







Building Research Infrastructure: The Development of a Technical Assistance Group-Service Center at an RCMI

 ,
, 
Abstract
:1. Background
2. Methods
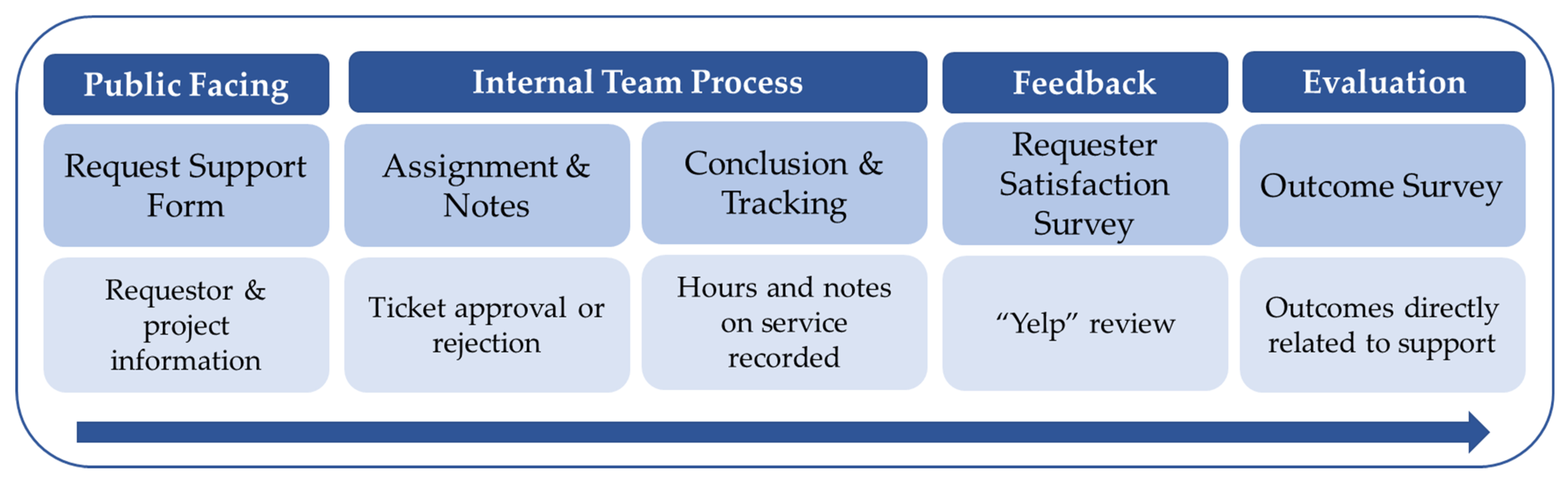
2.1. Technical Assistance Group-Service Center (TAG-SC) Development
2.1.1. Phase I: Initial Framework (Grant Years 1–3, 2017–2020)
Developing a Ticket System Using REDCap
2.1.2. Phase II: Pilot Year (Grant Year 4, 2020–2021)
2.1.3. Phase III: Year 1 of TAG-SC (Grant Year 5, 2021–2022)
2.2. Statistical Analyses
3. Results
3.1. Phase I: Initial Framework (Grant Years 1–3, 2017–2020)
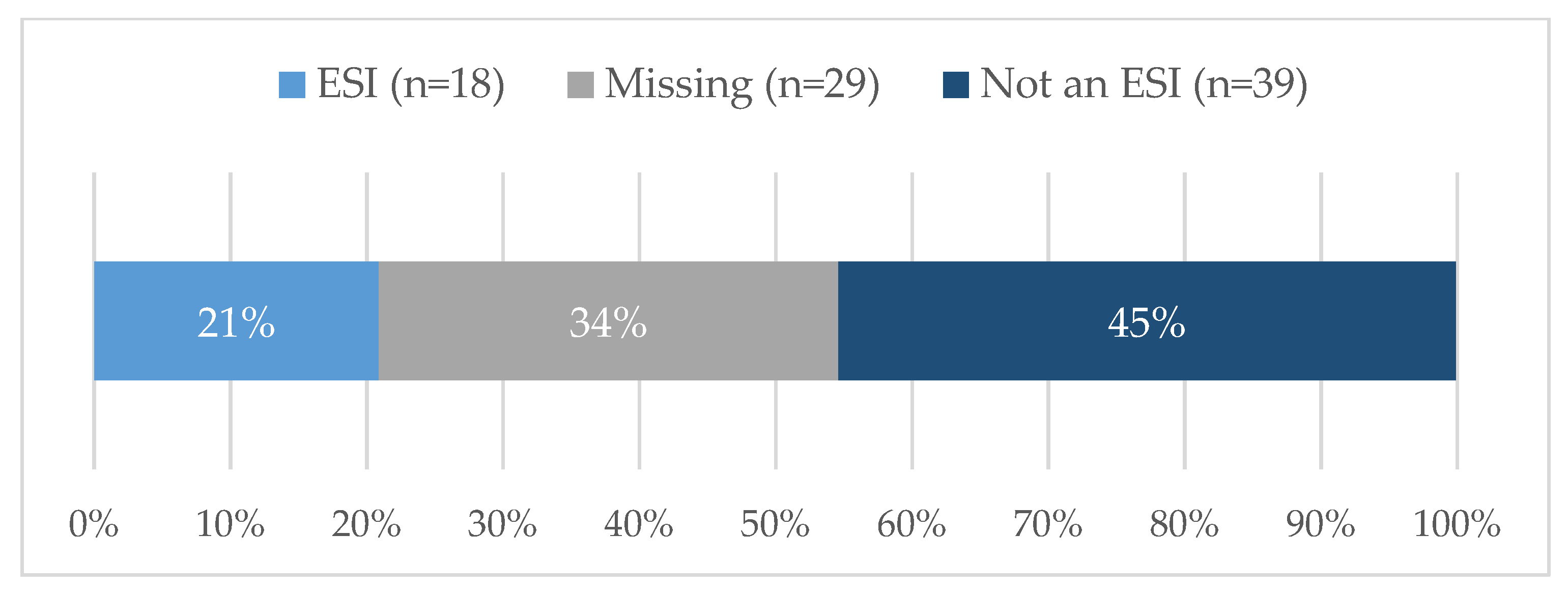
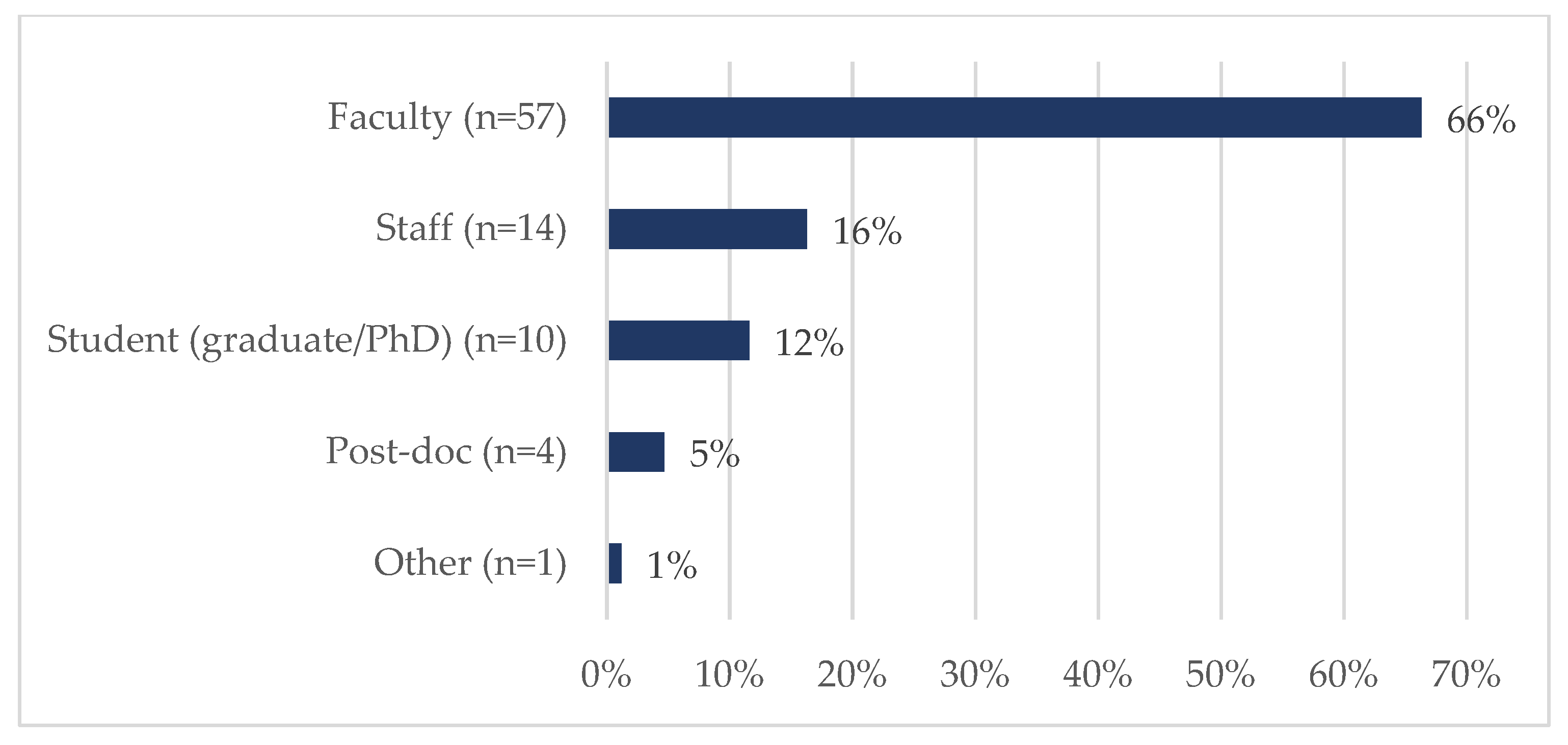
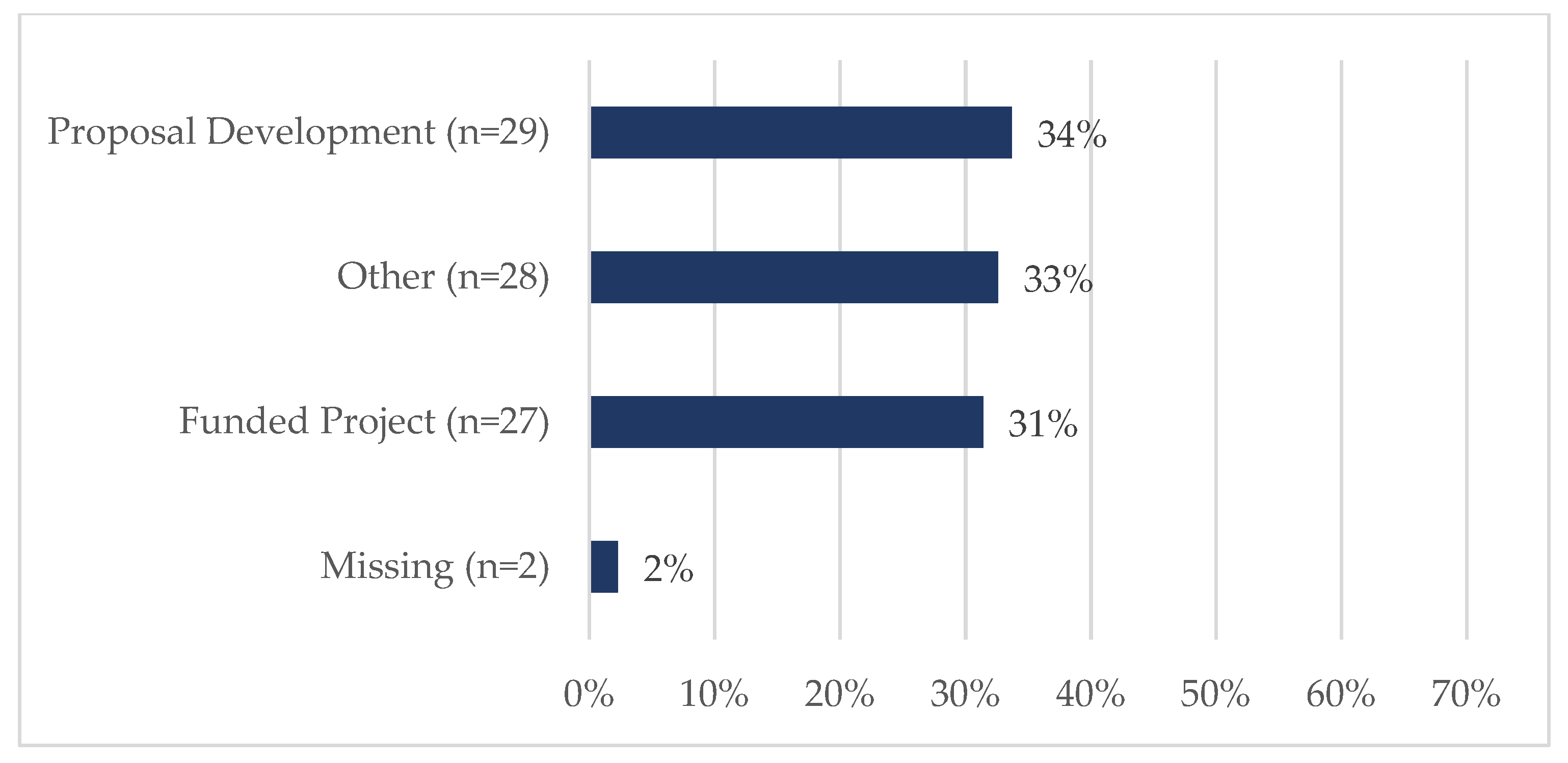
3.2. Phase II: Pilot Year (Grant Year 4, 2020–2021) and Phase III: Year 1 of TAG-SC (Grant Year 5, 2021–2022)
4. Discussion
4.1. Lessons Learned
4.1.1. Improved Tracking and Evaluation
4.1.2. Limited Number of “Shoulder Taps”
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- CHER. Home. Available online: https://nau.edu/cher/ (accessed on 15 September 2022).
- SHERC. Available online: https://nau.edu/sherc/about-us/ (accessed on 26 July 2022).
- National Institute on Minority Health and Health Disparities. Available online: https://www.nimhd.nih.gov/ (accessed on 15 September 2022).
- RCMI. Grants. Available online: https://www.nimhd.nih.gov/programs/extramural/research-centers/rcmi/rcmi-grants.html (accessed on 26 July 2022).
- RCMI. Specialized Centers. Available online: https://www.nimhd.nih.gov/programs/extramural/research-centers/rcmi/specialized-centers.html (accessed on 26 July 2022).
- Ofili, E.O.; Tchounwou, P.B.; Fernandez-Repollet, E.; Yanagihara, R.; Akintobi, T.H.; Lee, J.E.; Malouhi, M.; Garner, S.T.; Hayes, T.T.; Baker, A.R.; et al. The Research Centers in Minority Institutions (RCMI) Translational Research Network: Building and Sustaining Capacity for Multi-Site Basic Biomedical, Clinical and Behavioral Research. Ethn. Dis. 2019, 29, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Research Infrastructure Core (RIC). Available online: https://nau.edu/sherc/research-infrastructure/ (accessed on 6 August 2022).
- RFA-MD-17-003: Research Centers in Minority Institutions (U54). Available online: https://grants.nih.gov/grants/guide/rfa-files/rfa-md-17-003.html (accessed on 27 September 2022).
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research Electronic Data Capture (REDCap)—A Metadata-Driven Methodology and Workflow Process for Providing Translational Research Informatics Support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap Consortium: Building an International Community of Software Platform Partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- REDCap. Available online: https://jefferson.ucc.nau.edu/redcap/index.php (accessed on 29 September 2022).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Question | Response Options |
|---|---|
| Professional role | Assistant Professor, Associate Professor, Professor, PhD student, Post-doc, Staff, Lecturer, Other |
| Type of support | Qualitative methodological/analytical support, Quantitative methodological/analytical support, Instrument development, Data management, Other |
| Research domain, if applicable | Social/Behavioral, Clinical, Biomedical, Biomedical & Clinical, Biomedical & Social/Behavioral, Social/Behavioral & Clinical |
| Type of project | SHERC pilot project, SHERC core project, SHERC campus community partnership, Other internal grant, External grant, Other |
| Project context | Funded project, Proposal development, Other |
| Variable | Common Response Options |
|---|---|
| Early Stage Investigator (ESI) Status | Yes, ESI No, not an ESI |
| Professional role | Faculty Student (graduate/PhD) Post-doc Staff Other |
| Request type | Mixed methodological support Qualitative methodological/analytical support Quantitative methodological/analytical support Instrument development Data management REDCap assistance Other |
| Project content area | Social/Behavioral Clinical Biomedical Other |
| Project type | External grant SHERC funded research or pilot project Other (includes University internal grants) |
| Project details | Funded project Proposal development Other |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lininger, M.R.; Kirby, C.; Laurila, K.A.; Roy, I.; Coder, M.; Propper, C.R.; Trotter, R.T., II; Baldwin, J.A. Building Research Infrastructure: The Development of a Technical Assistance Group-Service Center at an RCMI. Int. J. Environ. Res. Public Health 2023, 20, 191. https://doi.org/10.3390/ijerph20010191
Lininger MR, Kirby C, Laurila KA, Roy I, Coder M, Propper CR, Trotter RT II, Baldwin JA. Building Research Infrastructure: The Development of a Technical Assistance Group-Service Center at an RCMI. International Journal of Environmental Research and Public Health. 2023; 20(1):191. https://doi.org/10.3390/ijerph20010191
Chicago/Turabian StyleLininger, Monica R., Christine Kirby, Kelly A. Laurila, Indrakshi Roy, Marcelle Coder, Catherine R. Propper, Robert T. Trotter, II, and Julie A. Baldwin. 2023. "Building Research Infrastructure: The Development of a Technical Assistance Group-Service Center at an RCMI" International Journal of Environmental Research and Public Health 20, no. 1: 191. https://doi.org/10.3390/ijerph20010191
APA StyleLininger, M. R., Kirby, C., Laurila, K. A., Roy, I., Coder, M., Propper, C. R., Trotter, R. T., II, & Baldwin, J. A. (2023). Building Research Infrastructure: The Development of a Technical Assistance Group-Service Center at an RCMI. International Journal of Environmental Research and Public Health, 20(1), 191. https://doi.org/10.3390/ijerph20010191