


Pollen Sensitization Can Increase the Allergic Reaction to Non-Cross-Reactive Allergens in a Soy-Allergic Patient
 , ,
, ,
Abstract
:1. Introduction
2. Case Presentation
3. SPT and sIgE Results
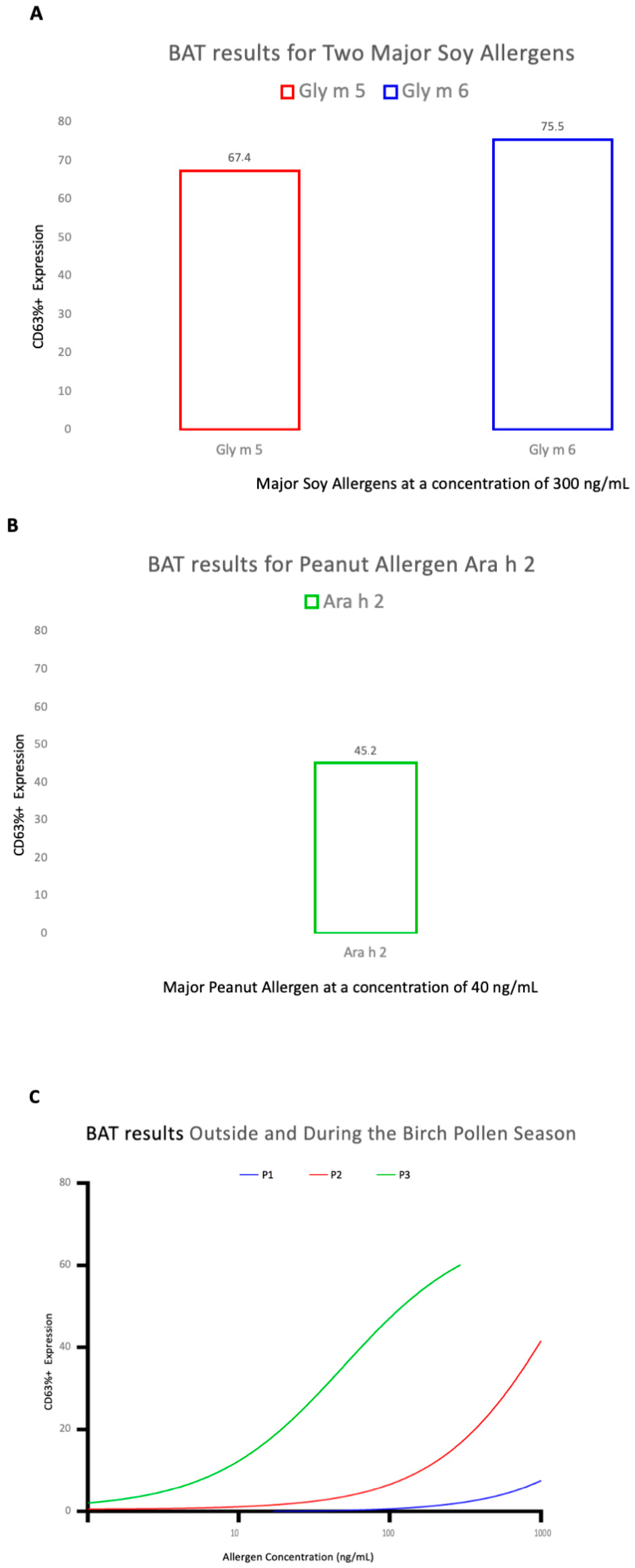
4. Basophil Activation Test (BAT)
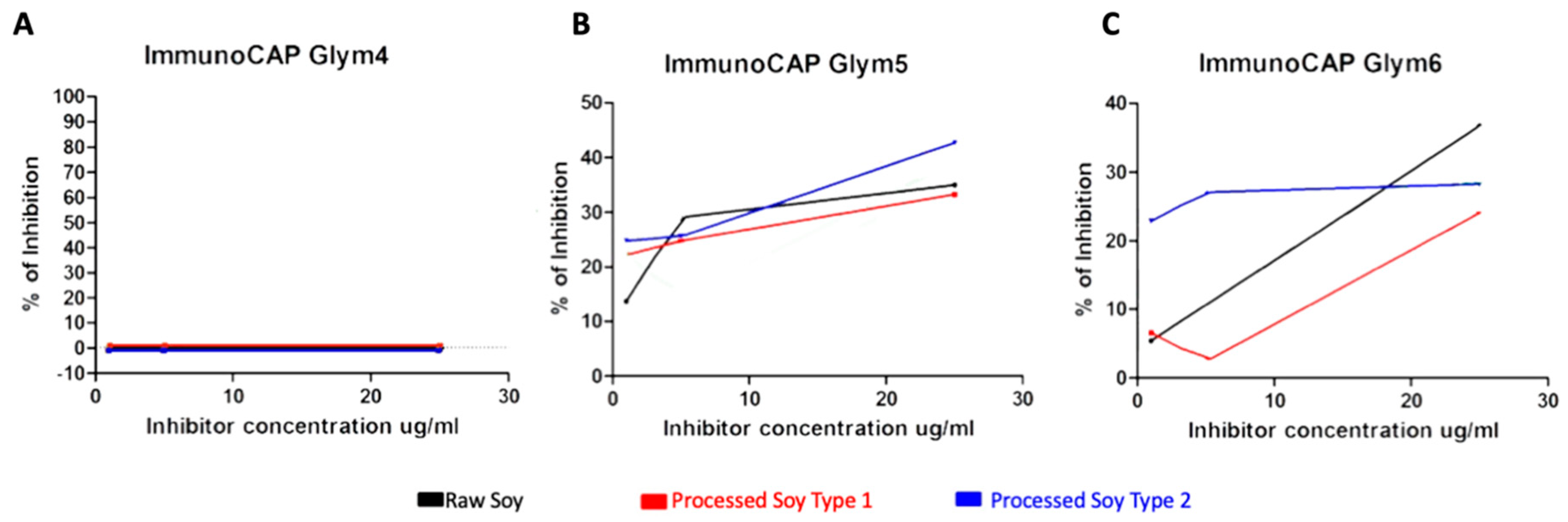
5. ImmunoCAP Inhibition Assay
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Taylor, S.L.; Houben, G.F.; Blom, W.M.; Westerhout, J.; Remington, B.C.; Crevel, R.W.; Brooke-Taylor, S.; Baumert, J.L. The population threshold for soy as an allergenic food–why did the reference dose decrease in VITAL 3.0? Trends Food Sci. Technol. 2021, 112, 99–108. [Google Scholar] [CrossRef]
- Cox, A.L.; Eigenmann, P.A.; Sicherer, S.H. Clinical Relevance of Cross-Reactivity in Food Allergy. J. Allergy Clin. Immunol. Pract. 2021, 9, 82–99. [Google Scholar] [CrossRef] [PubMed]
- Smits, M.; Verhoeckx, K.; Knulst, A.; Welsing, P.; de Jong, A.; Houben, G.; Le, T. Ranking of 10 legumes according to the preva-lence of sensitization as a parameter to characterize allergenic proteins. Toxicol. Rep. 2021, 8, 767–773. [Google Scholar] [CrossRef] [PubMed]
- European Commission Directive 2007/68EC of 27th November 2007. Available online: https://eur-lex.europa.eu/eli/dir/2007/68/oj (accessed on 6 January 2023).
- Food Allergen Labeling and Consumer Protection Act of 2004. 21 USC 301 Note. Available online: https://www.fda.gov/food/food-allergensgluten-free-guidance-documents-regulatory-information/food-allergen-labeling-and-consumer-protection-act-2004-falcpa (accessed on 10 January 2023).
- Allergen Nomenclature WHO/IUIS Allergen Nomenclature Sub-committee. Available online: http://www.allergome.org (accessed on 14 January 2023).
- Holzhauser, T.; Wackermann, O.; Ballmer-Weber, B.K.; Bindslev-Jensen, C.; Scibilia, J.; Perono-Garoffo, L.; Utsumi, S.; Poulsen, L.K.; Vieths, S. Soybean (Gly-cine max) allergy in Europe: Gly m 5 (beta-conglycinin) and Gly m 6 (glycinin) Are Potential Diagnostic Markers For Severe Allergic Reactions To Soy. J. Allergy Clin. Immunol. 2009, 123, 452–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evrard, B.; Cosme, J.; Raveau, M.; Junda, M.; Michaud, E.; Bonnet, B. Utility of the Basophil Activation Test Using Gly m 4, Gly m 5 and Gly m 6 Molecular Allergens for Characterizing Anaphylactic Reactions to Soy. Front. Allergy 2022, 3. [Google Scholar] [CrossRef]
- Medic, J.; Atkinson, C.; Hurburgh, C.R. Current Knowledge in Soybean Composition. J. Am. Oil Chem. Soc. 2014, 91, 363–384. [Google Scholar] [CrossRef]
- Fukutomi, Y.; Sjölander, S.; Nakazawa, T.; Borres, M.P.; Ishii, T.; Nakayama, S.; Tanaka, A.; Taniguchi, M.; Saito, A.; Yasueda, H.; et al. Clinical relevance of IgE to recombinant Gly m 4 in the diagnosis of adult soybean allergy. J. Allergy Clin. Immunol. 2012, 129, 860–863. [Google Scholar] [CrossRef] [Green Version]
- Berkner, H.; Neudecker, P.; Mittag, D.; Ballmer-Weber, B.K.; Schweimer, K.; Vieths, S.; Rösch, P. Cross-reactivity of pollen and food allergens: Soybean Gly m 4Is A Member of The Bet v 1 Superfamily and Closely Resembles Yellow Lupine Proteins. Biosci. Rep. 2009, 29, 183–192. [Google Scholar] [CrossRef] [Green Version]
- Katelaris, C.H. Food allergy and oral allergy or pollen-food syndrome. Curr. Opin. Allergy Clin. Immunol. 2010, 10, 246–251. [Google Scholar] [CrossRef]
- Asero, R.; Ariano, R.; Aruanno, A.; Barzaghi, C.; Borelli, P.; Busa, M.; Celi, G.; Cinquini, M.; Cortellini, G.; D’Auria, F.; et al. Systemic allergic reactions inductions by labile plant-food allergens: Seeking Potential Cofactors. A Multicenter Study. Allergy 2021, 76, 1473–1479. [Google Scholar] [CrossRef]
- Hao, G.D.; Zheng, Y.W.; Wang, Z.X.; Kong, X.A.; Song, Z.J.; Lai, X.X.; Spangfort, M.D. High correlation of specific IgE sensitization between birch pollen, soy and apple allergens indicates pollen-food allergy syndrome among birch pollen allergic patients in northern China. J. Zhejiang Univ. Sci. B 2016, 17, 399–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosma, P.; Sjölander, S.; Landgren, E.; Borres, M.P.; Hedlin, G. Severe reactions after the intake of soy drink in birch pollen-allergic children sensitized to Gly m 4. Acta Paediatr. 2010, 100, 305–306. [Google Scholar] [CrossRef] [PubMed]
- Chan, E.S.; Greenhawt, M.J.; Fleischer, D.M.; Caubet, J.-C. Managing Cross-Reactivity in Those with Peanut Allergy. J. Allergy Clin. Immunol. Pract. 2018, 7, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Kleine-Tebbe, J.; Wangorsch, A.; Vogel, L.; Crowell, D.N.; Haustein, U.-F.; Vieths, S. Severe oral allergy syndrome and anaphylactic reactions caused by a Bet v 1– related PR-10 protein in soybean, SAM22. J. Allergy Clin. Immunol. 2002, 110, 797–804. [Google Scholar] [CrossRef]
- Mittag, D.; Vieths, S.; Vogel, L.; Becker, W.-M.; Rihs, H.-P.; Helbling, A.; Wüthrich, B.; Ballmer-Weber, B.K. Soybean allergy in patients allergic to birch pollen: Clinical Investigation and Molecular Characterization of Allergens. J. Allergy Clin. Immunol. 2004, 113, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Schulten, V.; Lauer, I.; Scheurer, S.; Thalhammer, T.; Bohle, B. A food matrix reduces digestion and absorption of food allergens in vivo. Mol. Nutr. Food Res. 2011, 55, 1484–1491. [Google Scholar] [CrossRef]
- Katelaris, C.H.; Beggs, P.J. Climate change: Allergens and Allergic Disease. Int. Med. J. 2018, 48, 129–134. [Google Scholar] [CrossRef] [Green Version]
- Burney, P.G.J.; Potts, J.; Kummeling, I.; Mills, E.N.C.; Clausen, M.; Dubakiene, R.; Barreales, L.; Pérez, C.F.; Fernandez-Rivas, M.; Le, T.-M.; et al. The prevalence and distribution of food sensitization in European adults. Allergy 2013, 69, 365–371. [Google Scholar] [CrossRef] [Green Version]
- Minami, T.; Fukutomi, Y.; Saito, A.; Sekiya, K.; Tsuburai, T.; Taniguchi, M.; Akiyami, K. Frequent episodes of adult soybean allergy during and following the pollen season. J. Allergy Clin. Immunol. Pract. 2015, 3, 441–442. [Google Scholar] [CrossRef]
- Biedermann, T.; Winther, L.; Till, S.J.; Panzner, P.; Knulst, A.; Valovirta, E. Birch pollen allergy in Europe. Allergy 2019, 74, 1237–1248. [Google Scholar] [CrossRef] [Green Version]
- D’Amato, G.; Cecchi, L.; Bonini, S.; Nunes, C.; Annesi-Maesano, I.; Behrendt, H.; Liccardi, G.; Popov, T.; Van Cauwenberge, P. Allergenic pollen and pollen allergy in Europe. Allergy 2007, 62, 976–990. [Google Scholar] [CrossRef] [PubMed]
- Arbes, S.J., Jr.; Gergen, P.J.; Ellitt, L.; Zeldin, D.C. Prevalence of positive skin test responses to 10 common allergens in the US population: Results From The Third National Health and Nutrition Examination Survey. J. Allergy Clin. Immunol. 2005, 116, 377–383. [Google Scholar] [CrossRef]
- Migueres, M.; Fontaine, J.-F.; Haddad, T.; Grosclaude, M.; Saint-Martin, F.; David, D.B.; Crestani, B. Characteristics of Patients with Respiratory Allergy in France and Factors Influencing Immunotherapy Prescription: A Prospective Observational Study (Realis). Int. J. Immunopathol. Pharmacol. 2011, 24, 387–400. [Google Scholar] [CrossRef] [PubMed]
- Ciprandi, G.; Cirillo, I. Monosensitization and polysensitization in allergic rhinitis. Eur. J. Intern. Med. 2011, 22, e75–e79. [Google Scholar] [CrossRef]
- Migueres, M.; Dávila, I.; Frati, F.; Azpeitia, A.; Jeanpetit, Y.; Lhéritier-Barrand, M.; Incorvaia, C.; Ciprandi, G. PlurAL study group Types of sensitization to aeroallergens: Definitions, Prevalences and Impact On The Diagnosis and Treatment of Allergic Respiratory Disease. Clin. Transl. Allergy 2014, 4, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magnusson, J.; Lin, X.P.; Dahlman-Höglund, A.; Hanson, L.; Telemo, E.; Magnusson, O.; Bengtsson, U.; Ahlstedt, S. Seasonal intestinal inflammation in patients with birch pollen allergy. J. Allergy Clin. Immunol. 2003, 112, 45–51. [Google Scholar] [CrossRef]
- Rentzos, G.; Lundberg, V.; Stotzer, P.; Pullerits, T.; Telemo, E. Intestinal allergic inflammation in birch pollen allergic patients in relation to pollen season, IgE sensitization profile and gastrointestinal symptoms. Clin. Transl. Allergy 2014, 4, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, X.P.; Magnusson, J.; Ahlstedt, S.; Dahlman-Hoglund, A.; Hanson, L.L.; Magnusson, O.; Bengtsson, U.; Telemo, E. Local aller-gic reaction in food-hypersensitive adults despite a lack of systemic food-specific IgE. J. Allergy Clin. Immunol. 2002, 109, 879–887. [Google Scholar] [CrossRef]
- Lee, K.S.; Kim, K.; Choi, Y.J.; Yang, S.; Kim, C.R.; Moon, J.H.; Kim, K.R.; Lee, Y.S.; Oh, J.W. Increased sensitization rates to tree pollens in allergic children and adolescents and a change in the pollen season in the metropolitan area of Seoul, Korea. Pediatr. Allergy Immunol. 2021, 32, 872–879. [Google Scholar] [CrossRef]
- Kim, J.H.; Oh, J.W.; Lee, H.B. Changes in sensitization rate to weed allergens in children with increased weeds pollen counts in Seoul metropolitan area. J. Korean Med. Sci. 2012, 27, 350–355. [Google Scholar] [CrossRef] [Green Version]
- Choi, Y.J.; Lee, K.S.; Oh, J.W. The impact of climate change on pollen season and allergic sensitization to pollens. Immunol. Allergy Clin. N. Am. 2021, 41, 97–109. [Google Scholar] [CrossRef] [PubMed]
- Rentzos, G.; Lundberg, V.; Lundqvist, C.; Rodrigues, R.; van Odijk, J.; Lundell, A.; Pullerits, T.; Telemo, E. Use of a basophil activation test as a complementary diagnostic tool in the diagnosis of severe peanut allergy in adults. Clin. Transl. Allergy 2015, 5, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshida, T.; Chinuki, Y.; Matsuki, S.; Morita, E. Positive basophil activation test with soymilk protein identifies Gly m 4–related soymilk allergy. J. Cutan. Immunol. Allergy 2021, 4, 128–131. [Google Scholar] [CrossRef]
- Briceno Noriega, D.; Teodorowicz, M.; Savelkoul, H.F.J.; Ruinemans-Koerts, J. The basophil activation test for clinical manage-ment of food allergies: Recent Advances and Future Directions. J. Asthma Allergy 2021, 14. [Google Scholar] [CrossRef] [PubMed]
- Stukus, D.R.; Mikhail, I. Pearls and Pitfalls in Diagnosing IgE-Mediated Food Allergy. Curr. Allergy Asthma Rep. 2016, 16, 1–10. [Google Scholar] [CrossRef]
- Sampson, H.A.; Aceves, S.; Bock, S.A.; James, J.; Jones, S.; Lang, D.; Nadeau, K.; Nowak-Wegrzyn, A.; Oppenheimer, J.; Perry, T.T.; et al. Food allergy: A Practice Parameter Update—2014. J. Allergy Clin. Immunol. 2014, 134, 1016–1025. [Google Scholar] [CrossRef]
- Bühlmann. Flow Cast Basophil Activation Test (BAT) Flow Cytometry; Bühlmann Laboratories AG: Schönenbuch, Switzerland, 2011; Available online: https://www.buhlmannlabs.ch//wp-content/uploads/2015/03/fk-ccr-tf038ml-05e.pdf (accessed on 9 September 2021).
- Vissers, Y.M.; Jansen, A.P.H.; Ruinemans-Koerts, J.; Wichers, J.; Savelkoul, H.F.J. IgE component resolved allergen profile and clinical symptoms in soy and peanut allergic patients. Allergy 2011, 66, 1125–1127. [Google Scholar] [CrossRef]
- Cabanillas, B.; Jappe, U.; Novak, N. Allergy to Peanut, Soybean and Other Legumes: Recent Advanced in Allergen Characteri-zation, Stability to Processing and IgE Cross-Reactivity. Mol. Nutr. Food Res. 2018, 62. [Google Scholar] [CrossRef]
- Schmidt-Hieltjes, Y.; Teodorowicz, M.; Jansen, A.; Hartog, G.D.; Elfvering-Berendsen, L.; de Jong, N.W.; Savelkoul, H.F.; Ruinemans-Koerts, J. An alternative inhibition method for determining cross-reactive allergens. Clin. Chem. Lab. Med. 2016, 55, 248–253. [Google Scholar] [CrossRef]
- Vissers, Y.M.; Iwan, M.; Adel-Patient, K.; Stahl Skov, P.; Rigby, N.M.; Johnson, P.E.; Mandrup Müller, P.; Przybylski-Nicaise, L.; Schaap, M.; Ruinemans-Koerts, J.; et al. Effect of roasting on the allergenicity of major peanut allergens ara h 1 and ara h2/6: The Necessity of Degranulation. Clin. Exp. Allergy 2011, 41, 1631–1642. [Google Scholar] [CrossRef]
- Kleine-Tebbe, J.; Herold, D.A.; Vieths, S. Soy allergy due to cross reactions to major birch pollen allergen Bet v 1. Allergologie 2008, 31, 303–313. [Google Scholar] [CrossRef]
- Ansotegui, I.J.; Melioli, G.; Canonica, G.W.; Caraballo, L.; Villa, E.; Ebisawa, M.; Passalacqua, G.; Savi, E.; Ebo, D.; Gómez, R.M.; et al. IgE allergy diagnostics and other relevant tests in allergy, a World Allergy Organization position paper. World Allergy Organ. J. 2020, 13, 100080. [Google Scholar] [CrossRef] [PubMed]
- Sin, B.A.; Inceoglu, O.; Mungan, D.; Celik, G.; Kaplan, A.; Misirligil, Z. Is it important to perform pollen skin prick test in the season? Ann. Allergy Asthma Immunol. 2001, 86, 382–386. [Google Scholar] [CrossRef] [PubMed]
- Beeh, K.M.; Beier, J.; Ruhl, R. Seasonal variations of serum-IgE and potential impact on dose-calculation of omalizumab (rhuMab-E25, anti-IgE). Pneumologie 2004, 58, 546–551. [Google Scholar] [CrossRef] [Green Version]
- Lam, H.C.Y.; Jarvis, D.; ECRHS I Investigators. Seasonal variation in total and pollen-specific immunoglobulin E levels in the European community respiratory health survey. Clin. Exp. Allergy 2021, 51, 1085–1088. [Google Scholar] [CrossRef]
- Olivieri, M.; Heinrich, J.; Schlünssen, V.; Antó, J.M.; Forsberg, B.; Janson, C.; Leynaert, B.; Norback, D.; Sigsgaard, T.; Svanes, C.; et al. The risk of respiratory symptoms on allergen exposure increases with increasing specific IgE levels. Allergy 2016, 71, 859–868. [Google Scholar] [CrossRef]
- Bohle, B. The impact of pollen-related food allergens on pollen allergy. Allergy 2007, 62, 3–10. [Google Scholar] [CrossRef]
- Hansen, K.S.; Vieths, S.; Vestergaard, H.; Skov, P.S.; Bindslev-Jensen, C.; Poulsen, L.K. Seasonal variation in food allergy to apple. J. Chromatogr. B Biomed. Appl. 2001, 756, 19–32. [Google Scholar] [CrossRef]
- Osterballe, M.; Hansen, T.K.; Mortz, C.G.; Bindslev-Jensen, C. The clinical relevance of sensitization to pollen-related fruits and vegetables in unselected pollen-sensitized adults. Allergy 2005, 60, 218–225. [Google Scholar] [CrossRef]
- Galli, S.J.; Tsai, M. IgE and mast cells in allergic disease. Nat. Med. 2012, 18, 693–704. [Google Scholar] [CrossRef] [Green Version]
- Carlsson, M.; Thorell, L.; Sjölander, A.; Larsson-Faria, S. Variability of Total and Free IgE Levels and IgE Receptor Expression in Allergic Subjects in and Out of Pollen Season. Scand. J. Immunol. 2015, 81, 240–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teodorowicz, M.; Van Neerven, J.; Savelkoul, H. Food Processing: The Influence of The Maillard Reaction On Immunogenicity and Allergenicity of Food Proteins. Nutrients 2017, 9, 835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van den Berg, L.; Mes, J.J.; Mensink, M.; Wanders, A.J. Protein quality of soy and the effect of processing: A quantitative re-view. Front. Nutr. 2022, 9, 1004754. [Google Scholar] [CrossRef] [PubMed]
- Toda, M.; Heilmann, M.; Ilchmann, A.; Vieths, S. The maillard reaction and food allergies: Is There A Link? Clin. Chem. Lab. Med. 2014, 52, 61–67. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| ImmunoCAP IgE (kU/L) * | Soy Diet | Symptoms | |||||
|---|---|---|---|---|---|---|---|
| Soybean | Gly m 4 | Gly m 5 | Gly m 6 | Bet v 1 | |||
| Outside of the Birch Pollen Season | 0.63 | 2.13 | 0.91 | 1.42 | 6.3 | Tolerance to processed soy | - |
| Peak of the Birch Pollen Season | 1.15 | 7.12 | 1.33 | 2.14 | 16.3 | Strict diet | OAS, AS, AP, D |
| DPA-Dx (Ku/L) | |||
|---|---|---|---|
| kU/L * | kU/L * | ||
| Birch | 38.5 | Peanut | 98.1 |
| rBet v 1 | 43.8 | rAra h 1 | 0.7 |
| rBet v 2 | <0.35 | rAra h 2 | 11.4 |
| rBet v 4 | <0.35 | rAra h 3 | 2 |
| rBet v 6 | <0.35 | rAra h 6 | 37.2 |
| rAra h 7 | 21.1 | ||
| rAra h 5 | <0.35 | ||
| rAra h 9 | <0.35 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Briceno Noriega, D.; Savelkoul, H.F.J.; Jansen, A.; Teodorowicz, M.; Ruinemans-Koerts, J. Pollen Sensitization Can Increase the Allergic Reaction to Non-Cross-Reactive Allergens in a Soy-Allergic Patient. Int. J. Environ. Res. Public Health 2023, 20, 6045. https://doi.org/10.3390/ijerph20116045
Briceno Noriega D, Savelkoul HFJ, Jansen A, Teodorowicz M, Ruinemans-Koerts J. Pollen Sensitization Can Increase the Allergic Reaction to Non-Cross-Reactive Allergens in a Soy-Allergic Patient. International Journal of Environmental Research and Public Health. 2023; 20(11):6045. https://doi.org/10.3390/ijerph20116045
Chicago/Turabian StyleBriceno Noriega, Daniela, Huub F. J. Savelkoul, Ad Jansen, Malgorzata Teodorowicz, and Janneke Ruinemans-Koerts. 2023. "Pollen Sensitization Can Increase the Allergic Reaction to Non-Cross-Reactive Allergens in a Soy-Allergic Patient" International Journal of Environmental Research and Public Health 20, no. 11: 6045. https://doi.org/10.3390/ijerph20116045
APA StyleBriceno Noriega, D., Savelkoul, H. F. J., Jansen, A., Teodorowicz, M., & Ruinemans-Koerts, J. (2023). Pollen Sensitization Can Increase the Allergic Reaction to Non-Cross-Reactive Allergens in a Soy-Allergic Patient. International Journal of Environmental Research and Public Health, 20(11), 6045. https://doi.org/10.3390/ijerph20116045