R.; Maple, M.; Hunter, S.; Mapedzahama, V.; Reddy, P. The Fly-in Fly-out and Drive-in Drive-out model of health care service provision for rural and remote Australia: Benefits and disadvantages. Rural Remote Health 2015, 15, 3068. [Google Scholar] [CrossRef] [PubMed]
- Hayden, E.M.; Davis, C.; Clark, S.; Joshi, A.U.; Krupinski, E.A.; Naik, N.; Ward, M.J.; Zachrison, K.S.; Olsen, E.; Chang, B.P.; et al. Telehealth in emergency medicine: A consensus conference to map the intersection of telehealth and emergency medicine. Acad. Emerg. Med. 2021, 28, 1452–1474. [Google Scholar] [CrossRef] [PubMed]
- Schulz, T.; Long, K.; Kanhutu, K.; Bayrak, I.; Johnson, D.; Fazio, T. Telehealth during the coronavirus disease 2019 pandemic: Rapid expansion of telehealth outpatient use during a pandemic is possible if the programme is previously established. J. Telemed. Telecare 2020, 1357633X2094204. [Google Scholar] [CrossRef] [PubMed]
- Caffery, L.; Bradford, N.; Wickramasinghe, S.; Hayman, N.; Smith, A. Outcomes of using telehealth for the provision of healthcare to Aboriginal and Torres Strait Islander people: A systematic review. Aust. Z. J. Public Health 2017, 41, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Fitts, M.S.; Russell, D.; Mathew, S.; Liddle, Z.; Mulholland, E.; Comerford, C.; Wakerman, J. Remote health service vulnerabilities and responses to the COVID-19 pandemic. Aust. J. Rural Health 2020, 28, 613–617. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Local | DIDO | FIFO | Telehealth | Patients Required to Travel | |
|---|---|---|---|---|---|
| Aboriginal Educator | |||||
| Aboriginal Health Worker | |||||
| Aboriginal Nurse | |||||
| Addiction Medicine | |||||
| Audiology | |||||
| Cardiology | |||||
| Chiropody | |||||
| Clinical Nurse Specialist | |||||
| Community Health | |||||
| Counselling | |||||
| Dentistry | |||||
| Diabetes Educator | |||||
| Diabetes Medicine | |||||
| Dietician/Nutritionist | |||||
| Ear, Nose and Throat | |||||
| Endocrinology | |||||
| Family Health | |||||
| General Practitioner | |||||
| Geriatric Medicine | |||||
| Mental Health Trainee | |||||
| Midwifery | † | ||||
| Neurology | |||||
| Occupational Therapy | |||||
| Optometry | ‡ | ||||
| Oral Hygienist | |||||
| Paediatric Medicine | |||||
| Pharmacist | |||||
| Physical Trainer | |||||
| Physiotherapy | |||||
| Psychiatry | |||||
| Psychology | |||||
| Psychoneurology | |||||
| Registered Nurse | |||||
| Renal Medicine | § | ||||
| Respiratory Medicine | |||||
| Sexual Health | |||||
| Social Worker | |||||
| Sonography | ¶ | ||||
| Speech Pathology | |||||
| Sports Medicine/Exercise Physiologist |
| Always | Weekly | Fortnightly | Monthly | Quarterly | Yearly | |
|---|---|---|---|---|---|---|
| Aboriginal Educator | ||||||
| Aboriginal Health Worker | ||||||
| Aboriginal Nurse | ||||||
| Addiction Medicine | ||||||
| Audiology | ||||||
| Cardiology | † | |||||
| Chiropody | ||||||
| Clinical Nurse Specialist | ||||||
| Community Health | ||||||
| Counselling | ||||||
| Dentistry | ‡ | |||||
| Diabetes Educator | ||||||
| Diabetes Medicine | ||||||
| Dietician/Nutritionist | ||||||
| Ear, Nose and Throat | ||||||
| Endocrinology | ||||||
| Family Health | ||||||
| General Practitioner | ||||||
| Geriatric Medicine | ||||||
| Mental Health Trainee | ||||||
| Midwifery | ||||||
| Neurology | § | |||||
| Occupational Therapy | ||||||
| Optometry | ¶ | †† | ||||
| Oral Hygienist | ||||||
| Paediatric Medicine | ||||||
| Pharmacist | ||||||
| Physical Trainer | ||||||
| Physiotherapy | ||||||
| Psychiatry | ||||||
| Psychology | ||||||
| Psychoneurology | ||||||
| Registered Nurse | ||||||
| Renal Medicine | ||||||
| Respiratory Medicine | ||||||
| Sexual Health | †‡ | |||||
| Social Worker | ||||||
| Sonography | ||||||
| Speech Pathology | ||||||
| Sports Medicine/ Exercise Physiologist |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Osborn, E.; Ritha, M.; Macniven, R.; Agius, T.; Christie, V.; Finlayson, H.; Gwynn, J.; Hunter, K.; Martin, R.; Moir, R.; et al. “No One Manages It; We Just Sign Them Up and Do It”: A Whole System Analysis of Access to Healthcare in One Remote Australian Community. Int. J. Environ. Res. Public Health 2022, 19, 2939. https://doi.org/10.3390/ijerph19052939
Osborn E, Ritha M, Macniven R, Agius T, Christie V, Finlayson H, Gwynn J, Hunter K, Martin R, Moir R, et al. “No One Manages It; We Just Sign Them Up and Do It”: A Whole System Analysis of Access to Healthcare in One Remote Australian Community. International Journal of Environmental Research and Public Health. 2022; 19(5):2939. https://doi.org/10.3390/ijerph19052939
Chicago/Turabian StyleOsborn, Eloise, Marida Ritha, Rona Macniven, Tim Agius, Vita Christie, Heather Finlayson, Josephine Gwynn, Kate Hunter, Robyn Martin, Rachael Moir, and et al. 2022. "“No One Manages It; We Just Sign Them Up and Do It”: A Whole System Analysis of Access to Healthcare in One Remote Australian Community" International Journal of Environmental Research and Public Health 19, no. 5: 2939. https://doi.org/10.3390/ijerph19052939
APA StyleOsborn, E., Ritha, M., Macniven, R., Agius, T., Christie, V., Finlayson, H., Gwynn, J., Hunter, K., Martin, R., Moir, R., Taylor, D., Tobin, S., Ward, K., & Gwynne, K. (2022). “No One Manages It; We Just Sign Them Up and Do It”: A Whole System Analysis of Access to Healthcare in One Remote Australian Community. International Journal of Environmental Research and Public Health, 19(5), 2939. https://doi.org/10.3390/ijerph19052939