
Cross-Country Adaptation of a Psychological Flexibility Measure: The Comprehensive Assessment of Acceptance and Commitment Therapy Processes

 ,
,  ,
, 
Highlights
- Cross-cultural translation and adaptation of a psychological flexibility scale, termed CompACT.
- Italian, German and Spanish versions showed semantic, conceptual and normative equivalence to the original scale.
- All versions demonstrated good content validity.
- Adults in the community and people with multiple sclerosis in each target country found CompACT easy to understand.
- The study procedures and findings are informative for researchers adapting self-report scales into multiple languages.
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation
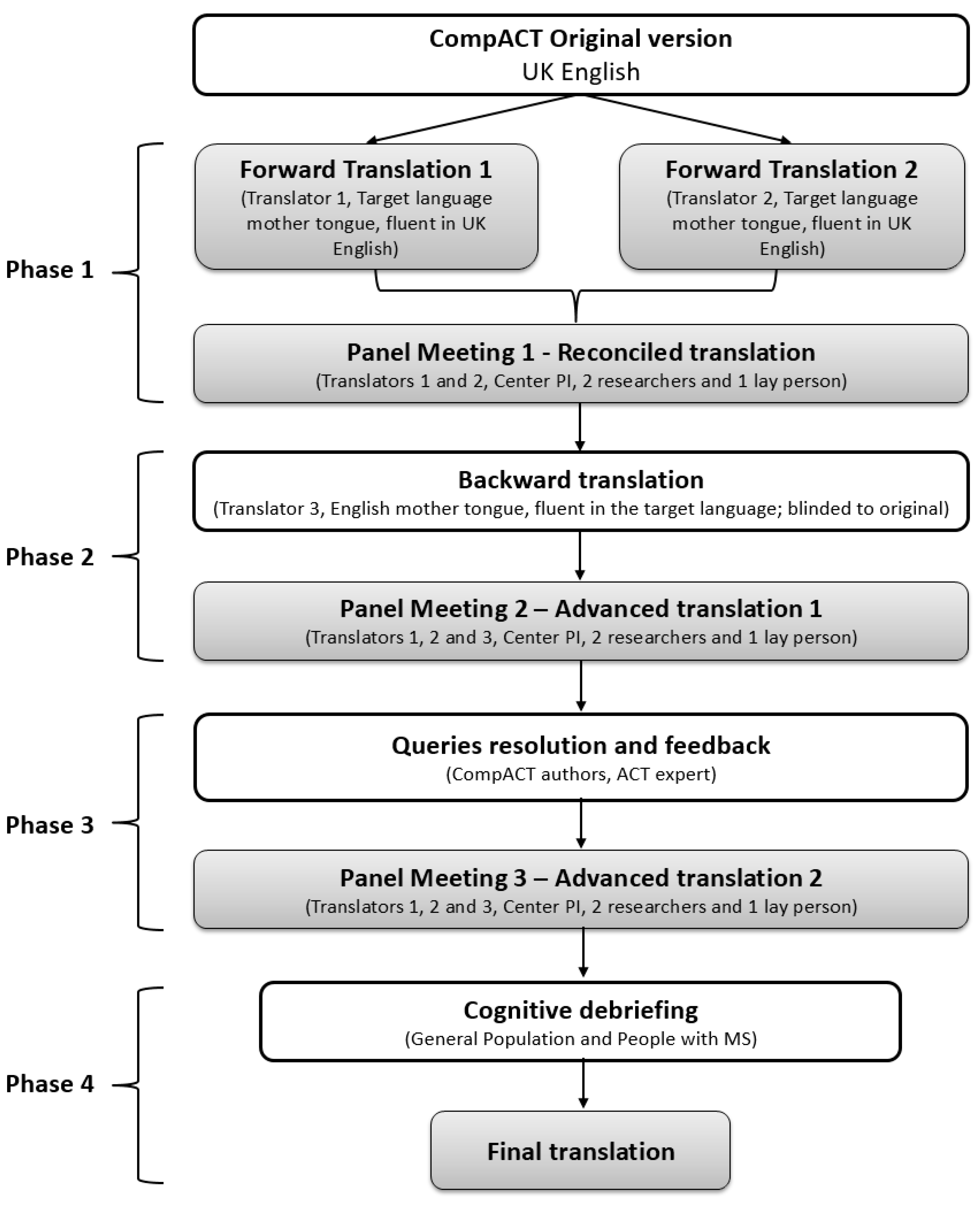
2.2. Translation-Adaptation
2.3. Cognitive Debriefing
2.3.1. Sampling and Recruitment
2.3.2. Interview Procedure for Cognitive Debriefing
2.4. Final Translations
2.5. Analyses
3. Results
3.1. Translations
3.1.1. Italy
3.1.2. Germany
3.1.3. Spain
3.2. Cognitive Debriefing
3.2.1. GP Sample
3.2.2. MS Patients
3.2.3. MH Discussion of the Findings
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hayes, S.C.; Strosahl, K.D.; Wilson, K.G. Acceptance and Commitment Therapy: An Experiential Approach to Behavior Change; Guilford Press: New York, NY, USA, 1999. [Google Scholar]
- Kashdan, T.B.; Rottenberg, J. Psychological flexibility as a fundamental aspect of health. Clin. Psychol. Rev. 2010, 30, 865–878. [Google Scholar] [CrossRef] [Green Version]
- Pakenham, K.I.; Mawdsley, M.; Brown, F.L.; Burton, N.W. Pilot evaluation of a resilience training program for people with multiple sclerosis. Rehabil. Psychol. 2018, 63, 29–42. [Google Scholar] [CrossRef] [Green Version]
- Hayes, S.C.; Luoma, J.B.; Bond, F.W.; Masuda, A.; Lillis, J. Acceptance and commitment therapy: Model, processes and outcomes. Behav. Res. Ther. 2006, 44, 1–25. [Google Scholar] [CrossRef] [Green Version]
- Southwick, S.M.; Vythilingam, M.; Charney, D.S. The psychobiology of depression and resilience to stress: Implications for prevention and treatment. Annu. Rev. Clin. Psychol. 2005, 1, 255–291. [Google Scholar] [CrossRef]
- Gloster, A.T.; Walder, N.; Levin, M.; Twohig, M.; Karekla, M. The empirical status of acceptance and commitment therapy: A review of meta-analyses. J. Contextual. Behav. Sci. 2020, 18, 181–192. [Google Scholar] [CrossRef]
- Pakenham, K.I.; Landi, G.; Boccolini, G.; Furlani, A.; Grandi, S.; Tossani, E. The moderating roles of psychological flexibility and inflexibility on the mental health impacts of COVID-19 pandemic and lockdown in Italy. J. Contextual. Behav. Sci. 2020, 17, 109–118. [Google Scholar] [CrossRef]
- Landi, G.; Pakenham, K.I.; Boccolini, G.; Grandi, S.; Tossani, E. Health Anxiety and Mental Health Outcome During COVID-19 Lockdown in Italy: The Mediating and Moderating Roles of Psychological Flexibility. Front. Psychol. 2020, 11, 2195. [Google Scholar] [CrossRef]
- Francis, A.W.; Dawson, D.L.; Golijani-Moghaddam, N. The development and validation of the Comprehensive assessment of Acceptance and Commitment Therapy processes (CompACT). J. Contextual. Behav. Sci. 2016, 5, 134–145. [Google Scholar] [CrossRef]
- Bond, F.W.; Hayes, S.C.; Baer, R.A.; Carpenter, K.M.; Guenole, N.; Orcutt, H.K.; Waltz, T.; Zettle, R.D. Preliminary psychometric properties of the Acceptance and Action Questionnaire-II: A revised measure of psychological inflexibility and experiential avoidance. Behav. Ther. 2011, 42, 676–688. [Google Scholar] [CrossRef] [Green Version]
- Doorley, J.D.; Goodman, F.R.; Kelso, K.C.; Kashdan, T.B. Psychological flexibility: What we know, what we do not know, and what we think we know. Soc. Personal. Psychol. Compass 2020, 14, e12566. [Google Scholar] [CrossRef]
- Kashdan, T.B.; Disabato, D.J.; Goodman, F.R.; Doorley, J.D.; McKnight, P.E. Understanding psychological flexibility: A multimethod exploration of pursuing valued goals despite the presence of distress. Psychol. Assess. 2020, 32, 829–850. [Google Scholar] [CrossRef] [PubMed]
- Wolgast, M. What does the Acceptance and Action Questionnaire (AAQ-II) really measure? Behav. Ther. 2014, 45, 831–839. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.C.; Villatte, M.; Levin, M.; Hildebrandt, M. Open, aware, and active: Contextual approaches as an emerging trend in the behavioral and cognitive therapies. Annu. Rev. Clin. Psychol. 2011, 7, 141–168. [Google Scholar] [CrossRef] [Green Version]
- Rolffs, J.L.; Rogge, R.D.; Wilson, K.G. Disentangling Components of Flexibility via the Hexaflex Model: Development and Validation of the Multidimensional Psychological Flexibility Inventory (MPFI). Assessment 2018, 25, 458–482. [Google Scholar] [CrossRef] [PubMed]
- Giovannetti, A.M.; Quintas, R.; Tramacere, I.; Giordano, A.; Confalonieri, P.; Messmer Uccelli, M.; Solari, A.; Pakenham, K.I. A resilience group training program for people with multiple sclerosis: Results of a pilot single-blind randomized controlled trial and nested qualitative study. PLoS ONE 2020, 15, e0231380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giovannetti, A.M.; Solari, A.; Pakenham, K.I. Effectiveness of a group resilience intervention for people with multiple sclerosis delivered via frontline services. Disabil. Rehabil. 2021, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Giovannetti, A.M.; Messmer Uccelli, M.; Solari, A.; Pakenham, K.I. Evaluation of a program for training psychologists in an acceptance and commitment therapy resilience intervention for people with multiple sclerosis: A single-arm longitudinal design with a nested qualitative study. Disabil. Rehabil. 2022, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Wild, D.; Grove, A.; Martin, M.; Eremenco, S.; McElroy, S.; Verjee-Lorenz, A.; Erikson, P.; ISPOR Task Force for Translation and Cultural Adaptation. Principles of Good Practice for the Translation and Cultural Adaptation Process for Patient-Reported Outcomes (PRO) Measures: Report of the ISPOR Task Force for Translation and Cultural Adaptation. Value Health J. Int. Soc. Pharm. Outcomes Res. 2005, 8, 94–104. [Google Scholar] [CrossRef] [Green Version]
- Polman, C.H.; Reingold, S.C.; Banwell, B.; Clanet, M.; Cohen, J.A.; Filippi, M.; Fujihara, K.; Havrdova, E.; Hutchinson, M.; Kappos, L.; et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann. Neurol. 2011, 69, 292–302. [Google Scholar] [CrossRef] [Green Version]
- Denzin, N.K.; Lincoln, Y.S. Handbook of Qualitative Research; Sage: London, UK, 2000. [Google Scholar]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [Green Version]
- Collins, D. Pretesting survey instruments: An overview of cognitive methods. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2003, 12, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Embretson, S.E.; Reise, S.P. Item Response Theory; Psychology Press: New York, NY, USA, 2013. [Google Scholar]
- Sousa, V.D.; Rojjanasrirat, W. Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: A clear and user-friendly guideline. J. Eval. Clin. Pract. 2011, 17, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Epstein, J.; Santo, R.M.; Guillemin, F. A review of guidelines for cross-cultural adaptation of questionnaires could not bring out a consensus. J. Clin. Epidemiol. 2015, 68, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Prinsen, C.; Mokkink, L.B.; Bouter, L.M.; Alonso, J.; Patrick, D.L.; de Vet, H.; Terwee, C.B. COSMIN guideline for systematic reviews of patient-reported outcome measures. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2018, 27, 1147–1157. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Characteristic | Italy (n = 8) | Germany (n = 8) | Spain (n = 8) |
|---|---|---|---|
| Age, years * | 57.0 (34.0–65.0) | 48.5 (24.0–62.0) | 53.5 (42.0–68.0) |
| Women ** | 7 (87.5) | 5 (62.5) | 7 (87.5) |
| Profession ** | |||
| Translator/conference Interpreter | 3 (37.5) | 3 (37.5) | 3 (37.5) |
| Neurologist | 1 (12.5) | 1 (12.5) | - |
| Physician | - | 1 (12.5) | 1 (12.5) |
| Psychologist/Neuropsychologist | 1 (12.5) | 1 (12.5) | 2 (25.5) |
| Lay person (technician) | 1 (12.5) | - | - |
| Lay person (administration employee) | 1 (12.5) | 1 (12.5) | |
| ACT expert | 2 (25.5) | 1 (12.5) | 1 (12.5) |
| Place of residence ** | |||
| Milan (Italy) | 6 (75.0) | - | - |
| Enna (Italy) | 1 (12.5) | - | - |
| Parma (Italy) | 1 (12.5) | ||
| Hamburg (Germany) | - | 7 (87.5) | - |
| Dresden (Germany) | - | 1 (12.5) | - |
| Barcelona (Spain) | - | - | 5 (62.5) |
| Madrid (Spain) | - | - | 1 (12.5) |
| Almeria (Spain) | 1 (12.5) | ||
| Esperança (Portugal) | 1 (12.5) |
| Where in the Questionnaire | Content of Concern | Italy | Germany | Spain | |||
|---|---|---|---|---|---|---|---|
| GP | PwMS | GP | PwMS | GP | PwMS | ||
| Item 2—One of my big goals is to be free from painful emotions | - Item too vague | 1 | 1 | ||||
| - Unclear expression: “big goal” | 1 | ||||||
| Item 3—I rush through meaningful activities without being really attentive to them | - Unclear item | 1 | |||||
| - Unclear expression: “meaningful activities” | 1 | ||||||
| Item 4—I try to stay busy to keep thoughts or feelings from coming | - Unclear item - Unclear expressions: “thoughts” and “feelings” | 2 | 1 | ||||
| Item 5—I act in ways that are consistent with how I wish to live my life | - Item too vague | 1 | |||||
| Item 6—I get so caught up in my thoughts that I am unable to do the things that I most want to do | - Unclear item, too nested | 1 | 1 | ||||
| Item 13—I am willing to fully experience whatever thoughts, feelings and sensations come up for me, without trying to change or defend against them | - Unclear expression: “to fully experience”. | 1 | |||||
| Item 20—Thoughts are just thoughts–they don’t control what I do | - Unclear item | 1 | 1 | ||||
| - Unclear expression: “thoughts do not control what I do” | 1 | ||||||
| - Unclear expression: “thoughts are just thoughts” | 2 | 1 | |||||
| Item 22—I can take thoughts and feelings as they come, without attempting to control or avoid them | - Unclear expression: “take thoughts and feeling as they come”. | 1 | |||||
| Response options | - Difficult to understand the response gradient - Option 3 (“Neither agree nor disagree”) is not useful | 1 | 1 | 2 | |||
| - Use number instead of label | 1 | ||||||
| General comments | - Too long statements (items) | 2 | |||||
| - Unclear item, too nested | 1 | 1 | |||||
| - Concerns on possible comprehension difficulties for people with cognitive impairment | 2 | ||||||
| - Identical items | 1 | 2 | 1 | 1 | |||
| - Include examples to clarify items | 1 | ||||||
| Characteristic | Italy (n = 8) | Germany (n = 6) | Spain (n = 4) |
|---|---|---|---|
| Age, years * | 36.5 (23.0–55.0) | 47.0 (36.0–55.0) | 53.5 (41.0–66.0) |
| Women ** | 6 (75.0) | 3 (50.0) | 3 (75.0) |
| Education ** | |||
| Middle school diploma | 0 (0) | 1 (17) | 0 (0) |
| High school diploma | 5 (62.5) | 2 (33) | 2 (50) |
| Degree | 3 (37.5) | 3 (50) | 2 (50) |
| Disease duration, years * | 5.0 (2.0–34.0) | 8.5 (1.0–21.0) | 15.0 (7.0–23.0) |
| MS type ** | |||
| Relapsing-remitting | 6 (75.0) | 4 (66.7) | 1 (25.0) |
| Secondary-progressive | 1 (12.5) | 2 (33.3) | 2 (50.0) |
| Primary-progressive | 1 (12.5) | 0 | 1 (25.0) |
| EDSS score * | 3.0 (1.0–8.0) | 2.5 (1.0–6.5) | 5.0 (4.0–6.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giovannetti, A.M.; Pöttgen, J.; Anglada, E.; Menéndez, R.; Hoyer, J.; Giordano, A.; Pakenham, K.I.; Galán, I.; Solari, A. Cross-Country Adaptation of a Psychological Flexibility Measure: The Comprehensive Assessment of Acceptance and Commitment Therapy Processes. Int. J. Environ. Res. Public Health 2022, 19, 3150. https://doi.org/10.3390/ijerph19063150
Giovannetti AM, Pöttgen J, Anglada E, Menéndez R, Hoyer J, Giordano A, Pakenham KI, Galán I, Solari A. Cross-Country Adaptation of a Psychological Flexibility Measure: The Comprehensive Assessment of Acceptance and Commitment Therapy Processes. International Journal of Environmental Research and Public Health. 2022; 19(6):3150. https://doi.org/10.3390/ijerph19063150
Chicago/Turabian StyleGiovannetti, Ambra Mara, Jana Pöttgen, Elisenda Anglada, Rebeca Menéndez, Jürgen Hoyer, Andrea Giordano, Kenneth Ian Pakenham, Ingrid Galán, and Alessandra Solari. 2022. "Cross-Country Adaptation of a Psychological Flexibility Measure: The Comprehensive Assessment of Acceptance and Commitment Therapy Processes" International Journal of Environmental Research and Public Health 19, no. 6: 3150. https://doi.org/10.3390/ijerph19063150