
Neurologists’ Knowledge, Practice, and Attitudes towards Pharmacovigilance and Adverse Drug Reactions Reporting Process in Epileptic Patients—Comparative Analysis from Poland and Egypt

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methodology
3. Results
3.1. Knowledge
3.2. Attitude
3.3. Practice
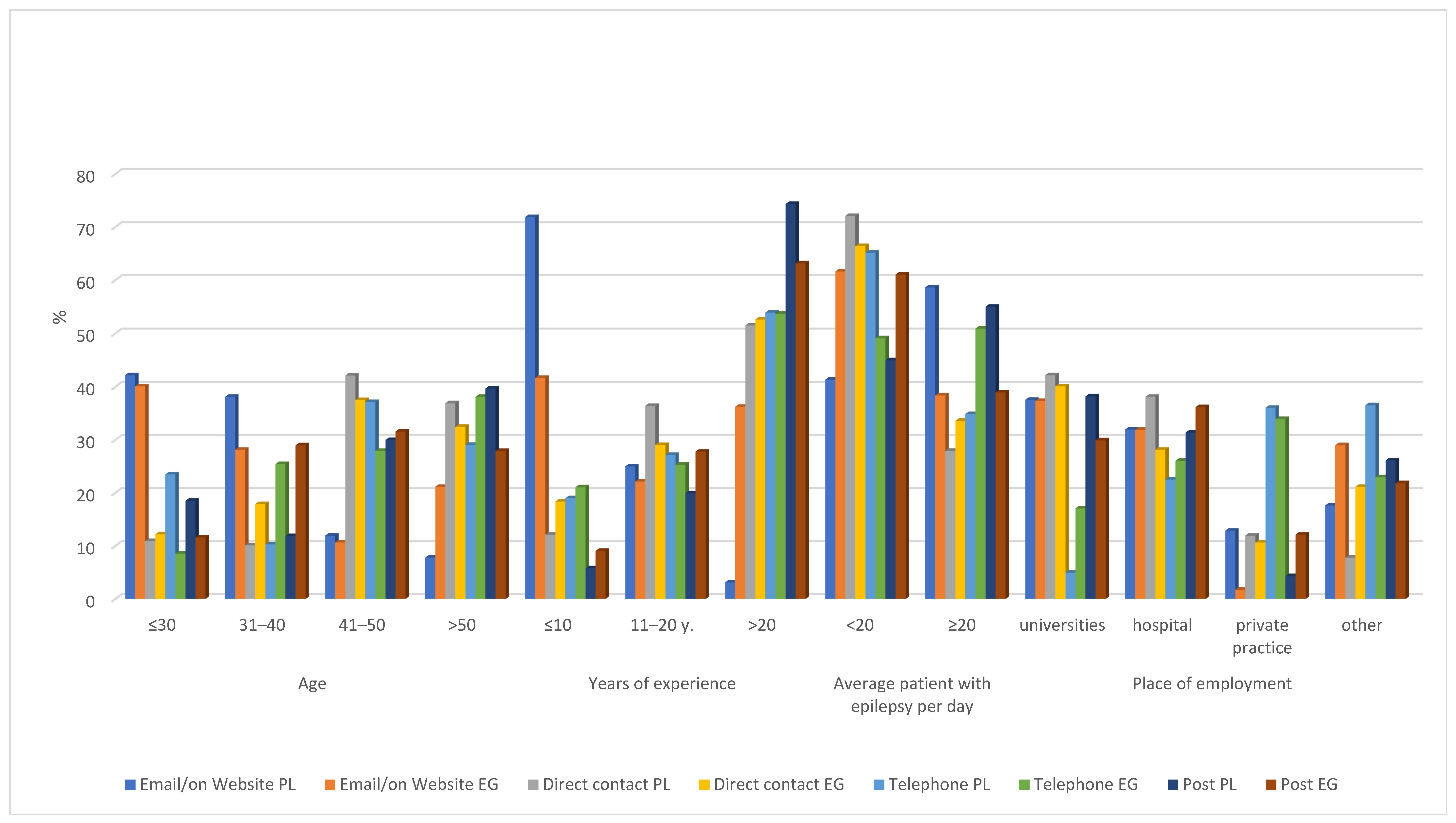
3.4. Communication Method Preferred by Neurologists to Send ADRs
3.5. Sources Used to Gather Information about ADRs
3.6. The Main Factors Discouraging Neurologists from Delivering Pharmacovigilance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. The Importance of Pharmacovigilance: Safety Monitoring of Medicinal Products. WHO Collaborating Centre for International Drug Monitoring. 2002. Available online: http://apps.who.int/medicinedocs/en/d/Js4893e/ (accessed on 24 January 2022).
- Wu, W.K.; Pantaleo, N. Evaluation of outpatient adverse drug reactions leading to hospitalization. Am. J. Health-Syst. Pharm. 2003, 60, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Kongkaew, C.; Noyce, P.R.; Ashcroft, D.M. Hospital admissions associated with adverse drug reactions: A systematic review of prospective observational studies. Ann. Pharmacother. 2008, 42, 1017–1025. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. IC for the NR of the IC of D. 1975: Manual of the International Statistical Classification of Diseases, Injuries, and Causes of Death: Based on the Recommendations of the Ninth Revision Conference, 1975, and Adopted by the Twenty-Ninth World Health Assembly. 1977. Available online: https://apps.who.int/iris/handle/10665/40492 (accessed on 24 January 2022).
- Magar, Y.B.; Hiray, R.S.; Ghongane, B.B. Utilization pattern of antiepileptic drugs and their adverse effects in tertiary healthcare and teaching hospital. Int. J. Basic Clin. Pharmacol. 2018, 8, 39–46. Available online: https://www.ijbcp.com/index.php/ijbcp/article/view/3055 (accessed on 19 January 2022). [CrossRef]
- Ferrendelli, J.A. Concerns with antiepileptic drug initiation: Safety, tolerability, and efficacy. Epilepsia 2001, 42, 28–30. [Google Scholar] [CrossRef]
- Landmark, C.J. Antiepileptic drugs in non-epilepsy disorders: Relations between mechanisms of action and clinical efficacy. CNS Drugs 2008, 22, 27–47. [Google Scholar] [CrossRef]
- Landmark, C.J.; Johannessen, S.I.; Tomson, T. Host factors affecting antiepileptic drug delivery-pharmacokinetic variability. Adv. Drug Deliv. Rev. 2012, 64, 896–910. [Google Scholar]
- Androsova, G.; Krause, R.; Borghei, M.; Wassenaar, M.; Auce, P.; Avbersek, A.; Becker, F.; Berghuis, B.; Campbell, E.; Coppola, A.; et al. Comparative effectiveness of antiepileptic drugs in patients with mesial temporal lobe epilepsy with hippocampal sclerosis. Epilepsia 2017, 58, 1734–1741. [Google Scholar] [CrossRef]
- Tomson, T.; Battino, D.; Bonizzoni, E.; Craig, J.; Lindhout, D.; Perucca, E.; Sabers, A.; Thomas, S.V.; Vajda, F.; Faravelli, F.; et al. Comparative risk of major congenital malformations with eight different antiepileptic drugs: A prospective cohort study of the EURAP registry. Lancet Neurol. 2018, 17, 530–538. [Google Scholar]
- Braillon, A.; Bewley, S. Prescribing in pregnancy shows the weaknesses in pharmacovigilance. BMJ 2018, 361, k2334. [Google Scholar] [CrossRef]
- Pugatch, P.M.; Torstensson, D.D.; Laufer, M. The Next Frontier in Ensuring the Quality of Medicines. Pugatch Consilium 2015. pp. 1–44. Available online: https://www.pugatch-consilium.com/reports/The%20Next%20Frontier.pdf (accessed on 24 January 2022).
- Hartman, J.; Härmark, L.; van Puijenbroek, E. A global view of undergraduate education in pharmacovigilance. Eur. J. Clin. Pharmacol. 2017, 73, 891–899. [Google Scholar] [CrossRef]
- Qato, D.M. Current state of pharmacovigilance in the Arab and Eastern Mediterranean region: Results of a 2015 survey. Int. J. Pharm. Pract. 2018, 26, 210–221. [Google Scholar] [CrossRef] [PubMed]
- Alshammari, T.M.; Alenzi, K.A.; Ata, S.I. National pharmacovigilance programs in Arab countries: A quantitative assessment study. Pharmacoepidemiol. Drug Saf. 2020, 29, 1001–1010. Available online: https://onlinelibrary.wiley.com/doi/abs/10.1002/pds.4991 (accessed on 19 January 2022). [CrossRef] [PubMed]
- Wilbur, K. Pharmacovigilance in the Middle East: A survey of 13 arabic-speaking countries. Drug Saf. 2013, 36, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Alraie, N.A.; Saad, A.A.; Sabry, N.A.; Farid, S.F. Adverse drug reactions reporting: A questionnaire-based study on Egyptian pharmacists’ attitudes following an awareness workshop. J. Eval. Clin. Pract. 2016, 22, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Kopciuch, D.; Zaprutko, T.; Paczkowska, A.; Ratajczak, P.; Zielińska-Tomczak, Ł.; Kus, K.; Nowakowska, E. Safety of medicines-Pharmacists’ knowledge, practice, and attitudes toward pharmacovigilance and adverse drug reactions reporting process. Pharmacoepidemiol. Drug Saf. 2019, 28, 1543–1551. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Safety of Medicines in Public Health Programmes: Pharmacovigilance an Essential Tool. WHO Press. 2006. Available online: https://apps.who.int/iris/handle/10665/43384 (accessed on 24 January 2022).
- Hardeep, J.K.B.; Rakesh, K. A survey on the knowledge, attitude and the practice of pharmacovigilance among the health care professionals in a teaching hospital in northern India. J. Clin. Diagn. Res. JCDR 2013, 7, 97. [Google Scholar]
- Das, L.; Bhattacharjee, P.; Ghosh, R.; Das, U.; Ray, T. Knowledge, attitude, and practice of pharmacovigilance among doctors in a tertiary care teaching hospital of Tripura. Natl. J. Physiol. Pharm. Pharmacol. 2017, 7, 218–223. Available online: http://www.scopemed.org/fulltextpdf.php?mno=242249 (accessed on 19 January 2022). [CrossRef]
- Bäckström, M.; Mjörndal, T.; Dahlqvist, R.; Nordkvist-Olsson, T. Attitudes to reporting adverse drug reactions in northern Sweden. Eur. J. Clin. Pharmacol. 2000, 56, 729–732. [Google Scholar] [CrossRef]
- Atif, M.; Ahmad, M.; Saleem, Q.; Curley, L.; Qamar-Uz-Zaman, M.; Babar, Z.U.D. Pharmaceutical policy in Pakistan. In Pharmaceutical Policy in Countries with Developing Healthcare Systems; Springer International Publishing: Cham, Switzerland, 2017; pp. 25–44. Available online: http://www.scopus.com/inward/record.url?scp=85030253084&partnerID=8YFLogxK (accessed on 19 January 2022).
- Aziz, Z.; Siang, T.C.; Badarudin, N.S. Reporting of adverse drug reactions: Predictors of under-reporting in Malaysia. Pharmacoepidemiol. Drug Saf. 2007, 16, 223–228. [Google Scholar] [CrossRef]
- Iffat, W.; Shakeel, S.; Rahim, N.; Anjum, F.; Nesar, S.; Ghayas, S. Pakistani physicians knowledge and attitude towards reporting adverse drug reactions. Afr. J. Pharm. Pharmacol. 2014, 8, 379–385. [Google Scholar]
- Thomas, T.M.; Udaykumar, P.; Scandashree, K. Knowledge, Attitude and Practice of Adverse Drug Reaction Reporting among Doctors in a Tertiary Health Care Centre in South India. Int. J. Pharmacol. Clin. Sci. 2013, 2, 82–88. Available online: https://www.ijphs.org/article/2013/2/3-3 (accessed on 19 January 2022).
- Okezie, E.O.; Olufunmilayo, F. Adverse drug reactions reporting by physicians in Ibadan, Nigeria. Pharmacoepidemiol. Drug Saf. 2008, 17, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Adhikari, A.; Indu, R.; Ray, M.; Bhattacharya, S.; Biswas, R.; Das, A.K. Knowledge, attitude and perception of physicians towards adverse drug reaction (ADR) reporting: A pharmacovigilance study. Int. J. Adv. Med. 2017, 4, 1685–1689. Available online: https://www.ijmedicine.com/index.php/ijam/article/view/858 (accessed on 19 January 2022). [CrossRef] [Green Version]
- Oshikoya, K.A.; Awobusuyi, J.O. Perceptions of doctors to adverse drug reaction reporting in a teaching hospital in Lagos, Nigeria. BMC Clin. Pharmacol. 2009, 9, 14. [Google Scholar] [CrossRef] [Green Version]
- Chatterjee, S.; Lyle, N.; Ghosh, S. A survey of the knowledge, attitude and practice of adverse drug reaction reporting by clinicians in eastern India. Drug Saf. 2006, 29, 641–642. [Google Scholar] [CrossRef]
- Rajesh, R.; Vidyasagar, S.; Varma, D.M. An Educational Intervention to assess Knowledge Attitude Practice of pharmacovigilance among Health care professionals in an Indian tertiary care teaching hospital. Int. J. PharmTech Res. 2011, 3, 678–692. [Google Scholar]
- Stoynova, V.; Getov, I.N.; Naseva, E.K.; Lebanova, H.V.; Grigorov, E.E. Physicians’ knowledge and attitude towards adverse event reporting system and result to intervention—randomized nested trial among Bulgarian physicians. Med. Glas. 2013, 10, 365–372. [Google Scholar]
- Bäckström, M.; Mjörndal, T. A small economic inducement to stimulate increased reporting of adverse drug reactions—A way of dealing with an old problem? Eur. J. Clin. Pharmacol. 2006, 62, 381–385. [Google Scholar] [CrossRef]
- Rishi, R.K.; Patel, R.K.; Bhandari, A. Opinion of physicians towards Adverse Drug Reactions reporting Results of pilot study. J. Community Nutr. Health Rural. Res. Inst. Physiol. Appl. Nutr. 2012, 1, 25. Available online: http://jcnh.in/download/OA3.pdf (accessed on 19 January 2022).
- Agarwal, R.; Daher, A.M.; Mohd Ismail, N. Knowledge, practices and attitudes towards adverse drug reaction reporting by private practitioners from klang valley in malaysia. Malays. J. Med. Sci. 2013, 20, 52–61. [Google Scholar]
- John, L.J.; Arifulla, M.; Cheriathu, J.J.; Sreedharan, J. Reporting of adverse drug reactions: An exploratory study among nurses in a teaching hospital, Ajman, United Arab Emirates. DARU J. Pharm. Sci. 2012, 20, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figueiras, A.; Tato, F.; Fontaiñas, J.; Takkouche, B.; Gestal-Otero, J.J. Physicians’ attitudes towards voluntary reporting of adverse drug events. J. Eval. Clin. Pract. 2001, 7, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Paveliu, M.S.; Bengea-Luculescu, S.; Toma, M.; Paveliu, S.F. Perception on adverse drug reaction reporting by physicians working in southern romania. Maedica 2013, 8, 17–25. [Google Scholar] [PubMed]
- Bisht, M.; Singh, S.; Dhasmana, D.C. Effect of educational intervention on adverse drug reporting by physicians: A cross-sectional study. ISRN Pharmacol. 2014, 2014, 259476. [Google Scholar] [CrossRef] [PubMed]
- Awodele, O.; Akinyede, A.; Adeyemi, O.A.; Awodele, D.F. Pharmacovigilance amongst doctors in private hospitals in Lagos West Senatorial District, Nigeria. Int. J. Risk Saf. Med. 2011, 23, 217–226. [Google Scholar] [CrossRef]
- Kamtane, R.A.; Jayawardhani, V. Knowledge, attitude and perception of physicians towards adverse drug reaction (ADR) reporting: A pharmacoepidemiological study. Asian J. Pharm. Clin. Res. 2012, 5, 210–214. [Google Scholar]
- Sanghavi, D.R.; Dhande, P.P.; Pandit, V.A. Perception of pharmacovigilance among doctors in a tertiary care hospital: Influence of an interventional lecture. Int. J. Risk Saf. Med. 2013, 25, 197–204. [Google Scholar] [CrossRef]
- Abu Farha, R.; Abu Hammour, K.; Rizik, M.; Aljanabi, R.; Alsakran, L. Effect of educational intervention on healthcare providers knowledge and perception towards pharmacovigilance: A tertiary teaching hospital experience. Saudi Pharm. J. 2018, 26, 611–616. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6035326/ (accessed on 19 January 2022). [CrossRef]
- Ahmad, A.; Patel, I.; Balkrishnan, R.; Mohanta, G.P.; Manna, P.K. An evaluation of knowledge, attitude and practice of Indian pharmacists towards adverse drug reaction reporting: A pilot study. Perspect. Clin. Res. 2013, 4, 204–210. [Google Scholar] [CrossRef]
- Inácio, P.; Cavaco, A.; Airaksinen, M. The value of patient reporting to the pharmacovigilance system: A systematic review. Br. J. Clin. Pharmacol. 2017, 83, 227–246. [Google Scholar] [CrossRef] [Green Version]
- Vilhelmsson, A. Consumer narratives in ADR reporting: An important aspect of public health? Experiences from reports to a Swedish consumer organization. Front. Public Health 2015, 3, 211. Available online: https://www.frontiersin.org/article/10.3389/fpubh.2015.00211 (accessed on 19 January 2022). [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Parameter | PL/EG | General |
|---|---|---|
| Age [years; mean (SD)] | 45.09 (30.01)/ 56 (33.12) | 42.05 (38.32) |
| Sex [female; N (%)] | 374 (57)/ 167 (38) | 752 (68.67) |
| Years of practice [years; mean (SD)] | 17.87 (10.01/ 15.98 (12.12) | 15.13 (11.12) |
| Place of employment; N (%) | ||
| Universities | 104 (16.01)/ 57 (13.77) | 118 (10.77) |
| Hospital | 197 (30.12)/ 123 (28.14) | 248 (22.64) |
| Private practice/private office | 288 (44.23)/ 162 (37.01) | 575 (52.51) |
| Other | 67 (10.12)/ 97 (22.05) | 154 (14.06) |
| Patient with epilepsy per day [mean (SD)] | 15.02 (6.34)/ 10.88 (7.07) | 12.04 (8.12) |
| Response N (%) PL/EG | Country/ p-Value | Age (%) | Years of Experience (%) | Average Patient with Epilepsy Per Day (%) | Place of Employment (%) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 656 (60)/ 439 (40) | ≤30 | 31–40 | 41–50 | >50 | ≤10 | 11–20 | >20 | <20 | ≥20 | Universities | Hospital | Private Practice/Private Office | Other | ||
| Knowledge | |||||||||||||||
| The most appropriate definition of pharmacovigilance: Correct answer | 377 (57.43)/ 159 (36.23) | PL | 42.01 * | 33.23 | 18.78 | 5.98 | 43.12 c | 37.89 | 18.99 | 48.12 | 51.88 | 43.09 ^ | 29.03 | 7.37 | 20.51 |
| EG | 34.44 a | 38.76 | 10.16 | 16.64 | 48.76 c | 29.09 | 22.15 | 62.77 f | 37.23 | 52.08 # | 26.77 | 18.09 | 3.06 | ||
| p-value: | NS | NS | 0.0134 | 0.0001 | NS | 0.0515 | NS | 0.0019 | 0.0019 | NS | NS | 0.0002 | <0.0001 | ||
| The most appropriate purpose of pharmacovigilance: correct answer | 420 (64.02)/ 198 (45.12) | PL | 29.97 * | 34.12 | 30.10 | 5.81 | 41.76 | 28.44 | 29.80 | 58.09 | 41.91 | 37.12 ^ | 29.04 | 15.12 | 18.72 |
| EG | 40.09 a | 28.12 | 10.65 | 21.14 | 33.10 | 37.32 | 29.58 | 55.90 | 44.10 | 27.12 | 31.87 # | 33.76 | 7.25 | ||
| p-value | 0.0127 | NS | <0.0001 | <0.0001 | 0.0394 | 0.0263 | NS | NS | NS | 0.0143 | NS | <0.0001 | 0.0002 | ||
| Functions of pharmacovigilance: correct answer | 472 (72.00)/ 145 (32.92) | PL | 44.09 * | 25.12 | 28.10 | 2.69 | 36.87 | 41.10 c | 22.03 | 53.50 | 46.50 | 39.21 ^ | 27.03 | 8.66 | 25.10 |
| EG | 29.10 | 37.31 | 18.87 | 14.72 | 44.09 c | 29.68 | 26.23 | 65.90 f | 34.10 | 47.14 ^ | 26.05 | 5.72 | 21.09 | ||
| p-value | 0.0013 | 0.0042 | 0.0265 | <0.0001 | NS | 0.0134 | NS | 0.0084 | 0.0084 | NS | NS | NS | NS | ||
| Definition of ADR: correct answer | 287 (43.76) 285/ (65.02) | PL | 39.10 * | 35.43 | 17.85 | 7.62 | 39.76 | 30.44 | 29.80 | 47.43 | 37.34 | 29.97 | 34.12 # | 30.10 | 5.81 |
| EG | 22.65 | 29.13 | 19.95 | 28.27 | 33.10 | 37.32 | 29.58 | 61.77 | 38.23 | 40.09 ^ | 28.12 | 10.65 | 21.14 | ||
| p-value | <0.0001 | NS | NS | <0.0001 | NS | NS | NS | 0.0006 | NS | 0.0112 | NS | <0.0001 | <0.0001 | ||
| The purpose of an ADR: correct answer | 303 (46.12)/ 242 (55.09) | PL | 37.55 a | 31.96 | 12.87 | 17.62 | 38.46 | 36.12 | 25.42 | 28.99 f | 71.01 | 30.97 | 34.12 ^ | 31.10 | 3.81 |
| EG | 40.34 * | 31.92 | 17.76 | 9.98 | 48.87 c | 33.32 | 17.81 | 43.71 | 56.29 | 40.09 ^ | 28.12 | 10.65 | 21.14 | ||
| p-value | NS | NS | NS | 0.0112 | 0.0148 | NS | 0.0332 | 0.0004 | 0.0004 | 0.0266 | NS | <0.0001 | <0.0001 | ||
| When serious ADRs should be reported?: Correct answer | 321 (48.98)/ 195 (44.34) | PL | 43.30 * | 28.98 | 19.10 | 7.62 | 41.38 c | 21.30 | 37.32 | 41.43 | 58.57 | 56.41 & | 9.52 | 12.09 | 21.98 |
| EG | 29.90 | 35.12 a | 12.45 | 22.53 | 56.34 c | 31.90 | 11.76 | 66.06 f | 33.94 | 39.59 ^ | 29.31 | 9.12 | 21.98 | ||
| p-value | 0.0024 | NS | 0.0489 | <0.0001 | 0.0010 | 0.0072 | <0.0001 | <0.0001 | <0.0001 | 0.0002 | <0.0001 | NS | NS | ||
| To whom should ADRs be reported?: Correct answer | 256 (39.10)/ 104 (23.77) | PL | 38.46 * | 26.12 | 33.65 | 1.77 | 41.90 c | 39.36 | 18.74 | 41.18 | 58.82 | 37.55 | 31.96 | 12.87 | 17.62 |
| EG | 28.87 | 33.32 * | 28.17 | 9.64 | 31.10 | 39.09 | 29.81 | 52.57 | 47.43 | 37.34 ^ | 31.92 | 1.76 | 28.98 | ||
| p-value | NS | NS | NS | 0.0006 | NS | NS | 0.0214 | 0.0487 | 0.0487 | NS | NS | 0.0012 | 0.0163 | ||
| Are you co-responsible for ADR reporting?: Yes | 415 (63.34)/ 211 (48.09) | PL | 33.76 * | 29.12 | 33.43 | 3.69 | 44.10 c | 38.12 | 17.78 | 28.98 f | 71.02 | 29.41 | 42.88 ^ | 9.62 | 18.09 |
| EG | 41.23 * | 12.38 | 27.15 | 19.24 | 29.09 | 31.65 | 39.26 | 36.47 f | 63.53 | 37.33 | 26.15 | 15.43 | 21.09 | ||
| p-value | NS | <0.0001 | NS | <0.0001 | 0.0035 | NS | <0.0001 | NS | NS | 0.0448 | <0.0001 | 0.0317 | NS | ||
| Attitude | |||||||||||||||
| Do you believe that many ADRs are preventable?: yes | 216 (32.98)/ 186 (42.34) | PL | 33.34 | 38.51 a | 12.54 | 15.61 | 40.04 | 26.61 | 33.35 | 44.09 | 55.91 | 39.90 ^# | 35.12 | 12.45 | 12.53 |
| EG | 22.57 | 26.12 | 33.74 | 17.57 | 33.98 | 31.61 | 34.41 | 56.32 | 43.68 | 12.05 #& | 29.76 | 12.76 ^& | 63.24 | ||
| p-value | 0.0169 | 0.0083 | <0.0001 | NS | NS | NS | NS | 0.0145 | 0.0145 | <0.0001 | NS | NS | <0.0001 | ||
| Do you think it is necessary to report ADRs from patients with epilepsy?: yes | 506 (77.09)/ 308 (70.09) | PL | 43.30 * | 28.98 | 19.10 | 7.62 | 41.38 | 21.30 | 37.32 | 41.43 | 58.57 | 56.41 & ^ | 9.52 | 12.09 | 21.98 |
| EG | 39.90 * | 35.12 | 12.45 | 12.53 | 53.34 | 33.90 | 11.76 | 66.06 f | 33.94 | 39.59 ^ | 29.31 | 9.12 | 21.98 | ||
| p-value | NS | NS | 0.0134 | 0.0204 | 0.0009 | 0.0001 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | NS | NS | ||
| Do you think the ADR reporting is a neurologist’s obligation?: yes | 460 (70.09)/ 264 (60.13) | PL | 4.01 | 33.23 g | 18.78 | 7.98 | 43.12 | 37.89 | 18.99 | 48.12 | 51.88 | 43.09 ^ | 29.03 | 6.37 | 21.51 |
| EG | 34.44 | 38.76 a | 10.16 | 16.64 | 48.76 | 29.09 | 22.15 | 62.77 f | 37.23 | 52.08 # | 26.77 | 18.09 | 3.06 | ||
| p-value | <0.0001 | NS | 0.0021 | 0.0004 | NS | 0.0166 | NS | 0.0003 | 0.0001 | 0.0196 | NS | <0.0001 | <0.0001 | ||
| Practice | |||||||||||||||
| Have you ever reported any ADRs from patient with epilepsy?: yes | 262 (39.90)/ 137 (31.11) | PL | 39.40 * | 31.23 | 18.78 | 10.59 | 38.12 | 43.89 c | 17.99 | 41.12 | 58.88 | 43.09 ^ | 29.03 | 7.37 | 20.51 |
| EG | 44.14 * | 28.76 | 17.76 | 9.34 | 43.76 c | 32.69 | 23.55 | 60.77 f | 39.23 | 52.08 # | 26.77 | 18.09 | 3.06 | ||
| p-value | NS | NS | NS | NS | NS | 0.0302 | NS | 0.0002 | 0.0002 | NS | NS | 0.0012 | <0.0001 | ||
| Do you report ADRs on a regular basis from patients with epilepsy?: yes | 215 (32.78)/ 127 (28.89) | PL | 42.15 * | 38.12 | 11.92 | 7.81 | 31.76 | 38.44 | 29.80 | 58.09 | 41.91 | 37.12 ^ | 29.04 | 15.12 | 18.72 |
| EG | 40.09 a | 28.12 | 10.65 | 21.14 | 33.10 | 37.32 | 29.58 | 55.90 | 44.10 | 27.12 # | 31.87 | 33.76 | 7.25 | ||
| p-value | NS | NS | NS | 0.0004 | NS | NS | NS | NS | NS | NS | NS | 0.0001 | 0.0036 | ||
| If yes, how many ADRs on average would be diagnosed (or observed) in a period of 6 months? | |||||||||||||||
| <5 | 544 (82.98)/ 334 (76.12) | PL | 29.10 | 37.31 * | 18.87 | 14.72 | 44.09 | 29.68 | 26.23 | 65.90 f | 34.10 | 47.14 ^ | 26.05 | 5.72 | 21.09 |
| EG | 44.09 * | 25.12 | 28.10 | 2.69 | 36.87 | 41.10 f | 22.03 | 53.50 | 46.50 | 39.21 ^ | 27.03 | 8.66 | 25.10 | ||
| p-value | <0.0001 | 0.0002 | 0.0014 | <0.0001 | 0.0349 | 0.0005 | NS | 0.0003 | 0.0003 | 0.0216 | NS | NS | NS | ||
| 5–10 | 79 (12.01)/ 75 (17.12) | PL | 56.41 h | 9.52 | 12.09 | 21.98 | 51.11 d | 17.58 | 31.31 | 58.17 | 41.83 | 41.23 & | 12.38 | 27.15 | 19.24 |
| EG | 39.59 a | 29.31 | 9.12 | 21.98 | 37.10 | 25.15 | 37.75 | 49.03 | 50.97 | 33.76 # | 29.12 | 33.43 | 3.69 | ||
| p-value | 0.0368 | 0.0018 | NS | NS | NS | NS | NS | NS | NS | NS | 0.0102 | NS | 0.0027 | ||
| >10 | 33 (5.01)/ 30 (6.76) | PL | 39.10 * | 35.43 | 17.85 | 7.62 | 39.76 | 30.44 | 29.80 | 47.43 | 37.34 | 29.97 # | 34.12 | 30.10 | 5.81 |
| EG | 22.65 | 29.13 | 19.95 | 28.27 | 33.10 | 37.32 | 29.58 | 61.77 f | 38.23 | 40.09 ^ | 28.12 | 10.65 | 21.14 | ||
| p-value | NS | NS | NS | 0.0310 | NS | NS | NS | NS | NS | NS | NS | NS | NS | ||
| What type of ADR is the one you report most frequently? | |||||||||||||||
| Severe | 481 (73.34)/ 286 (65.09) | PL | 37.55 * | 31.96 | 12.87 | 17.62 | 39.38 | 21.30 | 39.32 | 41.43 | 58.57 | 37.55 ^ | 29.00 | 14.14 | 19.31 |
| EG | 37.34 a | 31.92 | 1.76 | 28.98 | 53.34 c | 33.90 | 11.76 | 66.06 f | 33.94 | 33.76 # | 30.12 # | 32.43 # | 3.69 | ||
| p-value | NS | NS | <0.0001 | 0.0002 | 0.0002 | 0.0001 | <0.0001 | <0.0001 | <0.0001 | NS | NS | <0.0001 | <0.0001 | ||
| Rare | 89 (13.65)/ 111 (25.34) | PL | 6.64 * | 20.10 | 28.12 | 45.14 | 43.12 c | 37.89 | 18.99 | 48.12 | 51.88 | 56.41 & | 9.52 | 12.09 | 21.98 |
| EG | 3.54 * | 28.90 | 31.90 | 35.66 | 48.76 c | 29.09 | 22.15 | 62.77 f | 37.23 | 39.59 ^ | 29.31 | 9.12 | 21.98 | ||
| p-value | NS | NS | NS | NS | NS | NS | NS | NS | NS | NS | NS | NS | NS | ||
| Unexpected | 85 (13.01)/ 42 (9.57) | PL | 20.89 | 18.12 | 27.12 | 33.87 | 29.56 | 31.17 | 39.27 | 51.09 | 48.91 | 37.55 ^ | 31.96 ^ | 12.87 | 17.62 |
| EG | 26.98 | 30.13 | 23.34 | 19.56 | 33.13 | 39.03 | 27.84 | 68.02 f | 31.98 | 37.34 ^ | 31.92 ^ | 1.76 | 28.98 ^ | ||
| p-value | NS | NS | NS | NS | NS | NS | NS | NS | NS | NS | NS | 0.0415 | NS | ||
| Response N(%) PL/EG | Country | Age (%) PL/EG | Years of Experience (%) PL/EG | Average Patient with Epilepsy Per Day (%) PL/EG | Place of Employment (%) PL/EG | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ≤30 | 31–40 | 41–50 | >50 | ≤10 | 11–20 | >20 | <20 | ≥20 | Universities | Hospital | Private Practice/Private Office | Other | |||
| Barriers | |||||||||||||||
| Apprehension about sending an inappropriate report | 40 (6.09)/ 25 (5.81) | PL | 35.77 a | 29.34 | 15.94 | 18.95 | 35.55 | 38.05 | 26.40 | 34.98 f | 65.02 | 36.66 #^ | 37.94 | 15.09 | 10.31 |
| EG | 28.90 | 31.03 * | 28.58 | 11.49 | 30.00 | 38.19 | 31.81 | 61.55 f | 38.45 | 33.76 # | 29.12 # | 33.43 # | 3.69 | ||
| p-value | NS | NS | NS | NS | NS | NS | NS | 0.0363 | 0.0363 | NS | NS | NS | NS | ||
| Lack of time to fill in a report | 243 (37.09)/ 154 (35.12) | PL | 12.41 | 19.57 | 38.04 g | 29.98 | 21.11 | 47.58 @ | 31.31 | 58.17 | 41.83 | 41.23 & | 12.38 | 27.15 | 19.24 |
| EG | 15.49 | 21.31 | 29.12 g | 34.08 | 37.10 | 25.15 | 37.75 | 49.03 | 50.97 | 33.76 # | 29.12 # | 33.43 # | 3.69 | ||
| p-value | NS | NS | NS | NS | 0.0005 | <0.0001 | NS | NS | NS | NS | <0.0001 | NS | <0.0001 | ||
| Concern that the report will generate extra work | 151 (23.09)/ 110 (25.12) | PL | 39.10 * | 35.43 | 17.85 | 7.62 | 39.76 | 30.44 | 29.80 | 47.43 | 37.34 | 29.97 # | 34.12 # | 30.10 # | 5.81 |
| EG | 15.65 | 23.13 | 22.95 | 38.27 g | 33.10 | 37.32 | 29.58 | 61.77 f | 38.23 | 40.09 ^ | 28.12 | 10.65 | 21.14 | ||
| p-value | <0.0001 | 0.0327 | NS | <0.0001 | NS | NS | NS | 0.0218 | NS | NS | NS | 0.0002 | 0.0002 | ||
| Absence of a fee for reporting ADRs | 79 (12.01)/ 66 (15.09) | PL | 46.09 * | 34.20 | 11.90 | 7.81 | 71.88 ** | 25.00 | 3.12 | 41.35 | 58.65 | 37.55 ^ | 31.96 | 12.87 | 17.62 |
| EG | 40.09 a | 28.12 | 10.65 | 21.14 | 41.65 d | 22.12 | 36.23 | 61.61 f | 38.39 | 37.34 ^ | 31.92 ^ | 1.76 | 28.98 ^ | ||
| p-value | NS | NS | NS | 0.0208 | 0.0002 | NS | <0.0001 | 0.0151 | 0.0151 | NS | NS | 0.0131 | NS | ||
| Level of knowledge makes it difficult to decide whether an ADR has occurred | 54 (8.25)/ 39 (8.98) | PL | 38.09 * | 37.15 | 18.78 | 5.98 | 43.12 ** | 37.89 | 18.99 | 38.00 f | 62.00 | 43.09 ^ | 29.03 ^ | 7.37 | 20.51 ^ |
| EG | 38.09 a | 32.27 | 10.00 | 19.64 | 48.76 ** | 29.09 | 22.15 | 62.77 f | 37.23 | 52.08 # ^ | 26.77 # | 18.09 # | 3.06 | ||
| p-value | NS | NS | NS | 0.0432 | NS | NS | NS | 0.0183 | 0.0183 | NS | NS | NS | 0.0141 | ||
| Do not feel the need to report reactions reported by patients | 36 (5.55)/14 (3.09) | PL | 12.41 | 19.57 | 38.04 g | 29.98 | 21.11 ** | 31.31 | 47.58 | 58.17 | 41.83 | 27.15 | 12.38 | 41.23 & | 19.24 |
| EG | 15.49 | 21.31 | 29.12 | 34.08 g | 37.10 | 25.15 | 37.75 | 49.03 | 50.97 | 3.69 | 29.12 $ | 33.43 $ | 33.76 $ | ||
| p-value | NS | NS | NS | NS | NS | NS | NS | NS | NS | NS | NS | NS | NS | ||
| Physicians’ yellow cards not available when needed | 52 (7.92)/30 (6.79) | PL | 42.01 * | 33.23 | 18.78 | 5.98 | 43.12 ** | 37.89 | 18.99 | 48.12 | 51.88 | 43.09 ^ | 29.03 ^ | 7.37 | 20.51 ^ |
| EG | 34.44 | 38.76 | 10.16 | 16.64 | 48.76 ** | 29.09 | 22.15 | 62.77 f | 37.23 | 52.08 # | 26.77 # | 18.09 # | 3.06 | ||
| p-value | NS | NS | NS | NS | NS | NS | NS | NS | NS | NS | NS | NS | 0.0289 | ||
| Activities | |||||||||||||||
| Strengthen training program on ADR reporting | 138 (21.07)/ 86 (19.54) | PL | 39.10 a | 25.43 | 15.35 | 20.12 | 39.76 | 30.44 | 29.80 | 47.43 | 37.34 | 29.97 # | 34.12 # | 30.10 # | 5.81 |
| EG | 13.62 | 23.13 | 23.98 | 39.27 g | 33.10 | 37.32 | 29.58 | 61.77 f | 38.23 | 40.09 ^ | 28.12 ^ | 10.65 | 21.14 | ||
| p-value | <0.0001 | NS | NS | 0.0018 | NS | NS | NS | 0.0365 | NS | NS | NS | 0.0007 | 0.0005 | ||
| ADR reporting should be compulsory in-service training | 157 (23.96)/ 93 (21.27) | PL | 36.41 a | 29.52 | 12.09 | 21.98 | 39.38 | 21.30 | 39.32 | 41.43 | 58.57 | 33.55 | 25.00 | 22.14 | 19.31 |
| EG | 39.59 a | 29.31 | 9.12 | 21.98 | 53.34 ** | 33.90 | 11.76 | 66.06 f | 33.94 | 33.76 # | 30.12 # | 32.43 # | 3.69 | ||
| p-value | NS | NS | NS | NS | 0.0318 | 0.0261 | <0.0001 | 0.0002 | 0.0002 | NS | NS | NS | 0.0005 | ||
| Institutional role should be more active | 240 (36.65)/ 134 (30.45) | PL | 14.77 | 15.88 | 51.45 g | 17.09 | 10.87 ** | 32.15 | 56.98 | 73.98 f | 26.02 | 44.98 ^ | 31.09 ^ | 3.49 | 20.44 ^ |
| EG | 14.50 | 13.46 | 29.04 | 43.00 g | 12.79 ** | 39.90 | 47.31 | 57.22 | 42.78 | 38.86 ^ | 29.49 | 13.60 | 18.05 | ||
| p-value | NS | NS | <0.0001 | <0.0001 | NS | NS | NS | 0.0009 | 0.0009 | NS | NS | 0.0003 | 0.5765 | ||
| Report forms should be included in prescribing pad | 45 (6.88)/ 54 (12.31) | PL | 9.93 | 12.12 | 29.51 | 48.44 g | 23.51 | 10.30 | 66.19 d | 56.88 | 43.12 | 12.17 | 17.88 | 37.51 $ | 32.44 |
| EG | 19.74 | 18.06 | 25.66 | 36.54 h | 8.57 ** | 25.43 | 66.00 | 63.09 | 36.91 | 10.90 | 10.12 | 42.10 $ & | 36.88 & $ | ||
| p-value | NS | NS | NS | NS | 0.0401 | 0.0538 | NS | NS | NS | NS | NS | NS | NS | ||
| An uncomplicated reporting system with quick feedback | 25 (3.74)/ 47 (10.81) | PL | 50.41 h | 8.52 | 19.09 | 21.98 | 39.38 d | 21.30 | 39.32 d | 41.43 | 58.57 | 32.55 | 33.00 | 15.15 | 19.31 |
| EG | 34.59 j | 25.31 | 18.12 | 21.98 | 53.34 ** | 33.90 | 11.76 | 66.06 f | 33.94 | 33.76 # | 30.12 # | 32.43 # | 3.69 | ||
| p-value | NS | NS | NS | NS | NS | NS | 0.0066 | 0.0441 | 0.0441 | NS | NS | NS | 0.0283 | ||
| Exercises should be included in undergraduate examination | 51 (7.70)/ 25 (5.62) | PL | 16.90 | 2.12 | 45.10 h | 35.88 h | 12.10 ** | 36.39 | 51.51 | 61.09 f | 38.91 | 42.15 # | 38.12 # | 11.92 | 7.81 |
| EG | 13.17 | 10.88 | 43.51 h | 32.44 h | 18.37 ** | 29.03 | 52.60 | 66.43 f | 33.57 | 40.09 ^ | 28.12 ^ | 10.65 | 21.14 | ||
| p-value | NS | NS | NS | NS | NS | NS | NS | NS | NS | NS | NS | NS | NS | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kopciuch, D.; Kamal, N.N.; Kamal, N.N.; Hamdy, N.A.; Paczkowska, A.; Zaprutko, T.; Ratajczak, P.; Fliciński, J.; Kus, K.; Nowakowska, E. Neurologists’ Knowledge, Practice, and Attitudes towards Pharmacovigilance and Adverse Drug Reactions Reporting Process in Epileptic Patients—Comparative Analysis from Poland and Egypt. Int. J. Environ. Res. Public Health 2022, 19, 4169. https://doi.org/10.3390/ijerph19074169
Kopciuch D, Kamal NN, Kamal NN, Hamdy NA, Paczkowska A, Zaprutko T, Ratajczak P, Fliciński J, Kus K, Nowakowska E. Neurologists’ Knowledge, Practice, and Attitudes towards Pharmacovigilance and Adverse Drug Reactions Reporting Process in Epileptic Patients—Comparative Analysis from Poland and Egypt. International Journal of Environmental Research and Public Health. 2022; 19(7):4169. https://doi.org/10.3390/ijerph19074169
Chicago/Turabian StyleKopciuch, Dorota, Nashwa Nabil Kamal, Nashaat Nabil Kamal, Nermin Aly Hamdy, Anna Paczkowska, Tomasz Zaprutko, Piotr Ratajczak, Jędrzej Fliciński, Krzysztof Kus, and Elżbieta Nowakowska. 2022. "Neurologists’ Knowledge, Practice, and Attitudes towards Pharmacovigilance and Adverse Drug Reactions Reporting Process in Epileptic Patients—Comparative Analysis from Poland and Egypt" International Journal of Environmental Research and Public Health 19, no. 7: 4169. https://doi.org/10.3390/ijerph19074169