
Barriers and Motivations to Provide Dental Care to Adult Patients with Movement Disorders


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample and Data Collection
2.2. Survey Design
2.3. Data Analysis
3. Results
3.1. Participants’ Demographics and Professional Backgrounds
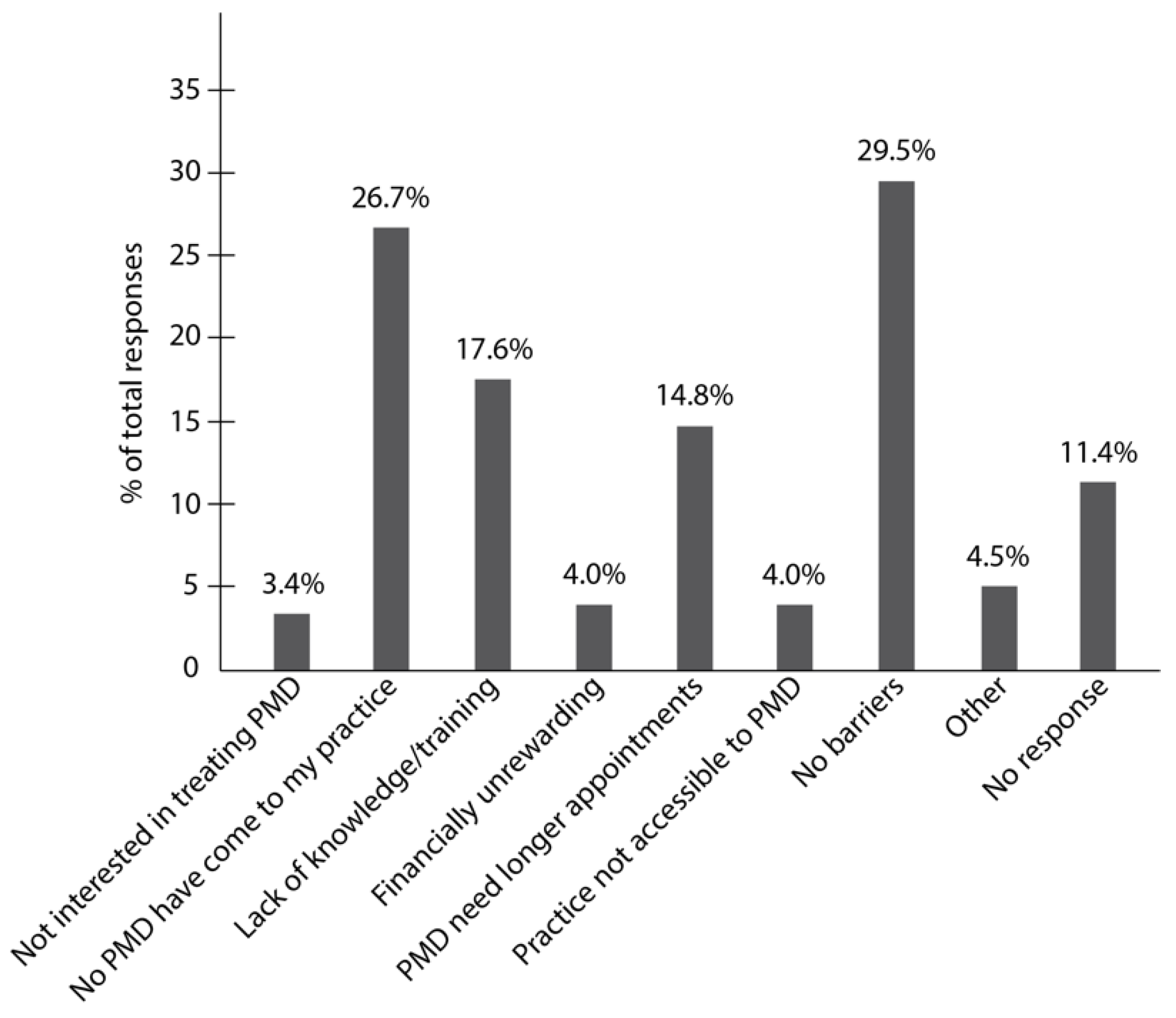
3.2. Barriers to Treating Patients with Movement Disorders
3.3. Motivations to Treat Adult Patients with Movement Disorders
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, A.; Gilbert, R.M. Epidemiology of Parkinson Disease. Neurol. Clin. 2016, 34, 955–965. [Google Scholar] [CrossRef] [PubMed]
- Polymeropoulos, M.H.; Lavedan, C.; Leroy, E.; Ide, S.E.; Dehejia, A.; Dutra, A.; Pike, B.; Root, H.; Rubenstein, J.; Boyer, R.; et al. Mutation in the ⍺-Synuclein Gene Identified in Families with Parkinson’s Disease. Science 1997, 276, 2045–2047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spillantini, M.; Schmidt, M.; Lee, V.; Trojanowski, J.; Jakes, R.; Goedert, M. Alpha-Synuclein in Lewy Bodies. Nature 1997, 388, 839–840. [Google Scholar] [CrossRef] [PubMed]
- Poewe, W.; Seppi, K.; Tanner, C.M.; Halliday, G.M.; Volkmann, J.; Schrag, A.; Lang, A.E. Parkinson Disease. Nat. Rev. Dis. Primers 2017, 3, 17013. [Google Scholar] [CrossRef]
- MacDonald, M.E.; Barnes, G.; Srinidhi, J.; Duyao, M.P.; Ambrose, C.M.; Myers, R.H.; Gray, J.; Conneally, P.M.; Young, A.; Penney, J. Gametic but Not Somatic Instability of CAG Repeat Length in Huntington’s Disease. J. Med. Genet. 1993, 30, 982–986. [Google Scholar] [CrossRef] [Green Version]
- Baig, S.S.; Strong, M.; Quarrell, O.W. The Global Prevalence of Huntington’s Disease: A Systematic Review and Discussion. Neurodegener. Dis. Manag. 2016, 6, 331–343. [Google Scholar] [CrossRef] [Green Version]
- Auffret, M.; Meuric, V.; Boyer, E.; Bonnaure-Mallet, M.; Vérin, M. Oral Health Disorders in Parkinson’s Disease: More than Meets the Eye. J. Parkinsons Dis. 2021, 11, 1507–1535. [Google Scholar] [CrossRef]
- Rozas, N.S.; Sadowsky, J.M.; Jones, D.J.; Jeter, C.B. Incorporating Oral Health into Interprofessional Care Teams for Patients with Parkinson’s Disease. Parkinsonism Relat. Disord. 2017, 43, 9–14. [Google Scholar] [CrossRef]
- Bollero, P.; Franco, R.; Cecchetti, F.; Miranda, M.; Barlattani, A.J.; Dolci, A.; Ottria, L. Oral Health and Implant Therapy in Parkinson’s Patients: Review. Oral Implant. 2017, 10, 105–111. [Google Scholar] [CrossRef]
- Rozas, N.S.; Tribble, G.D.; Jeter, C.B. Oral Factors That Impact the Oral Microbiota in Parkinson’s Disease. Microorganisms 2021, 9, 1616. [Google Scholar] [CrossRef]
- Shen, L. Gut, Oral and Nasal Microbiota and Parkinson’s Disease. Microb. Cell Fact. 2020, 19, 50. [Google Scholar] [CrossRef] [PubMed]
- Rada, R.E. Comprehensive Dental Treatment of a Patient with Huntington’s Disease: Literature Review and Case Report. Spec. Care Dentist. 2008, 28, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Saft, C.; Andrich, J.E.; Müller, T.; Becker, J.; Jackowski, J. Oral and Dental Health in Huntington’s Disease—An Observational Study. BMC Neurol. 2013, 13, 114. [Google Scholar] [CrossRef] [PubMed]
- Batista, L.M.; Portela de Oliveira, M.T.; Magalhaes, W.B.; Bastos, P.L. Oral Hygiene in Patients with Parkinson’s Disease. RI Med. J. 2015, 98, 35–37. [Google Scholar]
- Bots-VantSpijker, P.C.; Vanobbergen, J.N.O.; Schols, J.M.G.A.; Schaub, R.M.H.; Bots, C.P.; de Baat, C. Barriers of Delivering Oral Health Care to Older People Experienced by Dentists: A Systematic Literature Review. Community Dent. Oral Epidemiol. 2014, 42, 113–121. [Google Scholar] [CrossRef]
- Lyu, J.; Zhang, X.; Nie, X.; Wei, L.; He, H. A Cross-Sectional Study of the Knowledge, Attitudes, and Behaviors of Obstetricians, Gynecologists, and Dentists Regarding Oral Health Care during Pregnancy. Ann. Palliat. Med. 2021, 10, 4242–4251. [Google Scholar] [CrossRef]
- Lim, M.A.W.T.; Liberali, S.A.C.; Calache, H.; Parashos, P.; Borromeo, G.L. Perceived Barriers Encountered by Oral Health Professionals in the Australian Public Dental System Providing Dental Treatment to Individuals with Special Needs. Spec. Care Dent. 2021, 41, 381–390. [Google Scholar] [CrossRef]
- D’Addazio, G.; Santilli, M.; Sinjari, B.; Xhajanka, E.; Rexhepi, I.; Mangifesta, R.; Caputi, S. Access to Dental Care-A Survey from Dentists, People with Disabilities and Caregivers. Int. J. Environ. Res. Public Health 2021, 18, 1556. [Google Scholar] [CrossRef]
- Krishnan, L.; Iyer, K.; Madan Kumar, P.D. Barriers to Utilisation of Dental Care Services among Children with Special Needs: A Systematic Review. Indian J. Dent. Res. 2020, 31, 486–493. [Google Scholar] [CrossRef]
- Hovden, E.S.; Ansteinsson, V.E.; Klepaker, I.V.; Widström, E.; Skudutyte-Rysstad, R. Dental Care for Drug Users in Norway: Dental Professionals’ Attitudes to Treatment and Experiences with Interprofessional Collaboration. BMC Oral Health 2020, 20, 299. [Google Scholar] [CrossRef]
- American Dental Association Sypply and Profile of Dentists. Available online: https://www.ada.org/en/science-research/health-policy-institute/data-center/supply-and-profile-of-dentists (accessed on 18 July 2021).
- Wong, A.; Itaya, L. Interdisciplinary Oral Health for Those with Special Health Care Needs. Dent. Clin. 2022, 66, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Freeman, R. Barriers to Accessing and Accepting Dental Care. Br. Dent. J. 1999, 187, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Devinsky, O.; Boyce, D.; Robbins, M.; Pressler, M. Dental Health in Persons with Disability. Epilepsy Behav. 2020, 110, 107174. [Google Scholar] [CrossRef] [PubMed]
- Friedlander, A.H.; Mahler, M.; Norman, K.M.; Ettinger, R.L. Parkinson Disease: Systemic and Orofacial Manifestations, Medical and Dental Management. J. Am. Dent. Assoc. 2009, 140, 658–669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gosnell, R.; Lazear, J.; Hemphill, J.C.; Dotson, D. Development of Guidelines for Improving Oral Health in Individuals with Parkinson’s Disease. Gerodontology 2019, 36, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Martimbianco, A.L.C.; Prosdocimi, F.C.; Anauate-Netto, C.; dos Santos, E.M.; Mendes, G.D.; Fragoso, Y.D. Evidence-Based Recommendations for the Oral Health of Patients with Parkinson’s Disease. Neurol. Ther. 2021, 10, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Jeter, C.B.; Rozas, N.S.; Sadowsky, J.M.; Jones, D.J. Parkinson’s Disease Oral Health Module: Interprofessional Coordination of Care. MedEdPORTAL 2018, 14, 10699. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| All (n = 176) | Have Treated PMD (n = 116) | Have Not Treated PMD (n = 60) | ||
|---|---|---|---|---|
| Gender N (%) | ||||
| Female | 48 (27.3) | 29 (25.0) | 19 (31.7) | |
| Male | 124 (70.4) | 85 (73.3) | 39 (65.0) | |
| NR | 2.3 (4.0) | 1.7 (2.0) | 3.3 (2.0) | |
| Age N (%) | ||||
| 21–50 years | 69 (39.2) | 42 (36.2) | 27 (45.0) | |
| >50 years | 103 (58.5) | 72 (62.1) | 31 (51.7) | |
| NR | 4 (2.3) | 2 (1.7) | 2 (3.3) | |
| Race/Ethnicity N (%) | ||||
| White | 106 (60.2) | 77 (66.4) | 29 (48.3) | |
| White Hispanic/Latino | 28 (15.9) | 11 (9.5) | 17 (28.3) | |
| Black | 7 (4.0) | 5 (4.3) | 2 (3.3) | |
| Black Hispanic/Latino | 3 (1.7) | 2 (1.7) | 1 (1.7) | |
| Asian | 25 (14.2) | 17 (14.7) | 8 (13.4) | |
| Other | 3 (1.7) | 2 (1.7) | 1 (1.7) | |
| NR | 4 (2.3) | 2 (1.7) | 2 (3.3) | |
| Continuing Education N (%) | ||||
| Geriatric Dentistry | 67 (38.0) | 49 (42.2) | 18 (30) | |
| Neurology Patient Dentistry | 15 (8.5) | 10 (8.6) | 5 (8.3) | |
| PMD Dentistry | 12 (6.8) | 9 (7.8) | 3 (5.0) | |
| Years of experience N (%) | ||||
| <5 Years | 24 (13.6) | 12 (10.3) | 12 (20.0) | |
| 6–10 Years | 7 (4.0) | 4 (3.5) | 3 (5.0) | |
| >10 Years | 143 (81.3) | 100 (86.2) | 43 (71.7) | |
| NR | 2 (1.1) | 0 | 2 (3.3) | |
| Type of practice N (%) | ||||
| Hospital based | 4 (2.3) | 3 (2.6) | 1 (1.7) | |
| University based | 4 (2.3) | 2 (1.7) | 2 (3.3) | |
| Individual | 120 (68.2) | 80 (69.0) | 40 (66.7) | |
| Small group practice | 34 (19.3) | 22 (19.0) | 12 (20.0) | |
| Large group practice | 7 (3.9) | 5 (4.3) | 2 (3.3) | |
| Other | 6 (3.4) | 3 (2.6) | 3 (5.0) | |
| PMD per month N (%) | ||||
| <10 | 102 (87.9) | |||
| 11–25 | 12 (10.3) | |||
| >25 | 2 (1.7) | |||
| Have Treated PMD (n = 116) | Have Not Treated PMD (n = 60) | |
|---|---|---|
| I am not interested in treating this patient population | 4 (3.4) | 2 (3.3) |
| No PMD have come to my practice | 14 (12.1) | 33 (55.0) * |
| My training is for a different patient population | 19 (16.4) | 12 (20.0) |
| It is financially unrewarding | 7 (6.0) | 0 |
| Patient appointments are longer than average | 25 (21.6) | 1 (1.7) * |
| My practice is not accessible to PMD | 5 (4.3) | 2 (3.32) |
| No barriers | 46 (39.7) | 6 (10.0) * |
| Other | 6 (5.2) | 3 (5.0) |
| None marked | 13 (11.2) | 7 (11.7) |
| Have Treated PMD (n = 116) | Have Not Treated PMD (n = 60) | |
|---|---|---|
| If I had more available time | 19 (16.4) | 8 (13.3) |
| If I had more available staff | 13 (11.2) | 8 (13.3) |
| If I had more available equipment | 21 (18.1) | 10 (16.7) |
| If I had the time to get training and education on the subject | 45 (38.8) | 23 (38.3) |
| If it would bring more income to my practice | 26 (22.4) | 6 (10) |
| If I were asked by a colleague to treat a PMD | 44 (37.9) | 13 (21.7) |
| If a family member or friend of mine had a MD | 37 (31.9) | 12 (20) |
| Other | 17 (14.7) | 5 (8.3) |
| None marked | 17 (14.7) | 16 (26.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rozas, N.S.; Strassner, H.D.; Sadowsky, J.M.; Jeter, C.B. Barriers and Motivations to Provide Dental Care to Adult Patients with Movement Disorders. Int. J. Environ. Res. Public Health 2022, 19, 5256. https://doi.org/10.3390/ijerph19095256
Rozas NS, Strassner HD, Sadowsky JM, Jeter CB. Barriers and Motivations to Provide Dental Care to Adult Patients with Movement Disorders. International Journal of Environmental Research and Public Health. 2022; 19(9):5256. https://doi.org/10.3390/ijerph19095256
Chicago/Turabian StyleRozas, Natalia S., Hillary D. Strassner, June M. Sadowsky, and Cameron B. Jeter. 2022. "Barriers and Motivations to Provide Dental Care to Adult Patients with Movement Disorders" International Journal of Environmental Research and Public Health 19, no. 9: 5256. https://doi.org/10.3390/ijerph19095256
APA StyleRozas, N. S., Strassner, H. D., Sadowsky, J. M., & Jeter, C. B. (2022). Barriers and Motivations to Provide Dental Care to Adult Patients with Movement Disorders. International Journal of Environmental Research and Public Health, 19(9), 5256. https://doi.org/10.3390/ijerph19095256