
Parents’ Experiences Using Digital Health Technologies in Paediatric Overweight and Obesity Support: An Integrative Review

Abstract
1. Introduction
2. Materials and Methods
3. Results
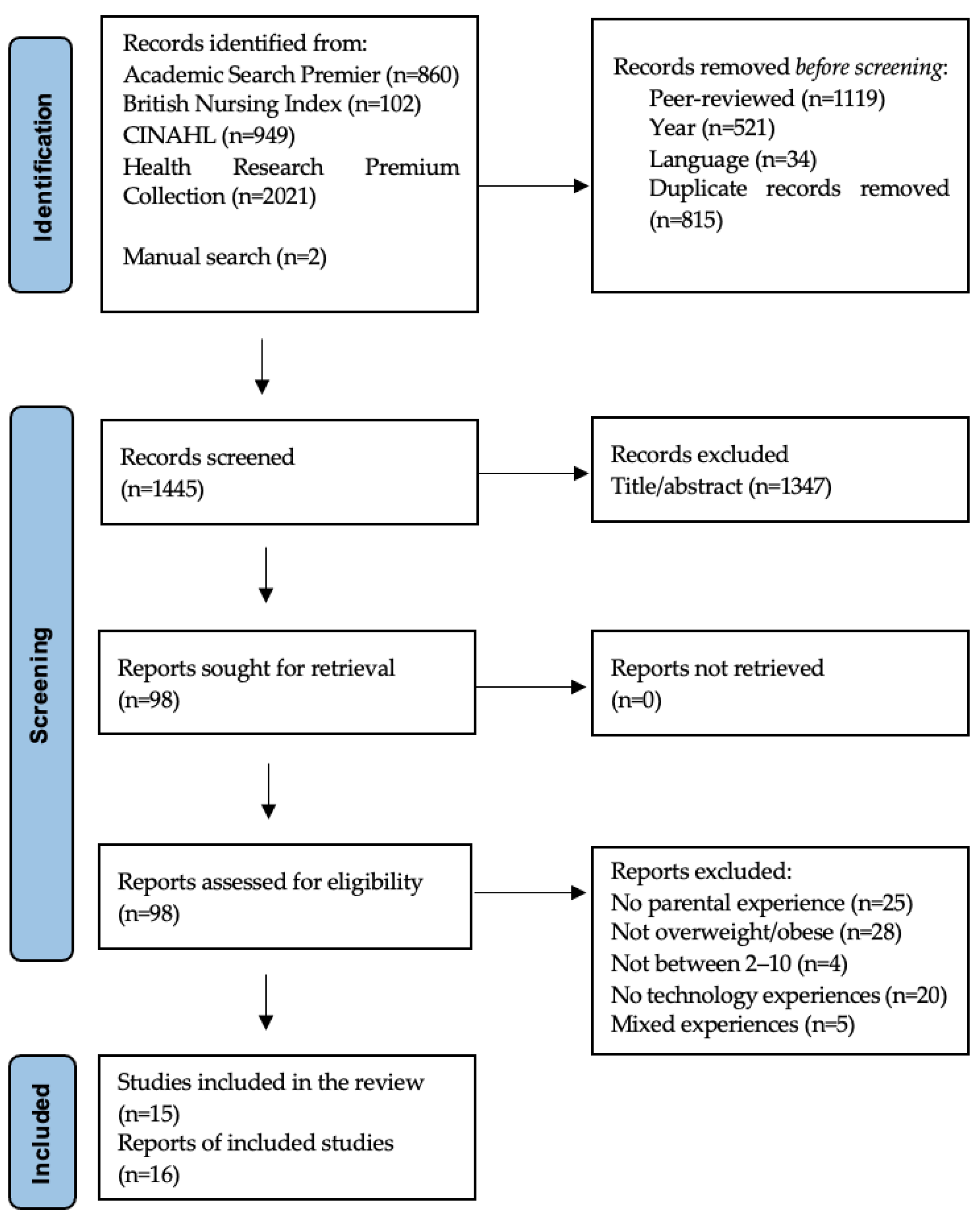
3.1. Selection
3.2. Quality Appraisal
3.3. Study Characteristics
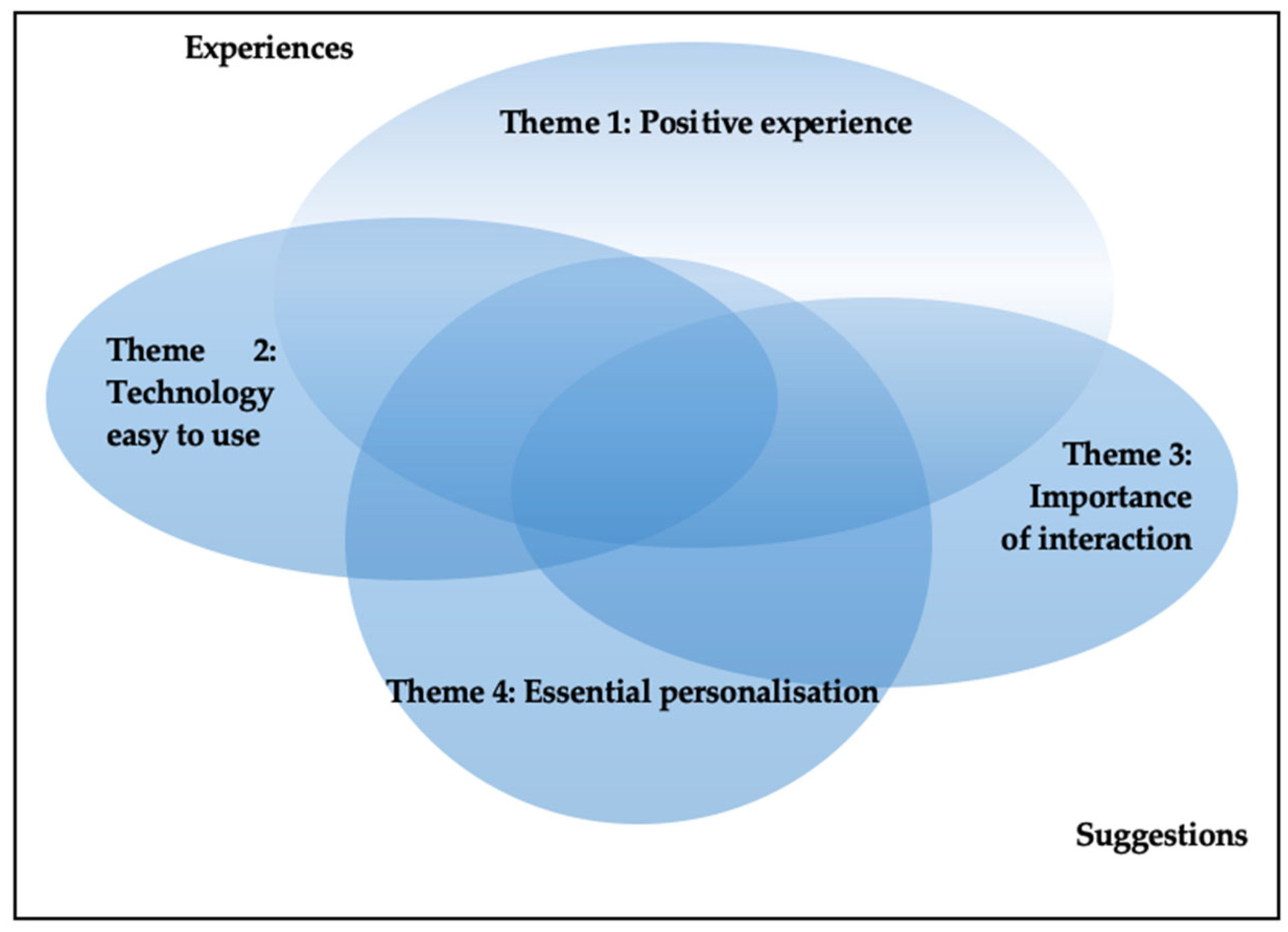
3.4. Findings
3.4.1. Theme 1: Positive Experience
3.4.2. Theme 2: Technology Easy to Use
3.4.3. Theme 3: Importance of Interaction
3.4.4. Theme 4: Essential Personalisation
3.4.5. Different Groups of Digital Health Technologies
4. Discussion
4.1. Findings
4.2. Implications, Future Research, and Limitations
4.3. Methodology
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Boolean Operators | Keyword(s) | Limitation | |
|---|---|---|---|
| Population | 1: Pediatric or child or childhood And 2a: obesity or overweight (database: CINAHL and ‘Academic search premier’) 2b: pediatric or child or childhood or children or pediatrics (database: ‘British nursing index’ and ‘Health premium research’) | ‘subject heading’ (Cinahl and Academic search premier) ‘mainsubject’ (British nursing index and health premium research) | |
| Population | and | parent* or caregiver* or mother* or father* | abstract |
| Exposure | and | telehealth or telemedicine or telecommunication* or ‘digital health’ or eHealth or ‘e-health’ or ‘electronic health’ or ‘m-health’ or mHealth or mobile* or ‘cell phone*’ or cellphone* or ‘mobile application*’ or telephone* or smartphone* or ‘smart phone*’ or ‘text messag*’ or SMS or tablet or app* or ‘e-mail*’ or online or internet or ‘web-based’ or ‘social media’ or web* or computer* or ‘digital tool*’ or ‘digital communication’ or technology or video* | abstract |
| Outcome | and | evaluation or ‘behavior* change*’ or attitude* or view* or perspective* or management or ‘health education’ or ‘lifestyle change*’ or ‘follow up’ or feasibility or satisfaction or perception* or experience* or opinion* or thoughts | abstract |
| Question Number: | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | Overall |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| JBI clinical appraisal checklist for randomised controlled trials [49] | ||||||||||||||
| Armstrong et al. (2018) [30] | Y | Y | Y | ? | N | ? | Y | N | Y | Y | Y | Y | Y | Included |
| Bala et al. (2019) [31] | Y | Y | Y | Y | N | ? | Y | Y | Y | Y | Y | Y | Y | Included |
| Chai et al. (2021) [32] | Y | Y | Y | ? | Y | Y | Y | N | ? | Y | Y | Y | ? | Included |
| Davis et al. (2016) [33] | Y | Y | Y | ? | N | ? | Y | Y | ? | Y | Y | Y | ? | Included |
| Johansson et al. (2020) [34] | Y | Y | Y | N | N | ? | Y | Y | Y | Y | Y | Y | Y | Included |
| Sze et al. (2015) [35] | Y | Y | Y | Y | N | N | Y | Y | Y | Y | Y | Y | Y | Included |
| Taveras et al. (2017) [36] | Y | Y | Y | Y | N | ? | Y | Y | Y | Y | Y | Y | Y | Included |
| Wright et al. (2013) [37] | Y | Y | N | N | N | ? | Y | Y | Y | Y | Y | Y | Y | Included |
| JBI clinical appraisal checklist for qualitative research [48] | ||||||||||||||
| Lee et al. (2019) [38] | ? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Included | |||
| Parra-Soto et al. (2020) [41] * | ? | Y | N | ? | ? | N | N | N | Y | ? | Not included | |||
| Sharifi et al. (2013) [39] | ? | Y | Y | Y | Y | ? | N | Y | Y | Y | Included | |||
| Thorén et al. (2021) [40] | ? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Included | |||
| JBI clinical appraisal checklist for quasi-experimental studies [49] | ||||||||||||||
| Pbert et al. (2016) [44] | Y | N | ? | N | Y | N | N | N | Y | Not included | ||||
| Parra-Soto et al. (2020) [41] * | Y | Y | ? | N | Y | Y | - | - | Y | Not included | ||||
| Militello et al. (2016) [43] | Y | Y | - | N | Y | Y | - | - | Y | Included | ||||
| Tripicchio et al. (2017) [45] | Y | N | Y | Y | Y | Y | Y | Y | Y | Included | ||||
| JBI clinical appraisal checklist for cross-sectional studies [47] | ||||||||||||||
| Mulgrew et al. (2011) [42] | Y | N | Y | N | Y | Y | N | Y | Included | |||||
| Theme 1 | Theme 2 | Theme 3 | Theme 4 | |
|---|---|---|---|---|
| SMS | Enjoyed, personalised [30]; Would continue to use/ recommend to others [30,43]; Might continue to use 50/50 [32]; Frequency right [30,32,35,39,43]; Helpful [30,32,39,43]; Relevant, motivating, easy to understand [32]; Timing right [32,39,43]; Satisfied [31,36]; Useful prompts [35,39] | Easy to use, hard to ignore, convenient, some preferred another medium, brief, hard to refer, asynchronous, space limits, wish for an option to change frequency, suggestion multimodal [39]; Initially hard to understand [43]; Easy access to clinicians [34] | Almost 50% worked better with a partner [31,32]; Easy to share [39]; Option to interact [39]; Easy access to clinicians [34] | Personalised [30,39]; Wish for an option to customise [39]; Wanting specific advice, ‘voice of authority’ [39] |
| Phone | Satisfied [31,32,33,42]; Would continue to use/ recommend to others [31,32,37,42,45]; Saves time and money [31]; Informative, convenient, time appropriate [32]; Helpful [32,33,45]; Useful [32,37] | Mostly no problems [31]; Easy to use [32,37]; Liked to use at home, liked to use on the phone, but 50% would prefer a website [37] | Interaction [31,32]; Clinician approachable [32]; Wanting a face-to-face interaction [33] | Personalised, appropriate [32]; Made for people like them [37] |
| Web- site | Satisfied [31,36]; Would continue to use [32,40]; Useful, enjoyed [40]; Divided as to usefulness [35] | Easy to use [32,35,40]; Few had problems [32]; Always accessible [40]; Liked one weblink [35] | Request to involve children, family, and friends, wanting community function, liked coaching function [40] | Divergent regarding the amount of information [40] |
| App | Would continue to use [45]; Helpful [34,45]; | |||
| Social media | Effective prompts, timing, and frequency right, a little under half would continue to use [32]; Useful, motivating [38] | Easy to understand [32]; Practical to use at home [38] | Peer support, involvement with a school-based programme [38] | Some felt it was not customised for children [38] |
References
- World Health Organization. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 12 April 2022).
- Júlíusson, P.B.; Eide, G.E.; Roelants, M.; Waaler, P.E.; Hauspie, R.; Bjerknes, R. Overweight and obesity in Norwegian children: Prevalence and socio-demographic risk factors. Acta Paediatr. 2010, 99, 900–905. [Google Scholar] [CrossRef] [PubMed]
- Flegal, K.M.; Tabak, C.J.; Ogden, C.L. Overweight in children: Definitions and interpretation. Health Educ. Res. 2006, 21, 755–760. [Google Scholar] [CrossRef] [PubMed]
- Helsedirektoratet. Nasjonal Faglig Retningslinje for Det Helsefremmende Og Forebyggende Arbeidet I Helsestasjon, Skolehelsetjeneste Og Helsestasjon For Ungdom. (National Guideline for Health Promotion and Preventive Work in Child and Youth Health Centres, and School Health Services, 0–20 Years); Helsedirektoratet: Oslo, Norway, 2022.
- Kansra, A.R.; Lakkunarajah, S.; Jay, M.S. Childhood and adolescent obesity: A review. Front. Pediatr. 2020, 8, 581461. [Google Scholar] [CrossRef] [PubMed]
- Lekhal, S.; Holme, H. Overvekt og fedme hos barn (Overweight and obesity in children). In Helsestasjonstjenesten Barns Psykiske Helse Og Utvikling (The Health Centres Service, Children’s Mental Health and Development); Holme, H., Olavesen, E.S., Valla, L., Hansen, M.B., Eds.; Gyldendal Akademisk: Oslo, Norway, 2016; pp. 241–256. [Google Scholar]
- Ball, G.D.C.; Ambler, K.A.; Keaschuk, R.A.; Rosychuk, R.J.; Holt, N.L.; Spence, J.C.; Jetha, M.M.; Sharma, A.M.; Newton, A.S. Parents as agents of change (PAC) in pediatric weight management: The protocol for the PAC randomized clinical trial. BMC Pediatr. 2012, 12, 114. [Google Scholar] [CrossRef]
- Davison, K.K.; Jurkowski, J.M.; Li, K.; Kranz, S.; Lawson, H.A. A childhood obesity intervention developed by families for families: Results from a pilot study. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 3. [Google Scholar] [CrossRef]
- Golan, M.; Kaufman, V.; Shahar, D.R. Childhood obesity treatment: Targeting parents exclusively v. parents and children. Br. J. Nutr. 2006, 95, 1008–1015. [Google Scholar] [CrossRef]
- Lupton, D. Digital Health: Critical and Cross-Disciplinary Perspectives; Routledge, Taylor & Francis Group: London, UK, 2018. [Google Scholar]
- Iakovleva, T.; Oftedal, E.M.; Bessant, J. Responsible innovation in digital health. In Responsible Innovation in Digital Health: Empowering the Patient; Iakovleva, T., Oftedal, E.M., Bessant, J., Eds.; Edward Elgar Publishing: Cheltenham, UK, 2019; pp. 1–8. [Google Scholar]
- Dhaliwal, J.; Nosworthy, N.M.I.; Holt, N.L.; Zwaigenbaum, L.; Avis, J.L.S.; Rasquinha, A.; Ball, G.D.C. Attrition and the management of pediatric obesity: An integrative review. Child. Obes. 2014, 10, 461–473. [Google Scholar] [CrossRef]
- Wu, Y.; Ma, X.; Fraser, W.D.; Li, M.; Wang, W.; Huang, H.; Landry, M.; Hao, Y.; Liu, H.; Semenic, S.; et al. Caregivers’ perceptions, challenges and service needs related to tackling childhood overweight and obesity: A qualitative study in three districts of Shanghai, China. BMC Public Health 2021, 21, 768. [Google Scholar] [CrossRef]
- Zarnowieki, D.; Mauch, C.E.; Middleton, G.; Matwiejczyk, L.; Watson, W.L.; Dibbs, J.; Dessaix, A.; Golley, R.K. A systematic evaluation of digital nutrition promotion websites and apps for supporting parents to influence children’s nutrition. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1. [Google Scholar] [CrossRef]
- Hammersley, M.L.; Jones, R.A.; Okely, A.D. Parent-focused childhood and adolescent overweight and obesity EHealth interventions: A systematic review and meta-analysis. J. Med. Internet Res. 2016, 18, e5893. [Google Scholar] [CrossRef]
- Fowler, L.A.; Grammer, A.C.; Staiano, A.E.; Fitzsimmons-Craft, E.E.; Chen, L.; Yaeger, L.H.; Wilfley, D.E. Harnessing technological solutions for childhood obesity prevention and treatment: A systematic review and meta-analysis of current applications. Int. J. Obes. 2021, 45, 957–981. [Google Scholar] [CrossRef]
- Kouvari, M.; Karipidou, M.; Tsiampalis, T.; Mamalaki, E.; Poulimeneas, D.; Bathrellou, E.; Panagiotakos, D.; Yannakoulia, M. Digital health interventions for weight management in children and adolescents: Systematic review and meta-analysis. J. Med. Internet Res. 2022, 24, e30675. [Google Scholar] [CrossRef] [PubMed]
- Skelton, J.A.; Martin, S.; Irby, M.B. Satisfaction and attrition in paediatric weight management. Clin. Obes. 2016, 6, 143–153. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. 7th International Conference on Health Promotion, Nairobi, Kenya, 26–30 October 2009. Available online: https://www.who.int/teams/health-promotion/enhanced-wellbeing/seventh-global-conference/community-empowerment (accessed on 29 March 2022).
- Ekambareshwar, M.; Ekambareshwar, S.; Mihrshahi, S.; Wen, L.M.; Baur, L.A.; Laws, R.; Taki, S.; Rissel, C. Process evaluations of early childhood obesity prevention interventions delivered via telephone or text messages: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 10. [Google Scholar] [CrossRef] [PubMed]
- Alexandrou, C.; Müssener, U.; Thomas, K.; Henriksson, H.; Löf, M. Adapting a parental support app to promote healthy diet and physical activity behaviors (MINISTOP) for a multi-ethnic setting: A qualitative study on the needs and preferences of parents and nurses within Swedish child health care. Nutrients 2021, 13, 2190. [Google Scholar] [CrossRef]
- Gabrielli, S.; Dianti, M.; Maimone, R.; Betta, M.; Filippi, L.; Ghezzi, M.; Forti, S. Design of a mobile app for nutrition education (TreC-LifeStyle) and formative evaluation with families of overweight children. JMIR Mhealth Uhealth 2017, 5, e7080. [Google Scholar] [CrossRef]
- Simione, M.; Frost, H.M.; Cournoyer, R.; Mini, F.N.; Cassidy, J.; Craddock, C.; Moreland, J.; Wallace, J.; Metlay, J.; Kistin, C.J.; et al. Engaging stakeholders in the adaptation of the connect for health pediatric weight management program for national implementation. Implement. Sci. Commun. 2020, 1, 55. [Google Scholar] [CrossRef]
- Øen, G.; Stormark, K. Participatory action research in the implementing process of evidence-based intervention to prevent childhood obesity: Project design of the ‘Healthy Future’ study. J. Obes. 2013, 2013, 437206. [Google Scholar] [CrossRef]
- Øen, G. Healthy future 2: Preventing childhood obesity using early parental support. Proj. Protoc. Res. Counc. Nor. 2021. Unpublished material. [Google Scholar]
- Whittemore, R.; Knafl, K. The integrative review: Updated methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef]
- Forsberg, C.; Wengström, Y. Att Göra Systematiska Litteraturstudier (To Do Systematic Literature Reviews), 4th ed.; Natur & Kultur: Stockholm, Sweden, 2016. [Google Scholar]
- Toronto, C.E.; Remington, R. A Step-by-Step Guide to Conducting an Integrative Review; Springer International Publishing AG: New York, NY, USA, 2020. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, S.; Mendelsohn, A.; Bennett, G.; Taveras, E.M.; Kimberg, A.; Kemper, A.R. Texting motivational interviewing: A randomized controlled trial of motivational interviewing text messages designed to augment childhood obesity treatment. Child. Obes. 2018, 14, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Bala, N.; Price, S.N.; Horan, C.M.; Gerber, M.W.; Taveras, E.M. Use of telehealth to enhance care in a family-centered childhood obesity intervention. Clin. Pediatr. 2019, 58, 789–797. [Google Scholar] [CrossRef] [PubMed]
- Chai, L.K.; Collins, C.E.; May, C.; Brown, L.J.; Ashman, A.; Burrows, T.L. Fidelity and acceptability of a family-focused technology-based telehealth nutrition intervention for child weight management. J. Telemed. Telecare 2021, 27, 98–109. [Google Scholar] [CrossRef]
- Davis, A.M.; Sampilo, M.; Gallagher, K.S.; Dean, K.; Saroja, M.B.; Yu, Q.; He, J.; Sporn, N.; Befort, C.A. Treating rural paediatric obesity through telemedicine vs. telephone: Outcomes from a cluster randomized controlled trial. J. Telemed. Telecare 2016, 22, 86–95. [Google Scholar] [CrossRef]
- Johansson, L.; Hagman, E.; Danielsson, P. A novel interactive mobile health support system for pediatric obesity treatment: A randomized controlled feasibility trial. BMC Pediatr. 2020, 20, 447. [Google Scholar] [CrossRef]
- Sze, Y.Y.; Tinuke, O.D.; Kilanowski, C.K.; Collins, R.L.; Epstein, L.H. Web-based and mobile delivery of an episodic future thinking intervention for overweight and obese families: A feasibility study. JMIR Mhealth Uhealth 2015, 3, e97. [Google Scholar] [CrossRef]
- Taveras, E.M.; Marshall, R.; Sharifi, M.; Avalon, E.; Fiechtner, L.; Horan, C.; Gerber, M.W.; Orav, E.J.; Price, S.N.; Sequist, T.; et al. Comparative effectiveness of clinical-community childhood obesity interventions: A randomized clinical trial. JAMA Pediatr. 2017, 171, e171325. [Google Scholar] [CrossRef]
- Wright, J.A.; Phillips, B.D.; Watson, B.L.; Newby, P.K.; Norman, G.J.; Adams, W.G. Randomized trial of a family-based, automated, conversational obesity treatment program for underserved populations. Obesity 2013, 21, E369–E378. [Google Scholar] [CrossRef]
- Lee, R.L.T.; Brown, M.; Leung, C.; Chen, H.; Louie, L.; Chen, J.; Lee, P.H. Family carers’ experiences of participating in a weight management programme for overweight children and adolescents with intellectual disabilities: An exploratory study. J. Adv. Nurs. 2019, 75, 388–399. [Google Scholar] [CrossRef]
- Sharifi, M.; Dryden, E.M.; Horan, C.M.; Price, S.; Marshall, R.; Hacker, K.; Finkelstein, J.A.; Taveras, E.M. Leveraging text messaging and mobile technology to support pediatric obesity-related behavior change: A qualitative study using parent focus groups and interviews. J. Med. Internet Res. 2013, 15, e2780. [Google Scholar] [CrossRef] [PubMed]
- Thorén, A.; Janson, A.; Persson, M. ‘Now she prefers jeans, like everyone else...’–Parents’ experiences of group- and web-based treatment of children’s obesity. Acta Paediatr. 2021, 110, 1869–1879. [Google Scholar] [CrossRef] [PubMed]
- Parra-Soto, S.; Ortega, A.; Celis-Morales, C.; Kain, J. Perception that mothers and/or guardians of overweight or obese preschool children have of a text messaging program to support behaviour change in their children. Glob. Pediatr. Health 2020, 7, 2333794X20961575. [Google Scholar] [CrossRef] [PubMed]
- Mulgrew, K.W.; Shaikh, U.; Nettiksimmons, J. Comparison of parent satisfaction with care for childhood obesity delivered face-to-face and by telemedicine. Telemed. E-Health 2011, 17, 383–387. [Google Scholar] [CrossRef] [PubMed]
- Militello, L.; Melnyk, B.M.; Hekler, E.B.; Small, L.; Jacobson, D. Automated behavioral text messaging and face-to-face intervention for parents of overweight or obese preschool children: Results from a pilot study. JMIR Mhealth Uhealth 2016, 4, e21. [Google Scholar] [CrossRef]
- Pbert, L.; Druker, S.; Barton, B.; Olendzki, B.; Andersen, V.; Persuitte, G.; Bram, J.; Kurtz, S.; Powers, E.M.; Crawford, S.; et al. Use of a FITLINE to support families of overweight and obese children in pediatric practices. Child. Obes. 2016, 12, 33–43. [Google Scholar] [CrossRef]
- Tripicchio, G.L.; Ammerman, A.S.; Neshteruk, C.; Faith, M.S.; Dean, K.; Befort, C.; Ward, D.S.; Truesdale, K.P.; Burger, K.S.; Davis, A. Technology components as adjuncts to family-based pediatric obesity treatment in low-income minority youth. Child. Obes. 2017, 13, 433–442. [Google Scholar] [CrossRef]
- Helsedirektoratet. Nasjonale Faglige Retningslinjer for Primærhelsetjenesten. Forebygging Og Behandling Av Overvekt Og Fedme Hos Barn Og Unge; Helsedirektoratet: Oslo, Norway, 2010.
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Systematic reviews of etiology and risk. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020. [Google Scholar]
- Lockwood, C.; Munn, Z.; Parritt, K. Qualitative research syntheses: Methodological guidance for systematic reviewers utilizing meta-aggregation. Int. J. Evid. Based Healthc. 2015, 13, 179–187. [Google Scholar] [CrossRef]
- Tufanaru, C.; Munn, Z.; Aromataris, E.; Campbell, J.; Hopp, L. Systematic reviews of effectiveness. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020. [Google Scholar]
- Tully, L.; Case, L.; Arthurs, N.; Sorensen, J.; Marcin, J.P.; O’Malley, G. Barriers and facilitators for implementing paediatric telemedicine: Rapid review of user perspectives. Front. Pediatr. 2021, 9, 630365. [Google Scholar] [CrossRef]
- Haines, J.; Douglas, S.; Mirotta, J.A.; O’Kane, C.; Breau, R.; Walton, K.; Krystia, O.; Chamoun, E.; Annis, A.; Darlington, G.A.; et al. Guelph family health study: Pilot study of a home-based obesity prevention intervention. Can. J. Public Health 2018, 109, 549–560. [Google Scholar] [CrossRef]
- Hammersley, M.L.; Okely, A.D.; Batterham, M.J.; Jones, R.A. An Internet-based childhood obesity prevention program (Time2bHealthy) for parents of preschool-aged children: Randomized controlled trial. J. Med. Internet Res. 2019, 21, e11964. [Google Scholar] [CrossRef] [PubMed]
- Slusser, W.; Whitley, M.; Izadpanah, N.; Kim, S.L.; Ponturo, D. Multidisciplinary pediatric obesity clinic via telemedicine within the Los Angeles metropolitan area: Lessons learned. Clin. Pediatr. 2016, 55, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Liu, F.; Mao, X.; Peng, W.; Wang, Y.; Huang, H.; Duan, M.; Wang, Y.; Yuan, C. The pediatric cancer survivors’ user experiences with digital health interventions: A systematic review of qualitative data. Cancer Nurs. 2022, 45, E68–E82. [Google Scholar] [CrossRef]
- Lee, J.; Jeongeun, K.; Ahjung, B.; Meiling, J.; Meihua, P.; Kyungryeon, K.; Hyeoiyun, L. Application design for child obesity management based on users’ preferences and needs. West J. Nurs. Res. 2020, 42, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Michou, M.; Panagiotakos, D.B.; Costarelli, V. Low health literacy and excess body weight: A systematic review. Cent. Eur. J. Public Health 2018, 26, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Parker, S.M.; Barr, M.; Stocks, N.; Denney-Wilson, E.; Zwar, N.; Karnon, J.; Kabir, A.; Nutbeam, D.; Roseleur, J.; Liaw, S.T.; et al. Preventing chronic disease in overweight and obese patients with low health literacy using eHealth and teamwork in primary healthcare (HeLP-GP): A cluster randomised controlled trial. BMJ Open 2022, 12, e060393. [Google Scholar] [CrossRef]
- Skelton, J.A.; Beech, B.M. Attrition in paediatric weight management: A review of the literature and new directions. Obes. Rev. 2011, 12, e273–e281. [Google Scholar] [CrossRef]
- DeSilva, S.; Vaidya, S.S. The application of telemedicine to pediatric obesity: Lessons from the past decade. Telemed. E-Health 2020, 27, 159–166. [Google Scholar] [CrossRef]
- Tully, L.; Burls, A.; Sorensen, J.; El-Moslemany, R.; O’Malley, G. Mobile health for pediatric weight management: Systematic scoping review. JMIR Mhealth Uhealth 2020, 8, e16214. [Google Scholar] [CrossRef] [PubMed]
- Whitley, A.; Yahia, N. Efficacy of clinic-based telehealth vs. face-to-face interventions for obesity treatment in children and adolescents in the United States and Canada: A systematic review. Child. Obes. 2021, 17, 299–310. [Google Scholar] [CrossRef]
- Conn, V.S.; Isaramalai, S.; Rath, S.; Jantarakupt, P.; Wadhawan, R.; Dash, Y. Beyond MEDLINE for literature searches. J. Nurs. Scholarsh. 2003, 35, 177–182. [Google Scholar] [CrossRef] [PubMed]


| Study, Country, Design | Children’s Age Criteria (Mean Age Included), Number of Participants, Number Lost, Percentage Lost | Main Findings |
|---|---|---|
| Armstrong et al. (2018) [30]. USA, RCT | 5–12 (9.9), 101 dyads, 19 lost, 18.8% | No BMI difference, reduced attrition for a visit. SMS feasible. |
| Bala et al. (2019) [31]. USA, RCT | 2–12 (8,0), 721 children, 57 lost, 7.9% | High satisfaction with technology components. Telehealth accessible and feasible approach. |
| Chai et al. (2021) [32]. Australia, RCT | 4–11 (9), 46 dyads, 16 lost, 34.8% | Overall high satisfaction. Components were easy to use. Telehealth consultations led to good adherence. The programme improved eating habits according to parents. Would like to continue using/recommend to others. |
| Davis et al. (2016) [33]. USA, RCT | 5–12 (9.14), 103 dyads, 8 lost, 7.76% | Both telemedicine and telephone appear feasible and acceptable methods with high satisfaction levels. Completion rate is high. No significant changes in BMI, physical activity, diet, or psychological effects in either group. |
| Johansson et al. (2020) [34]. Sweden, RCT | 5–12 (8.4 and 9.8), 28 children, 3 lost, 10.7% | BMI reduction and attendance were better in the intervention group. Parents and clinicians found the experience positive and accessible. |
| Lee et al. (2019) [38]. China, Qualitative | 8–16, 20 family caregivers | The mHealth intervention was well-received, and caregivers found it useful. |
| Militello et al. (2016) [43]. USA, Experimental | 3–5 (54.47 months), 15 children, 13 parents, non-lost | Acceptable and feasible. The intervention improved parental knowledge, beliefs, and behaviours towards a healthier lifestyle. |
| Mulgrew et al. (2011) [42]. USA, Cross-sectional | Under 12 years (6.3 and 8.1), 25 surveys, 10 telemedicine surveys | No significant difference between most groups; slightly easier to understand explanations about children’s health in the face-to-face group. All would use telehealth again. |
| Sharifi et al. (2013) [39]. USA, Qualitative | 6–12 (8.7), 31 parents | High acceptability. 2–3 SMS/week appropriate. Want relevant and personalised information. Links can be provided if necessary. |
| Sze et al. (2015) [35]. USA, Experimental | 8–12 (11), 20 dyads, 0 lost | High adherence, easy to use, helpful and useful. |
| Taveras et al. (2017) [36]. USA, RCT | See Bala et al. (2019) [31] | Both groups improved family-centred outcomes for childhood obesity and improvements in child BMI and parental empowerment. |
| Thorén et al. (2021) [40]. Sweden, Qualitative | 5–13, 14 parents | Parents found the programme helpful for the whole family to introduce a healthier lifestyle, predominantly positive experiences. |
| Tripicchio et al. (2017) [45]. USA, Experimental | 2–18 (9.6), 64 children, 16 lost, 25% | Technology components were highly acceptable. Group 3 had significant BMI reductions, but the other groups did not. |
| Wright et al. (2013) [37]. USA, RCT | 9–12 (10.3), 50 dyads, 7 lost, 14% | High interactive voice technology (IVR) users decreased BMI compared to low users. Of those who made calls, >75% agreed that the calls were useful, suitable, credible, and helpful. |
| Study | Duration and Intervention | Parental Digital Use |
|---|---|---|
| Armstrong et al. (2018) [30]. | 12 weeks. Group 1: monthly health visit. SMS-reminders. Group 2: same as group 1 + daily SMSs (Monday–Friday). The first SMS of the week was a text-based dialogue. | Parents responded at least once to 80% of SMSs, and twice or more times to 30%. |
| Bala et al. (2019) [31]. | 1 year. 1st group: monthly SMS and email of neighbourhood resource guide. 2nd group: 6 individual sessions (in-person, video call, or phone), twice weekly SMSs, possibility to reply and receive automated age-specific feedback, GIS map of the neighbourhood and referrals to community resources. Choice between SMS and mail. | 2nd group: 93% chose SMS. 99% responded to at least one SMS, and 61% responded to more than half. 28% used video calls at least once. Parents used video calls in 14–23% and phone calls in 69–86% of visits. |
| Chai et al. (2021) [32]. | 12 weeks. Group 1: 2 video consultations with dietitian, website and Facebook group posting summary with website links as prompts. Group 2: same as group 1 + SMS targeting both parents with a link to the website. Group 3: Waitlist, all components at week 12. | Telehealth: 78–96% attendance, 86% attended by mother and child, 82% in the afternoon. Devices used on the website: desktop (66%); mobile (27%); tablet (7%). Visits through links (64%). |
| Davis et al. (2016) [33]. | 8 months. Group-based intervention (8 weeks weekly, then monthly). Off-site leaders met parents via telemedicine or speakerphone; on-site school representatives met with the children. Meetings lasted approximately one hour. | Overall attendance rate: 89.40%. |
| Johansson, et al. (2020) [34]. | Group 1: standard care. Group 2: standard care + daily weight, SMS communication between parents/clinician, activity monitor connected to a gamified app for children. | Weight frequent at the beginning, than sable at 2.4/week. Messages median (IQR) frequency of 4 (6), ranging from 0 to 13. |
| Lee, et al. (2019) [38]. | Mixture of seminars and workshops, both physical and using mHealth (WhatsApp and Messenger). The research team uploaded the information to the mHealth tools. | |
| Militello et al. (2016) [43]. | 7 weeks. 4 parts: (a) face-to-face visits; (b) reminders (manual); (c) triggers (SMS); and (d) reinforcements (homework). Participants responded to SMSs twice weekly, receiving automated feedback. Parents also developed skill-trigger SMSs, where they select the skill, verbiage, and day(s) and time to receive SMSs. | The number of SMSs sent: 7–39, mean 22.31 (SD 9.47). 69% changed the frequency of tailored SMS (1–5 /week). 58.8% of SMSs sent in the afternoon. The initial response rate for conversational SMSs only 26%. After shortening and simplifying, the increased response rate is 80%. |
| Mulgrew et al. (2011) [42]. | Cross-sectional survey assessing parent satisfaction: Group 1: telemedicine group seen at rural clinics, with a rural provider in the clinic and paediatrician and dietician present via video call; Group 2: regular on-site visits. | Telemedicine group: 70% answered the survey after the first visit. 30% had had 2–9 prior telemedicine consultations (Mean 1.6). |
| Sharifi et al. (2013) [39]. | Two phases: (A) participants received SMS during focus groups to discuss the experience; (B) some participants reviewed a 3-week mock intervention, receiving 3 SMSs/weekly. | |
| Sze et al. (2015) [35]. | 4 weeks. Preintervention nutrition intervention for all. Group 1: personally tailored, device-friendly interactive website, where participants generated their own cues to listen to at least 2/daily + SMS/email prompts 2/daily, weekly sessions. Group 2: same + own audio recordings of episodic future thinking x2/daily. | Devices used: Adult group 1: desktop 21.3%, tablet 16.5%, mobile phone 62.2%; Adult group 2: desktop 34.2%, tablet 2.7%, mobile phone 63.1%. |
| Taveras et al. (2017) [36]. | See Bala et al. (2019) [31]. | |
| Thorén et al. (2021) [40]. | 4 weekly group sessions, followed by 12-week web-based programme targeting parents and children. Weekly modules. Device-friendly. Participants also received physical activity on prescription. | Most parents used the web-based weekly coaching modules. All families registered in the web-based programme. |
| Tripicchio et al. (2017) [45]. | 12 weeks. Group 1: weekly 2-h group sessions. Group 2: Same + tablets with fitness app with instructions for use. Group 3: Same as group 2 + individual video calls every other week. | 81.3–100% used the app at least once. Group 3 used the app significantly more than group 2. Families received at least one call, and 44.5% received five sessions or more. Calls lasted, on average, 0.5–1 h. |
| Wright et al. (2013) [37]. | 12 weeks. Parents and children received telephone counselling intervention delivered by automated IVR. Participants called twice/week, option to complete both at once. IVR asked questions and provided tailored feedback. | 76% of parents called at least once. Of parents who called more than once, the mean number of total calls was 9.1 (5.2). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fidjeland, T.G.; Øen, K.G. Parents’ Experiences Using Digital Health Technologies in Paediatric Overweight and Obesity Support: An Integrative Review. Int. J. Environ. Res. Public Health 2023, 20, 410. https://doi.org/10.3390/ijerph20010410
Fidjeland TG, Øen KG. Parents’ Experiences Using Digital Health Technologies in Paediatric Overweight and Obesity Support: An Integrative Review. International Journal of Environmental Research and Public Health. 2023; 20(1):410. https://doi.org/10.3390/ijerph20010410
Chicago/Turabian StyleFidjeland, Torbjørg Goa, and Kirsten Gudbjørg Øen. 2023. "Parents’ Experiences Using Digital Health Technologies in Paediatric Overweight and Obesity Support: An Integrative Review" International Journal of Environmental Research and Public Health 20, no. 1: 410. https://doi.org/10.3390/ijerph20010410
APA StyleFidjeland, T. G., & Øen, K. G. (2023). Parents’ Experiences Using Digital Health Technologies in Paediatric Overweight and Obesity Support: An Integrative Review. International Journal of Environmental Research and Public Health, 20(1), 410. https://doi.org/10.3390/ijerph20010410