
Distorted Body Image and Mental Pain in Anorexia Nervosa


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Measures
- (a)
- Body Shape Questionnaire (BSQ-34) [30]: belongs to self-report measures and contains 34 test items. Its purpose is to examine a person’s well-being in relation to their appearance over the last four weeks. The higher the average test score, the higher the level of body dissatisfaction (Cronbach’s α = 0.97).
- (b)
- Yale Brown Obsessive Compulsive Scale modified for Body Dysmorphic Disorder (BDD-YBOCS) [31]: is a tool designed to capture the changes in the severity of obsessive-compulsive symptoms. It is used to study dysmorphic disorders of the body. It consists of 12 closed questions, two of which have been extended with additional qualitative questions (Cronbach’s α = 0.87).
- (c)
- Body Image Disturbance Questionnaire (BIDQ) [1]: this questionnaire assesses beliefs about physical appearance. The tool consists of 5 open questions and 7 closed questions in which answers are given on the Likert scale from 1 to 5. This tool assesses body image disturbance on a continuum including body image dissatisfaction, distress, and disfunction. BIDQ positively correlates also with body image dysphoria (Cronbach’s α = 0.86).
- (d)
- Eating Attitudes Test (EAT-26) [32,33]: is a questionnaire for the assessment of eating disorders, enabling the assessment of eating habits and the degree of interest in the weight and size of one’s own body. It consists of two parts: A—contains 26 items and B—contains 6 items. Scores above 20 points indicate harmful eating behavior and a high probability of eating disorders (Cronbach’s α = 0.97).
- (e)
- Center for Epidemiologic Studies Depression Scale-Revised (CESD-R) [34]: is a self-report scale that examines the occurrence of symptoms of affective disorders, in particular depressive mood, over the past two weeks. The tool contains 20 test items on well-being and behavior. The answers are given on a Likert scale from 0 (not at all or less than 1 day) to 4 (almost every day for 2 weeks) (Cronbach’s α = 0.95).
- (f)
- The Psychache Scale [20]: is a tool based on Shneidman’s definition of psychological pain, which is pain associated with psychache. It is a measure of self-esteem constructed from 13 test items, assessed on a 5-point Likert scale. This scale’s aim is to check the relationship of psychological pain with the appearance of suicidal thoughts and activities among the population of healthy people and people diagnosed with depressive disorders (Cronbach’s α = 0.98).
2.4. Statistical Analysis
2.4.1. Mann–Whitney U
2.4.2. Correlations
2.4.3. Regression Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cash, T.F.; Philips, K.A.; Santos, M.T.; Hrabosky, J.I. Measuring ‘‘negative body image’’: Validation of the Body Image Disturbance Questionnaire in a nonclinical population. Body Image 2004, 5, 363–372. [Google Scholar] [CrossRef]
- Grogan, S. Body image: Understanding body dissatisfaction in men, women, and children; Routledge: London, UK, 2021. [Google Scholar] [CrossRef]
- Kostecka, B.; Kordyńska, K.K.; Murawiec, S.; Kucharska, K. Distorted body image in women and men suffering from Anorexia Nervosa—A literature review. Arch. Psychiatry Psychother. 2019, 21, 13–21. [Google Scholar] [CrossRef]
- Bruch, H. Perceptual and Conceptual Disturbances in Anorexia Nervosa. Psychosom. Med. 1962, 24, 187–194. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Sattler, F.A.; Eickmeyer, S.; Eisenkolb, J. Body image disturbance in children and adolescents with anorexia nervosa and bulimia nervosa: A systematic review. Eat. Weight Disord. Stud. Anorexia Bulim. Obes. 2020, 25, 857–865. [Google Scholar] [CrossRef] [PubMed]
- Nitsch, K.; Prajs, E.; Kurpisz, J.; Tyburski, E. Obraz ciała i jego zaburzenia. Aspekty teoretyczne w kontekście wybranych jednostek psychopatologicznych. Psychiatr. Psychol. Klin. 2012, 12, 176–182. [Google Scholar]
- Izydorczyk, B.; Rybicka-Klimczyk, A. Poznawcze aspekty obrazu ciała u kobiet a zaburzenia odżywiania. Endokrynol. Pol. 2009, 60, 287–294. [Google Scholar]
- Rosen, J.C.; Reiter, J. Development of the Body Dysmorphic Disorder Examination. Behav. Res. Ther. 1996, 34, 755–766. Available online: https://www.sciencedirect.com/science/article/pii/0005796796000241 (accessed on 27 April 2006). [CrossRef]
- Castle, D.J.; Rossell, S.; Kyrios, M. Body Dysmorphic Disorder. Psychiatry Clin. N. Am. 2006, 29, 521–538. Available online: https://www.sciencedirect.com/science/article/pii/S0193953X06000141 (accessed on 27 April 2006). [CrossRef]
- Wojtczak, K.; Rabe-Jabłońska, J. Dysmorfofobia przed wystąpieniem i jako składowa innych zaburzeń psychicznych. Psychiatr. Psychol. Klin. 2006, 6, 14–23. [Google Scholar]
- Namysłowska, I.; Paszkiewicz, E.; Siewierska, A. Gdy Odchudzanie Jest Chorobą. Anoreksja i Bulimia; WAB: Warszawa, Poland, 2000. [Google Scholar]
- Drywień, M.E. Zaburzenia odżywiania. Kosmos. Probl. Nauk Biol. 2010, 59, 337–344. [Google Scholar]
- Brytek-Matera, A. Obraz Ciała–Obraz Siebie. Wizerunek Własnego Ciała w Ujęciu Psychospołecznym; Difin: Warszawa, Poland, 2008. [Google Scholar]
- Przewoźnik, D.A. Wybrane zagadnienia dotyczące neurobiologii jadłowstrętu psychicznego. Neuropsychiatr. Neuropsychol. 2013, 8, 118–122. [Google Scholar]
- Mahler, M.S. Thoughts about development and individuation. Psychoanal. Study Child 1963, 18, 307–324. [Google Scholar] [CrossRef]
- Bowlby, J. Attachment and Loss (t. II); Hogarth Press and the Institute of Psychoanalysis: London, UK, 1973. [Google Scholar]
- Chodkiewicz, J. Ból Psychiczny—Konceptualizacja i Narzędzia Pomiaru. Psychiatria 2013, 10, 109–115. Available online: https://journals.viamedica.pl/psychiatria/article/view/36415 (accessed on 27 April 2006).
- Shneidman, E. The Suicidal Mind, 1st ed.; Oxford University Press: Oxford, UK, 1996. [Google Scholar]
- Chodkiewicz, J.; Miniszewska, J.; Strzelczyk, D.; Gąsior, K. Polish Adaptation of the Psychache Scale by Ronald Holden and Co-workers. Psychiatr. Pol. 2017, 51, 369–381. [Google Scholar] [CrossRef]
- Freud, S. A Difficulty in the Path of Psychoanalysis. In The Standard Edition of the Complete Psychological Works of Sigmund Freud, (1917–1919): “An Infantile Neurosis” and Other Works; The Hogarth Press and The Institute of Psychoanalysis: London, UK, 1955; Volume XVII, pp. 135–144. [Google Scholar]
- DeLisle, M.M.; Holden, R.R. Differentiating Between Depression, Hopelessness, and Psychache in University Undergraduates. Meas. Evaluation Couns. Dev. 2009, 42, 46–63. [Google Scholar] [CrossRef]
- Holden, R.R.; Mehta, K.; Cunningham, E.J.; McLeod, L.D. Development and preliminary validation of a scale of psychache. Can. J. Behav. Sci./Rev. Can. Des Sci. Du Comport. 2001, 33, 224–232. [Google Scholar] [CrossRef]
- Meerwijk, E.L.; Weiss, S.J. Toward a Unifying Definition of Psychological Pain. J. Loss Trauma 2011, 16, 402–412. [Google Scholar] [CrossRef]
- Radziwiłłowicz, W.; Reszka, N. Zachowania autodestruktywne u dziewcząt z rozpoznaniem jadłowstrętu psychicznego. Psychiatria 2008, 5, 144–155. [Google Scholar]
- Arcelus, J.; Mitchell, A.J.; Wales, J.; Nielsen, S. Mortality Rates in Patients with Anorexia Nervosa and Other Eating Disorders: A Meta-analysis of 36 Studies. Arch. Gen. Psychiatry 2011, 68, 724–731. [Google Scholar] [CrossRef] [Green Version]
- Lian, B.; Forsberg, S.E.; Fitzpatrick, K.K. Adolescent Anorexia: Guiding Principles and Skills for the Dietetic Support of Family-Based Treatment. J. Acad. Nutr. Diet. 2019, 119, 23–25. [Google Scholar] [CrossRef]
- Paul, T.; Schroeter, K.; Dahme, B.; Nutzinger, D.O. Self-Injurious Behavior in Women with Eating Disorders. Am. J. Psychiatry 2002, 159, 408–411. [Google Scholar] [CrossRef] [PubMed]
- Bodell, L.P.; Cheng, Y.; Wildes, J.E. Psychological Impairment as a Predictor of Suicide Ideation in Individuals with Anorexia Nervosa. Suicide Life-Threat. Behav. 2019, 49, 520–528. Available online: https://onlinelibrary.wiley.com/doi/abs/10.1111/sltb.12459 (accessed on 26 March 2018). [CrossRef] [PubMed]
- Cooper, P.J.; Taylor, M.J.; Cooper, Z.; Fairbum, C.G. The development and validation of the body shape questionnaire. Int. J. Eat. Disord. 1987, 6, 485–494. [Google Scholar] [CrossRef]
- Phillips, K.A.; Hollander, E.; Rasmussen, S.A.; Aronowitz, B.R.; DeCaria, C.; Goodman, W.K. A severity rating scale for body dysmorphic disorder: Development, reliability, and validity of a modified version of the Yale–Brown Obsessive Compulsive Scale. Psychopharmacol. Bull. 1997, 33, 17–22. [Google Scholar] [PubMed]
- Garner, D.M.; Olmsted, M.P.; Bohr, Y.; Garfinkel, P.E. The eating attitudes test: Psychometric features and clinical correlates. Psychol. Med. 1982, 12, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Rogoza, R.; Brytek-Matera, A.; Garner, D.M. Analysis of the EAT-26 in a non-clinical sample. Arch. Psychiatry Psychother. 2016, 18, 54–58. [Google Scholar] [CrossRef]
- Koziara, K. Assessment of depressiveness in population. Psychometric evaluation of the Polish version of the CESD-R. Psychiatr. Pol. 2016, 50, 1109–1117. [Google Scholar] [CrossRef]
- Caspi, A.; Amiaz, R.; Davidson, N.; Czerniak, E.; Gur, E.; Kiryati, N. Computerized assessment of body image in anorexia nervosa and bulimia nervosa: Comparison with standardized body image assessment tool. Arch. Womens Ment. Health 2017, 20, 139–147. [Google Scholar] [CrossRef]
- Oldershaw, A.; Startup, H.; Lavender, T. Anorexia Nervosa and a Lost Emotional Self: A Psychological Formulation of the Development, Maintenance, and Treatment of Anorexia Nervosa. Front. Psychol. 2019, 10, 219. [Google Scholar] [CrossRef] [Green Version]
- Carter, F.A.; Jordan, J.; McIntosh, V.V.; Luty, S.E.; McKenzie, J.M.; Frampton, C.M.; Bulik, C.M.; Joyce, P.R. The long-term efficacy of three psychotherapies for anorexia nervosa: A randomized, controlled trial. Int. J. Eat. Disord. 2011, 44, 647–654. [Google Scholar] [CrossRef]
- Schmidt, U.; Oldershaw, A.; Jichi, F.; Sternheim, L.; Startup, H.; McIntosh, V.; Jordan, J.; Tchanturia, K.; Wolff, G.; Rooney, M.; et al. Out-patient psychological therapies for adults with anorexia nervosa: Randomised controlled trial. Br. J. Psychiatry 2012, 201, 392–399. [Google Scholar] [CrossRef] [Green Version]
- Zipfel, S.; Wild, B.; Groß, G.; Friederich, H.C.; Teufel, M.; Schellberg, D.; Giel, K.E.; de Zwaan, M.; Dinkel, A.; Herpertz, S.; et al. Focal psychodynamic therapy, cognitive behaviour therapy, and optimised treatment as usual in outpatients with anorexia nervosa (ANTOP study): Randomised controlled trial. Lancet 2014, 383, 127–137. [Google Scholar] [CrossRef]
- Fairburn, C.G.; Bailey-Straebler, S.; Basden, S.; Doll, H.A.; Jones, R.; Murphy, R.; O’Connor, M.E.; Cooper, Z. A transdiagnostic comparison of enhanced cognitive behaviour therapy (CBT-E) and interpersonal psychotherapy in the treatment of eating disorders. Behav. Res. Ther. 2015, 70, 64–71. [Google Scholar] [CrossRef] [Green Version]
- Jagielska, G.; Kacperska, I. Outcome, comorbidity, and prognosis in anorexia nervosa. Psychiatr. Pol. 2017, 51, 205–218. [Google Scholar] [CrossRef]
- Marucci, S.; Ragione, L.D.; De Iaco, G.; Mococci, T.; Vicini, M.; Guastamacchia, E.; Triggiani, V. Anorexia Nervosa and Comorbid Psychopathology. Endocr. Metab. Immune Disord. Drug Targets 2018, 18, 316–324. [Google Scholar] [CrossRef]
- Junne, F.; Zipfel, S.; Martus, P.; Giel, K.; Resmark, G.; Teufel, M.; Dinkel, A.; Burgmer, M.; Rothermund, E.; Ziser, K.; et al. The Relationship of Body Image With Symptoms of Depression and Anxiety in Patients With Anorexia Nervosa During Outpatient Psychotherapy: Results of the ANTOP Study. Psychotherapy 2016, 53, 141–151. [Google Scholar] [CrossRef]
- Tomba, E.; Tecuta, L.; Crocetti, E.; Squarcio, F.; Tomei, G. Residual eating disorder symptoms and clinical features in remitted and recovered eating disorder patients: A systematic review with meta-analysis. Int. J. Eat. Disord. 2019, 52, 759–776. [Google Scholar] [CrossRef] [Green Version]
- Shafran, R.; Fairburn, C.G.; Robinson, P.; Lask, B. Body checking and its avoidance in eating disorders. Int. J. Eat. Disord. 2004, 35, 93–101. [Google Scholar] [CrossRef]
- Bamford, B.H.; Attoe, C.; Mountford, V.A.; Morgan, J.F.; Sly, R. Body checking and avoidance in low weight and weight restored individuals with anorexia nervosa and non-clinical females. Eat. Behav. 2014, 15, 5–8. [Google Scholar] [CrossRef]
- Cash, T.; Pruzinsky, T.; Cash, T.F.; Pruzinsky, T. (Eds.) Body Image: A Handbook of Theory, Research, and Clinical Practice; Guilford Press: New York, NY, USA, 2002. [Google Scholar]
- Tomba, E.; Tecuta, L.; Gardini, V.; Lo Dato, E. Mental Pain in Eating Disorders: An Exploratory Controlled Study. J. Clin. Med. 2021, 10, 3584. [Google Scholar] [CrossRef]


{kind=link}
| AN | HCs | Mann-Whitney U Test | |||
|---|---|---|---|---|---|
| n = 36 | n = 69 | U | Z | p | |
| Mean (SD) | Mean (SD) | ||||
| Age | 24.08 (6.13) | 22.90 (2.42) | 1274,5 | 0.22 | <0.825 |
| MI | 16.76 (1.60) | 23.54 (4.64) | 2433.0 | 8.04 | <0.001 |
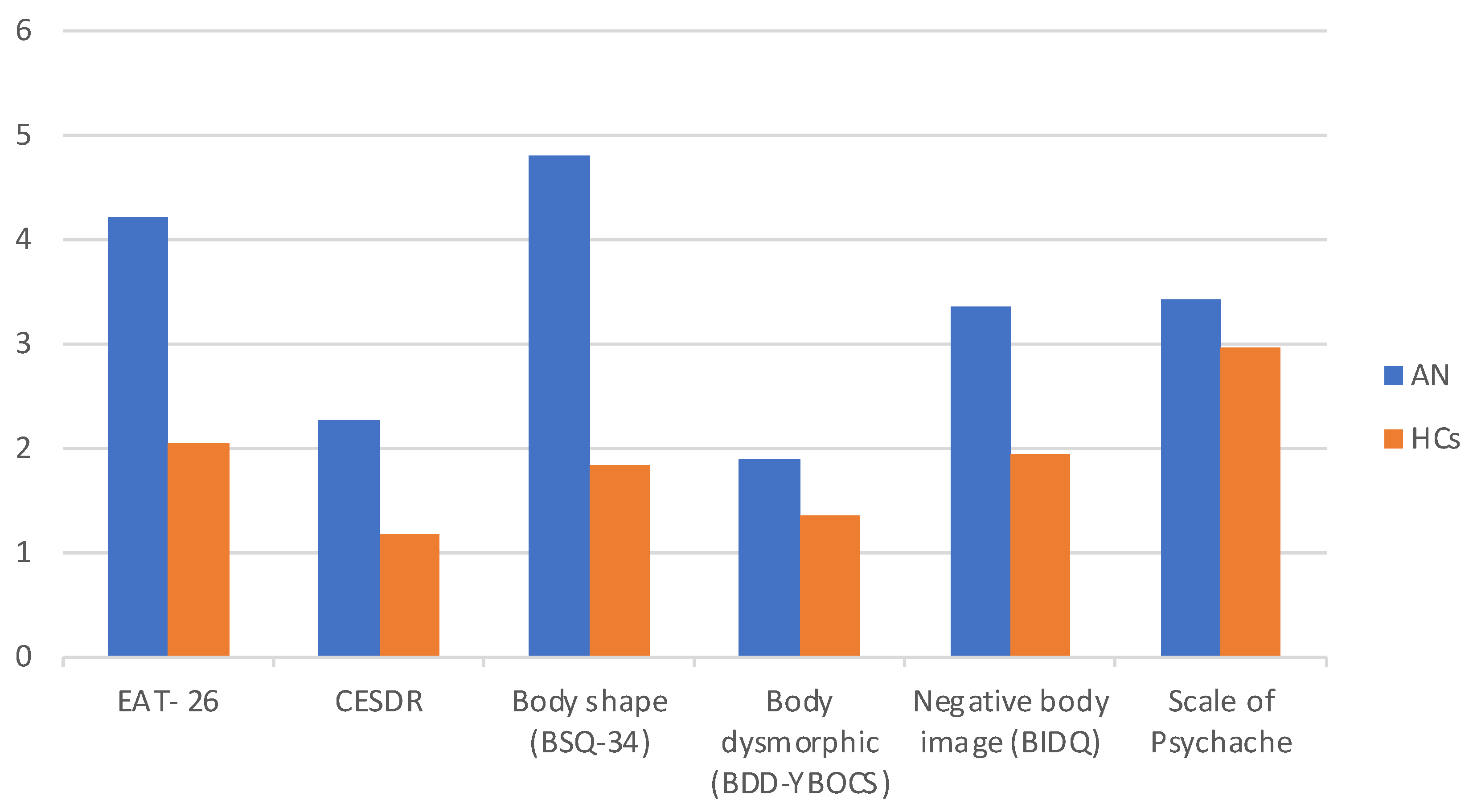
| EAT-26 | 4.22 (0.80) | 2.05 (0.69) | 123.50 | −7.56 | <0.001 |
| CESDR | 2.27 (0.99) | 1.17 (0.82) | 489.00 | −5.09 | <0.001 |
| Body shape (BSQ-34) | 4.80 (0.90) | 1.83 (0.95) | 387.00 | −5.77 | <0.001 |
| Body dysmorphic (BDD-YBOCS) | 1.88 (0.37) | 1.36 (0.37) | 383.00 | −5.80 | <0.001 |
| Negative body image (BIDQ) | 3.35 (0.92) | 1.95 (0.68) | 312.50 | −6.28 | <0.001 |
| Scale of Psychache | 3.42 (1.03) | 2.96 (1.42) | 337.00 | −6.12 | <0.001 |
| AN | HCs | |||||
|---|---|---|---|---|---|---|
| BSQ-34 | BDD-YBOCS | BIDQ | BSQ-34 | BDD-YBOCS | BIDQ | |
| Scale of Psychache | 0.67 ** | 0.63 ** | 0.68 ** | 0.37 ** | 0.51 ** | 0.53 ** |
| CESDR Eat-26 | 0.56 ** 0.63 ** | 0.51 ** 0.59 ** | 0.48 ** 0.45 ** | 0.39 ** 0.78 ** | 0.57 ** 0.60 ** | 0.54 ** 0.49 ** |
| B | SE | Β | t | 95% CI for B | Adjusted R² | F | ||
|---|---|---|---|---|---|---|---|---|
| AN group | ||||||||
| Model 1 | Constant | 0.35 | 0.52 | 0.68 | [–0.70, 1.41] | 0.62 | 30.02 *** | |
| EAT-26 | 0.47 | 0.16 | 0.37 | 2.94 ** | [0.15, 0.80] | ΔR² = 0.65 | ΔF = 30.02 *** | |
| CESDR | 0.58 | 0.13 | 0.54 | 4.27 *** | [0.38, 1.90] | |||
| Model 2 | Constant | –0.17 | 0.50 | –0.33 | [–1.20, 0.87] | 0.69 | 26.95 *** | |
| EAT-26 | 0.37 | 0.15 | 0.29 | 2.43 * | [0.06, 0.67] | ΔR² = 0.72 | ΔF = 26.95 *** | |
| CESDR | 0.45 | 0.13 | 0.42 | 3.56 *** | [0.19, 0.70] | |||
| BIDQ | 0.35 | 0.13 | 0.32 | 2.83 ** | [0.10, 0.61] | |||
| HCs group | ||||||||
| Model 1 | Constant | 0.61 | 0.23 | 2.61 | [0.14, –1.07] | 0.55 | 42.61 *** | |
| EAT-26 | 0.14 | 0.13 | 0.10 | 1.12 | [–0.11, –0.40] | ΔR² = 0.56 | ΔF = 42.61 *** | |
| CESDR | 0.81 | 0.11 | 0.70 | 7.60 *** | [0.60, 1.02] | |||
| Model 2 | Constant | 0.36 | 0.27 | 1.36 | [–0.17, 0.89] | 0.57 | 30.45 *** | |
| EAT-26 | 0.06 | 0.13 | 0.04 | 0.45 | [–0.21, 0.33] | ΔR² = 0.58 | ΔF = 30.45 ** | |
| CESDR | 0.73 | 0.11 | 0.63 | 6.46 *** | [0.51, 0.96] | |||
| BIDQ | 0.25 | 0.14 | 0.18 | 1.80 | [–0.03, 0.52] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciwoniuk, N.; Wayda-Zalewska, M.; Kucharska, K. Distorted Body Image and Mental Pain in Anorexia Nervosa. Int. J. Environ. Res. Public Health 2023, 20, 718. https://doi.org/10.3390/ijerph20010718
Ciwoniuk N, Wayda-Zalewska M, Kucharska K. Distorted Body Image and Mental Pain in Anorexia Nervosa. International Journal of Environmental Research and Public Health. 2023; 20(1):718. https://doi.org/10.3390/ijerph20010718
Chicago/Turabian StyleCiwoniuk, Natalia, Magdalena Wayda-Zalewska, and Katarzyna Kucharska. 2023. "Distorted Body Image and Mental Pain in Anorexia Nervosa" International Journal of Environmental Research and Public Health 20, no. 1: 718. https://doi.org/10.3390/ijerph20010718
APA StyleCiwoniuk, N., Wayda-Zalewska, M., & Kucharska, K. (2023). Distorted Body Image and Mental Pain in Anorexia Nervosa. International Journal of Environmental Research and Public Health, 20(1), 718. https://doi.org/10.3390/ijerph20010718