
Generativity and Gendered Pathways to Health: The Role of Human, Social, and Financial Capital Past Mid-Life

 , ,
, ,
Abstract
:1. Introduction
1.1. Capital Drivers of Generativity
1.2. Impacts of Generativity
1.3. Gendered Pathway to Generativity
1.4. The Present Study
2. Materials and Methods
2.1. Data and Sample
2.2. Measures
2.2.1. Human, Social, and Financial Capital
2.2.2. Generativity
2.2.3. Physical Health
2.2.4. Mental Health
2.2.5. Covariates
2.3. Analyses
3. Results
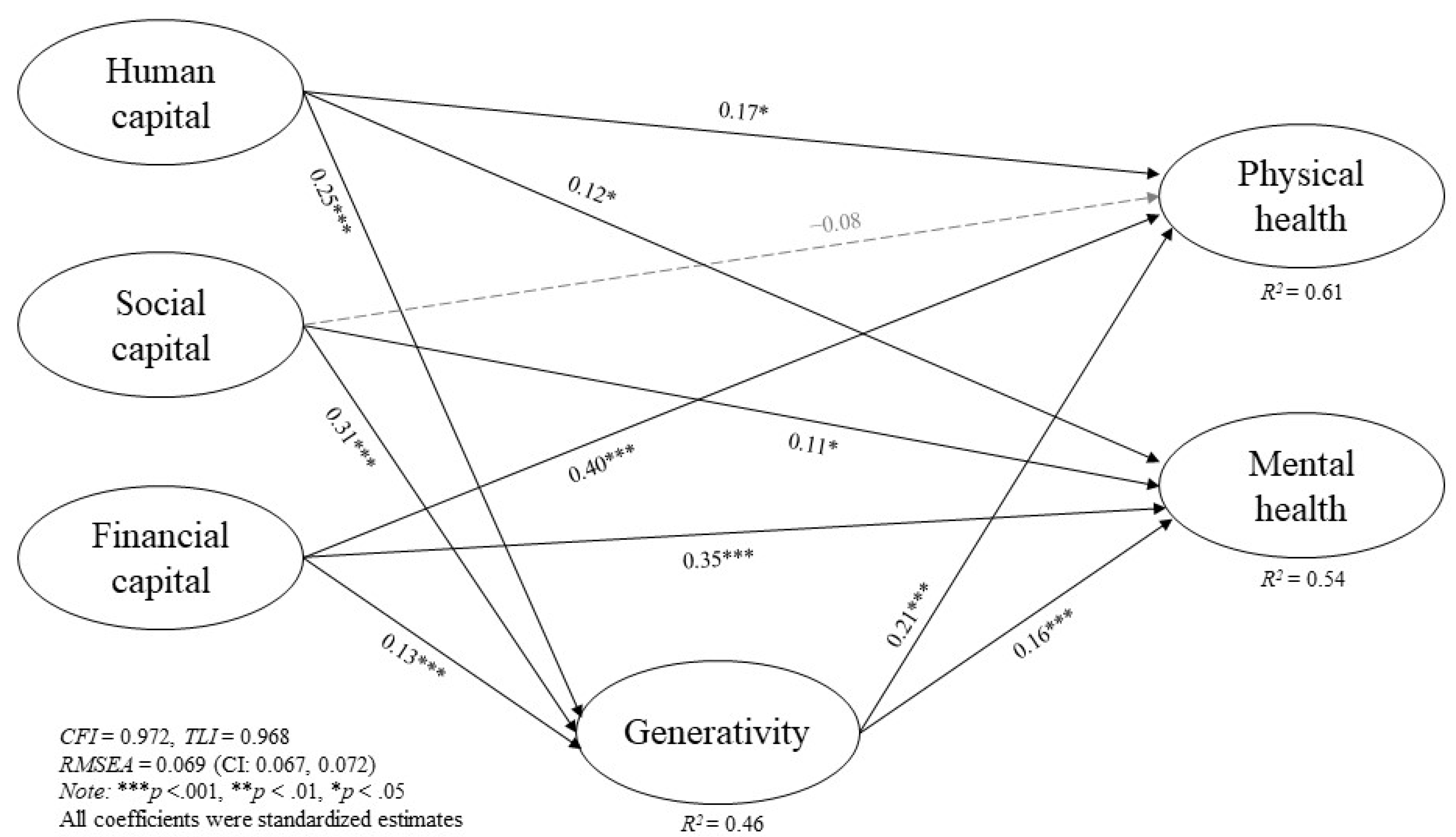
3.1. Path Analyses
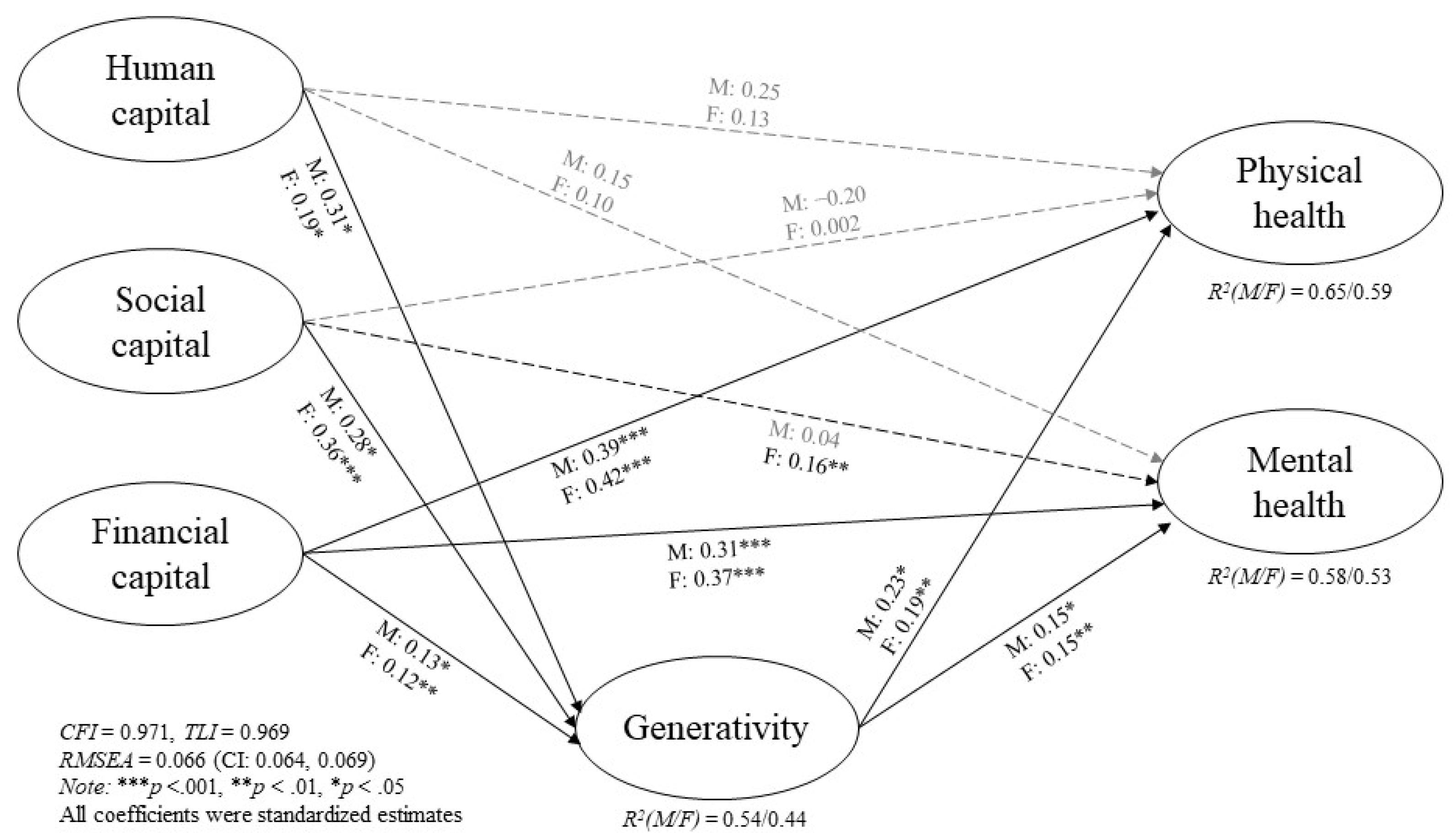
3.2. Gendered Differences
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McAdams, D.P.; de St. Aubin, E.D.; Logan, R.L. Generativity among young, midlife, and older adults. Psychol. Aging 1993, 8, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Grossman, M.R.; Gruenewald, T.L. Failure to meet generative self-expectations is linked to poorer cognitive-affective well-being. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2020, 75, 792–801. [Google Scholar] [CrossRef] [PubMed]
- Villar, F. Successful ageing and development: The contribution of generativity in older age. Ageing Soc. 2012, 32, 1087–1105. [Google Scholar] [CrossRef] [Green Version]
- Kotre, J.N.; Kotre, J. Outliving the Self: Generativity and the Interpretation of Lives; Johns Hopkins University Press: Baltimore, MD, USA, 1984. [Google Scholar]
- Gruenewald, T.L.; Liao, D.H.; Seeman, T.E. Contributing to others, contributing to oneself: Perceptions of generativity and health in later life. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2012, 67, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Nelson, N.A.; Bergeman, C.S. Development of generative concern across mid- to later life. Gerontologist 2021, 61, 430–438. [Google Scholar] [CrossRef] [PubMed]
- McAdams, D.P.; de St Aubin, E. A theory of generativity and its assessment through self-report, behavioral acts, and narrative themes in autobiography. J. Personal. Soc. Psychol. 1992, 62, 1003–1015. [Google Scholar] [CrossRef]
- Kim, S.; Chee, K.H.; Gerhart, O. Redefining generativity: Through life course and pragmatist lenses. Sociol. Compass 2017, 11, e12533. [Google Scholar] [CrossRef]
- Hung, N.; Chen, Y.-C.; Yung, R.M.P.C.; Kwan, M.S.M.; To, A.K.Y.; Ellmon, S.M.F.; Chan, C.L.W. Generativity in later-life: The interplay between retirement status and human, social, and financial capital. Manuscr. Submitt. Publ. 2021. [Google Scholar]
- McNamara, T.K.; Gonzales, E. Volunteer Transitions Among Older Adults: The Role of Human, Social, and Cultural Capital in Later Life. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2011, 66, 490–501. [Google Scholar] [CrossRef] [Green Version]
- Halvorsen, C.J.; Chen, Y.C. The diversity of interest in later-life entrepreneurship: Results from a nationally representative survey of Americans aged 50 to 70. PLoS ONE 2019, 14, e0217971. [Google Scholar] [CrossRef]
- Becker, G.S. Human capital and the economy. Proc. Am. Philos. Soc. 1992, 136, 85–92. [Google Scholar]
- Coleman, J.S. Social capital in the creation of human capital. Am. J. Sociol. 1988, 94, S95–S120. [Google Scholar] [CrossRef]
- Choi, N.G.; Kim, J. The effect of time volunteering and charitable donations in later life on psychological wellbeing. Ageing Soc. 2011, 31, 590–610. [Google Scholar] [CrossRef]
- Bourdieu, P. The forms of capital. In Handbook of Theory and Research for the Sociology of Education; Richardson, J., Ed.; Greenwood: Westport, CT, USA, 1986; pp. 241–258. [Google Scholar]
- Xiao, J.J.; Chen, C.; Chen, F. Financial capability and financial satisfaction. Soc. Indic. Res. 2014, 118, 415–432. [Google Scholar] [CrossRef]
- Cheng, S.T.; Chan, W.; Chan, A.C.M. Older people’s realisation of generativity in a changing society: The case of Hong Kong. Ageing Soc. 2008, 28, 609–627. [Google Scholar] [CrossRef] [Green Version]
- Cheng, S.T. Generativity in later life: Perceived respect from younger generations as a determinant of goal disengagement and psychological well-being. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2009, 64, P45–P54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serrat, R.; Villar, F.; Giulianib, M.F.; Zacares, J.J. Older people’s participation in political organizations: The role of generativity and its impact on well-being. Educ. Gerontol. 2017, 43, 128–138. [Google Scholar] [CrossRef]
- Carlson, M.C.; Seeman, T.; Fried, L.P. Importance of generativity for healthy aging in older women. Aging Clin. Exp. Res. 2000, 12, 132–140. [Google Scholar] [CrossRef]
- Gruenewald, T.L.; Karlamangla, A.S.; Greendale, G.A.; Singer, B.H.; Seeman, T.E. Feelings of usefulness to others, disability, and mortality in older adults: The MacArthur study of successful aging. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2007, 62, P28–P37. [Google Scholar] [CrossRef] [Green Version]
- Homan, K.J.; Greenberg, J.S.; Mailick, M.R. Generativity and well-being of midlife and aging parents with children with developmental or mental health problems. Res. Aging 2020, 42, 95–104. [Google Scholar] [CrossRef]
- Ackerman, S.; Zuroff, D.C.; Moskowitz, D.S. Generativity in midlife and young adults: Links to agency, communion and subjective well-being. Int. J. Aging Hum. Dev. 2000, 50, 17–41. [Google Scholar] [CrossRef] [PubMed]
- Weiss, D.; Kunzmann, U. Longitudinal changes in subjective social status are linked to changes in positive and negative affect in midlife, but not in later adulthood. Psychol. Aging 2020, 35, 937–947. [Google Scholar] [CrossRef] [PubMed]
- Maselko, J.; Sebranek, M.; Mun, M.H.; Perera, B.; Ahs, J.; Ostbye, T. Contribution of generative leisure activities to cognitive function in elderly Sri Lankan adults. J. Am. Geriatr. Soc. 2014, 62, 1707–1713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.C.; Putnam, M.; Lee, Y.S.; Morrow-Howell, N. Activity patterns and health outcomes in later life: The role of nature of engagement. Gerontologist 2019, 59, 698–708. [Google Scholar] [CrossRef]
- Fried, L.P.; Carlson, M.C.; Freedman, M.; Frick, K.D.; Glass, T.A.; Hill, J.; McGill, S.; Rebok, G.W.; Seeman, T.; Tielsch, J.; et al. A social model for health promotion for an aging population: Initial evidence on the experience corps model. J. Urban Health 2004, 81, 64–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Østbye, T.; Clancy, S.; Stankevitz, K.; Malhotra, R.; Ogundare, O.; Shah, V.; Pati, S.; Boddicker-Young, P.; Maselko, J. Generativity among elderly in a rural area of Maharashtra, India: Correlates and relationship with quality of life approved. Asia Pac. J. Public Health 2018, 30, 276–285. [Google Scholar] [CrossRef]
- Karacan, E. Timing of parenthood and generativity development: An examination of age and gender effects in Turkish sample. J. Adult Dev. 2014, 21, 207–215. [Google Scholar] [CrossRef]
- Peterson, B.E.; Stewart, A.J. Generativity and social motives in young adults. J. Personal. Soc. Psychol. 1993, 65, 186–198. [Google Scholar] [CrossRef]
- Huta, V.; Zuroff, D.C. Examining mediators of the link between generativity and well-being. J. Adult Dev. 2007, 14, 47–52. [Google Scholar] [CrossRef]
- Moieni, M.; Irwin, M.R.; Seeman, T.E.; Robles, T.F.; Lieberman, M.D.; Breen, E.C.; Okimoto, S.; Lengacher, C.; Arevalo, J.M.G.; Olmstea, R.; et al. Feeling needed: Effects of a randomized generativity intervention on well-being and inflammation in older women. Brain Behav. Immun. 2020, 84, 97–105. [Google Scholar] [CrossRef]
- Hunsaker, A.; Hargittai, E.A. Review of Internet use among older adults. New Media Soc. 2018, 20, 3937–3954. [Google Scholar] [CrossRef]
- Lubben, J.; Blozik, E.; Gillmann, G.; Iliffe, S.; von Renteln-Kruse, W.; Beck, J.C.; Stuck, A.E. Performance of an abbreviated version of the Lubben Social Network Scale among three European community-dwelling older adult populations. Gerontologist 2006, 46, 503–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hira, T.K.; Mugenda, O.M. Predictors of financial satisfaction: Differences between retirees and non-retirees. J. Financ. Couns. Plan. 1998, 9, 75–84. [Google Scholar]
- Villar, F.; Serrat, R.; Pratt, M.W. Older age as a time to contribute: A scoping review of generativity in later life. Ageing Soc. 2021, 1–22. [Google Scholar] [CrossRef]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Gonzales, E.; Matz-Costa, C.; Morrow-Howell, N. Increasing opportunities for the productive engagement of older adults: A response to population aging. Gerontologist 2015, 55, 252–261. [Google Scholar] [CrossRef]
- Tabuchi, M.; Nakagawa, T.; Miura, A.; Gondo, Y. Generativity and interaction between the old and young: The role of perceived respect and perceived rejection. Gerontologist 2015, 55, 537–547. [Google Scholar] [CrossRef] [Green Version]
- Carragher, L. Opportunities for generativity in later life for older men. Aust. J. Adult Learn. 2017, 57, 351–365. [Google Scholar]
- Hwang, T.-J.; Rabheru, K.; Peisah, C.; Reichman, W.; Ikeda, M. Loneliness and social isolation during the COVID-19 pandemic. Int. Psychogeriatr. 2020, 32, 1217–1220. [Google Scholar] [CrossRef]
- Robb, C.E.; de Jager, C.A.; Ahmadi-Abhari, S.; Giannakopoulou, P.; Udeh-Momoh, C.; McKeand, J.; Price, G.; Car, J.; Majeed, A.; Ward, H.; et al. Associations of Social Isolation with Anxiety and Depression During the Early COVID-19 Pandemic: A Survey of Older Adults in London, UK. Front. Psychiatry 2020, 11, 991. [Google Scholar] [CrossRef] [PubMed]
- Pietrabissa, G.; Simpson, S.G. Psychological Consequences of Social Isolation During COVID-19 Outbreak. Front. Psychol. 2020, 11, 2201. [Google Scholar] [CrossRef] [PubMed]
- Gruenewald, T.L.; Tanner, E.K.; Fried, L.P.; Carlson, M.C.; Xue, Q.-L.; Parisi, J.M.; Rebok, G.W.; Yarnell, L.M.; Seeman, T.E. The Baltimore experience corps trial: Enhancing generativity via intergenerational activity engagement in later life. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2016, 71, 661–670. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Whole | Men | Women | χ2 or t |
|---|---|---|---|---|
| M (SD) or % | M (SD) or % | M (SD) or % | ||
| Human capital (HC) | ||||
| Education attainment (Above college) | 57.53% | 58.49% | 56.91% | χ2 = 0.27 |
| Continuing education (yes) | 57.08% | 48.62% | 62.56% | χ2 = 20.96 *** |
| Social capital (SC) | ||||
| Engaged in community services (yes) | 63.93% | 60.78% | 65.97% | χ2 = 3.09 |
| Engaged in educational, cultural or professional association (yes) | 57.08% | 55.50% | 58.10% | χ2 = 0.73 |
| Whether voted (yes) | 85.57% | 84.86% | 86.03% | χ2 = 0.29 |
| Providing care for vulnerable groups (yes) | 70.87% | 69.95% | 71.47% | χ2 = 0.29 |
| Frequency of social contact with friends or families ‡ | 1.94 (0.97) | 1.79 (1.00) | 2.05 (0.93) | t = −4.42 *** |
| Social network (Lubben social network scale) | 12.63 (6.45) | 11.25 (6.29) | 13.52 (6.40) | t = −5.80 *** |
| Financial capital (FC, Financial situation scale) | 12.57 (4.48) | 12.49 (4.63) | 12.62 (4.38) | t = −0.47 |
| Generativity (GEN, Loyola generativity scale) | 8.19 (2.88) | 7.72 (2.95) | 8.50 (2.82) | t = −4.41 *** |
| Physical health (PH) | ||||
| Self-rated health | 6.79 (1.94) | 6.50 (1.97) | 6.87 (1.91) | t = −1.88 |
| Mobility limitation † | 1.27 (0.60) | 1.29 (0.66) | 1.25 (0.56) | t = 0.95 |
| Mental health (MH, WHO-5) | 11.96 (5.44) | 11.61 (5.47) | 12.19 (5.42) | t = −1.72 |
| Covariates | ||||
| Gender (woman) | 60.69% | -- | -- | -- |
| Age (age 45–55) | 29.58% | 23.85% | 33.28% | χ2 = 16.36 *** |
| 55–65 | 46.98% | 47.48% | 46.66% | |
| 65+ | 23.44% | 28.67% | 20.06% | |
| Marital status (married) | 60.60% | 70.87% | 53.94% | χ2 = 31.78 *** |
| Employment (working) | 44.63% | 44.27% | 44.87% | χ2 = 0.04 |
| Income ‡ | 2.59 (1.49) | 2.68 (1.53) | 2.54 (1.46) | t = 1.58 |
| Assets ‡ | 2.74 (1.29) | 2.70 (1.32) | 2.76 (1.28) | t = −0.80 |
| Financial ownerships | 2.30 (1.65) | 2.04 (1.67) | 2.47 (1.62) | t = −4.14 *** |
| Number of chronic diseases † | 0.75 (0.93) | 0.92 (0.98) | 0.63 (0.87) | t = 4.99 *** |
| Paths | Total Sample | Men | Women |
|---|---|---|---|
| Direct effect | β | β | β |
| HC → PH | 0.17 * | 0.25 * | 0.12 |
| HC → MH | 0.11 * | 0.15 * | 0.1 |
| SC → PH | −0.08 | −0.20 | 0.002 |
| SC → MH | 0.11 * | 0.04 | 0.16 ** |
| FC → PH | 0.40 *** | 0.39 *** | 0.42 *** |
| FC → MH | 0.35 *** | 0.31 *** | 0.37 *** |
| Indirect effect | |||
| HC → GEN → PH | 0.05 ** | 0.07 * | 0.04 † |
| (CI: 0.03, 0.10) | (CI: 0.03, 0.22) | (CI: 0.00, 0.09) | |
| HC → GEN → MH | 0.04 ** | 0.05 * | 0.03 † |
| (CI: 0.02, 0.08) | (CI: 0.01, 0.18) | (CI: 0.00, 0.07) | |
| SC → GEN → PH | 0.07 *** | 0.06 | 0.07 *** |
| (CI: 0.03, 0.11) | (CI: −0.01, 0.14) | (CI: 0.02, 0.13) | |
| SC → GEN → MH | 0.05 *** | 0.04 | 0.05 ** |
| (CI: 0.02, 0.08) | (CI: −0.01, 0.11) | (CI: 0.02, 0.10) | |
| FC → GEN → PH | 0.03 * | 0.03 | 0.02 † |
| (CI: 0.01, 0.06) | (CI: 0.00, 0.08) | (CI: 0.00, 0.06) | |
| FC → GEN → MH | 0.02 * | 0.02 | 0.02 † |
| (CI: 0.01, 0.04) | (CI: 0.00, 0.07) | (CI: 0.00, 0.04) | |
| Relative importance of indirect path | % | % | % |
| HC → PH + HC → GEN → PH | 100.00 ‡ | 100.00 ‡ | 100 |
| HC → PH | 77.27 ‡ | 78.12 ‡ | 75 |
| HC → GEN → PH | 22.78 ‡ | 21.88 ‡ | 25 |
| HC → MH + HC → GEN → MH | 100.00 ‡ | 100.00 ‡ | 100 |
| HC → MH | 73.33 ‡ | 75.00 ‡ | 76.92 |
| HC → GEN → MH | 26.67 ‡ | 25.00 ‡ | 23.08 |
| SC → PH + SC → GEN → PH | 100 | 100 | 100 |
| SC → PH | -- | -- | 0 |
| SC → GEN → PH | -- | -- | 100.00 ‡ |
| SC → MH + SC → GEN → MH | 100.00 ‡ | 100 | 100.00 ‡ |
| SC → MH | 68.75 ‡ | 50 | 76.19 ‡ |
| SC → GEN → MH | 31.25 ‡ | 50 | 23.81 ‡ |
| FC → PH + FC → GEN → PH | 100.00 ‡ | 100.00 ‡ | 100.00 ‡ |
| FC → PH | 93.02 ‡ | 92.86 ‡ | 95.45 ‡ |
| FC → GEN → PH | 6.98 ‡ | 7.14 | 4.55 |
| FC → MH + FC → GEN → MH | 100.00 ‡ | 100.00 ‡ | 100.00 ‡ |
| FC → MH | 94.59 ‡ | 93.94 ‡ | 94.87 ‡ |
| FC → GEN → MH | 5.41 ‡ | 6.06 | 5.13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-C.; Hung, N.; Lau, B.H.P.; Choy Yung, R.M.P.; Fung, E.S.M.; Chan, C.L.W. Generativity and Gendered Pathways to Health: The Role of Human, Social, and Financial Capital Past Mid-Life. Int. J. Environ. Res. Public Health 2022, 19, 4956. https://doi.org/10.3390/ijerph19094956
Chen Y-C, Hung N, Lau BHP, Choy Yung RMP, Fung ESM, Chan CLW. Generativity and Gendered Pathways to Health: The Role of Human, Social, and Financial Capital Past Mid-Life. International Journal of Environmental Research and Public Health. 2022; 19(9):4956. https://doi.org/10.3390/ijerph19094956
Chicago/Turabian StyleChen, Yu-Chih, Natalee Hung, Bobo H. P. Lau, Rebecca M. P. Choy Yung, Ellmon S. M. Fung, and Cecilia L. W. Chan. 2022. "Generativity and Gendered Pathways to Health: The Role of Human, Social, and Financial Capital Past Mid-Life" International Journal of Environmental Research and Public Health 19, no. 9: 4956. https://doi.org/10.3390/ijerph19094956
APA StyleChen, Y.-C., Hung, N., Lau, B. H. P., Choy Yung, R. M. P., Fung, E. S. M., & Chan, C. L. W. (2022). Generativity and Gendered Pathways to Health: The Role of Human, Social, and Financial Capital Past Mid-Life. International Journal of Environmental Research and Public Health, 19(9), 4956. https://doi.org/10.3390/ijerph19094956